

Increased Epicardial Adipose Tissue (EAT), Left Coronary Artery Plaque Morphology, and Valvular Atherosclerosis as Risks Factors for Sudden Cardiac Death from a Forensic Perspective

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sudden Cardiac Death Group
2.3. Control Group
2.4. Heart Characteristics and Left Coronary Artery Plaque Morphology
2.5. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Results Report 2020–2021. Available online: https://www.who.int/about/accountability/results/who-results-report-2020-2021 (accessed on 1 December 2022).
- Chugh, S.S.; Jui, J.; Gunson, K.; Stecker, E.C.; John, B.T.; Thompson, B.; Ilias, N.; Vickers, C.; Dogra, V.; Daya, M.; et al. Current Burden of Sudden Cardiac Death: Multiple Source Surveillance versus Retrospective Death Certificate-Based Review in a Large U.S. Community. J. Am. Coll. Cardiol. 2004, 44, 1268–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, C.M.; Chae, C.U.; Grodstein, F.; Rose, L.M.; Rexrode, K.M.; Ruskin, J.N.; Stampfer, M.J.; Manson, J.E. Prospective Study of Sudden Cardiac Death among Women in the United States. Circulation 2003, 107, 2096–2101. [Google Scholar] [CrossRef]
- Adabag, A.S.; Luepker, R.V.; Roger, V.L.; Gersh, B.J. Sudden Cardiac Death: Epidemiology and Risk Factors. Nat. Rev. Cardiol. 2010, 7, 216–225. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.Y.; Sotoodehnia, N.; Bůžková, P.; Lopez, F.L.; Yee, L.M.; Heckbert, S.R.; Prineas, R.; Soliman, E.Z.; Adabag, S.; Konety, S.; et al. Atrial Fibrillation and the Risk of Sudden Cardiac Death: The Atherosclerosis Risk in Communities (ARIC) Study and Cardiovascular Health Study (CHS). JAMA Intern. Med. 2013, 173, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.; Norby, F.L.; Katz, R.; Sotoodehnia, N.; Adabag, S.; DeFilippi, C.R.; Kestenbaum, B.; Chen, L.Y.; Heckbert, S.R.; Folsom, A.R.; et al. Development and Validation of a Sudden Cardiac Death Prediction Model for the General Population. Circulation 2016, 134, 806–816. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Schlesinger, S.; Norat, T.; Riboli, E. Body Mass Index, Abdominal Fatness, and the Risk of Sudden Cardiac Death: A Systematic Review and Dose–Response Meta-Analysis of Prospective Studies. Eur. J. Epidemiol. 2018, 33, 711–722. [Google Scholar] [CrossRef] [Green Version]
- Hirata, Y.; Tabata, M.; Kurobe, H.; Motoki, T.; Akaike, M.; Nishio, C.; Higashida, M.; Mikasa, H.; Nakaya, Y.; Takanashi, S.; et al. Coronary Atherosclerosis Is Associated with Macrophage Polarization in Epicardial Adipose Tissue. J. Am. Coll. Cardiol. 2011, 58, 248–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruzdeva, O.V.; Dyleva, Y.A.; Belik, E.V.; Sinitsky, M.Y.; Stasev, A.N.; Kokov, A.N.; Brel, N.K.; Krivkina, E.O.; Bychkova, E.E.; Tarasov, R.S.; et al. Relationship between Epicardial and Coronary Adipose Tissue and the Expression of Adiponectin, Leptin, and Interleukin 6 in Patients with Coronary Artery Disease. J. Pers. Med. 2022, 12, 129. [Google Scholar] [CrossRef]
