
Encrusted Uretero-Pyelitis Caused by Corynebacterium urealyticum: Case Report and Literature Review
 , , ,
, , ,
Abstract
:1. Background
2. Case Report
2.1. Presentation
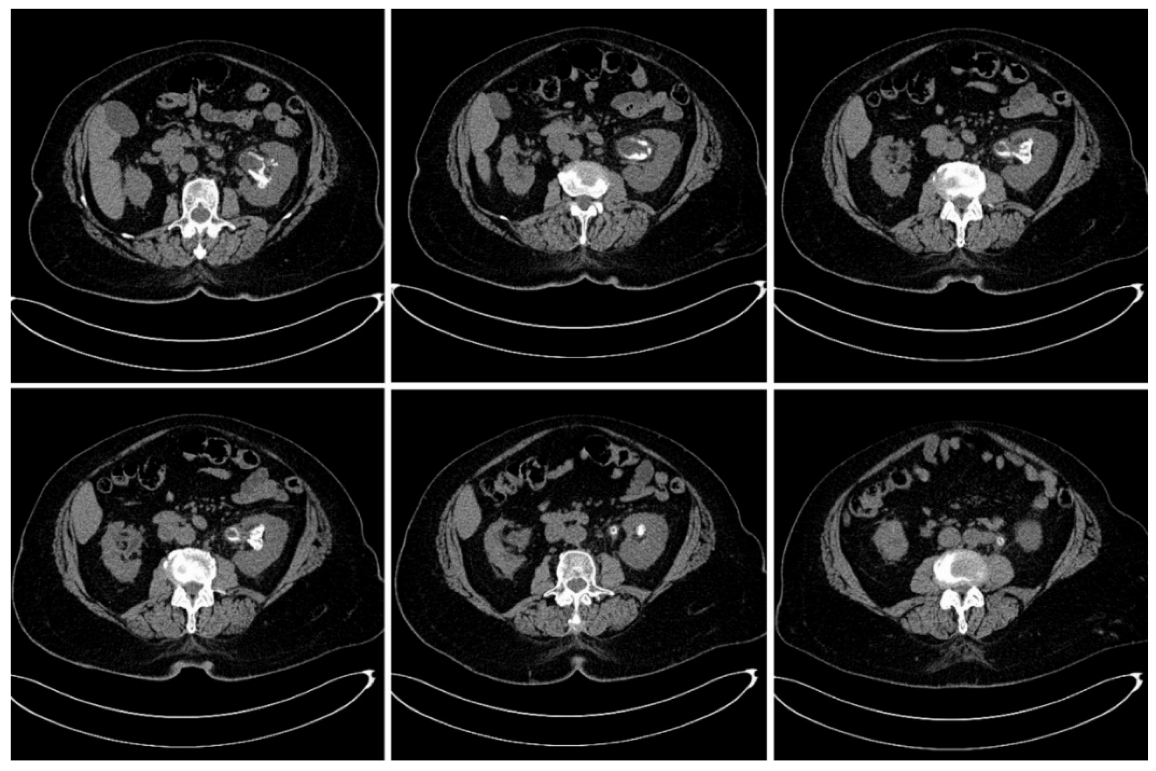
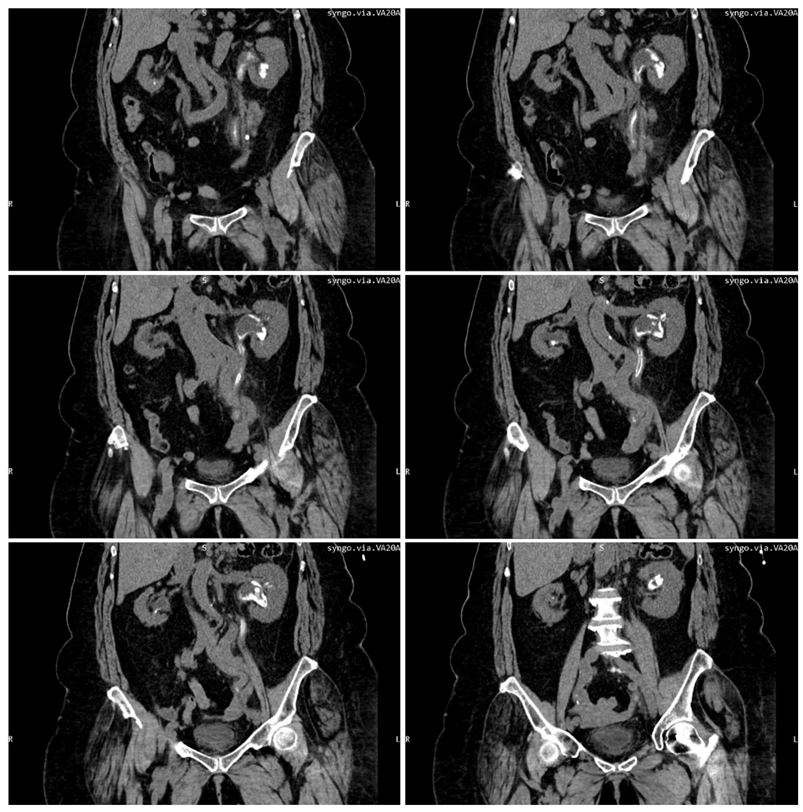
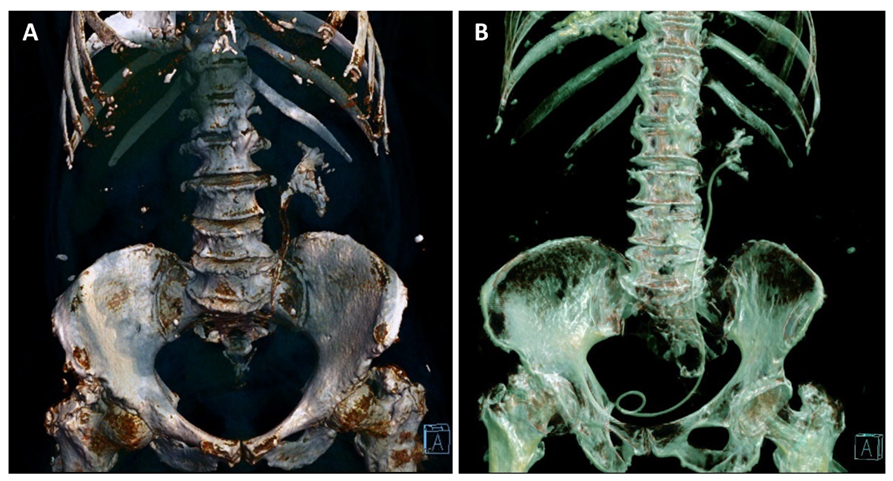
2.2. Diagnosis
2.3. Therapy
2.4. Hospital Discharge
2.5. Follow-Up
3. Discussion
4. Literature Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Morales, J.M.; Aguado, J.M.; Diaz-Gonzalez, R.; Salto, E.; Andres, A.; Campo, C.; Praga, M.; A Martinez, M.; Leiva, O.; Rodriguez-Noriega, A. Alkaline-encrusted pyelitis/cystitis and urinary tract infection due to corynebacterium urealyticum: A new severe complication after renal transplantation. Transplant. Proc. 1992, 24, 81–82. [Google Scholar]
- Bluth, M.H.; Salem, N.; Salem, L.; Saber, S.; Ismail, G.A. Corynebacterium urealyticum: A comprehensive review of an understated organism. Infect. Drug Resist. 2015, 8, 129–145. [Google Scholar] [CrossRef]
- Tauch, A.; Trost, E.; Tilker, A.; Ludewig, U.; Schneiker, S.; Goesmann, A.; Arnold, W.; Bekel, T.; Brinkrolf, K.; Brune, I.; et al. The lifestyle of Corynebacterium urealyticum derived from its complete genome sequence established by pyrosequencing. J. Biotechnol. 2008, 136, 11–21. [Google Scholar] [CrossRef]
- Bernard, K. Corynebacterium species and coryneforms: An update on taxonomy and diseases attributed to these taxa. Clin. Microbiol. Newsl. 2005, 27, 9–18. [Google Scholar] [CrossRef]
- Marty, N.; Agueda, L.; Lapchine, L.; Clavé, D.; Henry-Ferry, S.; Chabanon, G. Adherence and hemagglutination ofCorynebacterium group D2. Eur. J. Clin. Microbiol. 1991, 10, 20–24. [Google Scholar] [CrossRef]
- Meria, P.; Desgrippes, A.; Arfi, C.; Le Duc, A. Encrusted cystitis and pyelitis. J. Urol. 1998, 160, 3–9. [Google Scholar] [CrossRef]
- Eschwege, P.; Hauk, M.; Blanchet, P.; Hiesse, C.; Vieillefond, A.; Blery, M.; Charpentier, B.; Benoit, G. Imaging analysis of encrusted cystitis and pyelitis in renal transplantation. Transplant. Proc. 1995, 27, 2444–2445. [Google Scholar]
- Thoumas, D.; Darmallaicq, C.; Pfister, C.; Savoye-Collet, C.; Sibert, L.; Grise, P.; Lemaitre, L.; Benozio, M. Imaging Characteristics of Alkaline-Encrusted Cystitis and Pyelitis. Am. J. Roentgenol. 2002, 178, 389–392. [Google Scholar] [CrossRef]
