
T Cell and Antibody Response Following Double Dose of BNT162b2 mRNA Vaccine in SARS-CoV-2 Naïve Heart Transplant Recipients
 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Studypopulation
2.2. Sample Processing
2.3. Antibody Response
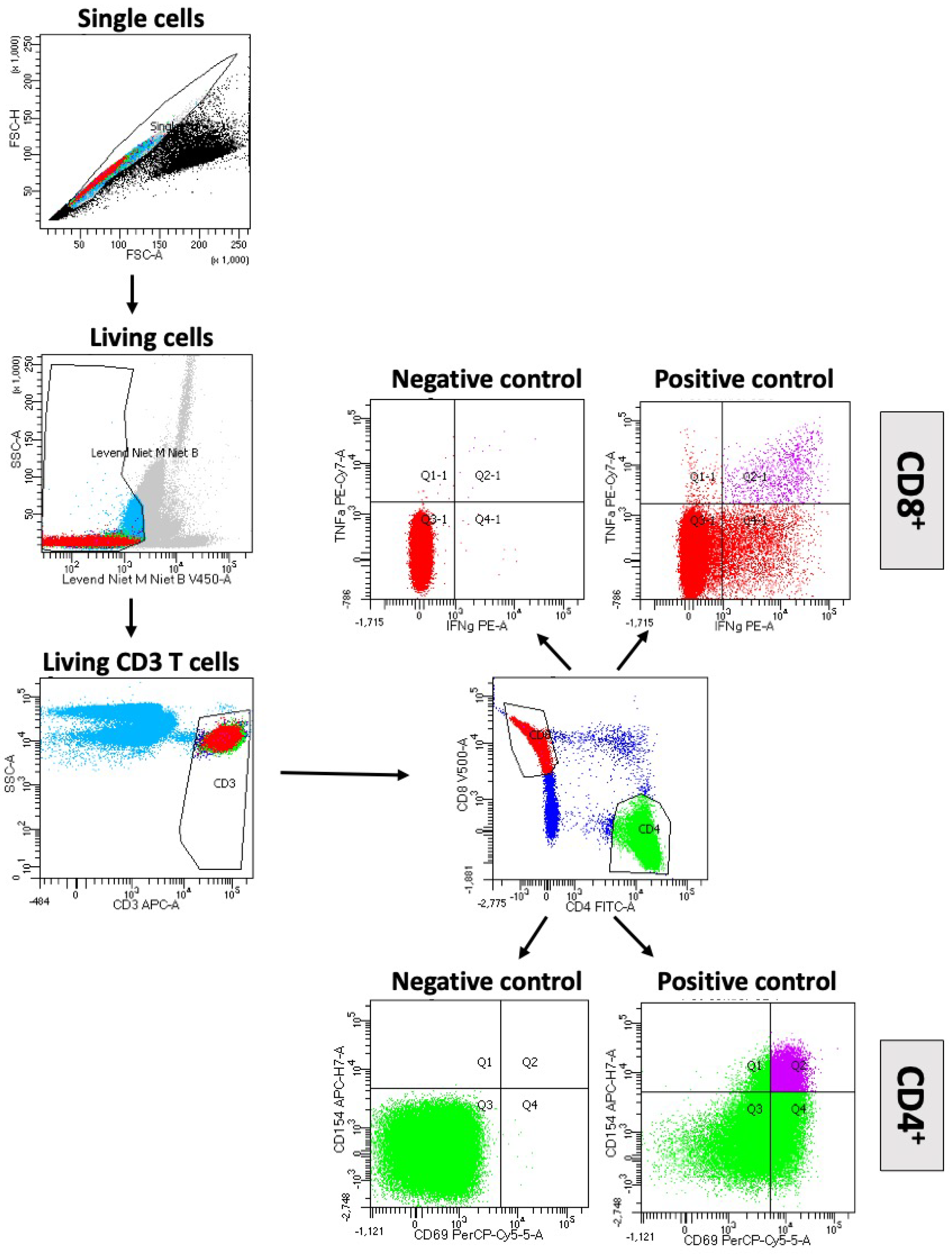
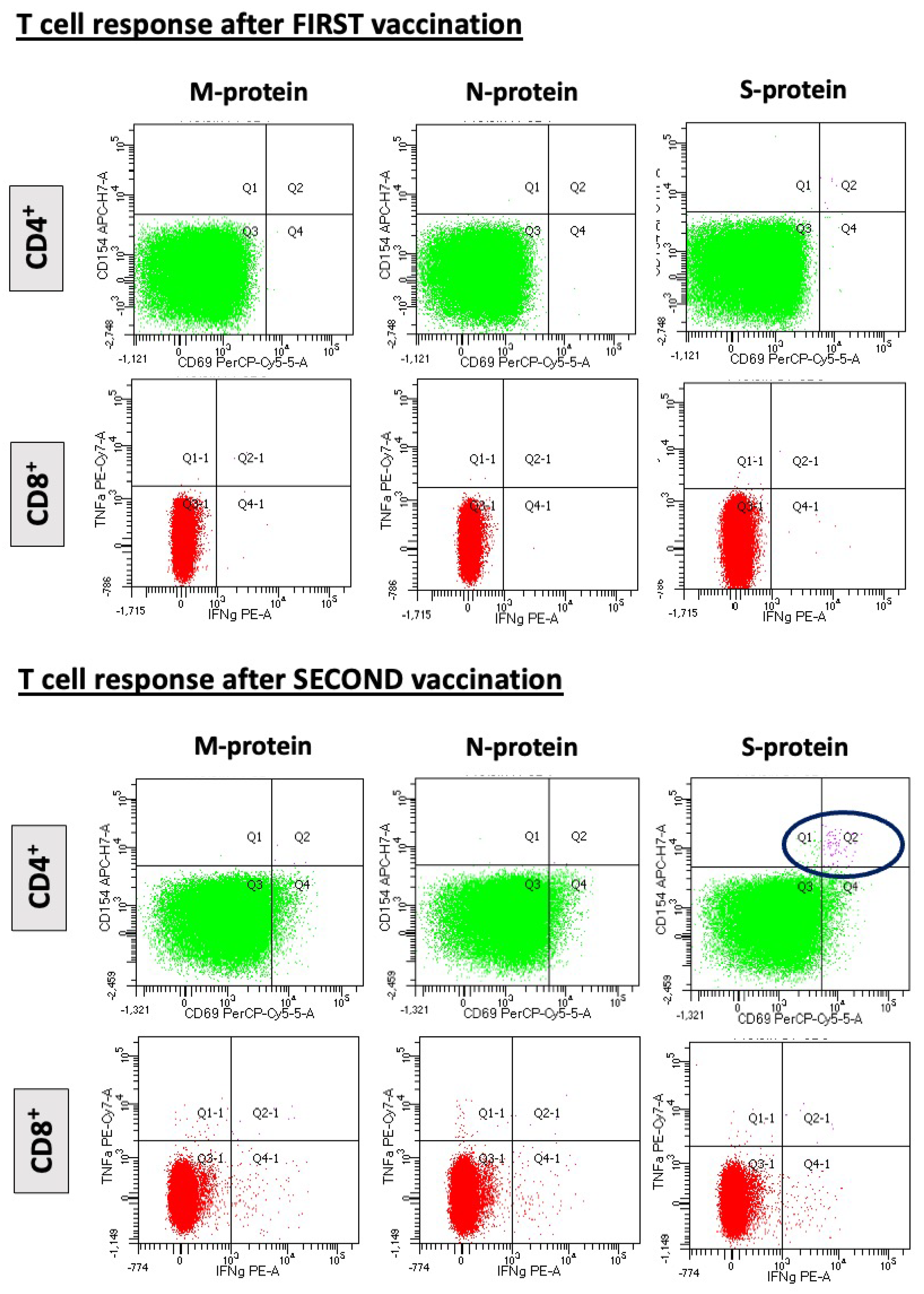
2.4. T-Cell Response
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Humoral and Cellular Immune Response after SARS-CoV-2 mRNA Vaccine
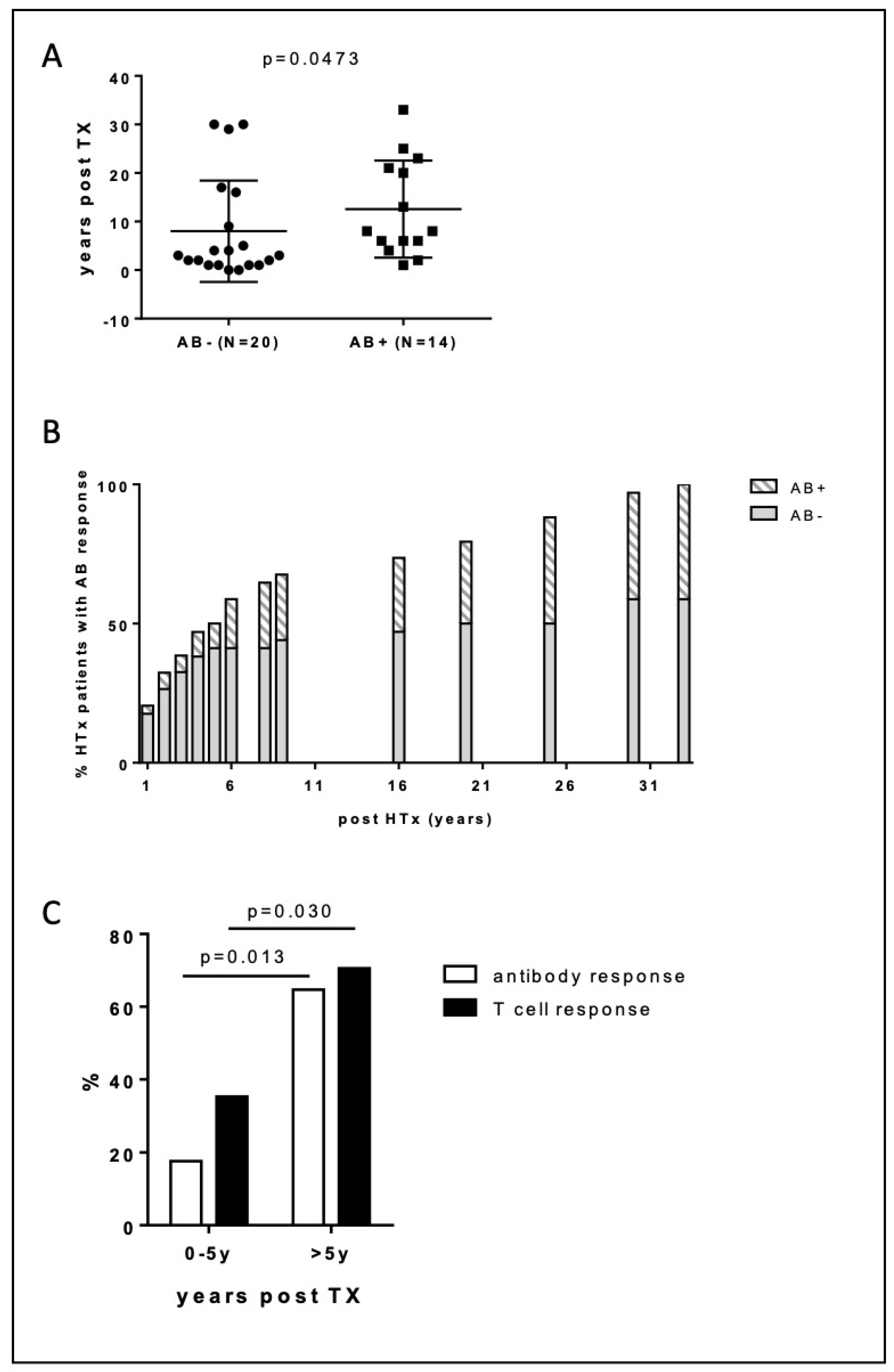
3.3. Responders vs. Non-Responders
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Latif, F.; Farr, M.A.; Clerkin, K.J.; Habal, M.V.; Takeda, K.; Naka, Y.; Restaino, S.; Sayer, G.; Uriel, N. Characteristics and Outcomes of Recipients of Heart Transplant with Coronavirus Disease 2019. JAMA Cardiol. 2020, 5, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Herrera, S.; Colmenero, J.; Pascal, M.; Escobedo, M.; Castel, M.A.; Sole-González, E.; Palou, E.; Egri, N.; Ruiz, P.; Mosquera, M.; et al. Cellular and Humoral Immune Response after MRNA-1273 SARS-CoV-2 Vaccine in Liver and Heart Transplant Recipients. Am. J. Transplant. 2021, 21, 3971–3979. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA J. Am. Med. Assoc. 2021, 325, 1784–1786. [Google Scholar] [CrossRef]
- Ben Zadok, O.I.; Shaul, A.A.; Ben-Avraham, B.; Yaari, V.; ben Zvi, H.; Shostak, Y.; Pertzov, B.; Eliakim-Raz, N.; Abed, G.; Abuhazira, M.; et al. Immunogenicity of the BNT162b2 MRNA Vaccine in Heart Transplant Recipients—A Prospective Cohort Study. Eur. J. Heart Fail. 2021, 23, 1555–1559. [Google Scholar] [CrossRef]
