
A Survey on Deep Learning for Precision Oncology



Abstract
:1. Introduction
2. Overview of Deep Learning in Precision Oncology
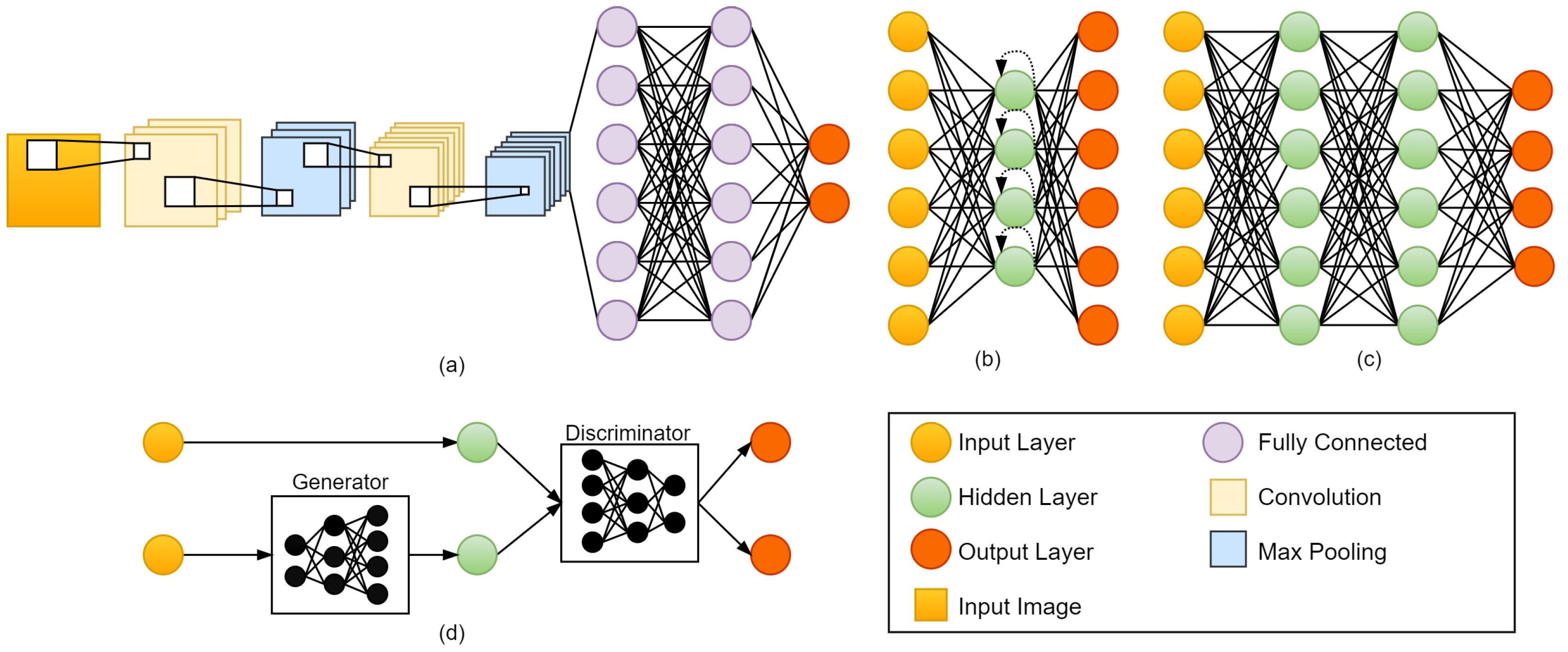
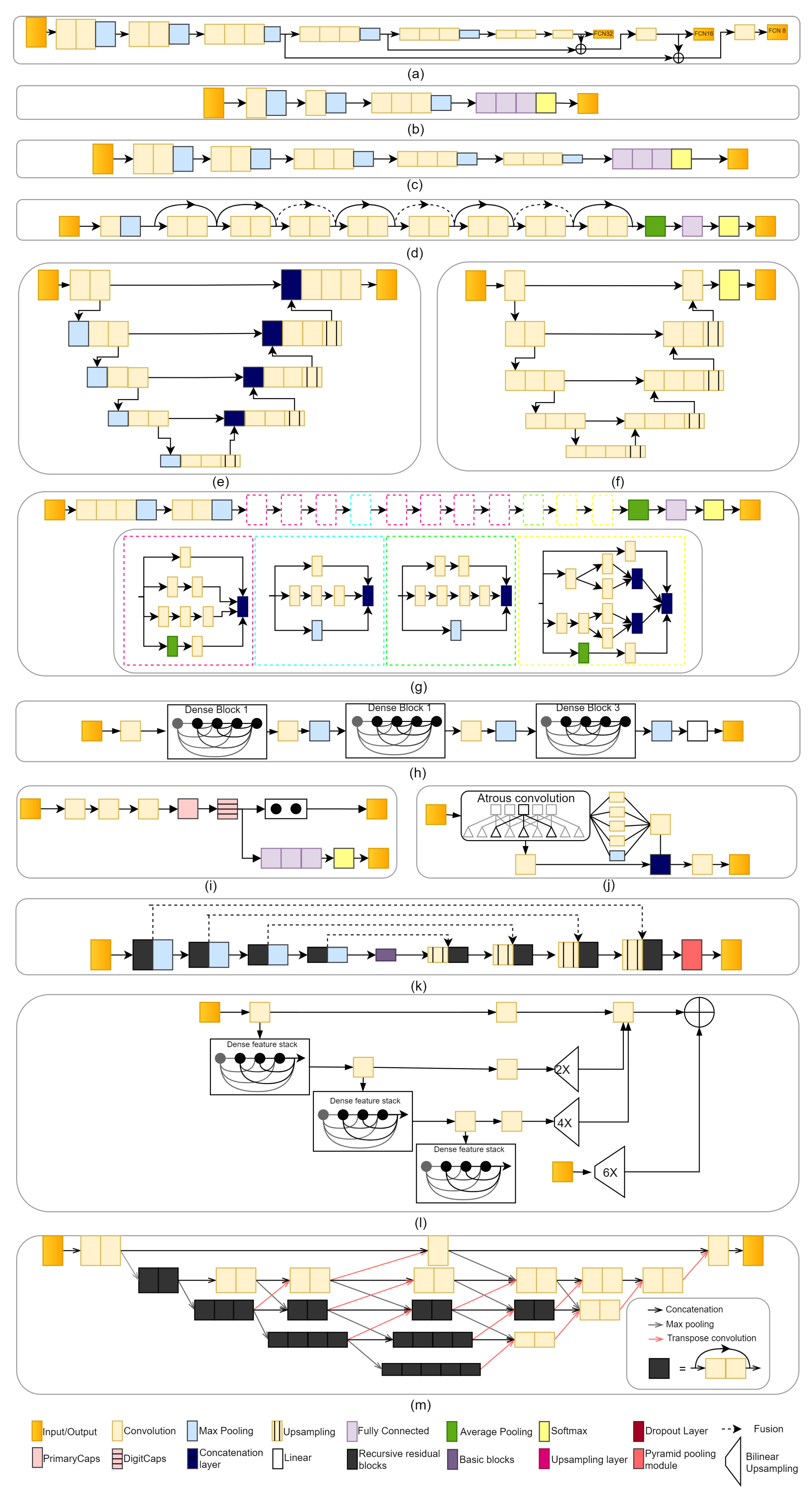
2.1. Convolutional Neural Network (CNN)
2.1.1. Fully Convolutional Network (FCN)
2.1.2. AlexNet
2.1.3. VGGNet
2.1.4. ResNet
2.1.5. U-Net
2.1.6. V-Net
2.1.7. GoogLeNet
2.1.8. DenseNet
2.1.9. CapsNet
2.1.10. DeepLab
2.1.11. RP-Net
2.1.12. Dense V-Network
2.1.13. BibNet
2.2. Recurrent Neural Network (RNN)
2.3. Deep Neural Network (DNN)
2.4. Generative Adversarial Network (GAN)
2.5. Other Methods
3. DL Methods by Applications
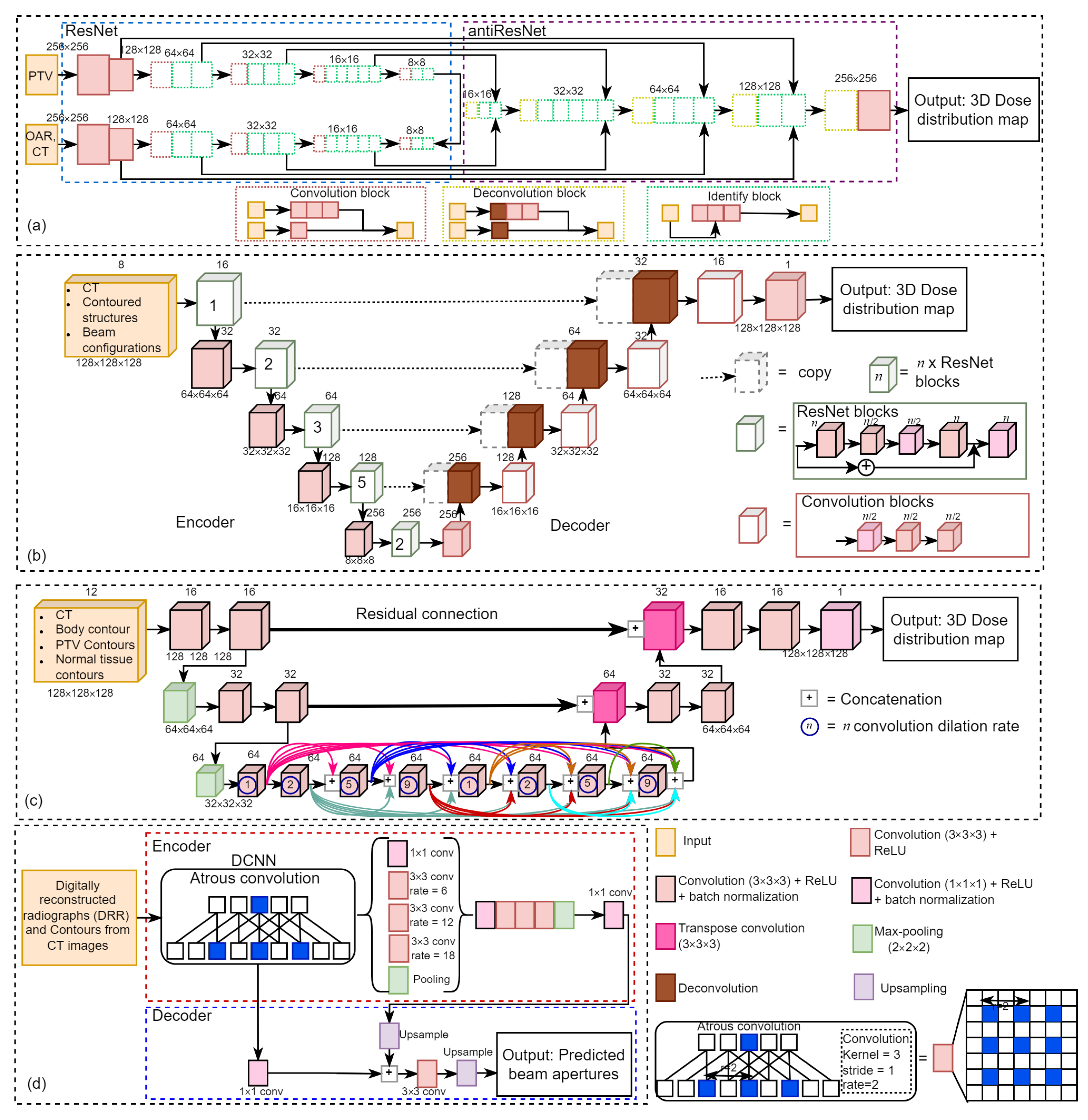
3.1. Dose Distribution for Treatment Planning of Radiotherapy
3.2. Survival Analysis and Risk Estimation after Treatment
3.3. Prediction of Treatment Response
3.4. Patient Stratification for Personalized Medicine
4. DL Methods by Anatomical Application Areas
4.1. Bladder
4.2. Brain
4.3. Breast
4.4. Bone
4.5. Cervix
4.6. Esophagus
4.7. Gastric
4.8. Head and Neck
4.9. Liver
4.10. Lung
4.11. Multi Cancer
4.12. Pelvic
4.13. Prostate
4.14. Rectum
4.15. Ovarian
4.16. Thyroid
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bode, A.M.; Dong, Z. Recent advances in precision oncology research. NPJ Precis. Oncol. 2018, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Kann, B.H.; Hosny, A.; Aerts, H.J. Artificial intelligence for clinical oncology. Cancer Cell 2021, 39, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhang, Q.; Lam, S.; Cai, J.; Yang, R. A review on application of deep learning algorithms in external beam radiotherapy automated treatment planning. Front. Oncol. 2020, 10, 2177. [Google Scholar] [CrossRef]
- Yu, J.; Goh, Y.; Song, K.J.; Kwak, J.; Cho, B.; Kim, S.S.; Lee, S.W.; Choi, E.K. Feasibility of automated planning for whole-brain radiation therapy using deep learning. J. Appl. Clin. Med. Phys. 2021, 22, 184–190. [Google Scholar] [CrossRef]
- Wei, J.; Cheng, J.; Gu, D.; Chai, F.; Hong, N.; Wang, Y.; Tian, J. Deep-learning-based radiomics predicts response to chemotherapy in colorectal liver metastases. Med. Phys. 2021, 48, 513–522. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, J.; Shen, L.; Chen, J.; Xia, L.; Ni, B.; Ge, L.; Wang, Y.; Lu, S. A multi-omics-based serial deep-learning approach to predict clinical outcomes of single-agent anti-PD-1/PD-L1 immunotherapy in advanced stage non-small-cell lung cancer. Am. J. Transl. Res. 2021, 13, 743. [Google Scholar] [PubMed]
- Lee, J.; An, J.Y.; Choi, M.G.; Park, S.H.; Kim, S.T.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, H.; et al. Deep learning–based survival analysis identified associations between molecular subtype and optimal adjuvant treatment of patients with gastric cancer. JCO Clin. Cancer Inform. 2018, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Mo, Z.; Zhu, W.; Liao, B.; Yang, Y.; Wu, F.X. Prediction of Target-Drug Therapy by Identifying Gene Mutations in Lung Cancer With Histopathological Stained Image and Deep Learning Techniques. Front. Oncol. 2021, 11, 901. [Google Scholar] [CrossRef]
- He, Y.; Guo, J.; Ding, X.; van Ooijen, P.; Zhang, Y.; Chen, A.; Oudkerk, M.; Xie, X. Convolutional neural network to predict the local recurrence of giant cell tumor of bone after curettage based on pre-surgery magnetic resonance images. Eur. Radiol. 2019, 29, 5441–5451. [Google Scholar] [CrossRef]
- Liu, Y.; Stojadinovic, S.; Hrycushko, B.; Wardak, Z.; Lau, S.; Lu, W.; Yan, Y.; Jiang, S.B.; Zhen, X.; Timmerman, R.; et al. A deep convolutional neural network-based automatic delineation strategy for multiple brain metastases stereotactic radiosurgery. PLoS ONE 2017, 12, e0185844. [Google Scholar] [CrossRef] [Green Version]
