
The Balance between the Left and Right Ventricular Deformation Evaluated by Speckle Tracking Echocardiography Is a Great Predictor of the Major Adverse Cardiac Event in Patients with Pulmonary Hypertension

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Echocardiography
2.3. 6MWD and Borg Dyspnea Scale
2.4. Follow-Up Assessment
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
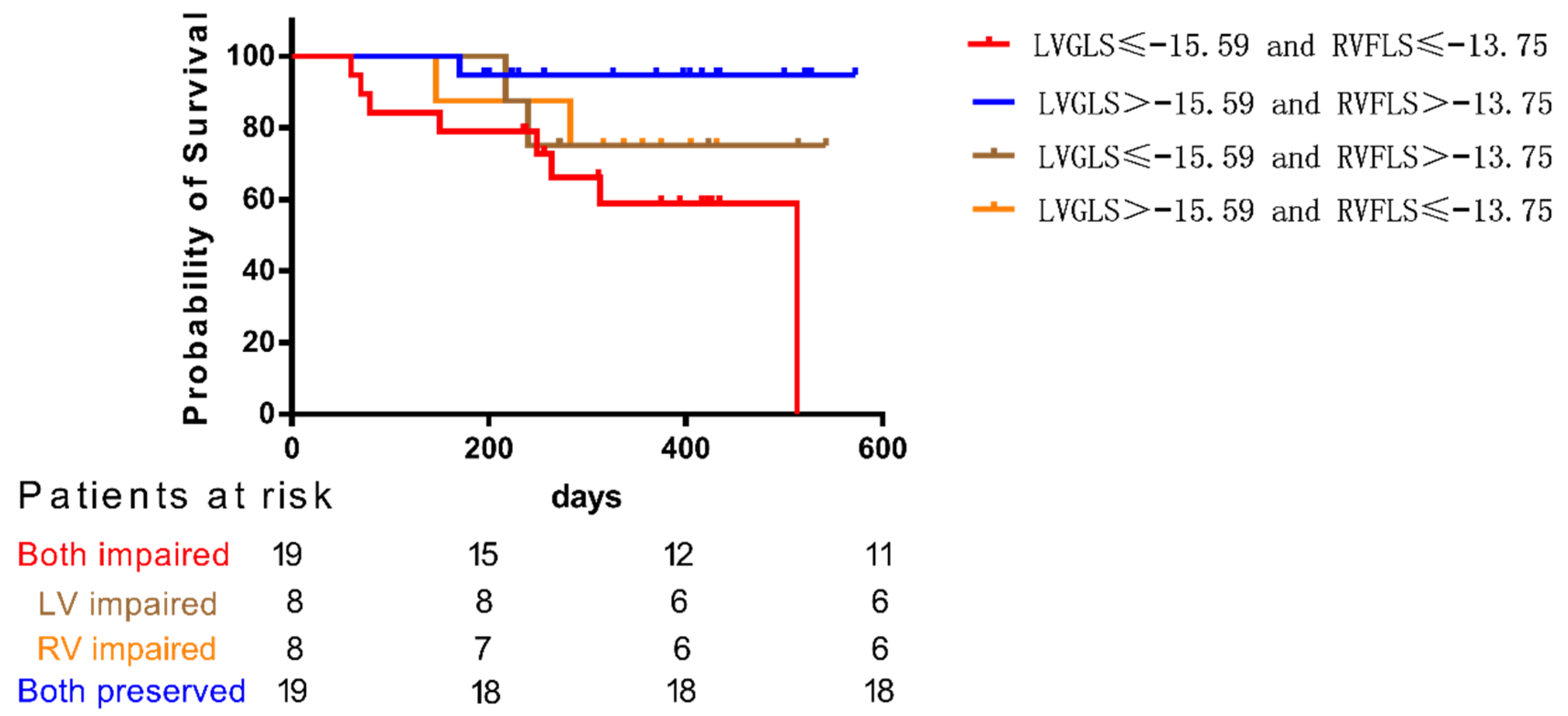
3.2. Prediction of MACE-Free Survival by LVGLS and RVFLS
3.3. Balance between Left and Right Atrial and Ventricular Longitudinal Deformations in PH Patients
3.4. Correlation between |LVGLS/RVFLS-1| and Clinical Measurements or Echocardiography-Derived Parameters
3.5. Prediction of Ominous Prognosis
4. Discussion
4.1. Significance of Baseline Parameters
4.2. Biventricular Balance
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bogaard, H.J.; Abe, K.; Vonk Noordegraaf, A.; Voelkel, N.F. The Right Ventricle under Pressure: Cellular and Molecular Mechanisms of Right-Heart Failure in Pulmonary Hypertension. Chest 2009, 135, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.; Sanchez-Quintana, D.; Bossone, E.; Bogaard, H.J.; Naeije, R. Anatomy, Function, and Dysfunction of the Right Ventricle: Jacc State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1463–1482. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.M.; Kim, N.H.; Rubin, L.J. The Right Ventricle in Pulmonary Hypertension. Coron. Artery Dis. 2005, 16, 13–18. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e578–e622. [Google Scholar] [CrossRef]
- Rosenkranz, S.; Howard, L.S.; Gomberg-Maitland, M.; Hoeper, M.M. Systemic Consequences of Pulmonary Hypertension and Right-Sided Heart Failure. Circulation 2020, 141, 678–693. [Google Scholar] [CrossRef]
- Longobardo, L.; Suma, V.; Jain, R.; Carerj, S.; Zito, C.; Zwicke, D.L.; Khandheria, B.K. Role of Two-Dimensional Speckle-Tracking Echocardiography Strain in the Assessment of Right Ventricular Systolic Function and Comparison with Conventional Parameters. J. Am. Soc. Echocardiogr. 2017, 30, 937–946.e6. [Google Scholar] [CrossRef] [PubMed]
- Shukla, M.; Park, J.-H.; Thomas, J.D.; Delgado, V.; Bax, J.J.; Kane, G.C.; Howlett, J.G.; White, J.A.; Fine, N.M. Prognostic Value of Right Ventricular Strain Using Speckle-Tracking Echocardiography in Pulmonary Hypertension: A systematic Review and Meta-Analysis. Can. J. Cardiol. 2018, 34, 1069–1078. [Google Scholar] [CrossRef] [PubMed]
- Todaro, M.C.; Carerj, S.; Zito, C.; Trifiro, M.P.; Consolo, G.; Khandheria, B. Echocardiographic Evaluation of Right Ventricular-Arterial Coupling in Pulmonary Hypertension. Am. J. Cardiovasc. Dis. 2020, 10, 272–283. [Google Scholar]