- Painter, M.M.; Mathew, D.; Goel, R.R.; Apostolidis, S.A.; Pattekar, A.; Kuthuru, O.; Baxter, A.E.; Herati, R.S.; Oldridge, D.A.; Gouma, S.; et al. Rapid Induction of Antigen-Specific CD4+ T Cells Guides Coordinated Humoral and Cellular Immune Responses to SARS-CoV-2 MRNA Vaccination. bioRxiv 2021. [Google Scholar] [CrossRef]
- Oberhardt, V.; Luxenburger, H.; Kemming, J.; Schulien, I.; Ciminski, K.; Giese, S.; Csernalabics, B.; Lang-Meli, J.; Janowska, I.; Staniek, J.; et al. Rapid and Stable Mobilization of CD8+ T Cells by SARS-CoV-2 MRNA Vaccine. Nature 2021, 597, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A.; et al. BNT162b2 Vaccine Induces Neutralizing Antibodies and Poly-Specific T Cells in Humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Malahe, S.R.K.; Hoek, R.A.S.; Dalm, V.A.S.H.; Broers, A.E.C.; den Hoed, C.M.; Manintveld, O.C.; Baan, C.C.; van Deuzen, C.M.; Papageorgiou, G.; Bax, H.I.; et al. Clinical Characteristics and Outcomes of Immunocompromised Patients With Coronavirus Disease 2019 Caused by the Omicron Variant: A Prospective, Observational Study. Clin. Infect. Dis. 2022; accepted. [Google Scholar] [CrossRef]
- Wurm, H.; Attfield, K.; Iversen, A.K.N.; Gold, R.; Fugger, L.; Haghikia, A. Recovery from COVID-19 in a B-Cell-Depleted Multiple Sclerosis Patient. Mult. Scler. J. 2020, 26, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Bange, E.M.; Han, N.A.; Wileyto, P.; Kim, J.Y.; Gouma, S.; Greenplate, A.R.; Porterfield, F.; Owoyemi, O.; Naik, K.; Galantino, M.; et al. CD8 T Cells Compensate for Impaired Humoral Immunity in COVID-19 Patients with Hematologic Cancer. Res. Sq. 2021; accepted. [Google Scholar] [CrossRef]
