

Primary Tumor Radiomic Model for Identifying Extrahepatic Metastasis of Hepatocellular Carcinoma Based on Contrast Enhanced Computed Tomography
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics and Imaging Criteria
2.2. Training and Test Sets
2.3. Image Acquisition
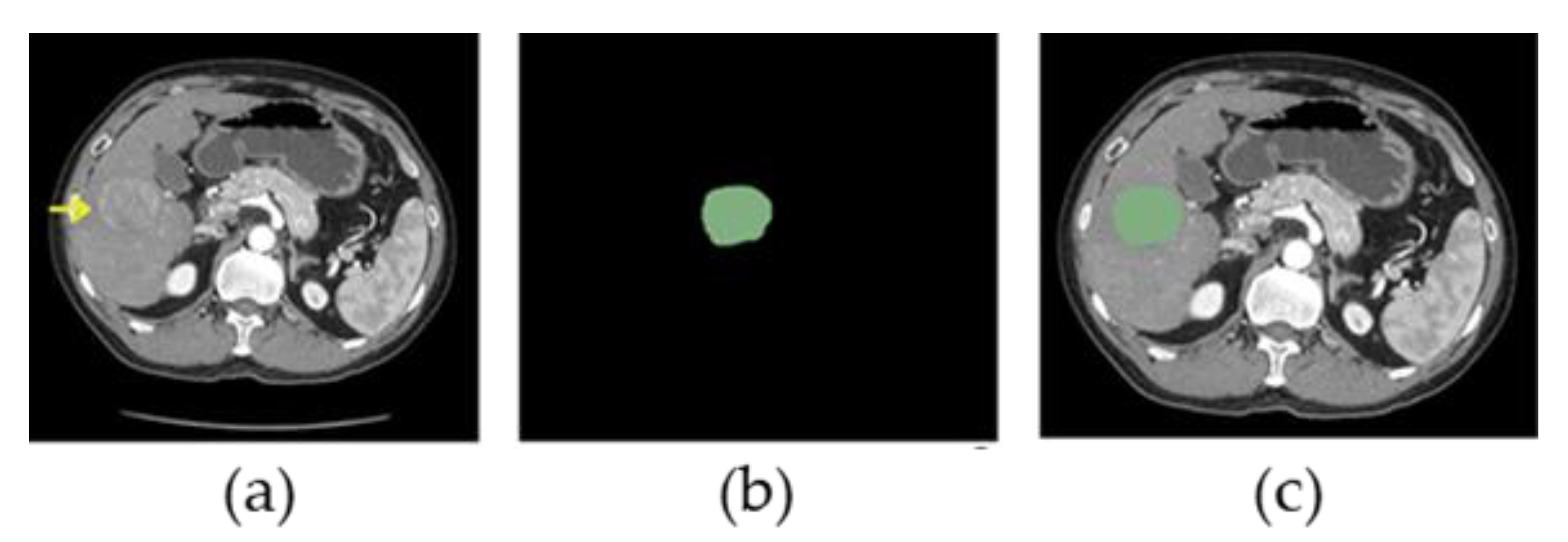
2.4. Segmentation of HCC
2.5. Feature Extraction
2.6. Data Refinement
2.7. Model Building and Statistical Analysis
3. Results
3.1. Patient Characteristics
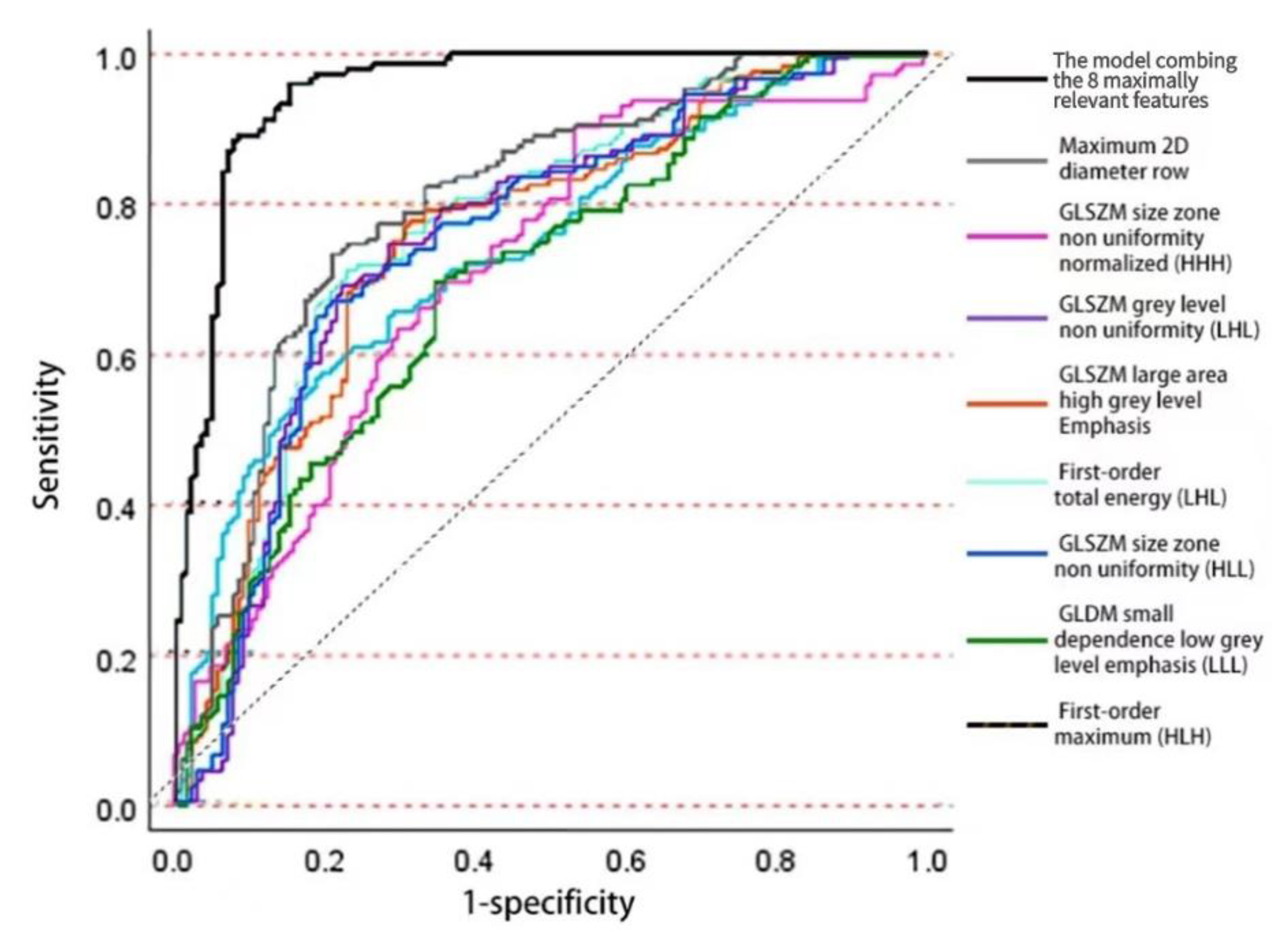
3.2. Training of Logistic Regression Model
- maximum 2D diameter row (b1 = 2.371, p = 3.249 × 10−8),
- first-order total energy with wavelet LHL (b2 = 2.006, p = 0.067),
- first-order maximum with wavelet HLH (b3 = 0.476, p = 0.119),
- GLSZM size zone nonuniformity normalized with wavelet HHH (b4 = 0.986, p = 4.341 × 10−6),
- GLSZM grey level nonuniformity with wavelet LHL (b5 = −2.148, p = 0.050),
- GLSZM large area high grey level Emphasis in original image (b6 = 1.732, p = 0.024),
- GLSZM size zone nonuniformity with wavelet HLL (b7 = −2.001, p = 0.177), and
- GLDM small dependence low grey level emphasis with wavelet LLL (b8 = 1.439, p = 4.018 × 10−3).