- Bemis, C.E.; Serur, J.R.; Borkenhagen, D.; Sonnenblick, E.H.; Urschel, C.W. Influence of Right Ventricular Filling Pressure on Left Ventricular Pressure and Dimension. Circ. Res. 1974, 34, 498–504. [Google Scholar] [CrossRef]
- Kasner, M.; Westermann, D.; Steendijk, P.; Drose, S.; Poller, W.; Schultheiss, H.P.; Tschope, C. Left Ventricular Dysfunction Induced by Nonsevere Idiopathic Pulmonary Arterial Hypertension: A Pressure-Volume Relationship Study. Am. J. Respir. Crit. Care Med. 2012, 186, 181–189. [Google Scholar] [CrossRef]
- Hardziyenka, M.; Campian, M.E.; Reesink, H.J.; Surie, S.; Bouma, B.J.; Groenink, M.; Klemens, C.A.; Beekman, L.; Remme, C.A.; Bresser, P.; et al. Right Ventricular Failure Following Chronic Pressure Overload Is Associated with Reduction in Left Ventricular Mass: Evidence for Atrophic Remodeling. J. Am. Coll. Cardiol. 2011, 57, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manders, E.; Bogaard, H.J.; Handoko, M.L.; Van De Veerdonk, M.C.; Keogh, A.; Westerhof, N.; Stienen, G.J.; Dos Remedios, C.G.; Humbert, M.; Dorfmüller, P.; et al. Contractile Dysfunction of Left Ventricular Cardiomyocytes in Patients with Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2014, 64, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Bosch, L.; Lam, C.S.; Gong, L.; Chan, S.P.; Sim, D.; Yeo, D.; Jaufeerally, F.; Leong, K.T.; Ong, H.Y.; Ng, T.P.; et al. Right Ventricular Dysfunction in Left-Sided Heart Failure with Preserved Versus Reduced Ejection Fraction. Eur. J. Heart Fail. 2017, 19, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship between the Right Ventricle and Its Load in Pulmonary Hypertension. J. Am. Coll. Cardiol. 2017, 69, 236–243. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography Endorsed by the European Association of Echocardiography, a Registered Branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713; quiz 786–788. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Kado, Y.; Obokata, M.; Nagata, Y.; Ishizu, T.; Addetia, K.; Aonuma, K.; Kurabayashi, M.; Lang, R.M.; Takeuchi, M.; Otsuji, Y. Cumulative Burden of Myocardial Dysfunction in Cardiac Amyloidosis Assessed Using Four-Chamber Cardiac Strain. J. Am. Soc. Echocardiogr. 2016, 29, 1092–1099.e2. [Google Scholar] [CrossRef]
- Horvath, I.T. Introduction: Sustainable Chemistry. Chem. Rev. 2018, 118, 369–371. [Google Scholar] [CrossRef]
- Sudano, I. The Yin and Yang of Light: A Cardiovascular Point of View. Eur. J. Prev. Cardiol. 2018, 25, 1873–1874. [Google Scholar] [CrossRef]
