
Tricuspid Regurgitation in Acute Heart Failure: Predicting Outcome Using Novel Quantitative Echocardiography Techniques
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Echocardiography
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cleland, J.; Swedberg, K.; Follath, F.; Komajda, M.; Cohen-Solal, A.; Aguilar, J.; Dietz, R.; Gavazzi, A.; Hobbs, R.; Korewicki, J.; et al. The EuroHeart Failure survey programme—A survey on the quality of care among patients with heart failure in Europe: Part 1: Patient characteristics and diagnosis. Eur. Heart Heart J. 2003, 24, 442–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.-P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Heart failure Audit 2020. Available online: https://www.nicor.org.uk/wp-content/uploads/2020/12/National-Heart-Failure-Audit-2020-FINAL.pdf (accessed on 1 June 2022).
- Arsalan, M.; Walther, T.; Smith, R.L.; Grayburn, P.A. Tricuspid regurgitation diagnosis and treatment. Eur. Heart J. 2017, 38, 634–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutlak, D.; Lessick, J.; Khalil, S.; Yalonetsky, S.; Agmon, Y.; Aronson, D. Tricuspid regurgitation in acute heart failure: Is there any incremental risk? Eur. Heart J. -Cardiovasc. Imaging 2018, 19, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Santas, E.; Chorro, F.J.; Miñana, G.; Méndez, J.; Muñoz, J.; Escribano, D.; García-Blas, S.; Valero, E.; Bodí, V.; Núñez, E.; et al. Tricuspid regurgitation and mortality risk across left ventricular systolic function in acute heart failure. Circ. J. 2015, 79, 1526–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, J.; Koelling, T.; Semigran, M.J.; Dec, G.W.; Levine, R.A.; Di Salvo, T.G. Usefulness of echocardiographic determined tricuspid regurgitation in predicting event-free survival in severe heart failure secondary to idiopathic-dilated cardiomyopathy or to ischemic cardiomyopathy. Am. J. Cardiol. 1998, 82, 1301–1303. [Google Scholar] [CrossRef] [PubMed]
- De la Espriella, R.; Santas, E.; Chorro, F.J.; Miñana, G.; Soler, M.; Bodí, V.; Valero, E.; Núñez, E.; Bayés-Genis, A.; Lupón, J.; et al. Functional tricuspid regurgitation and recurrent admissions in patients with acute heart failure. Int. J. Cardiol. 2019, 291, 83–88. [Google Scholar] [CrossRef]
- Chioncel, O.; Mebazaa, A.; Maggioni, A.P.; Harjola, V.-P.; Rosano, G.; Laroche, C.; Piepoli, M.F.; Crespo-Leiro, M.G.; Lainscak, M.; Ponikowski, P.; et al. Acute heart failure congestion and perfusion status–impact of the clinical classification on in-hospital and long-term outcomes; insights from the ESC-EORP-HFA Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2019, 21, 1338–1352. [Google Scholar] [CrossRef]
