A 45-year-old male had suffered intermittent compressive left occipital headache radiating from the left shoulder for 5 years (10–15 days per month). His headache had worsened for a month (7/10 on the Visual Analog Scale). Brain computed tomography angiography showed severe stenosis at the orifice of the left vertebral artery (VA). A stent was inserted and the location of the balloon-mounted stent (Biotronik, Pro-kinteic Energy 5.0 × 13 mm) was confirmed under fluoroscopic guidance (
Figure 1a,b). Due to the atheroma of the VA ostium, the balloon-mounted stent (arrow) distally migrated during inflation because of the hardening plaque (
Figure 1c,d). It can be observed that the atheroma moved down from the VA origin as a result (Red block). An expansion of the narrowed left VA orifice (balloon angioplasty using Submarine 6–20) was confirmed, and the stent was positioned properly and VA flow improved (
Figure 1e,f). His headache improved in a few days without recurrence during the one-year follow-up. Vertebrobasilar insufficiency can cause headaches, although the mechanism is not understood. Bow hunter’s syndrome, which occurs due to the rotational compression of the VA, accompanies headaches in approximately 7–9% of cases [
1,
2]. Few reports also showed that headache often occurs in lateral medullary ischemia due to an atherothrombotic cause (52–73%) [
3,
4]. The chronic headache, reported and attributed to vertebrobasilar insufficiency in this study, rapidly improved after stent insertion for the left VA severe stenosis.
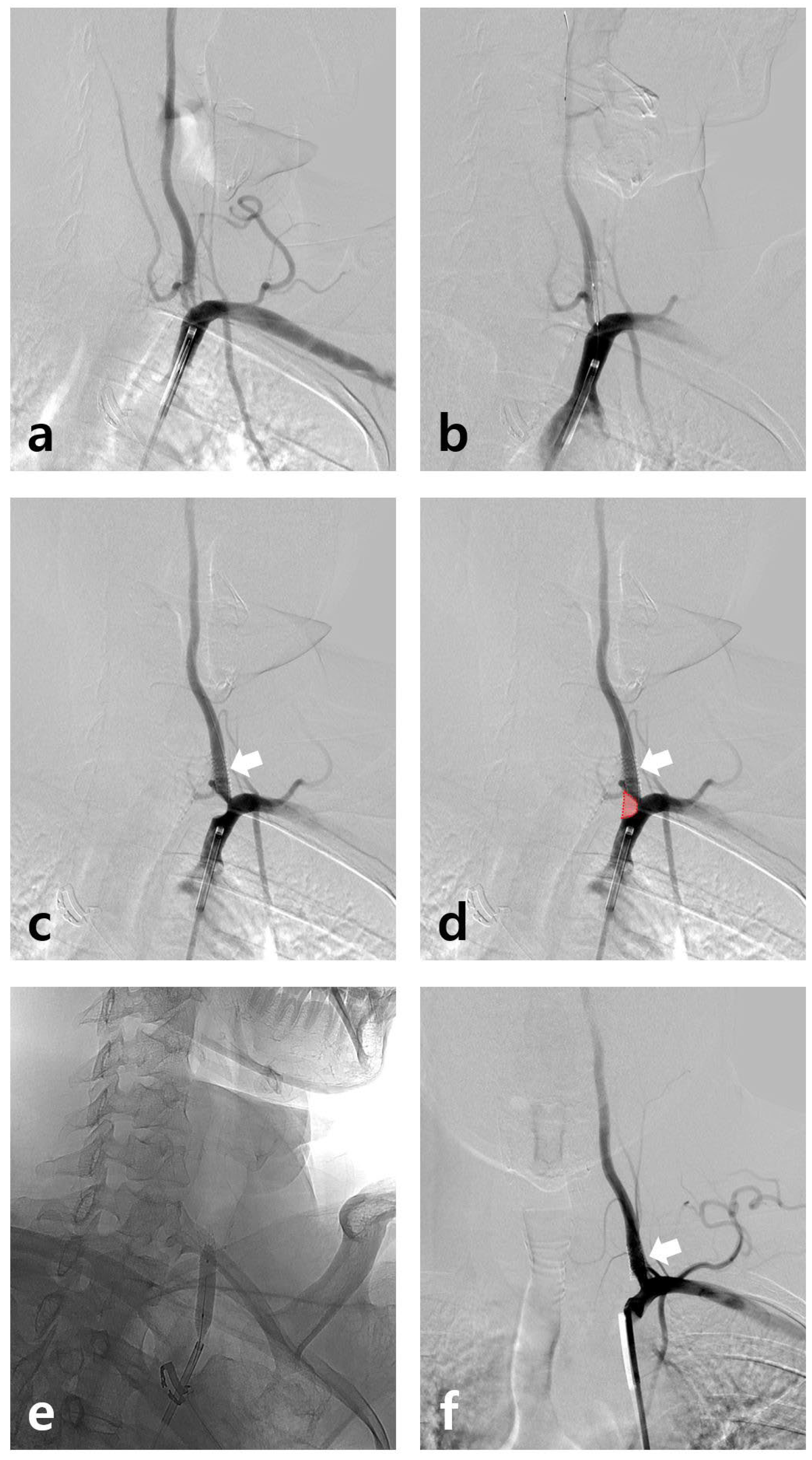
Figure 1.
(a) Stenosis from the left VA ostium confirmed on subclavian artery angiography. (b) The location of the balloon-mounted stent (Biotronik, Pro-kinteic Energy 5.0 × 13 mm) confirmed under fluoroscopic guidance. (c,d) Due to the atheroma of the VA ostium, the balloon-mounted stent (arrow) distally migrated during inflation. It can be observed that the atheroma moved down from the VA origin as a result (red block). (e) Additional balloon angioplasty using Submarine 6–20 was conducted in the ostium. (f) The stent is well-maintained (arrow) and VA flow improved.
