
Role of Echocardiography in the Diagnosis and Interventional Management of Atrial Septal Defects


Abstract
:1. Introduction
2. Diagnosis
3. ASD Closure Methods
4. Patient Selection for Device Occlusion
5. Three-Dimensional Echocardiogram
6. TEE and ICE
7. Balloon Sizing
8. Device Occlusion
8.1. Amplatzer Septal Occluder
8.2. Gore HELEX® Device
8.3. Amplatzer Cribriform Device (ACD)
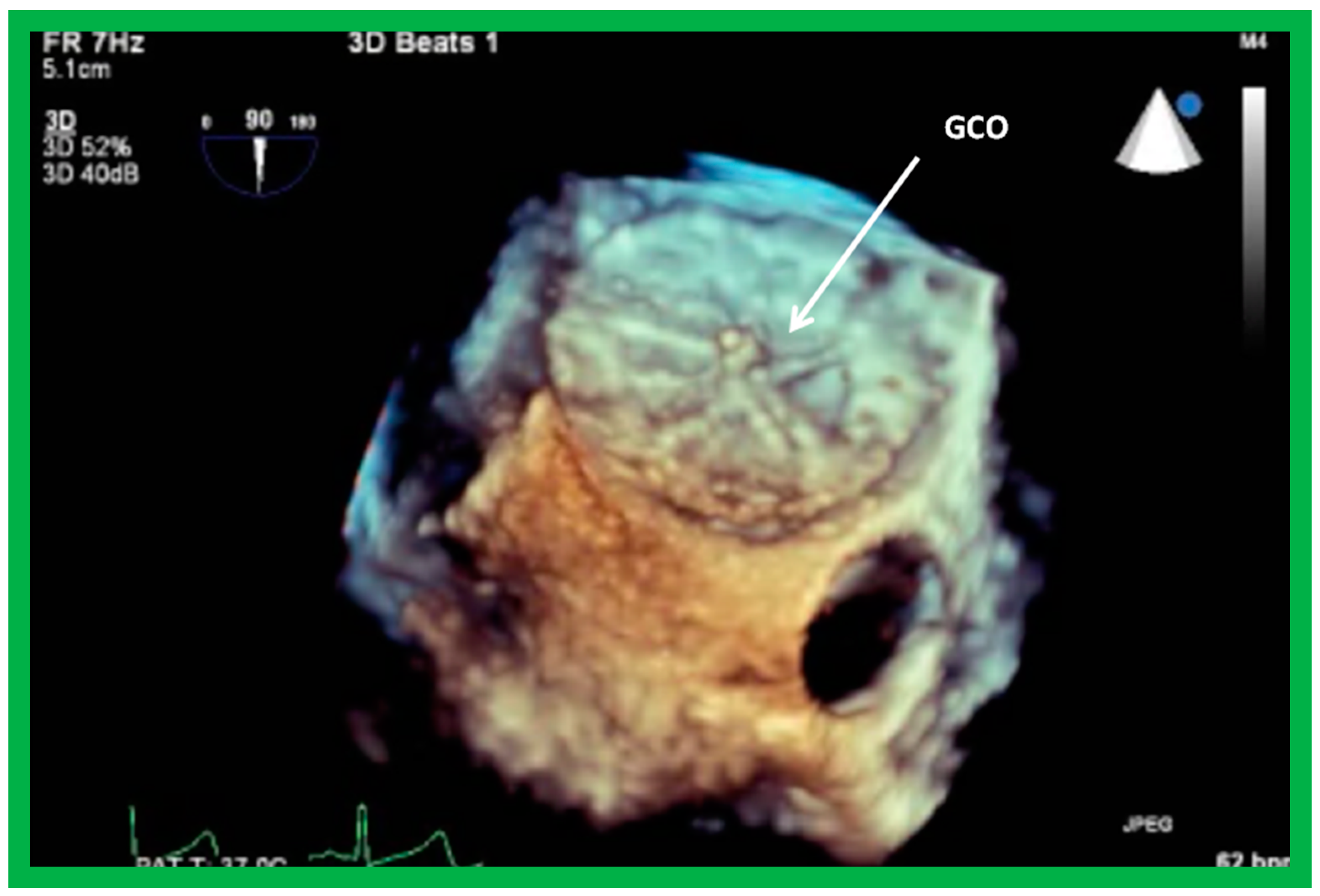
8.4. GORE® CARDIOFORMASD Occluder (GCO)
8.5. Septal Rims
8.6. Multiple Defects
9. Follow-Up after Device Occlusion
9.1. Ventricular Dimensions and Function
9.2. Device Position
9.3. Atrioventricular Valvar Function
9.4. Residual Shunts
9.5. Long-Term Effects
9.6. Obstruction of Systemic and Pulmonary Venous Drainage
9.7. Thrombus Formation
9.8. Device Migration
10. Summary and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References and Note
- Rao, P.S. Diagnosis and management of acyanotic heart disease: Part II—left-to-right shunt lesions. Indian J. Pediatr. 2005, 72, 503–512. [Google Scholar] [CrossRef]
- Rao, P.S. Congenital heart defects—A review. In Congenital Heart Disease—Selected Aspects; Rao, P.S., Ed.; InTech: Rijeka, Croatia, 2012; pp. 3–44, Chapter 1; ISBN 978-953-307-472-6. [Google Scholar]
- Rao, P.S. Atrial septal defect—A Review. In Atrial Septal Defect; Rao, P.S., Ed.; InTech: Rijeka, Croatia, 2012; pp. 3–20, Chapter 1; ISBN 978-953-51-0531-2. [Google Scholar]
- Rao, P.S. Atrial septal defect. In Pediatric Cardiology: How It Has Evolved over the Last 50 Years; Rao, P.S., Ed.; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2020; pp. 321–386. ISBN 9781527548886. [Google Scholar]
- Steele, P.M.; Fuster, V.; Cohen, M.; Ritter, D.G.; McGoon, D.C. Isolated atrial septal defect with pulmonary vascular obstructive disease--long-term follow-up and prediction of outcome after surgical correction. Circulation 1987, 76, 1037–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, P.S. Other acyanotic heart defects presenting in the neonate. In A Multidisciplinary Approach to Perinatal Cardiology; Rao, P.S., Vidyasagar, D., Eds.; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2021; Volume 2, pp. 615–654. ISBN 978-1-5275-6744-3. [Google Scholar]
- Rao, P.S. Non-surgical closure of atrial septal defects in children. In Atrial and Ventricular Septal Defects: Molecular Determinants, Impact of Environmental Factors and Non-Surgical Interventions; Larkin, S.A., Ed.; Nova Science Publishers, Inc.: New York, NY, USA, 2013; Softcover; ISBN 978-1-62618-326-1. [Google Scholar]