- Meng, X.; Li, Y.; Li, H.; Wang, Y.; Zhu, W.; Lu, X. Right Atrial Function in Patients with Pulmonary Hypertension: A Study with Two-Dimensional Speckle-Tracking Echocardiography. Int. J. Cardiol. 2018, 255, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Guo, S.L.; Wu, W.F.; Wang, Q.; Su, H.Y.; Tan, Z.; Wang, F.; He, Q.Y. Right Atrial Evaluation in Patients with Pulmonary Hypertension: A Real-Time 3-Dimensional Transthoracic Echocardiographic Study. J. Ultrasound. Med. 2016, 35, 49–61. [Google Scholar] [CrossRef]
- Lahm, T.; Douglas, I.S.; Archer, S.L.; Bogaard, H.J.; Chesler, N.C.; Haddad, F.; Hemnes, A.R.; Kawut, S.M.; Kline, J.A.; Kolb, T.M.; et al. Assessment of Right Ventricular Function in the Research Setting: Knowledge Gaps and Pathways Forward. An Official American Thoracic Society Research Statement. Am. J. Respir. Crit. Care Med. 2018, 198, e15–e43. [Google Scholar] [CrossRef] [PubMed]
- Kerckhoffs, R.C.; Omens, J.H.; McCulloch, A.D. Mechanical Discoordination Increases Continuously after the Onset of Left Bundle Branch Block Despite Constant Electrical Dyssynchrony in a Computational Model of Cardiac Electromechanics and Growth. Europace 2012, 14 (Suppl. S5), v65–v72. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; DuPree, J.; Lees, H.A.; Giovannini, S.; Seo, D.O.; Buford, T.W.; Sweet, K.; Morgan, D.; Strehler, K.Y.; et al. Late-Life Enalapril Administration Induces Nitric Oxide-Dependent and Independent Metabolic Adaptations in the Rat Skeletal Muscle. Age 2013, 35, 1061–1075. [Google Scholar] [CrossRef]
- Sato, T.; Tsujino, I.; Ohira, H.; Oyama-Manabe, N.; Ito, Y.M.; Yamada, A.; Ikeda, D.; Watanabe, T.; Nishimura, M. Right Atrial Volume and Reservoir Function Are Novel Independent Predictors of Clinical Worsening in Patients with Pulmonary Hypertension. J. Heart Lung. Transplant. 2015, 34, 414–423. [Google Scholar] [CrossRef]
- Vonk-Noordegraaf, A. The Shrinking Heart in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2010, 362, 267–268. [Google Scholar] [CrossRef]
- Goransson, C.; Vejlstrup, N.; Carlsen, J. Reproducibility of Peak Filling and Peak Emptying Rate Determined by Cardiovascular Magnetic Resonance Imaging for Assessment of Biventricular Systolic and Diastolic Dysfunction in Patients with Pulmonary Arterial Hypertension. Int. J. Cardiovasc. Imaging 2018, 34, 777–786. [Google Scholar] [CrossRef]
- Zimmer, A.; Teixeira, R.B.; Bonetto, J.H.; Bahr, A.C.; Türck, P.; de Castro, A.L.; Campos-Carraro, C.; Visioli, F.; Fernandes-Piedras, T.R.; Casali, K.R.; et al. Role of Inflammation, Oxidative Stress, and Autonomic Nervous System Activation During the Development of Right and Left Cardiac Remodeling in Experimental Pulmonary Arterial Hypertension. Mol. Cell Biochem. 2020, 464, 93–109. [Google Scholar] [CrossRef]