- Cappuccino, L.; Bottino, P.; Torricella, A.; Pontremoli, R. Nephrolithiasis by Corynebacterium urealyticum infection: Literature review and case report. J. Nephrol. 2014, 27, 117–125. [Google Scholar] [CrossRef]
- Simoons-Smit, A.M.; Savelkoul, P.H.M.; Newling, D.W.W.; Vandenbroucke-Grauls, C.M.J. Chronic cystitis caused by Corynebacterium urealyticum detected by polymerase chain reaction. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 949–952. [Google Scholar] [CrossRef]
- Aguado, J.M.; Morales, J.M.; Salto, E.; Lumbreras, C.; Lizasoain, M.; Diaz-Gonzalez, R.; Martinez, M.A.; Andres, A.; Praga, M.; Noriega, A.R. Encrusted Pyelitis And Cystitis by Corynebacterium Urealyticum (CDC GROUP D2): A New and Threatening Complication Following Renal Transplant. Transplantation 1993, 56, 617–622. [Google Scholar] [CrossRef]
- Khallouk, A.; Wallerand, H.; Kleinclauss, F.; Bittard, H.; Bernardini, S. Conservative management of Corynebacterium urealyticum encrusted cystitis. Prog. Urol. 2006, 16, 496–498. [Google Scholar]
- Meria, P.; Desgrippes, A.; Fournier, R.; Arfi, C.; Antoine, C.; Martinat l Teillac, P.; Le Duc, A. The conservative management of Corynebacterium group D2 encrusted pyelitis. BJU Int. 1999, 84, 270–275. [Google Scholar] [CrossRef]
- Dominguez-Gil, B.; Herrero, J.C.; Carreño, A.; Morales, E.; Andres, A.; Aguado, J.M.; Díaz-González, R.; Benito, A.; Morales, J.M. Ureteral stenosis secondary to encrustation by urea-splitting Corynebacterium urealyticum in a kidney transplant patient. Nephrol. Dial. Transplant. 1999, 14, 977–978. [Google Scholar] [CrossRef]
- Hertig, A.; Duvic, C.; Chretien, Y.; Jungers, P.; Grünfeld, J.P.; Rieu, P. Encrusted pyelitis of native kidneys. J. Am. Soc. Nephrol. 2000, 11, 1138–1140. [Google Scholar] [CrossRef]
- Giannakopoulos, S.; Alivizatos, G.; Deliveliotis, C.; Skolarikos, A.; Kastriotis, J.; Sofras, F. Encrusted Cystitis and Pyelitis. Eur. Urol. 2001, 39, 446–448. [Google Scholar] [CrossRef]