- Cockerham, J.T.; Martin, T.C.; Gutierrez, F.R.; Hartmann, A.F.; Goldring, D.; Strauss, A.W. Spontaneous closure of secundum atrial septal defect in infants and young children. Am. J. Cardiol. 1983, 52, 1267–1271. [Google Scholar] [CrossRef]
- Ghisla, R.P.; Hannon, D.W.; Meyer, R.A.; Kaplan, S. Spontaneous closure of isolated secundum atrial septal defects in infants: An echocardiographic study. Am. Heart J. 1985, 109, 1327–1333. [Google Scholar] [CrossRef]
- Kirklin, J.W.; Dushane, J.W.; Patrick, R.T.; Donald, D.E.; Hetzel, P.S.; Harshbarger, H.G.; Wood, E.H. Intracardiac surgery with the aid of a mechanical pump-oxygenator system (gibbon type): Report of eight cases. Proc. Staff. Meet. Mayo Clin. 1955, 30, 201–206. [Google Scholar]
- Kirklin, J.W.; Swan, H.J.; Wood, E.H.; Burchell, H.B.; Edwards, J.H. Anatomic, physiologic, and surgical considerations in repair of interatrial communications in man. J. Thorac. Surg. 1955, 29, 37–49; discussion 49–53. [Google Scholar]
- Rao, P.S. Present status of surgery in congenital heart disease. Indian J. Pediatr. 1981, 48, 349–364. [Google Scholar] [CrossRef]
- Chopra, P.S.; Rao, P.S. Surgical management of congenital heart disease: Current trends. Indian J. Pediatr. 1991, 58, 623–640. [Google Scholar]
- King, T.D.; Mills, N.L. Nonoperative closure of atrial septal defects. Surgery 1974, 75, 383–388. [Google Scholar]
- Rashkind, W.J. Experimental transvenous closure of atrial and ventricular septal defects. Circulation 1975, 52, II-8. [Google Scholar]
- Mills, N.L.; King, T.D. Nonoperative closure of left-to-right shunts. J. Thorac. Cardiovasc. Surg. 1976, 72, 371–378. [Google Scholar] [CrossRef]
- King, T.D.; Thompson, S.L.; Steiner, C.; Mills, N.L. Secundum atrial septal defect: Nonoperative closure during cardiac catheterization. J. Am. Med. Assoc. 1976, 235, 2506–2509. [Google Scholar] [CrossRef]
- Rashkind, W.J.; Cuaso, C.E. Transcatheter closure of atrial septal defects in children. Eur. J. Cardiol. 1977, 8, 119–120. [Google Scholar]
- Chopra, P.S.; Rao, P.S. History of the development of atrial septal occlusion devices. Curr. Interv. Cardiol. Rep. 2000, 2, 63–69. [Google Scholar]