- Hahn, R.T. State-of-the-art review of echocardiographic imaging in the evaluation and treatment of functional tricuspid regurgitation. Circ. Cardiovasc. Imaging 2016, 9, e005332. [Google Scholar] [CrossRef] [Green Version]
- Addetia, K.; Yamat, M.; Mediratta, A.; Medvedofsky, D.; Patel, M.; Ferrara, P.; Mor-Avi, V.; Lang, R.M. Comprehensive two-dimensional interrogation of the tricuspid valve using knowledge derived from three-dimensional echocardiography. J. Am. Soc. Echocardiogr. 2016, 29, 74–82. [Google Scholar] [CrossRef]
- Stankovic, I.; Daraban, A.M.; Jasaityte, R.; Neskovic, A.N.; Claus, P.; Voigt, J.U. Incremental value of the en face view of the tricuspid valve by two-dimensional and three-dimensional echocardiography for accurate identification of tricuspid valve leaflets. J. Am. Soc. Echocardiogr. 2014, 27, 376–384. [Google Scholar] [CrossRef] [Green Version]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. J. Cardio-Thorac. Surg. 2021, 60, 727–800. [Google Scholar]
- Grayburn, P.A.; Sannino, A.; Packer, M. Proportionate and disproportionate functional mitral regurgitation: A new conceptual framework that reconciles the results of the MITRA-FR and COAPT trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef]
- Packer, M.; Grayburn, P.A. New evidence supporting a novel conceptual framework for distinguishing proportionate and disproportionate functional mitral regurgitation. JAMA Cardiol. 2020, 5, 469–475. [Google Scholar] [CrossRef]
- Hagendorff, A.; Knebel, F.; Helfen, A.; Stöbe, S.; Doenst, T.; Falk, V. Disproportionate mitral regurgitation: Another myth? A critical appraisal of echocardiographic assessment of functional mitral regurgitation. Int. J. Cardiovasc. Imaging 2021, 37, 183–196. [Google Scholar] [CrossRef]
- Berrill, M.; Beeton, I.; Fluck, D.; John, I.; Lazariashvili, O.; Stewart, J.; Ashcroft, E.; Belsey, J.; Sharma, P.; Baltabaeva, A. Disproportionate Mitral Regurgitation Determines Survival in Acute Heart Failure. Front. Cardiovasc. Med. 2021, 8, 742224. [Google Scholar] [CrossRef]
- Fortuni, F.; Dietz, M.F.; Prihadi, E.A.; van der Bijl, P.; De Ferrari, G.M.; Bax, J.J.; Delgado, V.; Marsan, N.A. Ratio between vena contracta width and tricuspid annular diameter: Prognostic value in secondary tricuspid regurgitation. J. Am. Soc. Echocardiogr. 2021, 34, 944–954. [Google Scholar] [CrossRef]