- Nie, D.; Zhang, H.; Adeli, E.; Liu, L.; Shen, D. 3D deep learning for multi-modal imaging-guided survival time prediction of brain tumor patients. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Athens, Greece, 17–21 October 2016; pp. 212–220. [Google Scholar]
- Cha, K.H.; Hadjiiski, L.M.; Samala, R.K.; Chan, H.P.; Cohan, R.H.; Caoili, E.M.; Paramagul, C.; Alva, A.; Weizer, A.Z. Bladder cancer segmentation in CT for treatment response assessment: Application of deep-learning convolution neural network—A pilot study. Tomography 2016, 2, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.H.; Hadjiiski, L.; Chan, H.P.; Weizer, A.Z.; Alva, A.; Cohan, R.H.; Caoili, E.M.; Paramagul, C.; Samala, R.K. Bladder cancer treatment response assessment in CT using radiomics with deep-learning. Sci. Rep. 2017, 7, 8738. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.; Hadjiiski, L.M.; Samala, R.K.; Chan, H.P.; Cha, K.H.; Richter, C.; Cohan, R.H.; Caoili, E.M.; Paramagul, C.; Alva, A.; et al. Deep-learning approach for assessment of bladder cancer treatment response. Tomography 2019, 5, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Andres, E.A.; Fidon, L.; Vakalopoulou, M.; Lerousseau, M.; Carré, A.; Sun, R.; Klausner, G.; Ammari, S.; Benzazon, N.; Reuzé, S.; et al. Dosimetry-driven quality measure of brain pseudo computed tomography generated from deep learning for MRI-only radiation therapy treatment planning. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 813–823. [Google Scholar] [CrossRef]
- Han, E.Y.; Cardenas, C.E.; Nguyen, C.; Hancock, D.; Xiao, Y.; Mumme, R.; Court, L.E.; Rhee, D.J.; Netherton, T.J.; Li, J.; et al. Clinical implementation of automated treatment planning for whole-brain radiotherapy. J. Appl. Clin. Med. Phys. 2021, 22, 94–102. [Google Scholar] [CrossRef]
- Jalalifar, A.; Soliman, H.; Sahgal, A.; Sadeghi-Naini, A. A Cascaded Deep-Learning Framework for Segmentation of Metastatic Brain Tumors Before and After Stereotactic Radiation Therapy. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1063–1066. [Google Scholar]
- Kazemifar, S.; McGuire, S.; Timmerman, R.; Wardak, Z.; Nguyen, D.; Park, Y.; Jiang, S.; Owrangi, A. MRI-only brain radiotherapy: Assessing the dosimetric accuracy of synthetic CT images generated using a deep-learning approach. Radiother. Oncol. 2019, 136, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Kazemifar, S.; Barragán Montero, A.M.; Souris, K.; Rivas, S.T.; Timmerman, R.; Park, Y.K.; Jiang, S.; Geets, X.; Sterpin, E.; Owrangi, A. Dosimetric evaluation of synthetic CT generated with GANs for MRI-only proton therapy treatment planning of brain tumors. J. Appl. Clin. Med. Phys. 2020, 21, 76–86. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Li, Y.; Qin, W.; Liang, X.; Xu, J.; Xiong, J.; Xie, Y. Magnetic resonance image (MRI) synthesis from brain computed tomography (CT) images based on deep-learning methods for magnetic resonance (MR)-guided radiotherapy. Quant. Imaging Med. Surg. 2020, 10, 1223. [Google Scholar] [CrossRef]
- Maspero, M.; Bentvelzen, L.G.; Savenije, M.H.; Guerreiro, F.; Seravalli, E.; Janssens, G.O.; van den Berg, C.A.; Philippens, M.E. Deep-learning-based synthetic CT generation for paediatric brain MR-only photon and proton radiotherapy. Radiother. Oncol. 2020, 153, 197–204. [Google Scholar] [CrossRef]
- Wang, T.; Lei, Y.; Tian, S.; Jiang, X.; Zhou, J.; Liu, T.; Dresser, S.; Curran, W.J.; Shu, H.K.; Yang, X. Learning-based automatic segmentation of arteriovenous malformations on contrast CT images in brain stereotactic radiosurgery. Med. Phys. 2019, 46, 3133–3141. [Google Scholar] [CrossRef]