- Rao, P.S. History of atrial septal occlusion devices. In Catheter Based Devices for Treatment of Noncoronary Cardiovascular Disease in Adults and Children; Rao, P.S., Kern, M.J., Eds.; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2003; pp. 3–9, Chapter 1. [Google Scholar]
- Alapati, S.; Rao, P.S. Historical aspects of trans-catheter occlusion of atrial septal defects. In Atrial Septal Defect; Rao, P.S., Ed.; InTech: Rijeka, Croatia, 2012; pp. 57–84, Chapter 5; ISBN 978-953-51-0531-2. [Google Scholar]
- Rao, P.S. History of trans-catheter interventions in pediatric cardiology. In Cardiac Catheterization and Imaging (From Pediatrics to Geriatrics); Vijayalakshmi, I.B., Ed.; Jaypee Publications: New Delhi, India, 2015; pp. 3–20, Chapter 1. [Google Scholar]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults with Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e81–e192. [Google Scholar] [CrossRef]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef]
- Rao, P.S.; Sideris, E.B.; Hausdort, G.; Rey, C.; Lloyd, T.R.; Beekman, R.H.; Worms, A.M.; Bourlon, F.; Onorato, E.; Khalilullah, M.; et al. International experience with secundum atrial septal defect occlusion by the buttoned device. Am. Heart J. 1994, 128, 1022–1035. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.S.; Wilson, A.D.; Levy, J.M.; Chopra, P.S. Role of “buttoned” double-disk device in the management of atrial septal defects. Am. Heart J. 1992, 123, 191–200. [Google Scholar] [CrossRef]
- Reddy, S.B.; Rao, P.; Ewenko, J.; Koscik, R.; Wilson, A.D. Echocardiographic predictors of success of catheter closure of atrial septal defect with the buttoned device. Am. Heart J. 1995, 129, 76–82. [Google Scholar] [CrossRef]
- Belohlavek, M.; Foley, D.A.; Gerber, T.C.; Greenleaf, J.F.; Seward, J.B. Three-dimentional ultrasound imaging of the atrial septum: Normal and pathologic anatomy. J. Am. Coll. Cardiol. 1993, 22, 1673–1678. [Google Scholar] [CrossRef] [Green Version]
- Marx, G.R.; Fulton, D.R.; Pandian, N.G.; Vogel, M.; Cao, Q.-L.; Ludomirsky, A.; Delabays, A.; Sugeng, L.; Klas, B. Delineation of site, relative size and dynamic geometry of atrial septal defects by real-time three-dimensional echocardiography. J. Am. Coll. Cardiol. 1995, 25, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.; Patel, H.T.; Pandain, N.G. Role of three-dimensional echocardiographic reconstruction in transcatheter occlusion of atrial septal defects. In Catheter Based Devices for Treatment of Noncoronary Cardiovascular Disease in Adults and Children; Rao, P.S., Kern, M.J., Eds.; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2003; pp. 133–141. [Google Scholar]