- Wharton, G.; Steeds, R.; Allen, J.; Phillips, H.; Jones, R.; Kanagala, P.; Lloyd, G.; Masani, N.; Mathew, T.; Oxborough, D.; et al. A minimum dataset for a standard adult transthoracic echocardiogram: A guideline protocol from the British Society of Echocardiography. Echo Res. Pract. 2015, 2, G9–G24. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Gérard, P.L.; Piérard, L.A. Long-term outcome of patients with heart failure and dynamic functional mitral regurgitation. Eur. Heart J. 2005, 26, 1528–1532. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, P.B.; Schwammenthal, E.; Levine, R.A.; Vandervoort, P.M. Exercise dynamics in secondary mitral regurgitation: Pathophysiology and therapeutic implications. Circulation 2017, 135, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Song, J.M.; Jang, M.K.; Choi, Y.S.; Kim, Y.J.; Min, S.Y.; Kim, D.H.; Kang, D.H.; Song, J.K. The vena contracta in functional tricuspid regurgitation: A real-time three-dimensional color Doppler echocardiography study. J. Am. Soc. Echocardiogr. 2011, 24, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. –Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badano, L.P.; Muraru, D.; Enriquez-Sarano, M. Assessment of functional tricuspid regurgitation. Eur. Heart J. 2013, 34, 1875–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, A.; Oxborough, D.; Augustine, D.X.; Bedair, R.; Harkness, A.; Rana, B.; Robinson, S.; Badano, L.P. Education Committee of the British Society of Echocardiography. Echocardiographic assessment of the tricuspid and pulmonary valves: A practical guideline from the British Society of Echocardiography. Echo Res. Pract. 2020, 7, G95–G122. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Dreyfus, G.D.; Martin, R.P.; Chan, K.J.; Dulguerov, F.; Alexandrescu, C. Functional tricuspid regurgitation: A need to revise our understanding. J. Am. Coll. Cardiol. 2015, 65, 2331–2336. [Google Scholar] [CrossRef] [Green Version]
- Kovalova, S.; Necas, J.; Cerbak, R.; Malik, P.; Vespalec, J. Echocardiographic volumetry of the right ventricle. Eur. J. Echocardiogr. 2005, 6, 15–23. [Google Scholar] [CrossRef]
- Jorstig, S.; Waldenborg, M.; Liden, M.; Thunberg, P. Right ventricular ejection fraction measurements using two-dimensional transthoracic echocardiography by applying an ellipsoid model. Cardiovasc. Ultrasound 2017, 15, 4. [Google Scholar] [CrossRef] [Green Version]
- Ashcroft, E.; Lazariashvili, O.; Belsey, J.; Berrill, M.; Sharma, P.; Baltabaeva, A. Right ventricular ejection fraction as predictor of outcome in acute heart failure using RV ellipsoid model: A retrospective analysis of a prospective cross-sectional study. JRSM Cardiovasc. Dis. 2021, 10, 20480040211002775. [Google Scholar]
- Fortuni, F.; Dietz, M.F.; Prihadi, E.A.; van der Bijl, P.; De Ferrari, G.M.; Knuuti, J.; Bax, J.J.; Delgado, V.; Marsan, N.A. Prognostic implications of a novel algorithm to grade secondary tricuspid regurgitation. JACC Cardiovasc. Imaging 2021, 14, 1085–1095. [Google Scholar] [CrossRef]