- de Amorim Correa, R.; de Oliveira, F.B.; Barbosa, M.M.; Barbosa, J.A.; Carvalho, T.S.; Barreto, M.C.; Campos, F.T.; Nunes, M.C. Left Ventricular Function in Patients with Pulmonary Arterial Hypertension: The Role of Two-Dimensional Speckle Tracking Strain. Echocardiography 2016, 33, 1326–1334. [Google Scholar] [CrossRef]
- Hardegree, E.L.; Sachdev, A.; Fenstad, E.R.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Oh, J.K.; Ammash, N.M.; Connolly, H.M.; Eidem, B.W.; et al. Impaired Left Ventricular Mechanics in Pulmonary Arterial Hypertension: Identification of a Cohort at High Risk. Circ. Heart Fail. 2013, 6, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Homsi, R.; Luetkens, J.A.; Skowasch, D.; Pizarro, C.; Sprinkart, A.M.; Gieseke, J.; Meyer Zur Heide Gen Meyer-Arend, J.; Schild, H.H.; Naehle, C.P. Left Ventricular Myocardial Fibrosis, Atrophy, and Impaired Contractility in Patients with Pulmonary Arterial Hypertension and a Preserved Left Ventricular Function: A Cardiac Magnetic Resonance Study. J. Thorac. Imaging 2017, 32, 36–42. [Google Scholar] [CrossRef]
- Kallianos, K.; Brooks, G.C.; Mukai, K.; Seguro de Carvalho, F.; Liu, J.; Naeger, D.M.; De Marco, T.; Ordovas, K.G. Cardiac Magnetic Resonance Evaluation of Left Ventricular Myocardial Strain in Pulmonary Hypertension. Acad. Radiol. 2018, 25, 129–135. [Google Scholar] [CrossRef]
- Querejeta Roca, G.; Campbell, P.; Claggett, B.; Vazir, A.; Quinn, D.; Solomon, S.D.; Shah, A.M. Impact of Lowering Pulmonary Vascular Resistance on Right and Left Ventricular Deformation in Pulmonary Arterial Hypertension. Eur. J. Heart Fail. 2015, 17, 63–73. [Google Scholar] [CrossRef] [PubMed]
- da Costa Junior, A.A.; Ota-Arakaki, J.S.; Ramos, R.P.; Uellendahl, M.; Mancuso, F.J.; Gil, M.A.; Fischer, C.H.; Moises, V.A.; de Camargo Carvalho, A.C.; Campos, O. Diagnostic and Prognostic Value of Right Ventricular Strain in Patients with Pulmonary Arterial Hypertension and Relatively Preserved Functional Capacity Studied with Echocardiography and Magnetic Resonance. Int. J. Cardiovasc. Imaging 2017, 33, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Haeck, M.L.; Scherptong, R.W.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Vliegen, H.W.; Delgado, V. Prognostic Value of Right Ventricular Longitudinal Peak Systolic Strain in Patients with Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 628–636. [Google Scholar] [CrossRef]
- Goda, A.; Ryo, K.; Delgado-Montero, A.; Tayal, B.; Handa, R.; Simon, M.A.; Gorcsan, J., 3rd. The Prognostic Utility of a Simplified Biventricular Echocardiographic Index of Cardiac Remodeling in Patients with Pulmonary Hypertension. J. Am. Soc. Echocardiogr. 2016, 29, 554–560. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Ctrl (N = 26) | PH (N = 54) | p |