3.3. Training of Deep Learning Model
3.4. Training of SVM Model
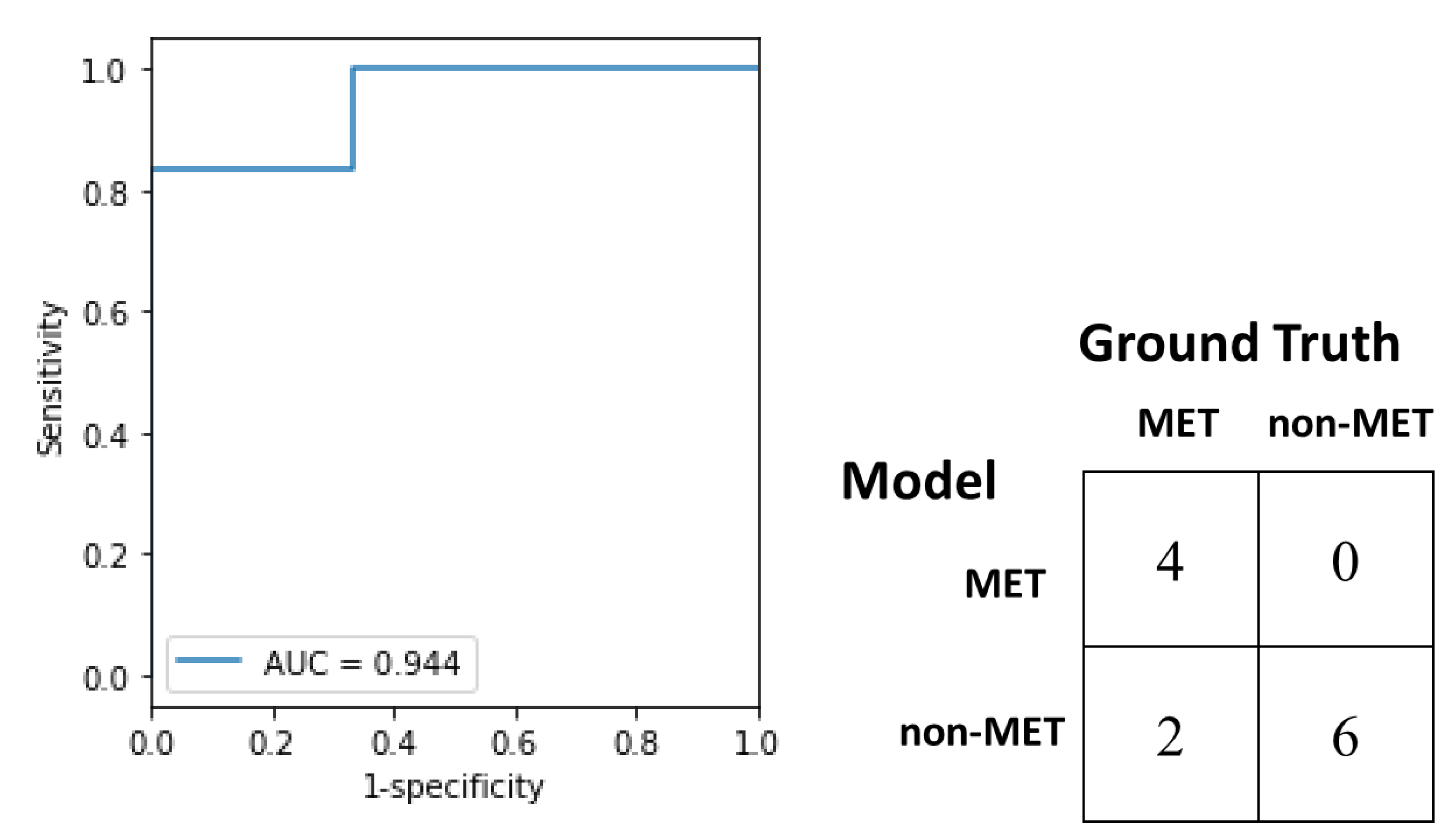
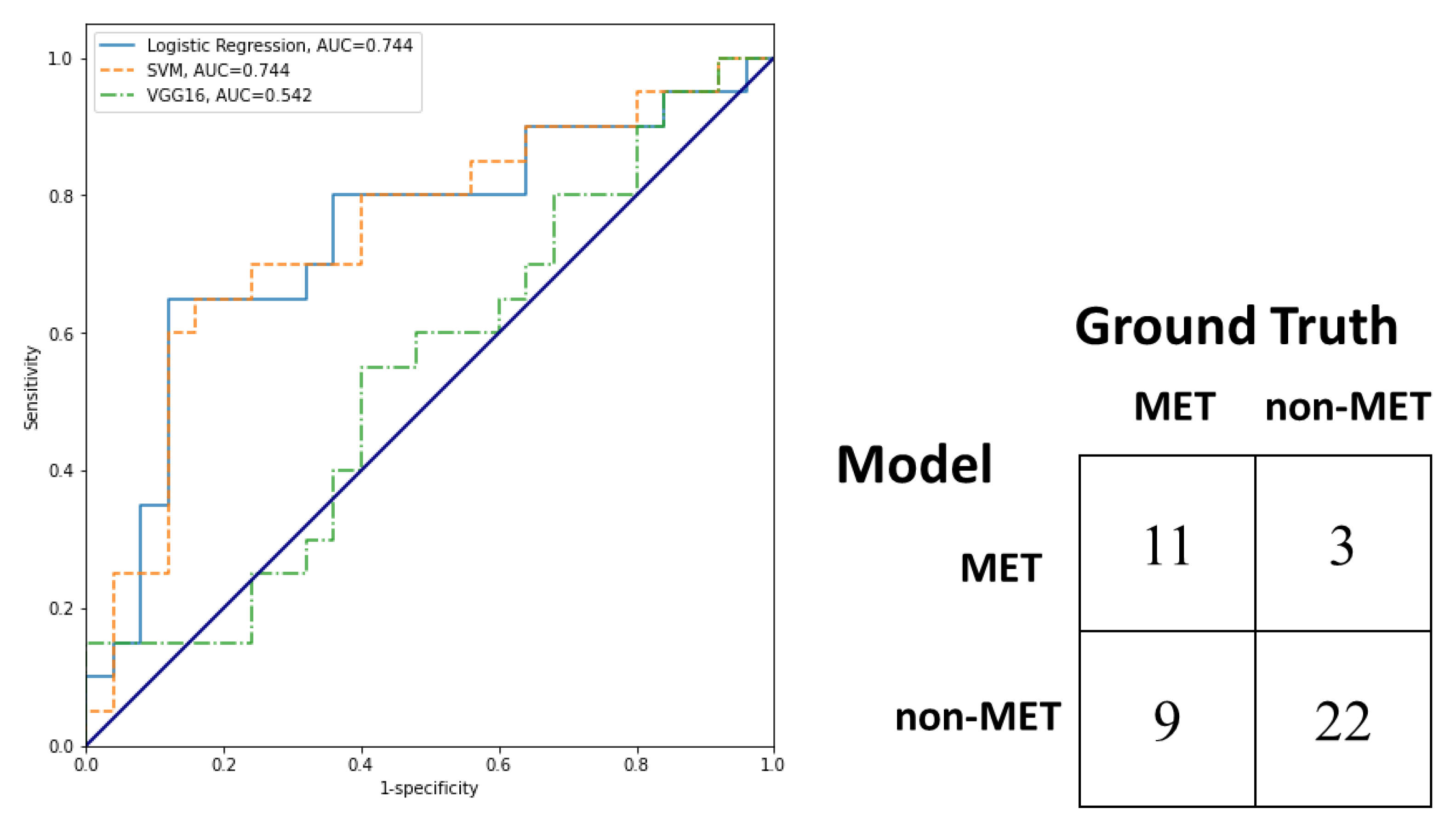
3.5. Test and External Validation of Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shape | Elongation |
| (14 features) | Flatness |
| Least axis length | |
| Major axis length | |
| Maximum 2D diameter column | |
| Maximum 2D diameter row | |
| Maximum 2D diameter slice | |
| Maximum 3D diameter | |
| Mesh volume | |
| Minor axis length | |
| Sphericity | |
| Surface area | |
| Surface volume ratio | |
| Voxel volume |
| First order | 10 percentiles |
| (18 features) | 90 percentiles |
| Energy | |
| Entropy | |
| Interquartile range | |
| Kurtosis | |
| Maximum | |
| Mean absolute deviation | |
| Mean | |
| Median | |
| Minimum | |
| Range | |
| Robust mean absolute deviation | |
| Root mean squared | |
| Skewness | |
| Total energy | |
| Uniformity | |
| Variance | |
| GLCM | Autocorrelation |
| (24 features) | Cluster prominence |
| Cluster shade | |
| Cluster tendency | |
| Contrast | |
| Correlation | |
| Difference average | |
| Difference entropy | |
| Difference variance | |
| Inverse difference | |
| Inverse difference moment | |
| Inverse difference moment normalised | |
| Inverse difference normalised | |
| Informational measure of correlation 1 | |
| Informational measure of correlation 2 | |
| Inverse variance | |
| Joint average | |
| Joint energy | |
| Joint entropy | |
| Maximal correlation coefficient | |
| Maximum probability | |
| Sum average | |
| Sum entropy | |
| Sum squares | |
| GLDM | Dependence entropy |
| (14 features) | Dependence nonuniformity |
| Dependence nonuniformity normalised | |
| Dependence variance | |
| Grey level nonuniformity | |
| Grey level variance | |
| High grey level emphasis | |
| Large dependence emphasis | |
| Large dependence high grey level emphasis | |
| Large dependence low grey level emphasis | |
| Low grey level emphasis | |
| Small dependence emphasis | |
| Small dependence high grey level emphasis | |
| Small dependence low grey level emphasis | |
| GLRLM | Grey level nonuniformity |
| (16 features) | Grey level nonuniformity normalised |
| Grey level variance | |
| High grey level run emphasis | |
| Long run emphasis | |
| Long run high grey level emphasis | |
| Long run low grey level emphasis | |
| Low grey level emphasis | |
| Run entropy | |
| Run length nonuniformity | |
| Run length nonuniformity normalised | |
| Run percentage | |
| Run variance | |
| Short run emphasis | |
| Short run high grey level emphasis | |
| Short run low grey level emphasis | |
| GLSZM | Grey level nonuniformity |