- Johri, A.M.; Witzke, C.; Solis, J.; Palacios, I.F.; Inglessis, I.; Picard, M.H.; Passeri, J.J. Real-Time Three-Dimensional Transesophageal Echocardiography in Patients with Secundum Atrial Septal Defects: Outcomes following Transcatheter Closure. J. Am. Soc. Echocardiogr. 2011, 24, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Deng, B.; Chen, K.; Huang, T.; Wei, Y.; Liu, Y.; Yang, L.; Qiu, Q.; Zheng, S.; Lv, H.; Wang, P.; et al. Assessment of atrial septal defect using 2D or real-time 3D transesophageal echocardiography and outcomes following transcatheter closure. Ann. Transl. Med. 2021, 9, 1309. [Google Scholar] [CrossRef] [PubMed]
- Roberson, D.A.; Cui, V.W. Three-dimensional Transesophageal Echocardiography of Atrial Septal Defect Device Closure. Curr. Cardiol. Rep. 2014, 16, 453. [Google Scholar] [CrossRef]
- Seo, J.-S.; Song, J.-M.; Kim, Y.-H.; Park, D.-W.; Lee, S.-W.; Kim, W.-J.; Kim, D.-H.; Kang, D.-H.; Song, J.-K. Effect of Atrial Septal Defect Shape Evaluated Using Three-Dimensional Transesophageal Echocardiography on Size Measurements for Percutaneous Closure. J. Am. Soc. Echocardiogr. 2012, 25, 1031–1040. [Google Scholar] [CrossRef]
- Hascoet, S.; Hadeed, K.; Marchal, P.; Dulac, Y.; Alacoque, X.; Heitz, F.; Acar, P. The relation between atrial septal defect shape, diameter, and area using three-dimensional transoesophageal echocardiography and balloon sizing during percutaneous closure in children. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Gillespie, M.J.; Javois, A.J.; Moore, P.; Forbes, T.; Paolillo, J.A.; for the GSO Investigator Group. Use of the GORE® CARDIOFORM Septal Occluder for percutaneous closure of secundum atrial septal defects: Results of the multicenter U.S. IDE trial. Catheter. Cardiovasc. Interv. 2020, 95, 1296–1304. [Google Scholar] [CrossRef]
- Rao, P.S. Outcomes of Device Closure of Atrial Septal Defects. Children 2020, 7, 111. [Google Scholar] [CrossRef]
- Contreras, A.E.; Ferrero-Guadagnoli, A.; Vilte, G.; Peirone, A. Is the 3D transesophageal Doppler color echocardiogram better than 2D to measure single defects of the interatrial septum in the catheterization laboratory? Arch. Cardiol. Mex. 2019, 89, 270–272. [Google Scholar] [CrossRef] [Green Version]