|---|---|---|---|
| Female (n (%)) | 22 (84.6) | 47 (87.04) | 0.819 |
| Age (y, x ± s) | 44.70 ± 14.65 | 44.58 ± 15.45 | 0.974 |
| BSA (m2, x ± s) | 1.56 ± 0.13 | 1.54 ± 0.12 | 0.603 |
| Etiology (%) | |||
| Idiopathic pulmonary arterial hypertension | - | 16 (29.63) | |
| Connective tissue disease | - | 24 (44.44) | |
| Congenital heart disease | - | 7 (12.96) | |
| Chronic thromboembolic pulmonary hypertension | - | 6 (11.11) | |
| Portal hypertension | - | 1 (1.85) | |
| Right heart catheterization | |||
| mPAP (mmHg, x ± s) | - | 53.80 ± 13.45 | |
| PCWP[mmHg, M (Q1, Q3)] | - | 13.00 (9.00, 15.00) | |
| PVR (Wood units, x ± s) | - | 10.66 ± 4.99 | |
| CI[L/min·m2, M (Q1, Q3)] | - | 2.50 (2.08, 3.53) | |
| NYHA classification (%) | |||
| I | - | 22 (40.74) | |
| II | - | 16 (29.63) | |
| III | - | 10 (18.52) | |
| IV | - | 6 (11.11) | |
| BNP[M (Q1, Q3) | - | 242.00 (84.50, 622.00) | |
| 6MWD[m, M (Q1, Q3) | - | 410.00 (360.00, 459.00) | |
| Echocardiography | |||
| TAPSE[mm, M (Q1, Q3)] | 24.50 (22.00, 26.00) | 16.00 (13.00, 18.00) | <0.001 |
| FAC (x ± s) | 43.62 ± 6.73 | 24.77 ± 8.46 | <0.001 |
| LVEF (%, x ± s) | 61.11 ± 3.62 | 59.50 ± 7.47 | 0.195 |
| RVSP (mmHg, x ± s) | - | 75.88 ± 25.40 | |
| Speckle tracking | |||
| LVGLS[%, M (Q1, Q3) | −18.28 (−20.00, −15.38) | −15.70 (−17.68, −12.80) | 0.004 |
| LVGLS[%, x ± s] | −18.05 ± 2.76 | −15.68 ± 4.50 | 0.004 |
| RVFLS (%, x ± s) | −19.90 ± 5.43 | −13.02 ± 5.02 | <0.001 |
| LASr (%, x ± s) | 36.88 ± 13.45 | 26.07 ± 10.00 | <0.001 |
| LASc[%, M (Q1, Q3) | 22.32 (16.88, 29.75) | 11.69 (8.22, 18.84) | <0.001 |
| LASp (%, x ± s) | 15.00 ± 5.79 | 12.33 ± 4.62 | 0.034 |
| RASr (%, x ± s) | 31.82 ± 12.87 | 25.63 ± 13.50 | 0.014 |
| RASc[%, M (Q1, Q3) | 17.18 (10.88, 23.43) | 8.02 (5.12, 14.80) | <0.001 |
| RASp (%, x ± s) | 15.15 ± 5.92 | 15.39 ± 8.37 | 0.899 |
| Variable | Ctrl (N = 26) | PH (N = 54) | p |
|---|---|---|---|
| |LVGLS/RVFLS-1| | 0.20 ± 0.17 | 0.27 (0.13, 0.66) | 0.009 |
| |LASr/RASr-1| | 0.23 (0.09, 0.67) | 0.39 (0.19, 0.64) | 0.058 |
| |LASc/RASc-1| | 0.34 ± 0.18 | 0.61 (0.19, 1.47) | 0.033 |
| |LASp/RASp-1| | 0.33 (0.20, 0.39) | 0.42 (0.22, 0.62) | 0.136 |
| Variable | Spreaman | Correlation (95% Confidence Interval) | p |
|---|---|---|---|
| |LVGLS/RVFLS-1| versus | |||
| BNP | 0.4125 | 0.137–0.6288 | 0.0036 |
| 6MWD | −0.1421 | −0.4065–0.1442 | 0.3148 |
| NYHA | 0.2366 | −0.04413–0.4828 | 0.088 |
| FAC | −0.3082 | −0.5398–−0.03314 | 0.0248 |
| TAPSE | −0.2307 | −0.4802–0.05326 | 0.0998 |
| RVSP | 0.3385 | 0.06692–0.5634 | 0.0132 |
| LVEF | 0.03285 | −0.2473–0.3079 | 0.8154 |
| LVGLS | 0.02415 | −0.2554–0.3 | 0.8637 |
| RVFLS | 0.559 | 0.3328–0.7243 | <0.0001 |