- Yoon, H.G.; Cheon, W.; Jeong, S.W.; Kim, H.S.; Kim, K.; Nam, H.; Han, Y.; Lim, D.H. Multi-parametric deep-learning model for prediction of overall survival after postoperative concurrent chemoradiotherapy in glioblastoma patients. Cancers 2020, 12, 2284. [Google Scholar] [CrossRef] [PubMed]
- Bakx, N.; Bluemink, H.; Hagelaar, E.; van der Sangen, M.; Theuws, J.; Hurkmans, C. Development and evaluation of radiotherapy deep learning dose prediction models for breast cancer. Phys. Imaging Radiat. Oncol. 2021, 17, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Byra, M.; Dobruch-Sobczak, K.; Klimonda, Z.; Piotrzkowska-Wroblewska, H.; Litniewski, J. Early prediction of response to neoadjuvant chemotherapy in breast cancer sonography using Siamese convolutional neural networks. IEEE J. Biomed. Health Inform. 2020, 25, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Chen, M.; Lu, W.; Zhao, B.; Jiang, S.; Zhou, L.; Kim, N.; Spangler, A.; Rahimi, A.; Zhen, X.; et al. Deep-learning based surface region selection for deep inspiration breath hold (DIBH) monitoring in left breast cancer radiotherapy. Phys. Med. Biol. 2018, 63, 245013. [Google Scholar] [CrossRef]
- El Adoui, M.; Drisis, S.; Benjelloun, M. Multi-input deep-learning architecture for predicting breast tumor response to chemotherapy using quantitative MR images. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1491–1500. [Google Scholar] [CrossRef]
- Gernaat, S.A.; van Velzen, S.G.; Koh, V.; Emaus, M.J.; Išgum, I.; Lessmann, N.; Moes, S.; Jacobson, A.; Tan, P.W.; Grobbee, D.E.; et al. Automatic quantification of calcifications in the coronary arteries and thoracic aorta on radiotherapy planning CT scans of Western and Asian breast cancer patients. Radiother. Oncol. 2018, 127, 487–492. [Google Scholar] [CrossRef]
- Ha, R.; Chin, C.; Karcich, J.; Liu, M.Z.; Chang, P.; Mutasa, S.; Pascual Van Sant, E.; Wynn, R.T.; Connolly, E.; Jambawalikar, S. Prior to initiation of chemotherapy, can we predict breast tumor response? Deep learning convolutional neural networks approach using a breast MRI tumor dataset. J. Digit. Imaging 2019, 32, 693–701. [Google Scholar] [CrossRef]
- Jiang, M.; Li, C.L.; Luo, X.M.; Chuan, Z.R.; Lv, W.Z.; Li, X.; Cui, X.W.; Dietrich, C.F. Ultrasound-based deep learning radiomics in the assessment of pathological complete response to neoadjuvant chemotherapy in locally advanced breast cancer. Eur. J. Cancer 2021, 147, 95–105. [Google Scholar] [CrossRef]
- Qu, Y.H.; Zhu, H.T.; Cao, K.; Li, X.T.; Ye, M.; Sun, Y.S. Prediction of pathological complete response to neoadjuvant chemotherapy in breast cancer using a deep learning (DL) method. Thorac. Cancer 2020, 11, 651–658. [Google Scholar] [CrossRef] [Green Version]
- Schreier, J.; Attanasi, F.; Laaksonen, H. A full-image deep segmenter for CT images in breast cancer radiotherapy treatment. Front. Oncol. 2019, 9, 677. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.W.; Huang, S.C.; Lee, Y.C.; Shen, Y.J.; Meng, S.I.; Gaol, J.L. Deep learning for bone marrow cell detection and classification on whole-slide images. Med. Image Anal. 2022, 75, 102270. [Google Scholar] [CrossRef] [PubMed]
- Jihong, C.; Penggang, B.; Xiuchun, Z.; Kaiqiang, C.; Wenjuan, C.; Yitao, D.; Jiewei, Q.; Kerun, Q.; Jing, Z.; Tianming, W. Automated Intensity Modulated Radiation Therapy Treatment Planning for Cervical Cancer Based on Convolution Neural Network. Technol. Cancer Res. Treat. 2020, 19, 1533033820957002. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, B.; Anderson, B.M.; Zhiqian, H.Y.; Gobeli, M.; Cazoulat, G.; Söderberg, J.; Samuelsson, E.; Lidberg, D.; Ward, C.; Taku, N.; et al. Automatic segmentation using deep learning to enable online dose optimization during adaptive radiation therapy of cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1096–1110. [Google Scholar] [CrossRef] [PubMed]