- Hellenbrand, W.E.; Fahey, J.T.; McGowan, F.X.; Weltin, G.G.; Kleinman, C.S. Transesophageal echocardiographic guidance of transcatheter closure of atrial septal defect. Am. J. Cardiol. 1990, 66, 207–213. [Google Scholar] [CrossRef]
- Singh, G.K.; Marino, C.; Rao, P.S. Ultrasound as an adjunct to cardiac intervention in the pediatric patient. J. Invasive Cardiol. 1996, 8, 341–349. [Google Scholar] [PubMed]
- Hijazi, Z.M.; Wang, Z.; Cao, Q.L.; Koenig, P.; Waight, D.; Lang, R. Transcatheter closure of atrial septal defects and patent foramen ovale under intracardiac echocardiographic guidance: Feasibility and comparison with transesophageal echocardiography. Cath. Cardiovasc. Interv. 2001, 52, 194–199. [Google Scholar] [CrossRef]
- Pedra, C.A.C.; Pedra, S.R.F.; Esteves, C.A.; Cassar, R.; Pontes, S.C.; Braga, S.L.N.; Fontes, V.F. Transcatheter closure of secundum atrial septal defects with complex anatomy. J. Invasive Cardiol. 2004, 16, 117–122. [Google Scholar] [PubMed]
- Podnar, T.; Martanovič, P.; Gavora, P.; Masura, J. Morphological variations of secundum-type atrial septal defects: Feasibility for percutaneous closure using Amplatzer septal occluders. Catheter. Cardiovasc. Interv. 2001, 53, 386–391. [Google Scholar] [CrossRef]
- King, T.D.; Thompson, S.L.; Mills, N.L. Measurement of atrial septal defect during cardiac catheterization: Experimental and clinical results. Am. J. Cardiol. 1978, 41, 537–542. [Google Scholar] [CrossRef]
- Sideris, E.B.; Rao, P.S. Transcatheter closure of atrial septal defects: Role of buttoned devices. J. Invasive Cardiol. 1996, 8, 289–296. [Google Scholar]
- Rao, P.; Langhough, R. Relationship of echocardiographic, shunt flow, and angiographic size to the stretched diameter of the atrial septal defect. Am. Heart J. 1991, 122, 505–508. [Google Scholar] [CrossRef]
- Rao, P.S.; Langhough, R.; Beekman, R.H.; Lloyd, T.R.; Sideris, E.B. Echocardiographic estimation of balloon-stretched diameter of secundum atrial septal defects for trans-catheter occlusion. Am. Heart J. 1992, 124, 172–175. [Google Scholar] [CrossRef] [Green Version]
- Carcagnì, A.; Presbitero, P. New echocardiographic diameter for Amplatzer sizing in adult patients with secundum atrial septal defect: Preliminary results. Catheter. Cardiovasc. Interv. 2004, 62, 409–414. [Google Scholar] [CrossRef]
- Nagm, A.M.; Rao, P.S. Percutaneous occlusion of complex atrial septal defects (Editorial). J. Invasive Cardiol. 2004, 16, 123–125. [Google Scholar]