- Xu, Y.; Cheng, X.; Hong, K.; Huang, C.; Wan, L. How to Interpret Epicardial Adipose Tissue as a Cause of Coronary Artery Disease: A Meta-Analysis. Coron. Artery Dis. 2012, 23, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Venteclef, N.; Guglielmi, V.; Balse, E.; Gaborit, B.; Cotillard, A.; Atassi, F.; Amour, J.; Leprince, P.; Dutour, A.; Clément, K.; et al. Human Epicardial Adipose Tissue Induces Fibrosis of the Atrial Myocardium through the Secretion of Adipo-Fibrokines. Eur. Heart J. 2015, 36, 795–805. [Google Scholar] [CrossRef]
- Mazurek, T.; Kiliszek, M.; Kobylecka, M.; Skubisz-Głuchowska, J.; Kochman, J.; Filipiak, K.; Królicki, L.; Opolski, G. Relation of Proinflammatory Activity of Epicardial Adipose Tissue to the Occurrence of Atrial Fibrillation. Am. J. Cardiol. 2014, 113, 1505–1508. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W. Epicardial Fat: Properties, Function and Relationship to Obesity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2007, 8, 253–261. [Google Scholar] [CrossRef]
- Marchington, J.M.; Mattacks, C.A.; Pond, C.M. Adipose Tissue in the Mammalian Heart and Pericardium: Structure, Foetal Development and Biochemical Properties. Comp. Biochem. Physiol. B 1989, 94, 225–232. [Google Scholar] [CrossRef]
- Nagy, E.; Jermendy, A.L.; Merkely, B.; Maurovich-Horvat, P. Clinical Importance of Epicardial Adipose Tissue. Arch. Med. Sci. AMS 2017, 13, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Gaborit, B.; Venteclef, N.; Ancel, P.; Pelloux, V.; Gariboldi, V.; Leprince, P.; Amour, J.; Hatem, S.N.; Jouve, E.; Dutour, A.; et al. Human Epicardial Adipose Tissue Has a Specific Transcriptomic Signature Depending on Its Anatomical Peri-Atrial, Peri-Ventricular, or Peri-Coronary Location. Cardiovasc. Res. 2015, 108, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, A.R.; Harte, A.L.; Howell, N.; Pritlove, D.C.; Ranasinghe, A.M.; da Silva, N.F.; Youssef, E.M.; Khunti, K.; Davies, M.J.; Bonser, R.S.; et al. Epicardial Adipose Tissue as a Source of Nuclear Factor-KappaB and c-Jun N-Terminal Kinase Mediated Inflammation in Patients with Coronary Artery Disease. J. Clin. Endocrinol. Metab. 2009, 94, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Mazurek, T.; Zhang, L.; Zalewski, A.; Mannion, J.D.; Diehl, J.T.; Arafat, H.; Sarov-Blat, L.; O’Brien, S.; Keiper, E.A.; Johnson, A.G.; et al. Human Epicardial Adipose Tissue Is a Source of Inflammatory Mediators. Circulation 2003, 108, 2460–2466. [Google Scholar] [CrossRef] [Green Version]
- McAninch, E.A.; Fonseca, T.L.; Poggioli, R.; Panos, A.L.; Salerno, T.A.; Deng, Y.; Li, Y.; Bianco, A.C.; Iacobellis, G. Epicardial Adipose Tissue Has a Unique Transcriptome Modified in Severe Coronary Artery Disease. Obes. Silver Spring Md 2015, 23, 1267–1278. [Google Scholar] [CrossRef]
