
Low-Milliampere CT Fluoroscopy-Guided Percutaneous Drainage Placement after Pancreatic Surgery: Technical and Clinical Outcome in 133 Consecutive Patients during a 14-Year Period
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
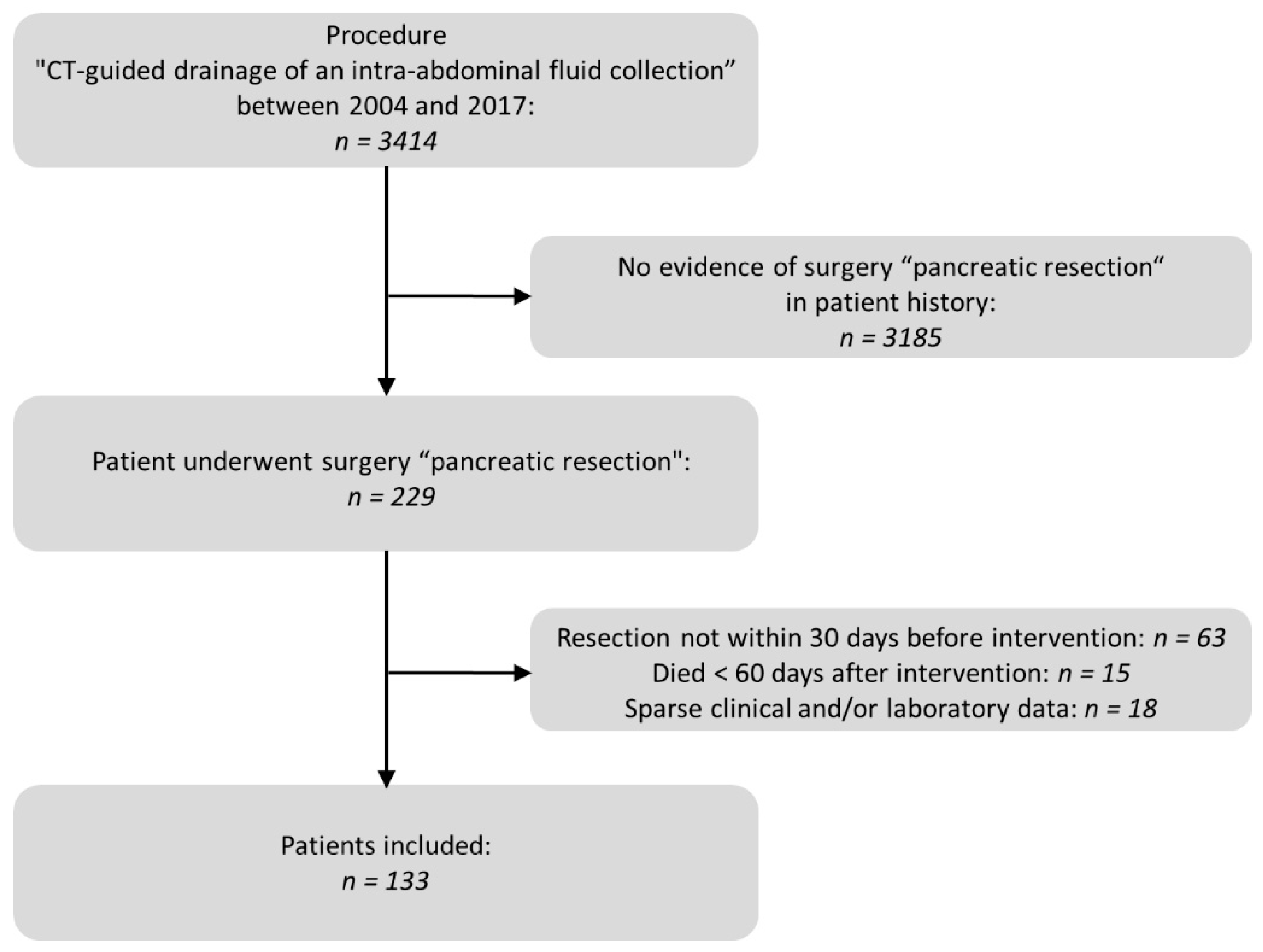
2.1. Study Subjects
2.2. CT Imaging Protocol
2.3. Analysis of Pre- and Peri-Interventional Period
2.4. Analysis of Post-Interventional Period
2.5. Statistical Analysis
3. Results
3.1. Pre- and Peri-Interventional Analysis
3.2. Post-Interventional Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.J.; Wong, M.C. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Torphy, R.J.; Fujiwara, Y.; Schulick, R.D. Pancreatic cancer treatment: Better, but a long way to go. Surg. Today 2020, 50, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Hackert, T.; Klaiber, U.; Pausch, T.; Mihaljevic, A.L.; Büchler, M.W. Fifty Years of Surgery for Pancreatic Cancer. Pancreas 2020, 49, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Asbun, H.J.; Moekotte, A.L.; Vissers, F.L.; Kunzler, F.; Cipriani, F.; Alseidi, A.; D’Angelica, M.I.; Balduzzi, A.; Bassi, C.; Björnsson, B.; et al. The Miami International Evidence-based Guidelines on Minimally Invasive Pancreas Resection. Ann. Surg. 2020, 271, 1–14. [Google Scholar] [CrossRef]
- Berry, A.J. Pancreatic surgery: Indications, complications, and implications for nutrition intervention. Nutr. Clin. Pract. 2013, 28, 330–357. [Google Scholar] [CrossRef]
- Sierzega, M.; Kulig, P.; Kolodziejczyk, P.; Kulig, J. Natural history of intra-abdominal fluid collections following pancreatic surgery. J. Gastrointest. Surg. 2013, 17, 1406–1413. [Google Scholar] [CrossRef]
- Tjaden, C.; Hinz, U.; Hassenpflug, M.; Fritz, F.; Fritz, S.; Grenacher, L.; Büchler, M.W.; Hackert, T. Fluid collection after distal pancreatectomy: A frequent finding. HPB 2016, 18, 35–40. [Google Scholar] [CrossRef]
- Cronin, C.G.; Gervais, D.A.; Castillo, C.F.; Mueller, P.R.; Arellano, R.S. Interventional radiology in the management of abdominal collections after distal pancreatectomy: A retrospective review. AJR Am. J. Roentgenol. 2011, 197, 241–246. [Google Scholar] [CrossRef]
- Kawaida, H.; Kono, H.; Hosomura, N.; Amemiya, H.; Itakura, J.; Fujii, H.; Ichikawa, D. Surgical techniques and postoperative management to prevent postoperative pancreatic fistula after pancreatic surgery. World J. Gastroenterol. 2019, 25, 3722–3737. [Google Scholar] [CrossRef]
- Sirinek, K.R. Diagnosis and treatment of intra-abdominal abscesses. Surg. Infect. 2000, 1, 31–38. [Google Scholar] [CrossRef]