- García, J.; Llorente, S.; Morales, M.D.; Vazquez, V.; Serrano, C.; Reus, M. Corynebacterium Urealyticum in Renal Trasplantation. CT and Ultrasonography Imaging Characteristics of Encrusted Cystitis and Pyelitis. Nefrologia 2004, 24, 288–293. [Google Scholar]
- Meria, P.; Margaryan, M.; Haddad, E.; Dore, B.; Lottmann, H.B. Encrusted cystitis and pyelitis in children: An unusual condition with potentially severe consequences. Urology 2004, 64, 569–573. [Google Scholar] [CrossRef]
- Lee, R.; Clement, M.R.; Carr, M.C.; Canning, D.A.; Brayman, K.L. Successful treatment of encrusted cystis and pyelitis with preservation of renal graft. Transplantation 2004, 78, 302–303. [Google Scholar] [CrossRef]
- Van Hooland, S.; Vandooren, A.K.; Lerut, E.; Oyen, R.; Maes, B. Alkaline encrusted pyelitis. Acta Clin. Belg. 2005, 60, 369–372. [Google Scholar] [CrossRef]
- Lieten, S.; Schelfaut, D.; Wissing, K.M.; Geers, C.; Tielemans, C. Alkaline-encrusted pyelitis and cystitis: An easily missed and life-threatening urinary infection. BMJ Case Rep. 2011, 2011, bcr1220103613. [Google Scholar] [CrossRef]
- Anagnostou, N.; Siddins, M.; Gordon, D.L. Encrusted cystitis and pyelitis. Intern. Med. J. 2012, 42, 596–597. [Google Scholar] [CrossRef]
- Saljoghi, R.; Lipsker, A.; Caillet, K.; Malaterre, J.; Le Roux, F.; Pignot, G.; Saint, F. Encrusted Uretero-pyelitis: Case Report. Urol. Case Rep. 2016, 7, 58–60. [Google Scholar] [CrossRef]
- Sánchez-Martín, F.M.; López-Martínez, J.M.; Kanashiro-Azabache, A.; Moncada, E.; Angerri-Feu, O.; Millán-Rodríguez, F.; Villavicencio-Mavrich, H. Corynebacterium urealyticum: Increased incidence of infection and encrusted uropathy. Actas Urol. Esp. 2016, 40, 102–107. [Google Scholar] [CrossRef]
- Vergura, M.; Carosi, I.; Ercolino, G.; Palladino, D.; Prencipe, M.; Scarlatella, A.; Aucella, F. Encrusted Pyelitis during a case of Thrombotic Thrombocytopenic Purpura. Ital. Nefrol. Organo Uff. Della Soc. Ital. Nefrol. 2018, 5, 35. [Google Scholar]
- Sakhi, H.; Join-Lambert, O.; Goujon, A.; Culty, T.; Loubet, P.; Dang, J.; Drouot, S.; de Bayser, H.; Michaud, C.; Ghislain, L.; et al. Encrusted Urinary Tract Infections Due to Corynebacteria Species. Kidney Int. Rep. 2020, 6, 179–186. [Google Scholar] [CrossRef]