- Rao, P.S. Techniques for closure of large atrial septal defects. Catheter. Cardiovasc. Interv. 2007, 70, 329–330. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.S. When and how should atrial septal defects be closed in adults. J. Invasive Cardiol. 2009, 21, 76–82. [Google Scholar]
- Berger, F.; Ewert, P.; Abdul-Khalid, H.; Nurnberg, J.H.; Lange, P.E. Percutaneous closure of large atrial septal defects with the Amplatzer septal occluder: Technical overkill or recommendable alternative treatment. J. Interv. Cardiol. 2001, 14, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Chessa, M.; Carminati, M.; Butera, G.; Bini, R.M.; Drago, M.; Rosti, L.; Giamberti, A.; Pomè, G.; Bossone, E.; Frigiola, A. Early and late complications associated with transcatheter occlusion of secundum atrial septal defect. J. Am. Coll. Cardiol. 2002, 39, 1061–1065. [Google Scholar] [CrossRef] [Green Version]
- Varma, C.; Benson, L.N.; Silversides, C.; Yip, J.; Warr, M.R.; Webb, G.; Siu, S.; McLaughlin, P.R. Outcomes and alternative techniques for device closure of the large secundum atrial septal defect. Catheter. Cardiovasc. Interv. 2003, 61, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.-D.; Hijazi, Z.M.; Kleinman, C.S.; Silverman, N.H.; Larntz, K. Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: Results of a multicenter nonrandomized trial. J. Am. Coll. Cardiol. 2002, 39, 1836–1844. [Google Scholar] [CrossRef] [Green Version]
- Mathewson, J.W.; Bichell, D.; Rothman, A.; Ing, F.F. Absent posteroinferior and antero-superior atrial septal defect rims: Factors affecting nonsurgical closure of large secundum defects using the Amplatzer occluder. J. Am. Soc. Echocardiogr. 2004, 17, 62–69. [Google Scholar] [CrossRef]
- Szkutnik, M.; Masura, J.; Bialkowski, J.; Gavora, P.; Banaszak, P.; Kusa, J.; Zembala, M. Transcatheter closure of double atrial septal defects with a single Amplatzer device. Catheter. Cardiovasc. Interv. 2004, 61, 237–241. [Google Scholar] [CrossRef]
- Pinto, R.J.; Dalvi, B. Closure of two atrial septal defects using two separate Amplatzer ASD devices. Indian Heart J. 2005, 57, 251–254. [Google Scholar]
- Cho, M.J.; Song, J.; Kim, S.-J.; Choi, E.Y.; Lee, S.Y.; Shim, W.S. Transcatheter Closure of Multiple Atrial Septal Defects with the Amplatzer Device. Korean Circ. J. 2011, 41, 549–551. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.S.; Ende, D.J.; Wilson, A.D.; Smith, P.A.; Chopra, P.S. Follow-up results of trans-catheter occlusion of atrial septal defect with buttoned device. Can. J. Cardiol. 1995, 11, 695–701. [Google Scholar] [PubMed]