- Bannehr, M.; Kucken, T.; Ulrike, K.; Haase-Fielitz, A.; Butter, C. Prognostic implications of a novel algorithm to grade secondary tricuspid regurgitation. J. Am. Soc. Echocardiogr. 2021, 34, 1316–1317. [Google Scholar] [CrossRef]
- Kebed, K.Y.; Addetia, K.; Henry, M.; Yamat, M.; Weinert, L.; Besser, S.A.; Mor-Avi, V.; Lang, R.M. Refining severe tricuspid regurgitation definition by echocardiography with a new outcomes-based "massive" grade. J. Am. Soc. Echocardiogr. 2020, 33, 1087–1094. [Google Scholar] [CrossRef]


{kind=link}
| Tricuspid Regurgitation | |||
|---|---|---|---|
| Proportionate TR (VC/TA < 0.24) n = 224 | Disproportionate TR (VC/TA ≥ 0.24) n = 132 | p Value | |
| Demographics | |||
| Age (years) | 81.0 (72.0–86.0) | 83.0 (76.0–88.0) | 0.0037 |
| BMI (Kg/m2) | 27.7 (23.2–32.0) | 26.4 (22.6–30.9) | 0.21 |
| Gender (female %) | 45.0 | 53.8 | 0.090 |
| Clinical background | |||
| Coronary artery disease (%) | 38.8 | 34.1 | 0.37 |
| Hypertension (%) | 55.4 | 57.6 | 0.68 |
| Diabetes (%) | 32.1 | 25.8 | 0.20 |
| Chronic Kidney Disease (%) | 43.3 | 52.3 | 0.10 |
| COPD (%) | 14.3 | 18.2 | 0.33 |
| Previous CVA (%) | 13.4 | 22.7 | 0.023 |
| Presenting features | |||
| eGFR (mL/m2) | 54.0 (38.5–61.0) | 48.5 (33.0–61.0) | 0.027 |
| Haemoglobin (g/L) | 122 (107–137) | 121 (108–136) | 0.85 |
| CRP (mg/L) | 14.0 (4.10–35.5) | 16.5 (7.50–36.0) | 0.20 |
| BNP (pg/L) | 901 (494–1586) | 1074 (603–2008) | 0.034 |
| Systolic BP (mmHg) | 135 (120–155) | 130 (114–150) | 0.10 |
| Diastolic BP (mmHg) | 73.0 (62.0–85.0) | 72.5 (61.8–86.3) | 0.81 |
| Sinus rhythm (%) | 40.9 | 32.3 | 0.11 |
| Atrial Fibrillation (%) | 45.0 | 53.8 | 0.11 |
| Outcome | |||
| 2-year mortality (%) | 36.5 | 47.7 | 0.032 |
| Tricuspid Regurgitation | |||
|---|---|---|---|
| Right Heart Parameters | Proportionate TR (VC/TA < 0.24 mL) | Disproportionate TR (VC/TA ≥ 0.24 mL) | p Value |
| Right atrium | n = 224 | n = 132 | |
| RA size (cm2) | 22.4 (17.6–27.6) | 25.2 (21.2–32.2) | <0.001 |
| Indexed RA size (cm2/m2) | 14.1 (11.5–18.3) | 11.6 (9.55–13.9) | <0.001 |
| Right ventricle size | |||
| RV end-diastolic (cm2) | 19.4 (16.0–24.5) | 21.8 (17.5–28.4) | 0.0027 |
| Indexed RV end-diastolic area (cm2/m2) | 10.1 (8.34–12.5) | 12.2 (9.80–15.3) | <0.001 |
| RV end-systolic area (cm2) | 11.7 (8.75–16.2) | 13.5 (10.3–18.9) | 0.0015 |
| Indexed RV end-systolic area (cm2/m2) | 6.27 (4.58–8,49) | 7.65 (5.49–10.6) | <0.001 |
| TV annulus (cm) | 3.50 (3.00–4.00) | 3.60 (3.08–4.10) | 0.55 |
| Tricuspid regurgitation | |||
| Regurgitant volume (mL) | 17.0 (8.00–32.0) | 61.0 (44.0–83.0) | <0.001 |
| ERO (cm2) | 0.20 (0.10–0.40) | 0.60 (0.40–0.80) | <0.001 |
| VC diameter (cm) | 0.50 (0.30–0.60) | 1.10 (0.90–1.32) | <0.001 |
| Right ventricle performance | |||
| RV FAC (%) | 37.9 (28.8–46.5) | 33.7 (25.6–45.0) | 0.16 |