| (16 features) | Grey level nonuniformity normalised |
| Grey level variance | |
| High grey zone emphasis | |
| Large area emphasis | |
| Large area high grey level emphasis | |
| Large area low grey level emphasis | |
| Low grey level zone emphasis | |
| Size zone nonuniformity | |
| Size zone nonuniformity normalised | |
| Small area emphasis | |
| Small area high grey level emphasis | |
| Small area low grey level emphasis | |
| Zone entropy | |
| Zone percentage | |
| Zone variance | |
| NGTDM | Busyness |
| (5 features) | Coarseness |
| Complexity | |
| Contrast | |
| Strength |
References
- American Cancer Society. Global Cancer Facts & Figures, 4th ed.; American Cancer Society: Atlanta, GA, USA, 2018; pp. 22–24. [Google Scholar]
- Gomaa, A.I.; Khan, S.A.; Toledano, M.B.; Waked, I.; Taylor-Robinson, S.D. Hepatocellular carcinoma: Epidemiology, risk factors and pathogenesis. World J. Gastroenterol. WJG 2008, 14, 4300–4308. [Google Scholar] [CrossRef] [PubMed]
- Sacco, R.; Bargellini, I.; Ginanni, B.; Bertini, M.; Faggioni, L.; Federici, G.; Romano, A.; Bertoni, M.; Metrangolo, S.; Altomare, E.; et al. Long-term results of sorafenib in advanced-stage hepatocellular carcinoma: What can we learn from routine clinical practice? Expert Rev. Anticancer Ther. 2012, 12, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gao, Z.H.; Qu, X.J. The adverse effects of sorafenib in patients with advanced cancers. Basic Clin. Pharmacol. Toxicol. 2015, 116, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Uchino, K.; Tateishi, R.; Shiina, S.; Kanda, M.; Masuzaki, R.; Kondo, Y.; Goto, T.; Omata, M.; Yoshida, H.; Koike, K. Hepatocellular carcinoma with extrahepatic metastasis: Clinical features and prognostic factors. Cancer 2011, 117, 4475–4483. [Google Scholar] [CrossRef] [PubMed]
- Natsuizaka, M.; Omura, T.; Akaike, T.; Kuwata, Y.; Yamazaki, K.; Sato, T.; Karino, Y.; Toyota, J.; Suga, T.; Asaka, M. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J. Gastroenterol. Hepatol. 2005, 20, 1781–1787. [Google Scholar] [CrossRef]
- Cheung, T.T.; Ho, C.L.; Lo, C.M.; Chen, S.; Chan, S.C.; Chok, K.S.; Fung, J.Y.; Yan Chan, A.C.; Sharr, W.; Yau, T.; et al. 11C-acetate and 18F-FDG PET/CT for clinical staging and selection of patients with hepatocellular carcinoma for liver transplantation on the basis of Milan criteria: Surgeon’s perspective. J. Nucl. Med. 2013, 54, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Yokoo, T.; Patel, A.D.; Lev-Cohain, N.; Singal, A.G.; Yopp, A.C.; Pedrosa, I. Extrahepatic metastasis risk of hepatocellular carcinoma based on α-fetoprotein and tumor staging parameters at cross-sectional imaging. Cancer Manag. Res. 2017, 9, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Xiao, S.; Chang, R.M.; Yang, M.Y.; Lei, X.; Liu, X.; Gao, W.B.; Xiao, J.L.; Yang, L.Y. Actin-like 6A predicts poor prognosis of hepatocellular carcinoma and promotes metastasis and epithelial-mesenchymal transition. Hepatology 2016, 63, 1256–1271. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Z.L.; Zeng, Z.C.; Tang, Z.Y.; Fan, J.; Sun, H.C.; Tan, Y.S. Expression of Cytokeratin 19 and Matrix Metalloproteinase 2 predicts lymph node metastasis in hepatocellular carcinoma. Mol. Biol. Rep. 2011, 38, 3531–3539. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Grove, O.; Gillies, R.J. Quantitative imaging in cancer evolution and ecology. Radiology 2013, 269, 8–15. [Google Scholar] [CrossRef]
- Kiryu, S.; Akai, H.; Nojima, M.; Hasegawa, K.; Shinkawa, H.; Kokudo, N.; Yasaka, K.; Ohtomo, K. Impact of hepatocellular carcinoma heterogeneity on computed tomography as a prognostic indicator. Sci. Rep. 2017, 7, 12689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Chakraborty, J.; Chapman, W.C.; Gerst, S.; Gonen, M.; Pak, L.M.; Jarnagin, W.R.; DeMatteo, R.P.; Do, R.K.; Simpson, A.L.; et al. Preoperative prediction of microvascular invasion in hepatocellular carcinoma using quantitative image analysis. J. Am. Coll. Surg. 2017, 225, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Choi, S.J.; Lee, S.H.; Lee, H.Y.; Park, H. Predicting survival using pretreatment CT for patients with hepatocellular carcinoma treated with transarterial chemoembolization: Comparison of models using radiomics. AJR Am. J. Roentgenol. 2018, 211, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; He, L.; Huang, Y.; Chen, S.; Wu, P.; Ye, W.; Liu, Z.; Liang, C. CT-based radiomics signature: A potential biomarker for preoperative prediction of early recurrence in hepatocellular carcinoma. Abdom. Radiol. 2017, 42, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Miranda Magalhaes Santos, J.M.; Clemente Oliveira, B.; Araujo-Filho, J.D.; Assuncao, A.N., Jr.; de MMachado, F.A.; Carlos Tavares Rocha, C.; Horvat, J.V.; Menezes, M.R.; Horvat, N. State-of-the-art in radiomics of hepatocellular carcinoma: A review of basic principles, applications, and limitations. Abdom. Radiol. 2020, 45, 342–353. [Google Scholar] [CrossRef]
- Limkin, E.J.; Sun, R.; Dercle, L.; Zacharaki, E.I.; Robert, C.; Reuzé, S.; Schernberg, A.; Paragios, N.; Deutsch, E.; Ferté, C. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Ann. Oncol. 2017, 28, 1191–1206. [Google Scholar] [CrossRef]