Figure 1.
(a) Stenosis from the left VA ostium confirmed on subclavian artery angiography. (b) The location of the balloon-mounted stent (Biotronik, Pro-kinteic Energy 5.0 × 13 mm) confirmed under fluoroscopic guidance. (c,d) Due to the atheroma of the VA ostium, the balloon-mounted stent (arrow) distally migrated during inflation. It can be observed that the atheroma moved down from the VA origin as a result (red block). (e) Additional balloon angioplasty using Submarine 6–20 was conducted in the ostium. (f) The stent is well-maintained (arrow) and VA flow improved.
Author Contributions
Conceptualization, S.W.H., Y.S.K. and H.G.K.; methodology, E.J.Y.; software, E.J.Y.; validation, S.W.H. and Y.S.K.; investigation, S.W.H. and Y.S.K.; resources, S.W.H.; writing—original draft preparation, S.W.H. and Y.S.K.; writing—review and editing, H.G.K.; visualization, E.J.Y. and H.G.K.; supervision, H.G.K.; funding acquisition, H.G.K. All authors have read and agreed to the published version of the manuscript.
Funding
This paper was supported by Wonkwang Grant in 2022.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to restrictions eg privacy or ethical.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Zaidi, H.A.; Albuquerque, F.C.; Chowdhry, S.A.; Zabramski, J.M.; Ducruet, A.F.; Spetzler, R.F. Diagnosis and management of bow hunter’s syndrome: 15-year experience at barrow neurological institute. World Neurosurg. 2014, 82, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Jost, G.F.; Dailey, A.T. Bow hunter’s syndrome revisited: 2 new cases and literature review of 124 cases. Neurosurg. Focus 2015, 38, E7. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S. Pure lateral medullary infarction: Clinical-radiological correlation of 130 acute, consecutive patients. Brain 2003, 126, 1864–1872. [Google Scholar] [PubMed]
- Kuwabara, S.; Hirayama, K. Headache in lateral medullary infarction. J. Neurol. Neurosurg. Psychiatry 1995, 59, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