- Zaffino, P.; Pernelle, G.; Mastmeyer, A.; Mehrtash, A.; Zhang, H.; Kikinis, R.; Kapur, T.; Spadea, M.F. Fully automatic catheter segmentation in MRI with 3D convolutional neural networks: Application to MRI-guided gynecologic brachytherapy. Phys. Med. Biol. 2019, 64, 165008. [Google Scholar] [CrossRef]
- Wang, C.W.; Liou, Y.A.; Lin, Y.J.; Chang, C.C.; Chu, P.H.; Lee, Y.C.; Wang, C.H.; Chao, T.K. Artificial intelligence-assisted fast screening cervical high grade squamous intraepithelial lesion and squamous cell carcinoma diagnosis and treatment planning. Sci. Rep. 2021, 11, 16244. [Google Scholar] [CrossRef]
- Hu, Y.; Xie, C.; Yang, H.; Ho, J.W.; Wen, J.; Han, L.; Lam, K.O.; Wong, I.Y.; Law, S.Y.; Chiu, K.W.; et al. Computed tomography-based deep-learning prediction of neoadjuvant chemoradiotherapy treatment response in esophageal squamous cell carcinoma. Radiother. Oncol. 2021, 154, 6–13. [Google Scholar] [CrossRef]
- Jiang, D.; Li, T.; Mao, R.; Du, C.; Liu, J. Deep Learning Based Dosimetry Evaluation at Organs-at-Risk in Esophageal Radiation Treatment Planning. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 868–871. [Google Scholar]
- Jiang, D.; Yan, H.; Chang, N.; Li, T.; Mao, R.; Du, C.; Guo, B.; Liu, J. Convolutional neural network-based dosimetry evaluation of esophageal radiation treatment planning. Med. Phys. 2020, 47, 4735–4742. [Google Scholar] [CrossRef]
- Zhang, L.; Dong, D.; Zhang, W.; Hao, X.; Fang, M.; Wang, S.; Li, W.; Liu, Z.; Wang, R.; Zhou, J.; et al. A deep learning risk prediction model for overall survival in patients with gastric cancer: A multicenter study. Radiother. Oncol. 2020, 150, 73–80. [Google Scholar] [CrossRef]
- Chen, T.; Liu, S.; Li, Y.; Feng, X.; Xiong, W.; Zhao, X.; Yang, Y.; Zhang, C.; Hu, Y.; Chen, H.; et al. Developed and validated a prognostic nomogram for recurrence-free survival after complete surgical resection of local primary gastrointestinal stromal tumors based on deep learning. EBioMedicine 2019, 39, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Cardenas, C.E.; Beadle, B.M.; Garden, A.S.; Skinner, H.D.; Yang, J.; Rhee, D.J.; McCarroll, R.E.; Netherton, T.J.; Gay, S.S.; Zhang, L.; et al. Generating High-Quality Lymph Node Clinical Target Volumes for Head and Neck Cancer Radiation Therapy Using a Fully Automated Deep Learning-Based Approach. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 801–812. [Google Scholar] [CrossRef]
- Chen, X.; Men, K.; Li, Y.; Yi, J.; Dai, J. A feasibility study on an automated method to generate patient-specific dose distributions for radiotherapy using deep learning. Med. Phys. 2019, 46, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamant, A.; Chatterjee, A.; Vallières, M.; Shenouda, G.; Seuntjens, J. Deep learning in head & neck cancer outcome prediction. Sci. Rep. 2019, 9, 2764. [Google Scholar]
- Dinkla, A.M.; Florkow, M.C.; Maspero, M.; Savenije, M.H.; Zijlstra, F.; Doornaert, P.A.; van Stralen, M.; Philippens, M.E.; van den Berg, C.A.; Seevinck, P.R. Dosimetric evaluation of synthetic CT for head and neck radiotherapy generated by a patch-based three-dimensional convolutional neural network. Med. Phys. 2019, 46, 4095–4104. [Google Scholar] [CrossRef]
- Fan, J.; Wang, J.; Chen, Z.; Hu, C.; Zhang, Z.; Hu, W. Automatic treatment planning based on three-dimensional dose distribution predicted from deep learning technique. Med. Phys. 2019, 46, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Fujima, N.; Andreu-Arasa, V.C.; Meibom, S.K.; Mercier, G.A.; Salama, A.R.; Truong, M.T.; Sakai, O. Deep learning analysis using FDG-PET to predict treatment outcome in patients with oral cavity squamous cell carcinoma. Eur. Radiol. 2020, 30, 6322–6330. [Google Scholar] [CrossRef] [PubMed]