- Sabiote, L.; Emiliani, E.; Kanashiro, A.K.; Balañà, J.; Mosquera, L.; Sánchez-Martín, F.M.; Millán, F.; Alonso, C.; Palou, J.; Angerri, O. Oral Acidification with l-Methionine as a Noninvasive Treatment for Encrusted Uropathy. J. Endourol. Case Rep. 2020, 6, 143–146. [Google Scholar] [CrossRef]
- Johnson, M.; Perkins, S.Q.; Leavitt, D. Alkaline Encrusted Pyelitis Causing Renal Failure in a Transplant Kidney: Treatment with Percutaneous Nephrolithotomy and Urinary Acidification. J. Endourol. Case Rep. 2020, 6, 435–437. [Google Scholar] [CrossRef]
- Loghmari, A.; Bouassida, K.; Belkacem, O.; Ben Othmame, M.; Hmida, W.; Jaidane, M. The importance of surgical treatment in encrusted cystitis and pyelitis: A case report. Int. J. Surg. Case Rep. 2020, 77, 392–396. [Google Scholar] [CrossRef]
- Kotait, M.M.; Nourie, N.; Mouawad, S.; Alkassis, M.; Moukarzel, M.; Chelala, D.N.; Azar, H. Ureaplasma urealyticum –encrusted pyelitis in a kidney graft patient: A case report and narrative review on encrusted pyelitis. Transpl. Infect. Dis. 2021, 24, e13755. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients | Special Criteria | Renal Failure | Obstructive Uropathy | Antibiotic Therapy | Urinary Diversion | Urinary Acidification | Surgical Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| J.M. Aguado et al., 1993, Spain [11] | 7 | Transplant | 6 | 7 | 7 | 7 | - | Unknown | Favorable = 4 Unfavorable = 3 |
| B. Domínguez-Gil et al., 1999, Spain [14] | 1 (female) | Transplant | 1 | 1 | 1 | 1 | - | 1 | Favorable = 1 |
| P. Meria et al., 1999, France [13] | 4 Male = 1 Female = 3 | Transplant (1) | 1 | 3 | 4 | 4 | 4 | 1 | Favorable = 3 Unfavorable = 1 |
| A. Hertig et al., 2000, France [15] | 4 Male = 2 Female = 2 | - | 3 | 3 | 2 | 3 | 2 | 1 | Death = 1 Favorable = 2 Unfavorable = 1 |
| S. Giannakopoulos et al., 2001, Greece [16] | 1 (male) | - | - | 1 | 1 | 1 | - | 1 | Favorable = 1 |
| S. Garcia et al., 2004, Spain [17] | 2 | Transplant | 1 | 2 | 2 | 1 | - | 1 | Favorable = 1 Unfavorable = 1 |
| P. Meria et al., 2004, France [18] | 2 (male) | Pediatric (2) Transplant (1) | 1 | 1 | 2 | 2 | 2 | 1 | Favorable = 1 Unfavorable = 1 |
| R. Lee et al., 2004, USA. [19] | 1 (male) | Pediatric Transplant | - | - | 1 | 1 | 1 | 1 | Faborable |