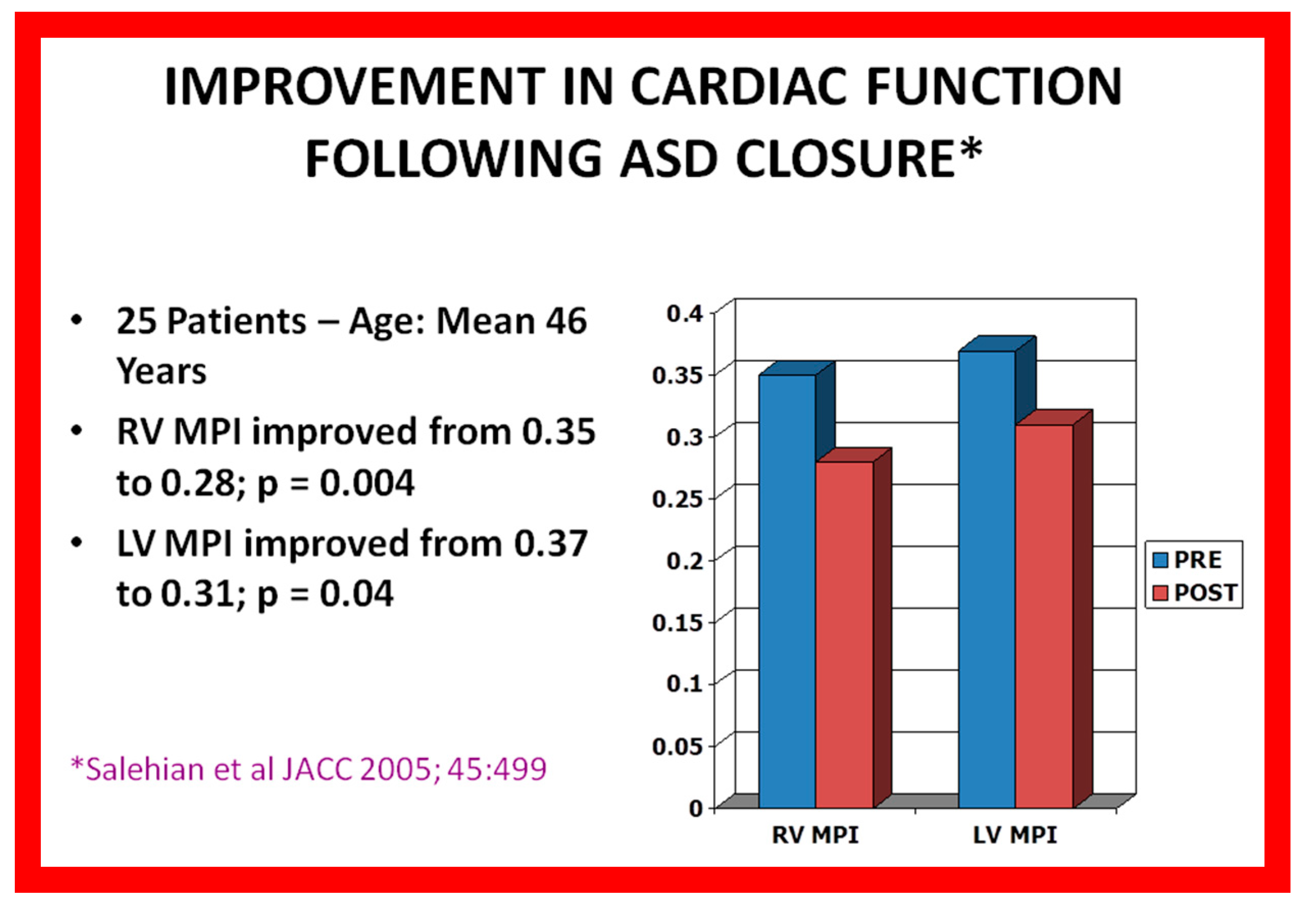
- Salehian, O.; Horlick, E.; Schwerzmann, M.; Haberer, K.; McLaughlin, P.; Siu, S.C.; Webb, G.; Therrien, J. Improvement in cardiac form and function after transcatheter closure of secundum atrial septal defects. J. Am. Coll. Cardiol. 2005, 45, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.S.; Sideris, E.B. Buttoned Device Closure of the Atrial Septal Defect. J. Interv. Cardiol. 1998, 11, 467–484. [Google Scholar] [CrossRef]
- Hartas, G.A.; Balaguru, D.; Brown, M.; Rao, P.S. Intermediate follow-up results of Amplatzer device occlusion of secundum atrial septal defects. In Proceedings of the 19th PICS-AICS 2015, Los Vegas, NV, USA, 18 September 2015; Volume 86, p. 574. [Google Scholar]
- Lloyd, T.R.; Rao, P.; Beekman, R.H.; Mendelsohn, A.M.; Sideris, E. Atrial septal defect occlusion with the buttoned device (a multi-institutional U.S. trial). Am. J. Cardiol. 1994, 73, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.S.; Berger, F.; Rey, C.; Haddad, J.; Meier, B.; Walsh, K.P.; Chandar, J.S.; Lloyd, T.R.; de Lezo, J.S.; Zamora, R.; et al. Results of transvenous occlusion of secundum atrial septal defects with 4th generation buttoned device: Comparison with 1st, 2nd and 3rd generation devices. J. Am. Coll. Cardiol. 2000, 36, 583–592. [Google Scholar] [CrossRef] [Green Version]
- Oster, M.; Bhatt, A.B.; Zaragoza-Macias, E.; Dendukuri, N.; Marelli, A. Interventional Therapy Versus Medical Therapy for Secundum Atrial Septal Defect: A Systematic Review (Part 2) for the 2018 AHA/ACC Guideline for the Management of Adults with Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e814–e830. [Google Scholar] [CrossRef]
- Moiduddin, N.; Cheatham, J.P.; Hoffman, T.M.; Phillips, A.B.; Kovalchin, J.P. Amplatzer Septal Occluder Associated with Late Pulmonary Venous Obstruction Requiring Surgical Removal with Acquired Aorta to Left Atrial Fistula. Am. J. Cardiol. 2009, 103, 1039–1040. [Google Scholar] [CrossRef]
- Hill, K.; Christian, K.; Kavanaugh-McHugh, A.; Doyle, T. Right-Sided Pulmonary Venous Obstruction Between a Right Aortic Arch and an Amplatzer Septal Occlusion Device Following Closure of a Secundum Atrial Septal Defect. Pediatr. Cardiol. 2009, 30, 855–857. [Google Scholar] [CrossRef]