- Gronberg, M.P.; Gay, S.S.; Netherton, T.J.; Rhee, D.J.; Court, L.E.; Cardenas, C.E. Dose prediction for head and neck radiotherapy using a three-dimensional dense dilated U-net architecture. Med. Phys. 2021, 48, 5567–5573. [Google Scholar] [CrossRef]
- Gurney-Champion, O.J.; Kieselmann, J.P.; Wong, K.H.; Ng-Cheng-Hin, B.; Harrington, K.; Oelfke, U. A convolutional neural network for contouring metastatic lymph nodes on diffusion-weighted magnetic resonance images for assessment of radiotherapy response. Phys. Imaging Radiat. Oncol. 2020, 15, 1–7. [Google Scholar] [CrossRef]
- Ibragimov, B.; Xing, L. Segmentation of organs-at-risks in head and neck CT images using convolutional neural networks. Med. Phys. 2017, 44, 547–557. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Lee, S.; Kwon, S.; Nam, W.; Cha, I.H.; Kim, H.J. Deep-learning-based survival prediction of oral cancer patients. Sci. Rep. 2019, 9, 6994. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.; Chun, J.; Chang, J.S.; Lee, C.G.; Keum, K.C.; Kim, J.S. Feasibility of continual deep-learning-based segmentation for personalized adaptive radiation therapy in head and neck area. Cancers 2021, 13, 702. [Google Scholar] [CrossRef]
- Koike, Y.; Anetai, Y.; Takegawa, H.; Ohira, S.; Nakamura, S.; Tanigawa, N. Deep-learning-based metal artifact reduction using cycle-consistent adversarial network for intensity-modulated head and neck radiation therapy treatment planning. Phys. Med. 2020, 78, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Koike, Y.; Ohira, S.; Akino, Y.; Sagawa, T.; Yagi, M.; Ueda, Y.; Miyazaki, M.; Sumida, I.; Teshima, T.; Ogawa, K. Deep-learning-based virtual noncontrast CT for volumetric modulated arc therapy planning: Comparison with a dual-energy CT-based approach. Med. Phys. 2020, 47, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Lalonde, A.; Winey, B.; Verburg, J.; Paganetti, H.; Sharp, G.C. Evaluation of CBCT scatter correction using deep convolutional neural networks for head and neck adaptive proton therapy. Phys. Med. Biol. 2020, 65, 245022. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Tang, F.; Huang, X.; Yang, K.; Zhong, T.; Hu, R.; Liu, S.; Yuan, X.; Zhang, Y. Deep-learning-based detection and segmentation of organs at risk in nasopharyngeal carcinoma computed tomographic images for radiotherapy planning. Eur. Radiol. 2019, 29, 1961–1967. [Google Scholar] [CrossRef]
- Li, X.; Wang, C.; Sheng, Y.; Zhang, J.; Wang, W.; Yin, F.F.; Wu, Q.; Wu, Q.J.; Ge, Y. An artificial intelligence-driven agent for real-time head-and-neck IMRT plan generation using conditional generative adversarial network (cGAN). Med. Phys. 2021, 48, 2714–2723. [Google Scholar] [CrossRef]
- Lin, L.; Dou, Q.; Jin, Y.M.; Zhou, G.Q.; Tang, Y.Q.; Chen, W.L.; Su, B.A.; Liu, F.; Tao, C.J.; Jiang, N.; et al. Deep learning for automated contouring of primary tumor volumes by MRI for nasopharyngeal carcinoma. Radiology 2019, 291, 677–686. [Google Scholar] [CrossRef]
- Liu, Z.; Fan, J.; Li, M.; Yan, H.; Hu, Z.; Huang, P.; Tian, Y.; Miao, J.; Dai, J. A deep-learning method for prediction of three-dimensional dose distribution of helical tomotherapy. Med. Phys. 2019, 46, 1972–1983. [Google Scholar] [CrossRef]
- Liu, K.; Xia, W.; Qiang, M.; Chen, X.; Liu, J.; Guo, X.; Lv, X. Deep learning pathological microscopic features in endemic nasopharyngeal cancer: Prognostic value and protentional role for individual induction chemotherapy. Cancer Med. 2020, 9, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, A.; Shi, H.; Huang, S.; Zheng, W.; Liu, Z.; Zhang, Q.; Yang, X. CT synthesis from MRI using multi-cycle GAN for head-and-neck radiation therapy. Comput. Med. Imaging Graph. 2021, 91, 101953. [Google Scholar] [CrossRef]