- Schraml, C.; Kaufmann, S.; Rempp, H.; Syha, R.; Ketelsen, D.; Notohamiprodjo, M.; Nikolaou, K. Imaging of HCC-current state of the art. Diagnostics 2015, 5, 513–545. [Google Scholar] [CrossRef] [Green Version]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, 104–107. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.W.; Wong, S.C.; Chiau, C.C.; Chan, T.M.; Tao, L.; Feng, J.; Chiu, K.W. Association patterns of ontological features signify electronic health records in liver cancer. J. Healthc. Eng. 2017, 2017, 6493016. [Google Scholar] [CrossRef] [Green Version]
- McCaw, Z.R.; Lane, J.M.; Saxena, R.; Redline, S.; Lin, X. Operating characteristics of the rank-based inverse normal transformation for quantitative trait analysis in genome-wide association studies. Biometrics 2020, 76, 1262–1272. [Google Scholar] [CrossRef]
- Blagus, R.; Lusa, L. SMOTE for high-dimensional class-imbalanced data. BMC Bioinform. 2013, 14, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Y.; Yuan, M.; Zhang, T.; Zhang, Y.D.; Li, H.; Yu, T.F. Radiomics approach to prediction of occult mediastinal lymph node metastasis of lung adenocarcinoma. Am. J. Roentgenol. 2018, 211, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokareva, A.O.; Chagovets, V.V.; Kononikhin, A.S.; Starodubtseva, N.L.; Nikolaev, E.N.; Frankevich, V.E. Comparison of the effectiveness of variable selection method for creating a diagnostic panel of biomarkers for mass spectrometric lipidome analysis. J. Mass Spectrom. 2021, 56, 4702. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Model-building strategies and methods for logistic regression. In Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 89–151. [Google Scholar]
- Babyak, M.A. What you see may not be what you get: A brief, nontechnical introduction to overfitting in regression-type model. Psychosom. Med. 2004, 66, 411–421. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the International Conference on Learning Representations, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Wakabayashi, T.; Ouhmich, F.; Gonzalez-Cabrera, C.; Felli, E.; Saviano, A.; Agnus, V.; Savadjiev, P.; Baumert, T.F.; Pessaux, P.; Marescaux, J.; et al. Radiomics in hepatocellular carcinoma: A quantitative review. Hepatol. Int. 2019, 13, 546–559. [Google Scholar] [CrossRef] [Green Version]
- Thibault, G.; Fertil, B.; Navarro, C.; Pereira, S.; Cau, P.; Levy, N.; Sequeira, J.; Mari, J.L. Shape and texture indexes application to cell nuclei classification. Int. J. Pattern Recognit. Artif. Intell. 2013, 27, 1357002. [Google Scholar] [CrossRef]
- Ganeshan, B.; Panayiotou, E.; Burnand, K.; Dizdarevic, S.; Miles, K. Tumour heterogeneity in non-small cell lung carcinoma assessed by CT texture analysis: A potential marker of survival. Eur. Radiol. 2012, 22, 796–802. [Google Scholar] [CrossRef]