| S. van Hooland et al., 2005, Belgium [20] | 1 (male) | Neobladder | 1 | - | 1 | 1 | 1 | - | Partially favorable |
| S. Lieten et al., 2011, Belgium [21] | 1 (male) | - | 1 | 1 | 1 | 1 | 1 | - | Death |
| N. Anagnostou et al., 2012, Australia [22] | 1 (male) | - | - | - | 1 | - | 1 | 1 | Death |
| L. Cappuccino et al., 2014, Italy [9] | 1 (male) | - | 1 | 1 | 1 | 1 | 1 | - | Favorable |
| R. Saljoghi et al., 2016, France [23] | 1 (male) | - | 1 | 1 | 1 | 1 | 1 | - | Favorable |
| F.M. Sánchez-Martín et al., 2016, Spain [24] | 12 Male = 2 Female = 10 | - | 8 | Unknown | 12 | 9 | 9 | 4 | Favorable = 8 Partially favorable = 2 Unfavorable = 2 |
| M. Vergura et al., 2018, Italy [25] | 1 (male) | Autoimmune thrombocyto-penic purpura | 1 | 1 | 1 | 1 | 1 | - | Death |
| H. Sakhi et al., 2020, France [26] | 15 Male = 6 Female = 9 | Transplant (4) Lymphoma (1) | 12 | 11 | 15 | 13 | 15 | 2 | Favorable = 7 Unfavorable = 4 Death = 4 |
| L. Sabiote et al., 2020, Spain [27] | 1 (male) | - | 1 | 1 | 1 | 1 | 1 | 1 | Favorable |
| M. Johnson et al., 2020, USA. [28] | 1 (female) | Transplant | 1 | 1 | 1 | 1 | - | 1 | Favorable |
| A. Loghmari et al., 2020, Tunisia [29] | 1 (male) | - | - | 1 | 1 | - | - | 1 | Favorable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusmir, A.V.; Paunescu, I.A.; Martis, S.; Latcu, S.; Novacescu, D.; Bardan, C.R.; Bob, F.; Licker, M.; Botoca, M.; Cumpanas, A.; et al. Encrusted Uretero-Pyelitis Caused by Corynebacterium urealyticum: Case Report and Literature Review. Diagnostics 2022, 12, 2239. https://doi.org/10.3390/diagnostics12092239
Rusmir AV, Paunescu IA, Martis S, Latcu S, Novacescu D, Bardan CR, Bob F, Licker M, Botoca M, Cumpanas A, et al. Encrusted Uretero-Pyelitis Caused by Corynebacterium urealyticum: Case Report and Literature Review. Diagnostics. 2022; 12(9):2239. https://doi.org/10.3390/diagnostics12092239
Chicago/Turabian StyleRusmir, Andrei Valentin, Ionut Andrei Paunescu, Sandra Martis, Silviu Latcu, Dorin Novacescu, Claudia Ramona Bardan, Flaviu Bob, Monica Licker, Mircea Botoca, Alin Cumpanas, and et al. 2022. "Encrusted Uretero-Pyelitis Caused by Corynebacterium urealyticum: Case Report and Literature Review" Diagnostics 12, no. 9: 2239. https://doi.org/10.3390/diagnostics12092239