- Asai, N.; Ohkuni, Y.; Yamazaki, I.; Kaneko, N.; Aoshima, M.; Kawamura, Y. Therapeutic impact of CT-guided percutaneous catheter drainage in treatment of deep tissue abscesses. Braz. J. Infect. Dis. 2013, 17, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Van Sonnenberg, E.; Wittich, G.R.; Goodacre, B.W.; Casola, G.; D’Agostino, H.B. Percutaneous abscess drainage: Update. World J. Surg. 2001, 25, 362–369, discussion 370–372. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.J.; Chin, K.W.; Fletcher, T.B.; Bakal, C.W.; Cardella, J.F.; Grassi, C.J.; Grizzard, J.D.; Kaye, A.D.; Kushner, D.C.; Larson, P.A.; et al. Quality improvement guidelines for percutaneous drainage/aspiration of abscess and fluid collections. J. Vasc. Interv. Radiol. 2010, 21, 431–435. [Google Scholar] [CrossRef]
- Jiang, L.; Ning, D.; Chen, X. Prevention and treatment of pancreatic fistula after pancreatic body and tail resection: Current status and future directions. Front. Med. 2020, 14, 251–261. [Google Scholar] [CrossRef]
- Men, S.; Akhan, O.; Köroğlu, M. Percutaneous drainage of abdominal abcess. Eur. J. Radiol. 2002, 43, 204–218. [Google Scholar] [CrossRef]
- Roberts, B.W. CT-guided Intra-abdominal Abscess Drainage. Radiol. Technol. 2015, 87, 187CT–203CT. [Google Scholar] [PubMed]
- Kim, Y.J.; Han, J.K.; Lee, J.M.; Kim, S.H.; Lee, K.H.; Park, S.H.; An, S.K.; Lee, J.Y.; Choi, B.I. Percutaneous drainage of postoperative abdominal abscess with limited accessibility: Preexisting surgical drains as alternative access route. Radiology 2006, 239, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Laganà, D.; Carrafiello, G.; Mangini, M.; Ianniello, A.; Giorgianni, A.; Nicotera, P.; Fontana, F.; Dionigi, G.; Fugazzola, C. Image-guided percutaneous treatment of abdominal-pelvic abscesses: A 5-year experience. Radiol. Med. 2008, 113, 999–1007. [Google Scholar] [CrossRef]
- Gee, M.S.; Kim, J.Y.; Gervais, D.A.; Hahn, P.F.; Mueller, P.R. Management of abdominal and pelvic abscesses that persist despite satisfactory percutaneous drainage catheter placement. AJR Am. J. Roentgenol. 2010, 194, 815–820. [Google Scholar] [CrossRef]
- Gervais, D.A.; Ho, C.H.; O’Neill, M.J.; Arellano, R.S.; Hahn, P.F.; Mueller, P.R. Recurrent abdominal and pelvic abscesses: Incidence, results of repeated percutaneous drainage, and underlying causes in 956 drainages. AJR Am. J. Roentgenol. 2004, 182, 463–466. [Google Scholar] [CrossRef]
- Maher, M.M.; Gervais, D.A.; Kalra, M.K.; Lucey, B.; Sahani, D.V.; Arellano, R.; Hahn, P.F.; Mueller, P.R. The inaccessible or undrainable abscess: How to drain it. Radiographics 2004, 24, 717–735. [Google Scholar] [CrossRef] [PubMed]
- Nattenmüller, J.; Filsinger, M.; Bryant, M.; Stiller, W.; Radeleff, B.; Grenacher, L.; Kauczor, H.U.; Hosch, W. Complications in CT-guided procedures: Do we really need postinterventional CT control scans? Cardiovasc. Interv. Radiol. 2014, 37, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Sun, S.; Gao, H.; Gao, Y.; Xu, Q.; Liu, X.; Miao, Y.; Wei, J. CT-guided percutaneous catheter drainage of pancreatic postoperative collections. Minim. Invasive Allied Technol. 2020, 29, 269–274. [Google Scholar] [CrossRef]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Geschwind, J.F.; Mitchell, S.E.; Venbrux, A.C.; Lillemoe, K.D. Pancreaticoduodenectomy: Role of interventional radiologists in managing patients and complications. J. Gastrointest. Surg. 2003, 7, 209–219. [Google Scholar] [CrossRef]