- Men, K.; Geng, H.; Cheng, C.; Zhong, H.; Huang, M.; Fan, Y.; Plastaras, J.P.; Lin, A.; Xiao, Y. More accurate and efficient segmentation of organs-at-risk in radiotherapy with convolutional neural networks cascades. Med. Phys. 2019, 46, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Neppl, S.; Landry, G.; Kurz, C.; Hansen, D.C.; Hoyle, B.; Stöcklein, S.; Seidensticker, M.; Weller, J.; Belka, C.; Parodi, K.; et al. Evaluation of proton and photon dose distributions recalculated on 2D and 3D Unet-generated pseudoCTs from T1-weighted MR head scans. Acta Oncol. 2019, 58, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.; Jia, X.; Sher, D.; Lin, M.H.; Iqbal, Z.; Liu, H.; Jiang, S. 3D radiotherapy dose prediction on head and neck cancer patients with a hierarchically densely connected U-net deep-learning architecture. Phys. Med. Biol. 2019, 64, 065020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolov, S.; Blackwell, S.; Zverovitch, A.; Mendes, R.; Livne, M.; De Fauw, J.; Patel, Y.; Meyer, C.; Askham, H.; Romera-Paredes, B.; et al. Deep learning to achieve clinically applicable segmentation of head and neck anatomy for radiotherapy. arXiv 2018, arXiv:1809.04430. [Google Scholar]
- Peng, H.; Dong, D.; Fang, M.J.; Li, L.; Tang, L.L.; Chen, L.; Li, W.F.; Mao, Y.P.; Fan, W.; Liu, L.Z.; et al. Prognostic value of deep learning PET/CT-based radiomics: Potential role for future individual induction chemotherapy in advanced nasopharyngeal carcinoma. Clin. Cancer Res. 2019, 25, 4271–4279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, M.; Li, Y.; Wu, A.; Jia, Q.; Li, B.; Sun, W.; Dai, Z.; Lu, X.; Zhou, L.; Deng, X.; et al. Multi-sequence MR image-based synthetic CT generation using a generative adversarial network for head and neck MRI-only radiotherapy. Med. Phys. 2020, 47, 1880–1894. [Google Scholar] [CrossRef]
- Tong, N.; Gou, S.; Yang, S.; Ruan, D.; Sheng, K. Fully automatic multi-organ segmentation for head and neck cancer radiotherapy using shape representation model constrained fully convolutional neural networks. Med. Phys. 2018, 45, 4558–4567. [Google Scholar] [CrossRef] [Green Version]
- Van Rooij, W.; Dahele, M.; Brandao, H.R.; Delaney, A.R.; Slotman, B.J.; Verbakel, W.F. Deep-learning-based delineation of head and neck organs at risk: Geometric and dosimetric evaluation. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 677–684. [Google Scholar] [CrossRef]
- Wang, C.; Liu, C.; Chang, Y.; Lafata, K.; Cui, Y.; Zhang, J.; Sheng, Y.; Mowery, Y.; Brizel, D.; Yin, F.F. Dose-distribution-driven PET image-based outcome prediction (DDD-PIOP): A deep learning study for oropharyngeal cancer IMRT application. Front. Oncol. 2020, 10, 1592. [Google Scholar] [CrossRef]
- Zhu, W.; Huang, Y.; Zeng, L.; Chen, X.; Liu, Y.; Qian, Z.; Du, N.; Fan, W.; Xie, X. AnatomyNet: Deep learning for fast and fully automated whole-volume segmentation of head and neck anatomy. Med. Phys. 2019, 46, 576–589. [Google Scholar] [CrossRef] [Green Version]
- Zhong, L.Z.; Fang, X.L.; Dong, D.; Peng, H.; Fang, M.J.; Huang, C.L.; He, B.X.; Lin, L.; Ma, J.; Tang, L.L.; et al. A deep learning MR-based radiomic nomogram may predict survival for nasopharyngeal carcinoma patients with stage T3N1M0. Radiother. Oncol. 2020, 151, 1–9. [Google Scholar] [CrossRef]