| LASr | −0.1518 | −0.4123–0.1316 | 0.2779 |
| LASc | −0.1656 | −0.424–0.1177 | 0.236 |
| LASp | 0.02411 | −0.2555–0.3 | 0.8639 |
| RASr | −0.3766 | −0.5925–0.1103 | 0.0054 |
| RASc | −0.3579 | −0.5783–−0.08888 | 0.0085 |
| RASp | −0.2129 | −0.4634–0.06904 | 0.1258 |
| Variables | Univariate Regression | Multivariate Regression | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95%CI | p | Hazard Ratio | 95%CI | p | |
| Age | 1.01 | 0.975–1.045 | 0.59 | |||
| BSA | 62.806 | 0.348–11,294.669 | 0.118 | |||
| BNP | 1.001 | 1.001–1.002 | 0.001 | |||
| 6MWD | 0.994 | 0.991–0.998 | 0.003 | 0.995 | 0.991–0.999 | 0.02 |
| NYHA | 2.062 | 1.227–3.464 | 0.006 | |||
| LVEF | 1.007 | 0.929–1.092 | 0.863 | |||
| FAC | 0.927 | 0.873–0.985 | 0.014 | |||
| TAPSE | 0.9 | 0.799–1.015 | 0.087 | |||
| TEI | 1.819 | 0.712–4.648 | 0.212 | |||
| RVSP | 1.041 | 1.012–1.070 | 0.005 | |||
| LVGLS | 1.295 | 1.077–1.557 | 0.006 | |||
| RVFLS | 1.238 | 1.080–1.420 | 0.002 | |||
| LASr | 0.954 | 0.898–1.013 | 0.124 | |||
| LASc | 0.911 | 0.833–0.996 | 0.041 | |||
| LASp | 1.012 | 0.891–1.149 | 0.856 | |||
| RASr | 0.95 | 0.904–0.997 | 0.038 | |||
| RASc | 0.946 | 0.869–1.030 | 0.201 | |||
| RASp | 0.928 | 0.861–1.001 | 0.053 | |||
| |LVGLS/RVFLS-1| | 4.026 | 1.872–8.662 | <0.001 | 3.152 | 1.413–7.034 | 0.005 |
| |LASr/RASr-1| | 1.28 | 0.800–2.046 | 0.303 | |||
| |LASc/RASc-1| | 0.501 | 0.210–1.197 | 0.12 | |||
| |LASp/RASp-1| | 1.441 | 1.126–1.845 | 0.004 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Ruan, B.; Qiao, Z.; Yang, M.; Zhuang, Q.; Wang, J.; Wang, W.; Zheng, Y.; Zhao, H.; Shen, X.; et al. The Balance between the Left and Right Ventricular Deformation Evaluated by Speckle Tracking Echocardiography Is a Great Predictor of the Major Adverse Cardiac Event in Patients with Pulmonary Hypertension. Diagnostics 2022, 12, 2266. https://doi.org/10.3390/diagnostics12092266
Zhang X, Ruan B, Qiao Z, Yang M, Zhuang Q, Wang J, Wang W, Zheng Y, Zhao H, Shen X, et al. The Balance between the Left and Right Ventricular Deformation Evaluated by Speckle Tracking Echocardiography Is a Great Predictor of the Major Adverse Cardiac Event in Patients with Pulmonary Hypertension. Diagnostics. 2022; 12(9):2266. https://doi.org/10.3390/diagnostics12092266
Chicago/Turabian StyleZhang, Xueming, Binqian Ruan, Zhiqing Qiao, Menghui Yang, Qi Zhuang, Jian Wang, Wei Wang, Ying Zheng, Hang Zhao, Xuedong Shen, and et al. 2022. "The Balance between the Left and Right Ventricular Deformation Evaluated by Speckle Tracking Echocardiography Is a Great Predictor of the Major Adverse Cardiac Event in Patients with Pulmonary Hypertension" Diagnostics 12, no. 9: 2266. https://doi.org/10.3390/diagnostics12092266