- Greulich, S.; Maxhera, B.; Vandenplas, G.; de Wiza, D.H.; Smiris, K.; Mueller, H.; Heinrichs, J.; Blumensatt, M.; Cuvelier, C.; Akhyari, P.; et al. Secretory Products from Epicardial Adipose Tissue of Patients with Type 2 Diabetes Mellitus Induce Cardiomyocyte Dysfunction. Circulation 2012, 126, 2324–2334. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.Y.-M.; Ho, S.S.-Y.; Wang, M.; Liu, E.K.-H.; Ho, S.; Li, P.K.-T.; Lui, S.-F.; Sanderson, J.E. Cardiac Valvular Calcification as a Marker of Atherosclerosis and Arterial Calcification in End-Stage Renal Disease. Arch. Intern. Med. 2005, 165, 327–332. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Stary, H.C.; Chandler, A.B.; Dinsmore, R.E.; Fuster, V.; Glagov, S.; Insull, W.; Rosenfeld, M.E.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A Definition of Advanced Types of Atherosclerotic Lesions and a Histological Classification of Atherosclerosis. A Report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation 1995, 92, 1355–1374. [Google Scholar] [CrossRef]
- Adabag, A.S.; Peterson, G.; Apple, F.S.; Titus, J.; King, R.; Luepker, R.V. Etiology of Sudden Death in the Community: Results of Anatomical, Metabolic, and Genetic Evaluation. Am. Heart J. 2010, 159, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Uretsky, B.F.; Thygesen, K.; Armstrong, P.W.; Cleland, J.G.; Horowitz, J.D.; Massie, B.M.; Packer, M.; Poole-Wilson, P.A.; Ryden, L. Acute Coronary Findings at Autopsy in Heart Failure Patients With Sudden Death. Circulation 2000, 102, 611–616. [Google Scholar] [CrossRef]
- Eckel, R.; Kahn, R.; Robertson, R.; Rizza, R. Preventing Cardiovascular Disease and Diabetes: A Call to Action from the American Diabetes Association and the American Heart Association. Diabetes Care 2006, 29, 1697–1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homan, E.A.; Reyes, M.V.; Hickey, K.T.; Morrow, J.P. Clinical Overview of Obesity and Diabetes Mellitus as Risk Factors for Atrial Fibrillation and Sudden Cardiac Death. Front. Physiol. 2019, 9, 1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remme, C.A. Sudden Cardiac Death in Diabetes and Obesity: Mechanisms and Therapeutic Strategies. Can. J. Cardiol. 2022, 38, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Papadakis, M.; Dhutia, H.; Cole, D.; Behr, E.R.; Tome, M.; Sharma, S.; Sheppard, M.N. Obesity and Sudden Cardiac Death in the Young: Clinical and Pathological Insights from a Large National Registry. Eur. J. Prev. Cardiol. 2018, 25, 395–401. [Google Scholar] [CrossRef]
- Adabag, S.; Huxley, R.R.; Lopez, F.L.; Chen, L.Y.; Sotoodehnia, N.; Siscovick, D.; Deo, R.; Konety, S.; Alonso, A.; Folsom, A.R. Obesity Related Risk of Sudden Cardiac Death in the Atherosclerosis Risk in Communities Study. Heart 2015, 101, 215–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, J.; Wennberg, P.; Lundblad, D.; Escher, S.A.; Jansson, J.-H. Diabetes Mellitus, High BMI and Low Education Level Predict Sudden Cardiac Death within 24 Hours of Incident Myocardial Infarction. Eur. J. Prev. Cardiol. 2016, 23, 1814–1820. [Google Scholar] [CrossRef]
