
How Significant Are Xpert Xpress SARS-CoV-2 Test Findings When Only an N2 Gene Is Detected?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Threshold for Positivity and Interpretation
2.3. Evaluating Agreement and Clinical Performance
3. Results
3.1. Concordance of the Xpert Test with the Standard qRT-PCR Test
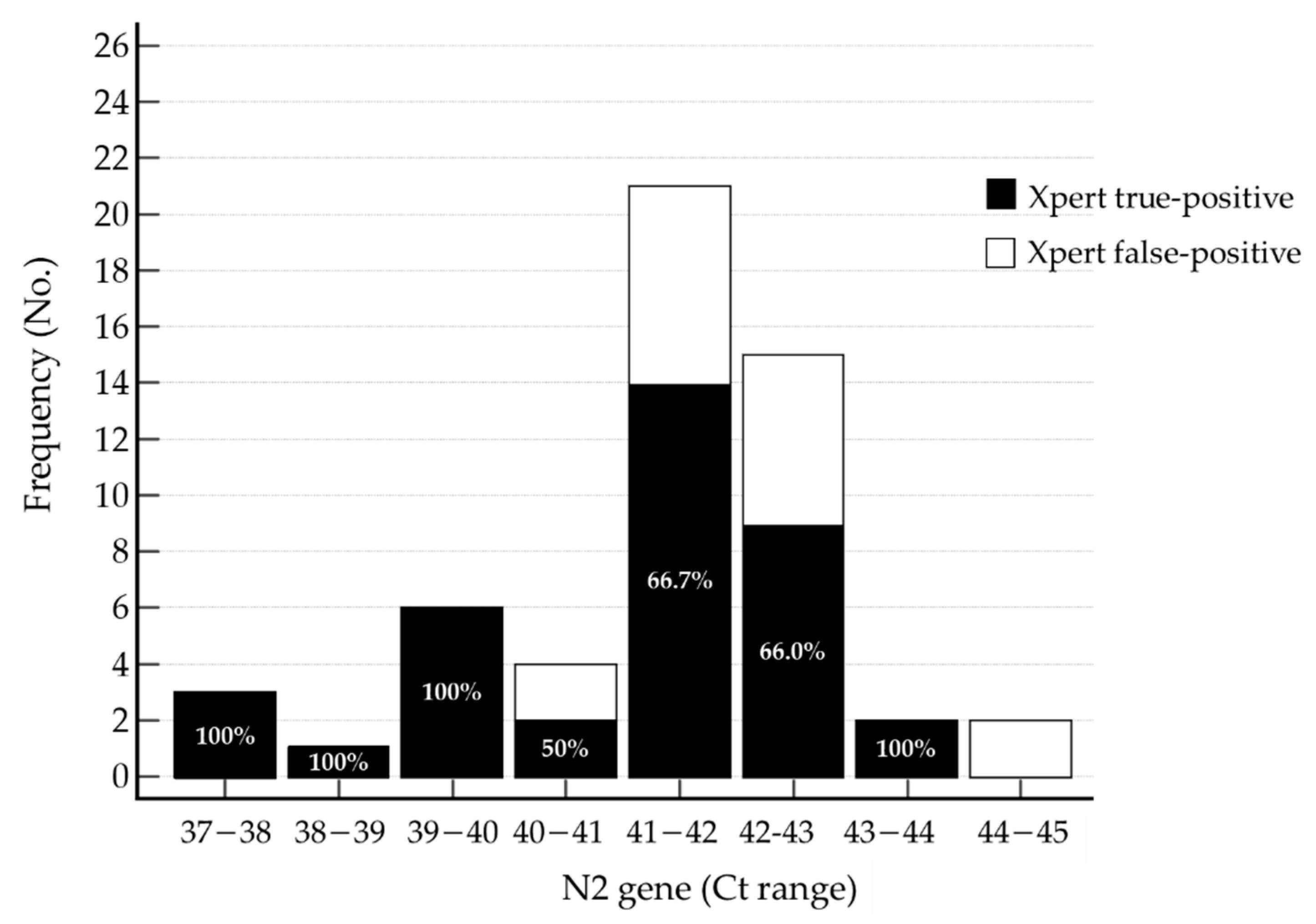
3.2. Evaluating True-Positive and False-Positive Xpert Test Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dugas, A.F.; Valsamakis, A.; Gaydos, C.A.; Forman, M.; Hardick, J.; Kidambi, P.; Amin, S.; Gupta, A.; Rothman, R.E. Evaluation of the Xpert Flu rapid PCR assay in high-risk emergency department patients. J. Clin. Microbiol. 2014, 52, 4353–4355. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, R.; Alahmari, A.; Ababtain, I.; Altamimi, A.; Alkhaldi, A.; Alhelail, M.; Alsalamah, M. The effect of COVID-19 on the characteristics of adult emergency department visits: A retrospective cohort tertiary hospital experience in Riyadh. J. Infect. Public Health 2022, 15, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Domingo, L.; Comas, M.; Jansana, A.; Louro, J.; Tizon-Marcos, H.; Cos, M.L.; Roquer, J.; Chillaron, J.J.; Cirera, I.; Pascual-Guardia, S.; et al. Impact of COVID-19 on hospital admissions and healthcare quality indicators in non-COVID patients: A retrospective study of the first COVID-19 year in a University Hospital in Spain. J. Clin. Med. 2022, 11, 1752. [Google Scholar] [CrossRef] [PubMed]
- Zhen, W.; Smith, E.; Manji, R.; Schron, D.; Berry, G.J. Clinical evaluation of three sample-to-answer platforms for detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58, 8. [Google Scholar] [CrossRef] [PubMed]
- Hinson, J.S.; Rothman, R.E.; Carroll, K.; Mostafa, H.H.; Ghobadi, K.; Smith, A.; Martinez, D.; Shaw-Saliba, K.; Klein, E.; Levin, S. Targeted rapid testing for SARS-CoV-2 in the emergency department is associated with large reductions in uninfected patient exposure time. J. Hosp. Infect. 2021, 107, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Lephart, P.R.; Bachman, M.A.; LeBar, W.; McClellan, S.; Barron, K.; Schroeder, L.; Newton, D.W. Comparative study of four SARS-CoV-2 Nucleic Acid Amplification Test (NAAT) platforms demonstrates that ID NOW performance is impaired substantially by patient and specimen type. Diagn. Microbiol. Infect. Dis. 2021, 99, 115200. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Song, J.U. Diagnostic accuracy of the Cepheid Xpert Xpress and the Abbott ID NOW assay for rapid detection of SARS-CoV-2: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 4523–4531. [Google Scholar] [CrossRef] [PubMed]