- Takaki, H.; Yamakado, K.; Kuriyama, N.; Nakatsuka, A.; Sakuma, H.; Isaji, S. Percutaneous drainage of pancreatic fistula following pancreatectomy with CT-fluoroscopic guidance. Diagn. Interv. Imaging 2017, 98, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Zink, S.I.; Soloff, E.V.; White, R.R.; Clary, B.M.; Tyler, D.S.; Pappas, T.N.; Paulson, E.K. Pancreaticoduodenectomy: Frequency and outcome of post-operative imaging-guided percutaneous drainage. Abdom. Imaging 2009, 34, 767–771. [Google Scholar] [CrossRef]
- Gupta, S.; Wallace, M.J.; Cardella, J.F.; Kundu, S.; Miller, D.L.; Rose, S.C. Quality improvement guidelines for percutaneous needle biopsy. J. Vasc. Interv. Radiol. 2010, 21, 969–975. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Hilal, M.A.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef]
- Bramhall, S.R.; Allum, W.H.; Jones, A.G.; Allwood, A.; Cummins, C.; Neoptolemos, J.P. Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: An epidemiological study. Br. J. Surg. 1995, 82, 111–115. [Google Scholar] [CrossRef]
- Michelassi, F.A.; Erroi, F.R.; Dawson, P.J.; Pietrabissa, A.N.; Noda, S.E.; Handcock, M.A.; Block, G.E. Experience with 647 consecutive tumors of the duodenum, ampulla, head of the pancreas, and distal common bile duct. Ann. Surg. 1989, 210, 544–554, discussion 554–546. [Google Scholar] [CrossRef] [PubMed]
- Nakase, A.; Matsumoto, Y.; Uchida, K.; Honjo, I. Surgical treatment of cancer of the pancreas and the periampullary region: Cumulative results in 57 institutions in Japan. Ann. Surg. 1977, 185, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.L.; Riall, T.S.; Coleman, J.; Belcher, K.A. One thousand consecutive pancreaticoduodenectomies. Ann. Surg. 2006, 244, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Mortele, K.J.; Girshman, J.; Szejnfeld, D.; Ashley, S.W.; Erturk, S.M.; Banks, P.A.; Silverman, S.G. CT-guided percutaneous catheter drainage of acute necrotizing pancreatitis: Clinical experience and observations in patients with sterile and infected necrosis. AJR Am. J. Roentgenol. 2009, 192, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Politano, A.D.; Hranjec, T.; Rosenberger, L.H.; Sawyer, R.G.; Tache Leon, C.A. Differences in morbidity and mortality with percutaneous versus open surgical drainage of postoperative intra-abdominal infections: A review of 686 cases. Am. Surg. 2011, 77, 862–867. [Google Scholar] [CrossRef]