- Rios, E.; Parmar, C.; Jermoumi, M.; Aerts, H. Robust radiomics feature quantification using semiautomatic volumetric segmentation. Med. Phys. 2014, 41, 452. [Google Scholar] [CrossRef]
- Yu, H.; Meng, X.; Chen, H.; Liu, J.; Gao, W.; Du, L.; Chen, Y.; Wang, Y.; Liu, X.; Liu, B.; et al. Predicting the level of tumor-infiltrating lymphocytes in patients with breast cancer: Usefulness of mammographic radiomics features. Front. Oncol. 2021, 11, 393. [Google Scholar] [CrossRef]
- Mao, B.; Zhang, L.; Ning, P.; Ding, F.; Wu, F.; Lu, G.; Geng, Y.; Ma, J. Preoperative prediction for pathological grade of hepatocellular carcinoma via machine learning-based radiomics. Eur. Radiol. 2020, 30, 6924–6932. [Google Scholar] [CrossRef] [PubMed]
- Prezzi, D.; Owczarczyk, K.; Bassett, P.; Siddique, M.; Breen, D.J.; Cook, G.J.; Goh, V. Adaptive statistical iterative reconstruction (ASIR) affects CT radiomics quantification in primary colorectal cancer. Eur. Radiol. 2019, 29, 5227–5235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Zhang, J.; Zhang, Q.F.; Xu, Y.K.; Zhou, J.; Liu, L. A radiomics nomogram for preoperative prediction of microvascular invasion risk in hepatitis B virus-related hepatocellular carcinoma. Diagn. Interv. Radiol. 2018, 24, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, G.W.; Zhu, F.P.; Xu, Q.; Wang, K.; Wu, M.Y.; Tang, W.W.; Li, X.C.; Wang, X.H. Machine-learning analysis of contrast-enhanced CT radiomics predicts recurrence of hepatocellular carcinoma after resection: A multi-institutional study. EBioMedicine 2019, 50, 156–165. [Google Scholar] [CrossRef] [Green Version]
- Shan, Q.Y.; Hu, H.T.; Feng, S.T.; Peng, Z.P.; Chen, S.L.; Zhou, Q.; Li, X.; Xie, X.Y.; Lu, M.D.; Wang, W.; et al. CT-based peritumoral radiomics signatures to predict early recurrence in hepatocellular carcinoma after curative tumour resection or ablation. Cancer Imaging 2019, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Coppola, F.; Giannini, V.; Gabelloni, M.; Panic, J.; Defeudis, A.; Lo Monaco, S.; Cattabriga, A.; Cocozza, M.A.; Pastore, L.V.; Polici, M.; et al. Radiomics and Magnetic Resonance Imaging of Rectal Cancer: From Engineering to Clinical Practice. Diagnostics 2021, 11, 756. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, J.H.; Choi, S.Y.; Lee, E.S.; Park, S.J.; Byun, J.Y.; Choi, B.I. Prediction of therapeutic response of hepatocellular carcinoma to transcatheter arterial chemoembolization based on pretherapeutic dynamic CT and textural findings. Am. J. Roentgenol. 2017, 209, 211–220. [Google Scholar] [CrossRef]





| Characteristics | Training Cohort (n = 165) | Test Set (n = 12) | p1 |
|---|---|---|---|