- Margolis, G.; Elbaz-Greener, G.; Ruskin, J.N.; Roguin, A.; Amir, O.; Rozen, G. The Impact of Obesity on Sudden Cardiac Death Risk. Curr. Cardiol. Rep. 2022, 24, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.J.F.; Ray, M.N. Structure Strategy Interventions: Increasing Reading Comprehension of Expository Text. Int. Electron. J. Elem. Educ. 2011, 4, 127–152. [Google Scholar]
- Fabre, A.; Sheppard, M.N. Sudden Adult Death Syndrome and Other Non-Ischaemic Causes of Sudden Cardiac Death. Heart 2006, 92, 316–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayanan, K.; Reinier, K.; Teodorescu, C.; Uy-Evanado, A.; Aleong, R.; Chugh, H.; Nichols, G.A.; Gunson, K.; London, B.; Jui, J.; et al. Left Ventricular Diameter and Risk Stratification for Sudden Cardiac Death. J. Am. Heart Assoc. 2014, 3, e001193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Yang, F.; Wan, K.; Mui, D.; Han, Y.; Chen, Y. Left Ventricular Midwall Fibrosis as a Predictor of Sudden Cardiac Death in Non-Ischaemic Dilated Cardiomyopathy: A Meta-Analysis. ESC Heart Fail. 2020, 7, 2184–2192. [Google Scholar] [CrossRef]
- Centurión, O.A.; Alderete, J.F.; Torales, J.M.; García, L.B.; Scavenius, K.E.; Miño, L.M. Myocardial Fibrosis as a Pathway of Prediction of Ventricular Arrhythmias and Sudden Cardiac Death in Patients With Nonischemic Dilated Cardiomyopathy. Crit. Pathw. Cardiol. 2019, 18, 89–97. [Google Scholar] [CrossRef]
- Gulati, A.; Jabbour, A.; Ismail, T.F.; Guha, K.; Khwaja, J.; Raza, S.; Morarji, K.; Brown, T.D.H.; Ismail, N.A.; Dweck, M.R.; et al. Association of Fibrosis With Mortality and Sudden Cardiac Death in Patients With Nonischemic Dilated Cardiomyopathy. JAMA 2013, 309, 896–908. [Google Scholar] [CrossRef] [Green Version]
- Koutalas, E.; Kanoupakis, E.; Vardas, P. Sudden Cardiac Death in Non-Ischemic Dilated Cardiomyopathy: A Critical Appraisal of Existing and Potential Risk Stratification Tools. Int. J. Cardiol. 2013, 167, 335–341. [Google Scholar] [CrossRef]
- Zorzi, A.; Perazzolo Marra, M.; Rigato, I.; De Lazzari, M.; Susana, A.; Niero, A.; Pilichou, K.; Migliore, F.; Rizzo, S.; Giorgi, B.; et al. Nonischemic Left Ventricular Scar as a Substrate of Life-Threatening Ventricular Arrhythmias and Sudden Cardiac Death in Competitive Athletes. Circ. Arrhythm. Electrophysiol. 2016, 9, e004229. [Google Scholar] [CrossRef]