- Leli, C.; Di Matteo, L.; Gotta, F.; Cornaglia, E.; Vay, D.; Megna, I.; Pensato, R.E.; Boverio, R.; Rocchetti, A. Performance of a SARS-CoV-2 antigen rapid immunoassay in patients admitted to the emergency department. Int. J. Infect. Dis. 2021, 110, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Roh, K.H.; Hong, K.H.; Seong, M.W.; Ryoo, N.; Kim, H.S.; Lee, J.; Kim, S.Y.; Ryu, S.W.; Kim, M.N.; et al. COVID-19 molecular testing in korea: Practical essentials and answers from experts based on experiences of emergency use authorization assays. Ann. Lab. Med. 2020, 40, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Falasca, F.; Sciandra, I.; Di Carlo, D.; Gentile, M.; Deales, A.; Antonelli, G.; Turriziani, O. Detection of SARS-COV N2 Gene: Very low amounts of viral RNA or false positive? J. Clin. Virol. 2020, 133, 104660. [Google Scholar] [CrossRef] [PubMed]
- Cepheid. 2021. Xpert® Xpress SARS-CoV-2. Available online: https://www.fda.gov/media/136314/download (accessed on 8 August 2022).
- Ending Isolation and Precautions for People with COVID-19: Interim Guidance. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html (accessed on 20 June 2022).
- World Health Organization. Coronavirus disease (COVID-19): Symptoms. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_3 (accessed on 20 June 2022).
- Jerbi, L.; Azrad, M.; Peretz, A. Evaluation of factors that affect the performance of COVID-19 molecular assays including presence of symptoms, number of detected genes and RNA extraction type. Mol. Diagn. Ther. 2022, 26, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Khoshchehreh, M.; Wald-Dickler, N.; Holtom, P.; Butler-Wu, S.M. A needle in the haystack? Assessing the significance of envelope (E) gene-negative, nucleocapsid (N2) gene-positive SARS-CoV-2 detection by the Cepheid Xpert Xpress SARS-CoV-2 assay. J. Clin. Virol. 2020, 133, 104683. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Healthcare Providers Cepheid Xpert Xpress SARS-CoV-2. Available online: https://www.fda.gov/media/136313/download (accessed on 20 June 2022).