- Bange, E.M.; Han, N.A.; Wileyto, P.; Kim, J.Y.; Gouma, S.; Robinson, J.; Greenplate, A.R.; Hwee, M.A.; Porterfield, F.; Owoyemi, O.; et al. CD8+ T Cells Contribute to Survival in Patients with COVID-19 and Hematologic Cancer. Nat. Med. 2021, 27, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Angyal, A.; Longet, S.; Moore, S.C.; Payne, R.P.; Harding, A.; Tipton, T.; Rongkard, P.; Ali, M.; Hering, L.M.; Meardon, N.; et al. T-Cell and Antibody Responses to First BNT162b2 Vaccine Dose in Previously Infected and SARS-CoV-2-Naive UK Health-Care Workers: A Multicentre Prospective Cohort Study. Lancet Microbe 2022, 3, e21–e31. [Google Scholar] [CrossRef]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 MRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Alidjinou, E.K.; Demaret, J.; En Edicte Corroyer-Simovic, B.; Labreuche, J.; Goffard, A.; Trauet, J.; Lupau, D.; Miczek, S.; Vuotto, F.; Dendooven, A.; et al. Immunogenicity of BNT162b2 Vaccine Booster against SARS-CoV-2 Delta and Omicron Variants in Nursing Home Residents: A Prospective Observational Study in Older Adults Aged from 68 to 98 Years. Lancet Reg. Health Eur. 2022, 17, 100385. [Google Scholar] [CrossRef] [PubMed]