- Owens, D.S.; Budoff, M.J.; Katz, R.; Takasu, J.; Shavelle, D.M.; Carr, J.J.; Heckbert, S.R.; Otto, C.M.; Probstfield, J.L.; Kronmal, R.A.; et al. Aortic Valve Calcium Independently Predicts Coronary and Cardiovascular Events in a Primary Prevention Population. JACC Cardiovasc. Imaging 2012, 5, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.Y.-M.; Wang, M.; Woo, J.; Lam, C.W.-K.; Li, P.K.-T.; Lui, S.-F.; Sanderson, J.E. Cardiac Valve Calcification as an Important Predictor for All-Cause Mortality and Cardiovascular Mortality in Long-Term Peritoneal Dialysis Patients: A Prospective Study. J. Am. Soc. Nephrol. 2003, 14, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.H.; Mintz, G.S.; Farhat, N.; Marso, S.P.; Taglieri, N.; Verheye, S.; Foster, M.C.; Margolis, M.P.; Templin, B.; Xu, K.; et al. Relation Between Angiographic Lesion Severity, Vulnerable Plaque Morphology and Future Adverse Cardiac Events (from the Providing Regional Observations to Study Predictors of Events in the Coronary Tree Study). Am. J. Cardiol. 2012, 110, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms Linking Obesity with Cardiovascular Disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef]
- Christensen, R.H.; Hansen, C.S.; von Scholten, B.J.; Jensen, M.T.; Pedersen, B.K.; Schnohr, P.; Vilsbøll, T.; Rossing, P.; Jørgensen, P.G. Epicardial and Pericardial Adipose Tissues Are Associated with Reduced Diastolic and Systolic Function in Type 2 Diabetes. Diabetes Obes. Metab. 2019, 21, 2006–2011. [Google Scholar] [CrossRef]
- Iacobellis, G.; Leonetti, F.; Singh, N.; M Sharma, A. Relationship of Epicardial Adipose Tissue with Atrial Dimensions and Diastolic Function in Morbidly Obese Subjects. Int. J. Cardiol. 2007, 115, 272–273. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Leonetti, F. Epicardial Adipose Tissue and Insulin Resistance in Obese Subjects. J. Clin. Endocrinol. Metab. 2005, 90, 6300–6302. [Google Scholar] [CrossRef]
- Eroglu, S.; Sade, L.E.; Yildirir, A.; Bal, U.; Ozbicer, S.; Ozgul, A.S.; Bozbas, H.; Aydinalp, A.; Muderrisoglu, H. Epicardial Adipose Tissue Thickness by Echocardiography Is a Marker for the Presence and Severity of Coronary Artery Disease. Nutr. Metab. Cardiovasc. Dis. NMCD 2009, 19, 211–217. [Google Scholar] [CrossRef]
- Stevens, S.M.; Reinier, K.; Chugh, S.S. Increased Left Ventricular Mass as a Predictor of Sudden Cardiac Death: Is It Time to Put It to the Test? Circ. Arrhythm. Electrophysiol. 2013, 6, 212–217. [Google Scholar] [CrossRef] [Green Version]
- Haider, A.W.; Larson, M.G.; Benjamin, E.J.; Levy, D. Increased Left Ventricular Mass and Hypertrophy Are Associated with Increased Risk for Sudden Death. J. Am. Coll. Cardiol. 1998, 32, 1454–1459. [Google Scholar] [CrossRef] [Green Version]
- Kannel, W.B.; Gordon, T.; Castelli, W.P.; Margolis, J.R. Electrocardiographic Left Ventricular Hypertrophy and Risk of Coronary Heart Disease. The Framingham Study. Ann. Intern. Med. 1970, 72, 813–822. [Google Scholar] [CrossRef]