- Aggoun, Y.; Gallet, B.; Acar, P.; Pulik, M.; Czitrom, D.; Lagier, A.; Laborde, F. Perforation of the aorta after percutaneous closure of an atrial septal defect with an Amplatz prosthesis, presenting with acute severe hemolysis. Arch. Mal. Coeur Vaiss. 2002, 95, 479–482. [Google Scholar]
- Chun, D.S.; Turrentine, M.W.; Moustapha, A.; Hoyer, M.H. Development of aorta-to-right atrial fistula following closure of secundum atrial septal defect using the Amplatzer septal occluder. Catheter. Cardiovasc. Interv. 2003, 58, 246–251. [Google Scholar] [CrossRef]
- Amin, Z.; Hijazi, Z.M.; Bass, J.L.; Cheatham, J.P.; Hellenbrand, W.E.; Kleinman, C.S. Erosion of Amplatzer septal occluder device after closure of secundum atrial septal defects: Review of registry of complications and recommendations to minimize future risk. Catheter. Cardiovasc. Interv. 2004, 63, 496–502. [Google Scholar] [CrossRef] [PubMed]
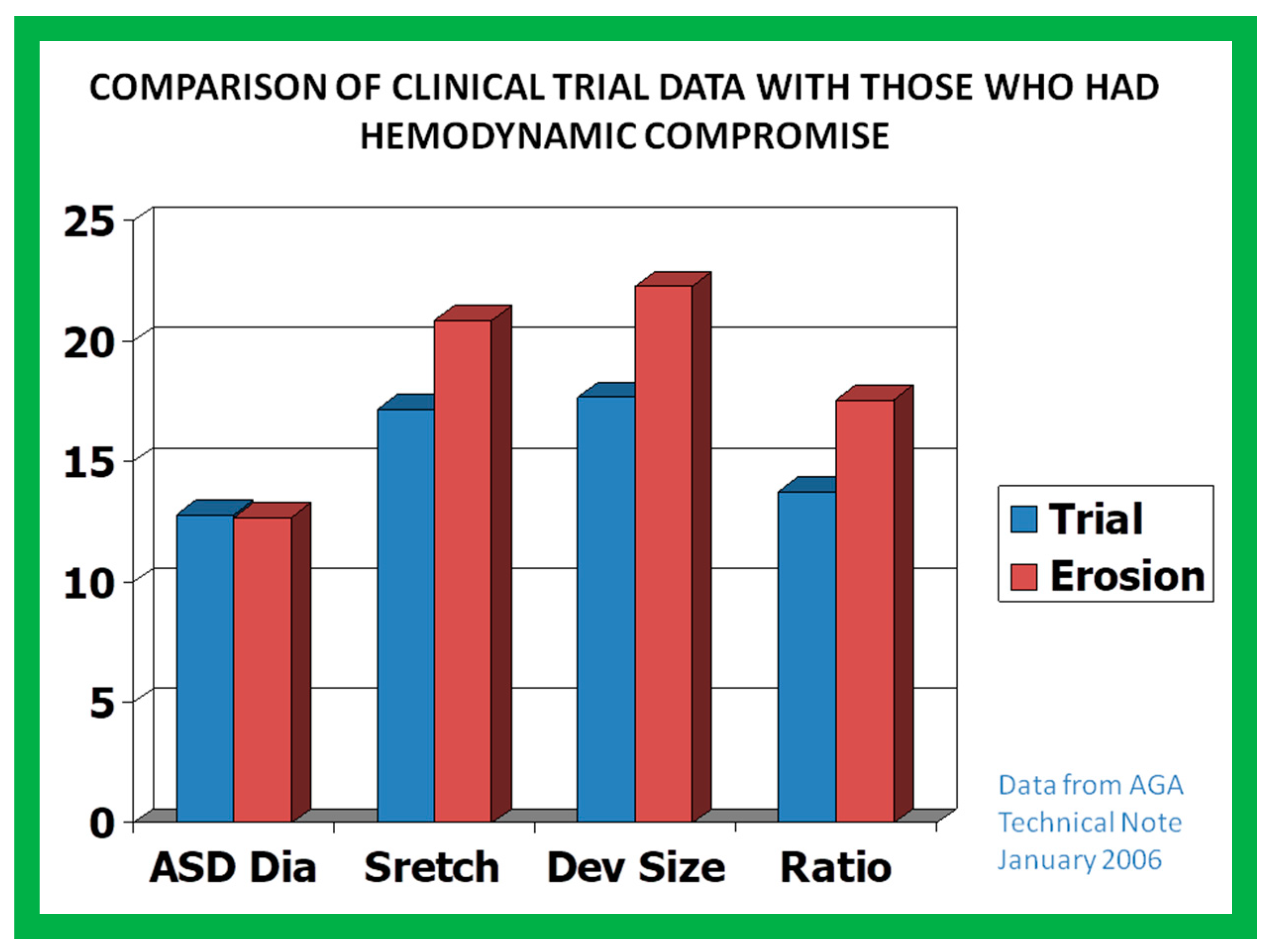
- AGA Medical Technical Note. January 2006; 1–4.
















































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Criteria |
|---|---|
| None | No defect by two-dimensional echo No color Doppler disturbance on right atrial side of device No RV volume overload * |
| Trivial | No defect by two-dimensional echo Minimal color disturbance on right atrial side of device (<l mm width at origin of color Doppler jet) No RV volume overload * |
| Small | No defect by two-dimensional echo 1 to 2 mm width of color Doppler jet, either in center or on periphery of device No RV volume overload * |
| Moderate | Defect visualized on two-dimensional echo >2 mm width of color jet RV volume overload * may be present |
| Large | Defect visualized by two-dimensional echo Large and/or multiple color Doppler jets RV volume overload * is present |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, P.S. Role of Echocardiography in the Diagnosis and Interventional Management of Atrial Septal Defects. Diagnostics 2022, 12, 1494. https://doi.org/10.3390/diagnostics12061494
Rao PS. Role of Echocardiography in the Diagnosis and Interventional Management of Atrial Septal Defects. Diagnostics. 2022; 12(6):1494. https://doi.org/10.3390/diagnostics12061494
Chicago/Turabian StyleRao, P. Syamasundar. 2022. "Role of Echocardiography in the Diagnosis and Interventional Management of Atrial Septal Defects" Diagnostics 12, no. 6: 1494. https://doi.org/10.3390/diagnostics12061494