- Turan, H.G.; Özdemir, M.; Acu, R.; Küçükay, F.; Özdemir, F.A.; Hekimoğlu, B.; Yıldırım, U.M. Comparison of seldinger and trocar techniques in the percutaneous treatment of hydatid cysts. World J. Radiol. 2017, 9, 405–412. [Google Scholar] [CrossRef]
- Furukawa, K.; Gocho, T.; Sakamoto, T.; Tsunematsu, M.; Haruki, K.; Horiuchi, T.; Shirai, Y.; Yasuda, J.; Shiozaki, H.; Onda, S.; et al. Intraoperative amylase level of pancreatic juice as a simple predictor of pancreatic fistula after pancreaticoduodenectomy. Pancreatology 2021, 21, 299–305. [Google Scholar] [CrossRef]
- Paik, K.Y.; Oh, J.S.; Kim, E.K. Amylase level after pancreaticoduodenectomy in predicting postoperative pancreatic fistula. Asian J. Surg. 2021, 44, 636–640. [Google Scholar] [CrossRef]
- Akinci, D.; Akhan, O.; Ozmen, M.N.; Karabulut, N.; Ozkan, O.; Cil, B.E.; Karcaaltıncaba, M. Percutaneous drainage of 300 intraperitoneal abscesses with long-term follow-up. Cardiovasc. Interv. Radiol. 2005, 28, 744–750. [Google Scholar] [CrossRef]
- Carlson, S.K.; Bender, C.E.; Classic, K.L.; Zink, F.E.; Quam, J.P.; Ward, E.M.; Oberg, A.L. Benefits and safety of CT fluoroscopy in interventional radiologic procedures. Radiology 2001, 219, 515–520. [Google Scholar] [CrossRef]
- Grosser, O.S.; Wybranski, C.; Kupitz, D.; Powerski, M.; Mohnike, K.; Pech, M.; Amthauer, H.; Ricke, J. Improvement of image quality and dose management in CT fluoroscopy by iterative 3D image reconstruction. Eur. Radiol. 2017, 27, 3625–3634. [Google Scholar] [CrossRef] [PubMed]
- Paprottka, P.M.; Helmberger, T.; Reiser, M.F.; Trumm, C.G. Computed tomography guidance: Fluoroscopy and more. Radiologe 2013, 53, 974–985. [Google Scholar] [CrossRef] [PubMed]
- Hohl, C.; Suess, C.; Wildberger, J.E.; Honnef, D.; Das, M.; Mühlenbruch, G.; Schaller, A.; Gunther, R.W.; Mahnken, A.H. Dose reduction during CT fluoroscopy: Phantom study of angular beam modulation. Radiology 2008, 246, 519–525. [Google Scholar] [CrossRef]
- Christe, A.; Heverhagen, J.; Ozdoba, C.; Weisstanner, C.; Ulzheimer, S.; Ebner, L. CT dose and image quality in the last three scanner generations. World J. Radiol. 2013, 5, 421–429. [Google Scholar] [CrossRef]
- Rathmann, N.; Haeusler, U.; Diezler, P.; Weiss, C.; Kostrzewa, M.; Sadick, M.; Schoenberg, S.O.; Diehl, S.J. Evaluation of radiation exposure of medical staff during CT-guided interventions. J. Am. Coll. Radiol. 2015, 12, 82–89. [Google Scholar] [CrossRef]
- Brook, I. Microbiology and management of abdominal infections. Dig. Dis. Sci. 2008, 53, 2585–2591. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.G.; Serufo, J.C.; Silva, R.A.; Marra, B.A.; Reis, C.M.; Hamdan, J.S.; Nicoli, J.R.; Carvalho, M.A.; Farias, L.M. Microbiologic profile of intra-abdominal infections at Belo Horizonte, Brazil. Am. J. Infect. Control 2003, 31, 135–143. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgery Technique | Total | Additional Resected Organs or Organ Systems and Performed Surgical Procedures 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Hemicolectomy | Splenectomy | Cholecystectomy | Gastrectomy | Adrenalectomy | Hepatectomy | Other Organ Systems | Other Anastomosis | ||