- Navarathna, D.H.; Sharp, S.; Lukey, J.; Arenas, M.; Villas, H.; Wiley, L.; Englett, I.; Juan, M.R.S.; Jinadatha, C. Understanding false positives and the detection of SARS-CoV-2 using the Cepheid Xpert Xpress SARS-CoV-2 and BD MAX SARS-CoV-2 assays. Diagn. Microbiol. Infect. Dis. 2021, 100, 115334. [Google Scholar] [CrossRef] [PubMed]
- Kanji, J.N.; Zelyas, N.; MacDonald, C.; Pabbaraju, K.; Khan, M.N.; Prasad, A.; Hu, J.; Diggle, M.; Berenger, B.M.; Tipples, G. False negative rate of COVID-19 PCR testing: A discordant testing analysis. Virol. J. 2021, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction-based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Long, D.R.; Gombar, S.; Hogan, C.A.; Greninger, A.L.; O’Reilly-Shah, V.; Bryson-Cahn, C.; Stevens, B.; Rustagi, A.; Jerome, K.R.; Kong, C.S.; et al. Occurrence and timing of subsequent severe acute respiratory syndrome Coronavirus 2 reverse-transcription polymerase chain reaction positivity among initially negative patients. Clin. Infect. Dis. 2021, 72, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Rakotosamimanana, N.; Randrianirina, F.; Randremanana, R.; Raherison, M.S.; Rasolofo, V.; Solofomalala, G.D.; Spiegel, A.; Heraud, J.M. GeneXpert for the diagnosis of COVID-19 in LMICs. Lancet Glob Health 2020, 8, e1457–e1458. [Google Scholar] [CrossRef]


{kind=link}
| % (No.) of Results on qRT-PCR | |||
|---|---|---|---|
| Positive | Inconclusive | Negative | |
| Xpert-positive with only an N2 signal | 16.7% (9/54) | 27.8% (15/54) | 55.5% (30/54) |
| Xpert-positive with both E and N2 signals | 96.5% (305/316) | 3.5% (11/316) | 0.0% (0/316) |
| Xpert-positive, total | 84.9% (314/370) | 7.0% (26/370) | 8.1% (30/370) |
| % (No.) of True-Positive Findings * | % (No.) of False-Positive Findings | |
|---|---|---|
| Xpert-positive with only an N2 signal | 68.5% (37/54) | 31.5% (17/54) |
| Xpert-positive with both E and N2 signals | 100.0% (316/316) | 0.0% (0/316) |
| Xpert-positive, total | 95.4% (353/370) | 4.6% (17/370) |
| qRT-PCR Results within Two Weeks after Xpert Testing | No Previous SARS-CoV-2 Infection History | Preconfirmed * | |
|---|---|---|---|
| At least one positive or inconclusive result | Total No. of individuals | 11 | 18 |
| No. (%) of symptomatic individuals † | 2 (18.2%) | 10 (55.6%) | |
| No positive results | Total No. of individuals | 17 ‡ | 8 |
| No. (%) of symptomatic individuals † | 2 (11.8%) | 3 (37.5%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, M.-K.; Chung, H.-S.; Lee, D.H.; Lee, M. How Significant Are Xpert Xpress SARS-CoV-2 Test Findings When Only an N2 Gene Is Detected? Diagnostics 2022, 12, 2133. https://doi.org/10.3390/diagnostics12092133
So M-K, Chung H-S, Lee DH, Lee M. How Significant Are Xpert Xpress SARS-CoV-2 Test Findings When Only an N2 Gene Is Detected? Diagnostics. 2022; 12(9):2133. https://doi.org/10.3390/diagnostics12092133
Chicago/Turabian StyleSo, Min-Kyung, Hae-Sun Chung, Duk Hee Lee, and Miae Lee. 2022. "How Significant Are Xpert Xpress SARS-CoV-2 Test Findings When Only an N2 Gene Is Detected?" Diagnostics 12, no. 9: 2133. https://doi.org/10.3390/diagnostics12092133