- Christensen, R.H.; von Scholten, B.J.; Hansen, C.S.; Heywood, S.E.; Rosenmeier, J.B.; Andersen, U.B.; Hovind, P.; Reinhard, H.; Parving, H.-H.; Pedersen, B.K.; et al. Epicardial, Pericardial and Total Cardiac Fat and Cardiovascular Disease in Type 2 Diabetic Patients with Elevated Urinary Albumin Excretion Rate. Eur. J. Prev. Cardiol. 2017, 24, 1517–1524. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Centeno, E.H.; Thomas, S.; Herdman, L.; Kotanidis, C.P.; Thomas, K.E.; et al. Non-Invasive Detection of Coronary Inflammation Using Computed Tomography and Prediction of Residual Cardiovascular Risk (the CRISP CT Study): A Post-Hoc Analysis of Prospective Outcome Data. The Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef] [Green Version]
- Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public. Health 2022, 19, 13934. [Google Scholar] [CrossRef]
- Levelt, E.; Pavlides, M.; Banerjee, R.; Mahmod, M.; Kelly, C.; Sellwood, J.; Ariga, R.; Thomas, S.; Francis, J.; Rodgers, C.; et al. Ectopic and Visceral Fat Deposition in Lean and Obese Patients With Type 2 Diabetes. J. Am. Coll. Cardiol. 2016, 68, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidovich, D.; Gastaldelli, A.; Sicari, R. Imaging Cardiac Fat. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 625–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.H.; Maron, B.J.; Olivotto, I.; Pencina, M.J.; Assenza, G.E.; Haas, T.; Lesser, J.R.; Gruner, C.; Crean, A.M.; Rakowski, H.; et al. Prognostic Value of Quantitative Contrast-Enhanced Cardiovascular Magnetic Resonance for the Evaluation of Sudden Death Risk in Patients with Hypertrophic Cardiomyopathy. Circulation 2014, 130, 484–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.S.; Coady, S.; Sorlie, P.D.; Levy, D.; Meigs, J.B.; D’Agostino, R.B.; Wilson, P.W.F.; Savage, P.J. Trends in Cardiovascular Complications of Diabetes. JAMA 2004, 292, 2495–2499. [Google Scholar] [CrossRef] [Green Version]
- González, N.; Moreno-Villegas, Z.; González-Bris, A.; Egido, J.; Lorenzo, Ó. Regulation of Visceral and Epicardial Adipose Tissue for Preventing Cardiovascular Injuries Associated to Obesity and Diabetes. Cardiovasc. Diabetol. 2017, 16, 44. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-Y.; Redheuil, A.; Ouwerkerk, R.; Lima, J.A.C.; Bluemke, D.A. Myocardial Fat Quantification in Humans: Evaluation by Two-Point Water-Fat Imaging and Localized Proton Spectroscopy. Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med. 2010, 63, 892–901. [Google Scholar] [CrossRef] [Green Version]
- Iacobellis, G. Epicardial Fat: A New Cardiovascular Therapeutic Target. Curr. Opin. Pharmacol. 2016, 27, 13–18. [Google Scholar] [CrossRef]
- Iacobellis, G.; Mohseni, M.; Bianco, S.D.; Banga, P.K. Liraglutide Causes Large and Rapid Epicardial Fat Reduction. Obes. Silver Spring Md 2017, 25, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Aizawa, Y.; Yuasa, S.; Kishi, S.; Fuse, K.; Fujita, S.; Ikeda, Y.; Kitazawa, H.; Takahashi, M.; Sato, M.; et al. The Effect of Dapagliflozin Treatment on Epicardial Adipose Tissue Volume. Cardiovasc. Diabetol. 2018, 17, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabkin, S.W.; Campbell, H. Comparison of Reducing Epicardial Fat by Exercise, Diet or Bariatric Surgery Weight Loss Strategies: A Systematic Review and Meta-Analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 406–415. [Google Scholar] [CrossRef]