- Florkow, M.C.; Guerreiro, F.; Zijlstra, F.; Seravalli, E.; Janssens, G.O.; Maduro, J.H.; Knopf, A.C.; Castelein, R.M.; van Stralen, M.; Raaymakers, B.W.; et al. Deep learning-enabled MRI-only photon and proton therapy treatment planning for paediatric abdominal tumours. Radiother. Oncol. 2020, 153, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, F.; Seravalli, E.; Janssens, G.; Maduro, J.; Knopf, A.; Langendijk, J.; Raaymakers, B.; Kontaxis, C. Deep learning prediction of proton and photon dose distributions for paediatric abdominal tumours. Radiother. Oncol. 2021, 156, 36–42. [Google Scholar] [CrossRef]
- Jackson, P.; Hardcastle, N.; Dawe, N.; Kron, T.; Hofman, M.S.; Hicks, R.J. Deep learning renal segmentation for fully automated radiation dose estimation in unsealed source therapy. Front. Oncol. 2018, 8, 215. [Google Scholar] [CrossRef] [Green Version]
- He, T.; Fong, J.N.; Moore, L.W.; Ezeana, C.F.; Victor, D.; Divatia, M.; Vasquez, M.; Ghobrial, R.M.; Wong, S.T. An imageomics and multi-network based deep-learning model for risk assessment of liver transplantation for hepatocellular cancer. Comput. Med. Imaging Graph. 2021, 89, 101894. [Google Scholar] [CrossRef] [PubMed]
- Ibragimov, B.; Toesca, D.; Chang, D.; Yuan, Y.; Koong, A.; Xing, L. Development of deep neural network for individualized hepatobiliary toxicity prediction after liver SBRT. Med. Phys. 2018, 45, 4763–4774. [Google Scholar] [CrossRef] [PubMed]
- Ibragimov, B.; Toesca, D.A.; Yuan, Y.; Koong, A.C.; Chang, D.T.; Xing, L. Neural networks for deep radiotherapy dose analysis and prediction of liver SBRT outcomes. IEEE J. Biomed. Health Inform. 2019, 23, 1821–1833. [Google Scholar] [CrossRef] [PubMed]
- Ibragimov, B.; Toesca, D.A.; Chang, D.T.; Yuan, Y.; Koong, A.C.; Xing, L.; Vogelius, I.R. Deep learning for identification of critical regions associated with toxicities after liver stereotactic body radiation therapy. Med. Phys. 2020, 47, 3721–3731. [Google Scholar] [CrossRef]
- Peng, J.; Kang, S.; Ning, Z.; Deng, H.; Shen, J.; Xu, Y.; Zhang, J.; Zhao, W.; Li, X.; Gong, W.; et al. Residual convolutional neural network for predicting response of transarterial chemoembolization in hepatocellular carcinoma from CT imaging. Eur. Radiol. 2020, 30, 413–424. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.B.; Xu, D.; Ye, M.; Sun, L.; Zhang, X.Y.; Li, X.T.; Nie, P.; Xing, B.C.; Sun, Y.S. Deep learning-assisted magnetic resonance imaging prediction of tumor response to chemotherapy in patients with colorectal liver metastases. Int. J. Cancer 2021, 148, 1717–1730. [Google Scholar] [CrossRef]
- Barragán-Montero, A.M.; Nguyen, D.; Lu, W.; Lin, M.H.; Norouzi-Kandalan, R.; Geets, X.; Sterpin, E.; Jiang, S. Three-dimensional dose prediction for lung IMRT patients with deep neural networks: Robust learning from heterogeneous beam configurations. Med. Phys. 2019, 46, 3679–3691. [Google Scholar] [CrossRef]
- Cui, Y.; Arimura, H.; Nakano, R.; Yoshitake, T.; Shioyama, Y.; Yabuuchi, H. Automated approach for segmenting gross tumor volumes for lung cancer stereotactic body radiation therapy using CT-based dense V-networks. J. Radiat. Res. 2021, 62, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Haq, R.; Hotca, A.; Apte, A.; Rimner, A.; Deasy, J.O.; Thor, M. Cardio-pulmonary substructure segmentation of radiotherapy computed tomography images using convolutional neural networks for clinical outcomes analysis. Phys. Imaging Radiat. Oncol. 2020, 14, 61–66. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Di Dong, Y.S.; Zhou, C.; Fang, M.; Zhu, Y.; Zhang, H.; Huang, Z.; Jiang, T.; Tian, J.; Chen, C. Predicting response to immunotherapy in advanced non-small-cell lung cancer using tumor mutational burden radiomic biomarker. J. Immunother. Cancer 2020, 8, e000550. [Google Scholar] [CrossRef]