| Classic pancreaticoduodenectomy | 34 (25.6%) 1 | 3 (2.3 %) 1 | 2 (1.5%) 1 | 1 (0.8 %) 1 | 7 (5.3%) 1 | 2 (1.5%) 1 | |||
| Pylorus-preserving pancreaticoduodenectomy | 45 (33.8%) 1 | 1 (0.8%) 1 | 3 (2.3 %) 1 | 6 (4.5%) 1 | |||||
| Distal pancreatectomy | 40 (30.1%) 1 | 3 (2.3 %) 1 | 30 (22.6%) 1 | 7 (5.3%) 1 | 3 (2.3%) 1 | 5 (3.8%) 1 | 1 (0.8 %) 1 | 11 (8.3%) 1 | 2 (1.5%) 1 |
| Pancreatic segmentectomy/Enucleation/Biopsy sampling | 9 (6.8%) 1 | 1 (0.8%) 1 | 1 (0.8%) 1 | 1 (0.8%) 1 | 2 (1.5%) 1 | ||||
| Duodenum-preserving pancreatic head resection | 5 (3.8%) 1 | 1 (0.8%) 1 | 1 (0.8%) 1 | 1 (0.8%) 1 | |||||
| Time from surgery to first intervention (days): | 13.5 ± 6.5 (4–30) 1 |
| Maximum extension of fluid collection (cm) | 8.1 ± 3.0 (3.3–18.0) 1 |
| Predominant location of fluid collection | Count |
| subdiaphragmatic | 5 (3.0%) 2 |
| abdominal wall | 4 (2.4%) 2 |
| perihepatic | 44 (26.3%) 2 |
| paragastric | 11 (6.6%) 2 |
| paracolic | 4 (2.4%) 2 |
| perisplenic | 15 (9.0%) 2 |
| peripancreatic | 72 (43.1%) 2 |
| perirenal | 5 (3.0%) 2 |
| paraaortal/paracaval | 4 (2.4%) 2 |
| pelvic | 3 (1.8%) 2 |
| Drainages per intervention | Count |
| 1 | 127 (76.0%) 2 |
| 2 | 39 (23.4%) 2 |
| 3 | 1 (0.6%) 2 |
| Diameter (French) | Count |
| 6 | 1 (0.7%) 2 |
| 7.5 | 3 (2.1%) 2 |
| 8 | 66 (46.8%) 2 |
| 10 | 53 (37.6%) 2 |
| 12 | 14 (9.9%) 2 |
| 14 | 3 (2.1%) 2 |
| 20 | 1 (0.7%) 2 |
| Technique | Count |
| Trocar | 151 (90.4%) 2 |
| Seldinger | 16 (9.6%) 2 |
| Access path | Count |
| transabdominal | 124 (74.3%) 2 |
| transhepatic | 17 (10.2%) 2 |
| transretroperitoneal | 26 (15.6%) 2 |
| Amount of Interventions | ||||||
|---|---|---|---|---|---|---|
| Surgery Technique | Count | Presence of POPF | Positive Proof of Germs in First Intervention | 1 | 2 | 3 |
| Classic pancreaticoduodenectomy | 34 | 11 (32.4%) 1 | 23 (67.6%) 1 | 25 (73.5%) 1 | 7 (20.6%) 1 | 2 (5.9%) 1 |
| Pylorus-preserving pancreaticoduodenectomy | 45 | 18 (40.0 %) 1 | 30 (66.7%) 1 | 38 (84.5%) 1 | 7 (15.5%) 1 | 0 (0.0%) 1 |
| Distal pancreatectomy | 40 | 23 (57.5%) 1 | 14 (35.0%) 1 | 28 (70.0%) 1 | 10 (25.0%) 1 | 2 (5.0%) 1 |
| Pancreatic segmentectomy/Enucleation/Biopsy sampling | 9 | 5 (55.6%) 1 | 5 (55.6%) 1 | 9 (100%) 1 | 0 (0.0%) 1 | 0 (0.0%) 1 |
| Duodenum-preserving pancreatic head resection | 5 | 2 (40.0%) 1 | 5 (100.0%) 1 | 3 (60.0%) 1 | 2 (40.0%) 1 | 0 (0.0%) 1 |
| Type of Complication | Count | Clavien-Dindo Classification |
|---|---|---|
| Minor complication: | ||
| Small pneumothorax | 2 (1.2%) 1 | I |
| Major complication: | ||
| Hemorrhage | 1 (0.6%) 1 | III a |