- Risgaard, B.; Winkel, B.G.; Jabbari, R.; Behr, E.R.; Ingemann-Hansen, O.; Thomsen, J.L.; Ottesen, G.L.; Gislason, G.H.; Bundgaard, H.; Haunsø, S.; et al. Burden of Sudden Cardiac Death in Persons Aged 1 to 49 Years: Nationwide Study in Denmark. Circ. Arrhythm. Electrophysiol. 2014, 7, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Guidi, B.; Aquaro, G.D.; Gesi, M.; Emdin, M.; Di Paolo, M. Postmortem Cardiac Magnetic Resonance in Sudden Cardiac Death. Heart Fail. Rev. 2018, 23, 651–665. [Google Scholar] [CrossRef]
- Thomsen, T. HeartScore: A New Web-Based Approach to European Cardiovascular Disease Risk Management. Eur. J. Cardiovasc. Prev. Rehabil. Off. J. Eur. Soc. Cardiol. Work. Groups Epidemiol. Prev. Card. Rehabil. Exerc. Physiol. 2005, 12, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Ullmann, S.G. Alternative Research Funding to Improve Clinical Outcomes. Circ. Arrhythm. Electrophysiol. 2015, 8, 492–498. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Autopsies N = 80 | A–H n = 40 | SCD n = 40 | p-Value (OR; CI 95%) |
|---|---|---|---|---|
| Age (years) MEAN ± SD | 56.11 ± 11.7 | 53.4 ± 13.00 | 58.82 ± 9.67 | 0.03 |
| Male/female (sex) no. (%) | 64 (80%) 16 (20%) | 36 (90%) 4 (10%) | 28 (70%) 12 (30%) | 0.03 (0.25; 0.07–0.89) |
| Heart and Coronary Artery Characteristic | ||||
| BMI (kg/m2), median [Q1–Q3] | 24.8 [23.25–26.6] | 23.9 [22.35–25.5] | 25.8 [24.42–28.2] | 0.0009 |
| Heart weight (g), median [Q1–Q3] | 420 [368.75–485] | 390 [347.5–425] | 480 [407.5–550] | <0.0001 |
| EAT LCx (cm), median [Q1–Q3] | 0.6 [0.3–0.725] | 0.3 [0.3–0.525] | 0.7 [0.6–0.8] | <0.0001 |
| EAT LAD (cm), median [Q1–Q3] | 0.6 [0.5–0.8] | 0.5 [0.3–0.6] | 0.8 [0.6–0.925] | <0.0001 |
| Lv thickness (cm), median [Q1–q3] | 1.1 [1–1.225] | 1 [1–1.3] | 1.2 [1–1.2] | 0.15 |
| IV thickness (cm), median [Q1–Q3] | 1.2 [1–1.3] | 1.2 [1–1.3] | 1.2 [1–1.425] | 0.19 |
| Histological Type of Left Coronary Artery Plaque | ||||
| No lesion, no. (%) | 11 (13.75%) | 11 (27.5%) | 0.01 | |
| Type I, no. (%) | 17 (21.25%) | 15 (37.5%) | 2 (5%) | 0.002 |
| Type II, no. (%) | 4 (5%) | 4 (10%) | 0.12 | |
| Type III, no. (%) | 6 (7.5%) | 3 (7.5%) | 3 (7.5%) | ns |
| Type IV, no. (%) | 3 (3.75%) | 3 (7.5%) | 0.18 | |
| Type Va no. (%) | 8 (10%) | 5 (12.5%) | 3 (7.5%) | 0.46 |
| Type Vb, no. (%) | 19 (23.75%) | 19 (47.5%) | 0.003 | |
| Type Vc no. (%) | 4 (5%) | 1 (2.5%) | 3 (7.5%) | 0.32 |
| Type Vi, no. (%) | 8 (10%) | 1 (2.5%) | 7 (17.5%) | 0.053 |
| Valvular Atherosclerosis | ||||
| Absent, no. (%) | 46 (57.5%) | 32 (80%) | 14 (35%) | 0.0001 (0.13; 0.04–0.37) |
| Mild, no. (%) | 30 (37.5%) | 8 (20%) | 22 (55%) | 0.001 (4.88; 1.80–13.21) |
| Moderate, no. (%) | 4 (5%) | 4 (10%) | 0.12 (9.98; 0.51–191.91) | |
| Left Ventricle Dilatation | ||||