| TAPSE (cm) | 1.50 (1.12–1.80) | 1.40 (1.10–1.80) | 0.16 |
| RV’S (cm/s) | 0.11 (0.09–0.14) | 0.10 (0.08–0.13) | 0.0023 |
| Right ventricular strain | |||
| GLS free wall (peak) (%) | −13.8 (−17.2–−10.3) | −12.8(−17.5–−9.66) | 0.23 |
| GLS free wall (end systole) (%) | −12.8 (−16.3–−9.43) | −12.2(−16.7–−8.45) | 0.50 |
| Systolic pulmonary artery pressure (mmHg) | 49.0(38.3–60.8) | 59.0(47.3–70.0) | <0.001 |
| Tricuspid Regurgitation | |||
|---|---|---|---|
| Left Heart Parameters | Proportionate TR (VC/TA < 0.24 mL) n = 224 | Disproportionate TR (VC/TA ≥ 0.24 mL) n = 132 | p Value |
| Left atrium | |||
| LA size (cm2) | 27.5 (23.2–32.8) | 29.3 (25.6–34.6) | 0.015 |
| Indexed LA size (cm2/m2) | 14.2 (11.9, 17.1) | 16.1 (13.9, 19.2) | <0.001 |
| Left ventricle volumes | |||
| LVEDV (mL) | 101 (75.0–138) | 93.0 (62.0–143) | 0.20 |
| Indexed LVEDV (mL/m2) | 53.5 (37.3–71.2) | 51.9 (36.6–73.2) | 0.65 |
| LVESV (mL) | 59.5 (35.3–87.0) | 49.0 (28.8–90.3) | 0.20 |
| Indexed LVESV (mL/m2) | 30.3 (18.3–46.0) | 27.7 (18.3–46.0) | 0.63 |
| Left ventricle performance | |||
| LV ejection fraction (%) | 43.0 (32.0–56.0) | 45.0 (33.0–56.0) | 0.63 |
| LV dP/dt (mmHg) | 928 (707–1242) | 855 (662–1218) | 0.65 |
| S’ (cm/s) | 0.07 (0.06–0.09) | 0.07 (0.06–0.10) | 0.70 |
| Left ventricular strain | |||
| GLS (%) | −9.48 (−12.4–−6.36) | −9.10 (−12.9–−5.82) | 0.69 |
| GLSR | −0.67 (−0.84–−0.48) | −0.66 (−0.91–−0.47) | 0.63 |
| >Mild Mitral Regurgitation | 36.6 | 51.5 | 0.0059 |
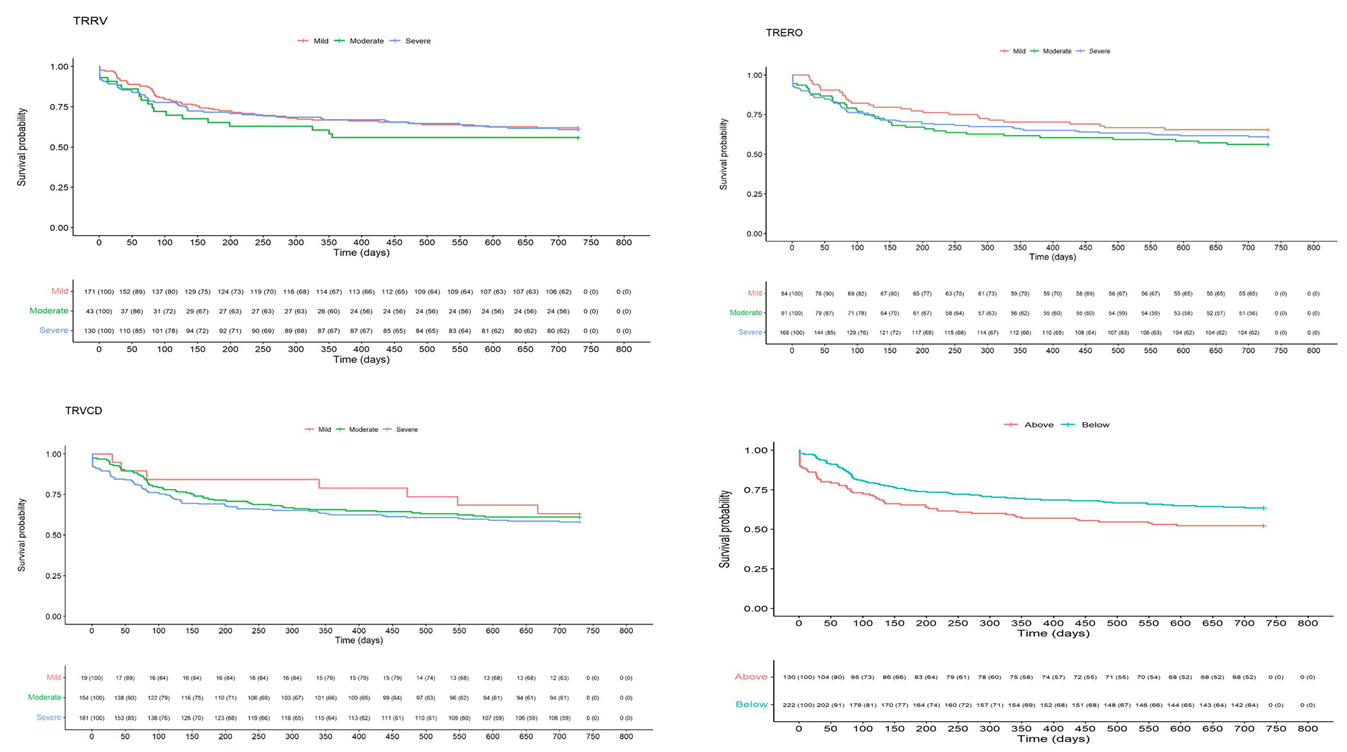
| Mild | Moderate | Severe | ||
|---|---|---|---|---|
| Regurgitant volume (TR RegVol) | Number at risk | 171 | 43 | 130 |
| Mortality n (%) | 65 (38.0) | 19 (44.2) | 51 (39.2) | |
| Hazard ratio (mild vs. moderate) [95% Cis] | 0.790 [0.458–1.364] | |||
| p-value (Logrank) | 0.400 | |||
| Hazard ratio (mild vs. severe) [95% Cis] | 0.937 [0.652–1.348] | |||
| p-value (Logrank) | 0.700 | |||
| Hazard ratio (moderate vs. severe) [95% Cis] | 1.186 [0.675–2.086] | |||
| p-value (Logrank) | 0.500 | |||
| p-value overall (Logrank) | 0.661 | |||
| Effective Regurgitant orifice (TR ERO) | Number at risk, n | 84 | 91 | 169 |
| Mortality, n (%) | 29 (34.5) | 40 (44.0) | 66 (39.1) | |
| Hazard ratio (mild vs. moderate) [95% Cis] | 0.722 [0.451–1.154] | |||
| p-value (Logrank) | 0.200 | |||
| Hazard ratio (mild vs. severe) [95% Cis] | 0.820 [0.544–1.237] | |||
| p-value (Logrank) | 0.400 | |||
| Hazard ratio (moderate vs. severe) [95% Cis] | 1.136 [0.753–1.715] | |||
| p-value (Logrank) | 0.500 | |||
| p-value overall (Logrank) | 0.404 | |||
| Vena contracta (TR VCD) | Number at risk | 19 | 154 | 181 |
| Mortality n (%) | 7 (36.8) | 60 (39.0) | 76 (42.0) | |
| Hazard ratio (mild vs. moderate) [95% Cis] | 0.872 [0.426–1.784] | |||