| C-Reactive Protein | Leukocytes | Interleukin-6 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Operation Technique | Elevated (n) | Success (n, %) | No Success (n, %) | Elevated(n) | Success (n, %) | No Success (n, %) | Elevated(n) | Success (n, %) | No Success (n, %) |
| Classic pancreaticoduodenectomy | 31 | 27 (87.1) | 4 (12.9) | 31 | 24 (77.4) | 7 (22.6) | 7 | 5 (71.4) | 2 (28.6) |
| Pylorus-preserving pancreaticoduodenectomy | 34 | 30 (88.2) | 4 (11.8) | 33 | 27 (81.8) | 6 (18.2) | 4 | 4 (100.0) | 0 (0.0) |
| Distal pancreatectomy | 35 | 29 (82.9) | 6 (17.1) | 38 | 28 (73.7) | 10 (26.3) | 4 | 4 (100.0) | 0 (0.0) |
| Pancreatic segmentectomy/Enucleation/Biopsy sampling | 6 | 6 (100.0) | 0 (0.0) | 5 | 4 (80.0) | 1 (20.0) | 1 | 1 (100.0) | 0 (0.0) |
| Duodenum-preserving pancreatic head resection | 6 | 6 (100.0) | 0 (0.0) | 4 | 4 (100.0) | 0 (0.0) | 0 | 0 (0.0) | 0 (0.0) |
| Total | 112 | 98 (87.5) | 14 (12.5) | 111 | 87 (78.4) | 24 (21.6) | 16 | 14 (87.5) | 2 (12.5) |
| C-Reactive Protein | Leukocytes | Interleukin-6 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Fluid Collection Infection Status | Elevated (n) | Success (n, %) | No Success (n, %) | Elevated (n) | Success (n, %) | No Success (n, %) | Elevated (n) | Success (n, %) | No Success (n, %) |
| Infected | 60 | 56 (93.3) | 4 (6.7) | 59 | 52 (88.1) | 7 (11.9) | 8 | 7 (87.5) | 1 (12.5) |
| Non-infected | 39 | 32 (82.0) | 7 (18.0) | 38 | 30 (78.9) | 8 (21.1) | 4 | 3 (75.0) | 1 (25.0) |
| Total | 99 | 88 (88.9) | 11 (11.1) | 97 | 82 (84.5) | 15 (15.5) | 12 | 10 (83.3) | 2 (16.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trumm, C.G.; Hackner, D.; Badmann, K.; Crispin, A.; Forbrig, R.; Ozpeynirci, Y.; Kuppinger, D.; Pedersen, V.; Liebig, T.; Stahl, R. Low-Milliampere CT Fluoroscopy-Guided Percutaneous Drainage Placement after Pancreatic Surgery: Technical and Clinical Outcome in 133 Consecutive Patients during a 14-Year Period. Diagnostics 2022, 12, 2243. https://doi.org/10.3390/diagnostics12092243
Trumm CG, Hackner D, Badmann K, Crispin A, Forbrig R, Ozpeynirci Y, Kuppinger D, Pedersen V, Liebig T, Stahl R. Low-Milliampere CT Fluoroscopy-Guided Percutaneous Drainage Placement after Pancreatic Surgery: Technical and Clinical Outcome in 133 Consecutive Patients during a 14-Year Period. Diagnostics. 2022; 12(9):2243. https://doi.org/10.3390/diagnostics12092243
Chicago/Turabian StyleTrumm, Christoph G., Danilo Hackner, Katharina Badmann, Alexander Crispin, Robert Forbrig, Yigit Ozpeynirci, David Kuppinger, Vera Pedersen, Thomas Liebig, and Robert Stahl. 2022. "Low-Milliampere CT Fluoroscopy-Guided Percutaneous Drainage Placement after Pancreatic Surgery: Technical and Clinical Outcome in 133 Consecutive Patients during a 14-Year Period" Diagnostics 12, no. 9: 2243. https://doi.org/10.3390/diagnostics12092243