| Absent, no. (%) | 33 (41.25%) | 24 (60%) | 9 (22.5%) | 0.001 (0.19; 0.07–0.51) |
| Mild, no. (%) | 29 (36.25%) | 15 (37.5%) | 14 (35%) | 0.81 (0.89; 0.36–2.23) |
| Moderate, no. (%) | 13 (16.25%) | 1 (2.5%) | 12 (30%) | 0.008 (16.7; 2.05–136.08) |
| Severe, no. (%) | 5 (6.25%) | 5 (12.5%) | 0.09 (12.5; 0.67–235.01) | |
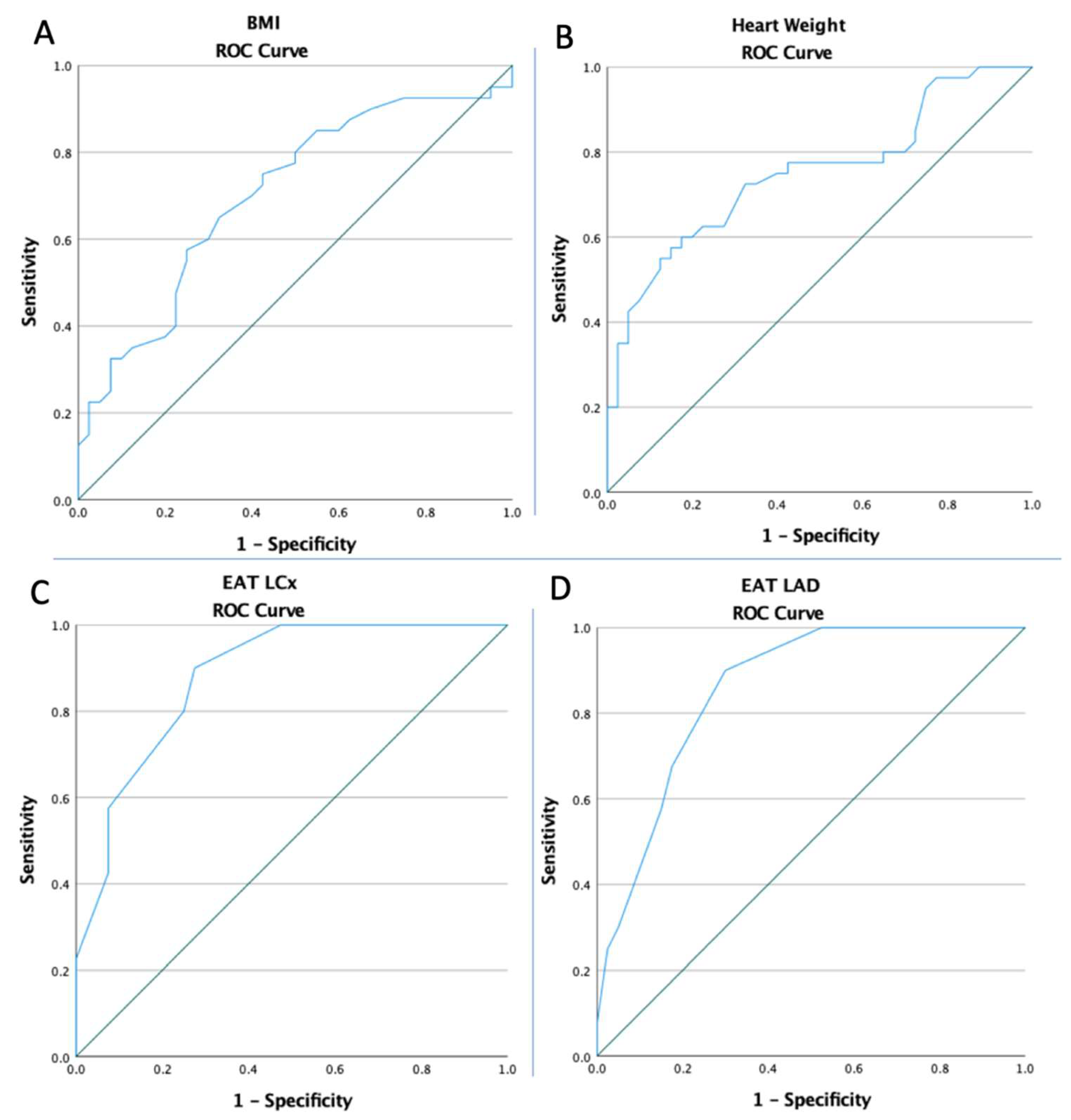
| Variables | Cut-Off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p-Value |
|---|---|---|---|---|---|---|---|
| Sudden Cardiac Death | |||||||
| BMI | 25.5 | 0.703 | 0.059 | 0.587–0.818 | 57.5% | 75% | 0.002 |
| Heart weight | 417.5 | 0.750 | 0.055 | 0.643–0.858 | 72.5% | 67.5% | <0.0001 |
| EAT LCx | 0.45 | 0.881 | 0.037 | 0.808–0.954 | 90% | 72.5% | <0.0001 |
| EAT LAD | 0.55 | 0.857 | 0.042 | 0.775–0.940 | 90% | 70% | <0.0001 |
| Sudden Cardiac Death | |||
|---|---|---|---|
| OR | 95% CI | p-Value | |
| >55 years | 2.53 | 1.02–6.29 | 0.045 |
| Male sex | 0.25 | 0.07–0.89 | 0.03 |
| Histological Type of Left Coronary Artery Plaque | |||
| No lesion | 0.06 | 0.008–0.55 | 0.01 |
| Type I plaque | 0.08 | 0.01–0.41 | 0.002 |
| Type Vb plaque | 17.19 | 3.64–81.10 | <0.001 |
| Valvular Atherosclerosis | |||
| Absent | 0.13 | 0.04–0.37 | <0.001 |
| Mild | 4.88 | 1.80–13.21 | 0.002 |
| Left Ventricle Dilatation | |||
| Absent | 0.19 | 0.07–0.51 | <0.001 |
| Moderate | 16.71 | 2.05–136.07 | 0.008 |
| Severe | 6.88 | 0.78–60.06 | 0.08 |
| High BMI | 4.05 | 1.56–10.51 | 0.004 |
| High heart weight | 5.47 | 2.09–14.28 | <0.001 |
| High EAT LCx | 23.72 | 6.83–82.36 | <0.001 |
| High EAT LAD | 21.07 | 6.11–72.18 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hogea, T.; Suciu, B.A.; Ivănescu, A.D.; Carașca, C.; Chinezu, L.; Arbănași, E.M.; Russu, E.; Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; et al. Increased Epicardial Adipose Tissue (EAT), Left Coronary Artery Plaque Morphology, and Valvular Atherosclerosis as Risks Factors for Sudden Cardiac Death from a Forensic Perspective. Diagnostics 2023, 13, 142. https://doi.org/10.3390/diagnostics13010142
Hogea T, Suciu BA, Ivănescu AD, Carașca C, Chinezu L, Arbănași EM, Russu E, Kaller R, Arbănași EM, Mureșan AV, et al. Increased Epicardial Adipose Tissue (EAT), Left Coronary Artery Plaque Morphology, and Valvular Atherosclerosis as Risks Factors for Sudden Cardiac Death from a Forensic Perspective. Diagnostics. 2023; 13(1):142. https://doi.org/10.3390/diagnostics13010142
Chicago/Turabian StyleHogea, Timur, Bogdan Andrei Suciu, Adrian Dumitru Ivănescu, Cosmin Carașca, Laura Chinezu, Emil Marian Arbănași, Eliza Russu, Réka Kaller, Eliza Mihaela Arbănași, Adrian Vasile Mureșan, and et al. 2023. "Increased Epicardial Adipose Tissue (EAT), Left Coronary Artery Plaque Morphology, and Valvular Atherosclerosis as Risks Factors for Sudden Cardiac Death from a Forensic Perspective" Diagnostics 13, no. 1: 142. https://doi.org/10.3390/diagnostics13010142