| p-value (Logrank) | 0.700 | |||
| Hazard ratio (mild vs. severe) [95% Cis] | 0.768 [0.377–1.564] | |||
| p-value (Logrank) | 0.500 | |||
| Hazard ratio (moderate vs. severe) [95% Cis] | 0.881 [0.628–1.236] | |||
| p-value (Logrank) | 0.500 | |||
| p-value overall (Logrank) | 0.659 | |||
| Below (VC/TA ≤ 0.24) (n = 224) | Above (VC/TA ≥ 0.24) (n = 132) | ||
|---|---|---|---|
| Disproportionate TR | Number at risk, n | 222 | 130 |
| Mortality, n (%) | 81 (36.5) | 62 (47.7) | |
| Hazard ratio (below vs. above) [95% Cis] | 1.48 [1.06–2.06] | ||
| p-value (Logrank) | 0.020 | ||
| Variable | B | SE | Wald | Exp(b) | 95% CIs | p |
|---|---|---|---|---|---|---|
| Age (n = 414) | 0.04425 | 0.01134 | 15.2307 | 1.0452 | 1.0223–1.0687 | 0.0001 |
| BMI (n = 411) | −0.003826 | 0.01326 | 0.08328 | 0.9962 | 0.9706–1.0224 | 0.7729 |
| CKD (n = 414) | 0.2744 | 0.2718 | 1.0187 | 1.3157 | 0.7723–2.2415 | 0.3128 |
| COPD (n = 414) | 0.7765 | 0.2182 | 12.6595 | 2.1738 | 1.4173–3.3342 | 0.0004 |
| Moderate + MR (n = 414) | 0.2667 | 0.1887 | 1.9975 | 1.3057 | 0.9020–1.8900 | 0.1576 |
| SPAP (n = 401) | 0.009458 | 0.004840 | 3.8187 | 1.0095 | 1.0000–1.0191 | 0.0507 |
| LVEDV (n = 411) | −0.004859 | 0.002217 | 4.8047 | 0.9952 | 0.9908–0.9995 | 0.0284 |
| Urea (n = 414) | 0.04250 | 0.02049 | 4.3023 | 1.0434 | 1.0023–1.0862 | 0.0381 |
| Sodium (n = 414) | −0.02667 | 0.01586 | 2.8291 | 0.9737 | 0.9439–1.0044 | 0.0926 |
| BNP (n = 414) | 0.0002427 | 0.00006974 | 12.1076 | 1.0002 | 1.0001–1.0004 | 0.0005 |
| Hb (n = 414) | −0.0004978 | 0.004365 | 0.01301 | 0.9995 | 0.9910–1.0081 | 0.9092 |
| eGFR (n = 413) | 0.001103 | 0.01188 | 0.008629 | 1.0011 | 0.9781–1.0247 | 0.9260 |
| Disproportionate TR (n = 352) | −0.01264 | 0.1842 | 0.004707 | 0.9874 | 0.6882–1.4168 | 0.9453 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berrill, M.; Ashcroft, E.; Fluck, D.; John, I.; Beeton, I.; Sharma, P.; Baltabaeva, A. Tricuspid Regurgitation in Acute Heart Failure: Predicting Outcome Using Novel Quantitative Echocardiography Techniques. Diagnostics 2023, 13, 109. https://doi.org/10.3390/diagnostics13010109
Berrill M, Ashcroft E, Fluck D, John I, Beeton I, Sharma P, Baltabaeva A. Tricuspid Regurgitation in Acute Heart Failure: Predicting Outcome Using Novel Quantitative Echocardiography Techniques. Diagnostics. 2023; 13(1):109. https://doi.org/10.3390/diagnostics13010109
Chicago/Turabian StyleBerrill, Max, Eshan Ashcroft, David Fluck, Isaac John, Ian Beeton, Pankaj Sharma, and Aigul Baltabaeva. 2023. "Tricuspid Regurgitation in Acute Heart Failure: Predicting Outcome Using Novel Quantitative Echocardiography Techniques" Diagnostics 13, no. 1: 109. https://doi.org/10.3390/diagnostics13010109