| Mean age | 63.4 | 63.8 | 0.894 |
| Sex | 0.758 | ||
| Male | 130 | 9 | |
| Female | 35 | 3 | |
| Hepatitis B | 79 | 5 | 0.677 |
| Liver cirrhosis | 79 | 6 | 0.887 |
| Mean tumor diameter (largest lesion, cm) | 5.44 | 6.94 | 0.380 |
| Mean number of HCC lesions | 2.44 | 3.83 | 0.204 |
| Portal invasion | 35 | 3 | 0.758 |
| Protocol Item | Parameter |
|---|---|
| Scan parameters | |
| Peak kilo voltage output | 120 kV |
| X-ray tube current | 700 mA |
| Contrast medium injection parameters | |
| Contrast agent | Iopamidol/Iohexol |
| Concentration | 350–370 mg/mL |
| Volume | 100–120 mL |
| Flow rate | 3–5 mL/s |
| Characteristics | No Metastasis (n = 151) | Metastasis (n = 26) | p 1 |
|---|---|---|---|
| Mean age | 63.7 | 61.6 | 0.353 |
| Sex | 0.413 | ||
| Male | 117 | 22 | |
| Female | 34 | 4 | |
| Hepatitis B | 73 | 11 | 0.569 |
| Liver cirrhosis | 76 | 9 | 0.138 |
| Mean tumor diameter (largest lesion, cm) | 5.10 | 8.06 | 0.007 * |
| Mean number of HCC lesions | 2.13 | 4.80 | 0.011 * |
| Portal invasion | 29 | 9 | 0.077 |
| Performance | Logistic | SVM | VGG16 | Logit vs. SVM | Logit vs. VGG16 |
|---|---|---|---|---|---|
| Accuracy | 0.733 | 0.666 | 0.533 | p = 0.223 | p = 0.066 |
| Sensitivity | 0.55 | 0.40 | 0.50 | p = 0.083 | p = 0.763 |
| Specificity | 0.88 | 0.88 | 0.56 | p = 1.000 | p = 0.021 |
| Balanced accuracy | 0.715 | 0.640 | 0.544 | ||
| F1 | 0.647 | 0.516 | 0.539 | ||
| MCC | 0.462 | 0.324 | 0.089 | ||
| AUC | 0.744 | 0.744 | 0.542 | p = 0.905 | p = 0.044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, L.W.C.; Wong, S.C.C.; Cho, W.C.S.; Huang, M.; Zhang, F.; Chui, M.L.; Lai, U.N.Y.; Chan, T.Y.K.; Cheung, Z.H.C.; Cheung, J.C.Y.; et al. Primary Tumor Radiomic Model for Identifying Extrahepatic Metastasis of Hepatocellular Carcinoma Based on Contrast Enhanced Computed Tomography. Diagnostics 2023, 13, 102. https://doi.org/10.3390/diagnostics13010102
Chan LWC, Wong SCC, Cho WCS, Huang M, Zhang F, Chui ML, Lai UNY, Chan TYK, Cheung ZHC, Cheung JCY, et al. Primary Tumor Radiomic Model for Identifying Extrahepatic Metastasis of Hepatocellular Carcinoma Based on Contrast Enhanced Computed Tomography. Diagnostics. 2023; 13(1):102. https://doi.org/10.3390/diagnostics13010102
Chicago/Turabian StyleChan, Lawrence Wing Chi, Sze Chuen Cesar Wong, William Chi Shing Cho, Mohan Huang, Fei Zhang, Man Lik Chui, Una Ngo Yin Lai, Tiffany Yuen Kwan Chan, Zoe Hoi Ching Cheung, Jerry Chun Yin Cheung, and et al. 2023. "Primary Tumor Radiomic Model for Identifying Extrahepatic Metastasis of Hepatocellular Carcinoma Based on Contrast Enhanced Computed Tomography" Diagnostics 13, no. 1: 102. https://doi.org/10.3390/diagnostics13010102