- Demaret, J.; Corroyer-Simovic, B.; Alidjinou, E.K.; Goffard, A.; Trauet, J.; Miczek, S.; Vuotto, F.; Dendooven, A.; Huvent-Grelle, D.; Podvin, J.; et al. Impaired Functional T-Cell Response to SARS-CoV-2 After Two Doses of BNT162b2 MRNA Vaccine in Older People. Front. Immunol. 2021, 12, 778679. [Google Scholar] [CrossRef] [PubMed]
- Zong, K.; Peng, D.; Yang, H.; Huang, Z.; Luo, Y.; Wang, Y.; Xiang, S.; Li, T.; Mou, T.; Wu, Z. Risk Factors for Weak Antibody Response of SARS-CoV-2 Vaccine in Adult Solid Organ Transplant Recipients: A Systemic Review and Meta-Analysis. Front. Immunol. 2022, 13, 888385. [Google Scholar] [CrossRef] [PubMed]
- Regele, F.; Heinzel, A.; Hu, K.; Raab, L.; Eskandary, F.; Faé, I.; Zelzer, S.; Böhmig, G.A.; Bond, G.; Fischer, G.; et al. Stopping of Mycophenolic Acid in Kidney Transplant Recipients for 2 Weeks Peri-Vaccination Does Not Increase Response to SARS-CoV-2 Vaccination—A Non-Randomized, Controlled Pilot Study. Front. Med. 2022, 9, 914424. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 34) | S-IgG Pos (n = 14) | S-IgG Neg (n = 20) | CD4 Pos (n = 18) | CD4 Neg (n = 16) | |
|---|---|---|---|---|---|
| Age (years) | 61 ± 11 | 59 ± 11 | 63 ± 10 | 60 ± 11 | 63 ± 11 |
| Male/Female (%) | 25 (74)/9 (26) | 8 (57)/6 (43) | 17 (85)/3 (15) | 11 (61)/7 (39) | 14 (88)/2 (13) |
| Time from HTx (years) | 10 ± 10 | 13 ± 10 | 8 ± 10 * | 11 ± 10 | 8 ± 11 |
| Blood draw post second vaccination (days) | 78 ± 27 | 76 ± 22 | 79 ± 30 | 83 ± 30 | 72 ± 22 |
| Medication | |||||
| CNI | |||||
| Tacrolimus | 23 (68) | 8 (57%) | 15 (75) | 10 (56%) | 12 (75%) |
| Ciclosporin | 12 (35) | 6 (43%) | 6 (30%) | 8 (44%) | 3 (19%) |
| MMF | 25 (74%) | 9 (64%) | 16 (80%) | 12 (67%) | 12 (75%) |
| CD4 positive | 18 (53) | 14 (100) | 4 (20) | / | / |
| AB positive | 14 (78) | / | / | 14 (78) | 0 (0) |
| Blood group | |||||
| A (%) | 18 (53) | 7 (50) | 11 (55) | 7 (39) | 11 (69) |
| B (%) | 2 (6) | 1 (7.1) | 1 (5) | 1 (6) | 1 (6) |
| O (%) | 12 (35) | 4 (28.6) | 8 (40) | 8 (44) | 4 (25) |
| AB (%) | 2 (6) | 2 (14.3) | 0 (0) | 2 (11) | 0 (0) |
| eGFR | 49 ± 18 | 54 ± 20 | 46 ± 15 | 52 ± 19 | 47 ± 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delrue, L.; Muylaert, A.; Beernaert, A.; De Pelsmaeker, I.; Boel, E.; Moya, A.; Verstreken, S.; Dierckx, R.; Heggermont, W.; Bartunek, J.; et al. T Cell and Antibody Response Following Double Dose of BNT162b2 mRNA Vaccine in SARS-CoV-2 Naïve Heart Transplant Recipients. Diagnostics 2022, 12, 2148. https://doi.org/10.3390/diagnostics12092148
Delrue L, Muylaert A, Beernaert A, De Pelsmaeker I, Boel E, Moya A, Verstreken S, Dierckx R, Heggermont W, Bartunek J, et al. T Cell and Antibody Response Following Double Dose of BNT162b2 mRNA Vaccine in SARS-CoV-2 Naïve Heart Transplant Recipients. Diagnostics. 2022; 12(9):2148. https://doi.org/10.3390/diagnostics12092148
Chicago/Turabian StyleDelrue, Leen, Annelies Muylaert, Ann Beernaert, Imke De Pelsmaeker, Elly Boel, Ana Moya, Sofie Verstreken, Riet Dierckx, Ward Heggermont, Jozef Bartunek, and et al. 2022. "T Cell and Antibody Response Following Double Dose of BNT162b2 mRNA Vaccine in SARS-CoV-2 Naïve Heart Transplant Recipients" Diagnostics 12, no. 9: 2148. https://doi.org/10.3390/diagnostics12092148