- Liang, B.; Tian, Y.; Chen, X.; Yan, H.; Yan, L.; Zhang, T.; Zhou, Z.; Wang, L.; Dai, J. Prediction of radiation pneumonitis with dose distribution: A convolutional neural network (CNN) based model. Front. Oncol. 2020, 9, 1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, B.; Doken, S.; Zhuang, T.; Wingerter, D.; Gidwani, M.; Mistry, N.; Ladic, L.; Kamen, A.; Abazeed, M.E. An image-based deep learning framework for individualising radiotherapy dose: A retrospective analysis of outcome prediction. Lancet Digit. Health 2019, 1, e136–e147. [Google Scholar] [CrossRef] [Green Version]
- Mu, W.; Jiang, L.; Shi, Y.; Tunali, I.; Gray, J.E.; Katsoulakis, E.; Tian, J.; Gillies, R.J.; Schabath, M.B. Non-invasive measurement of PD-L1 status and prediction of immunotherapy response using deep learning of PET/CT images. J. Immunother. Cancer 2021, 9, e002118. [Google Scholar] [CrossRef]
- Tian, P.; He, B.; Mu, W.; Liu, K.; Liu, L.; Zeng, H.; Liu, Y.; Jiang, L.; Zhou, P.; Huang, Z.; et al. Assessing PD-L1 expression in non-small cell lung cancer and predicting responses to immune checkpoint inhibitors using deep learning on computed tomography images. Theranostics 2021, 11, 2098. [Google Scholar] [CrossRef]
- Tseng, H.H.; Luo, Y.; Cui, S.; Chien, J.T.; Ten Haken, R.K.; Naqa, I.E. Deep reinforcement learning for automated radiation adaptation in lung cancer. Med. Phys. 2017, 44, 6690–6705. [Google Scholar] [CrossRef]
- Xing, Y.; Zhang, Y.; Nguyen, D.; Lin, M.H.; Lu, W.; Jiang, S. Boosting radiotherapy dose calculation accuracy with deep learning. J. Appl. Clin. Med. Phys. 2020, 21, 149–159. [Google Scholar] [CrossRef]
- Xu, Y.; Hosny, A.; Zeleznik, R.; Parmar, C.; Coroller, T.; Franco, I.; Mak, R.H.; Aerts, H.J. Deep learning predicts lung cancer treatment response from serial medical imaging. Clin. Cancer Res. 2019, 25, 3266–3275. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Yang, J.; Liang, Y.; Liao, B.; Zhu, W.; Mo, X.; Huang, K. Identification and Validation of Efficacy of Immunological Therapy for Lung Cancer From Histopathological Images Based on Deep Learning. Front. Genet. 2021, 12, 121. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.Q.; Chen, L.; Cooper, G.F.; Young, J.D.; Lu, X. Precision oncology beyond targeted therapy: Combining omics data with machine learning matches the majority of cancer cells to effective therapeutics. Mol. Cancer Res. 2018, 16, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakellaropoulos, T.; Vougas, K.; Narang, S.; Koinis, F.; Kotsinas, A.; Polyzos, A.; Moss, T.J.; Piha-Paul, S.; Zhou, H.; Kardala, E.; et al. A deep learning framework for predicting response to therapy in cancer. Cell Rep. 2019, 29, 3367–3373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maspero, M.; Houweling, A.C.; Savenije, M.H.; van Heijst, T.C.; Verhoeff, J.J.; Kotte, A.N.; van den Berg, C.A. A single neural network for cone-beam computed tomography-based radiotherapy of head-and-neck, lung and breast cancer. Phys. Imaging Radiat. Oncol. 2020, 14, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Nyflot, M.J.; Thammasorn, P.; Wootton, L.S.; Ford, E.C.; Chaovalitwongse, W.A. Deep learning for patient-specific quality assurance: Identifying errors in radiotherapy delivery by radiomic analysis of gamma images with convolutional neural networks. Med. Phys. 2019, 46, 456–464. [Google Scholar] [CrossRef]
- Yang, J.; Veeraraghavan, H.; Armato, S.G., III; Farahani, K.; Kirby, J.S.; Kalpathy-Kramer, J.; van Elmpt, W.; Dekker, A.; Han, X.; Feng, X.; et al. Autosegmentation for thoracic radiation treatment planning: A grand challenge at AAPM 2017. Med. Phys. 2018, 45, 4568–4581. [Google Scholar] [CrossRef]
- Liu, Y.; Lei, Y.; Fu, Y.; Wang, T.; Tang, X.; Jiang, X.; Curran, W.J.; Liu, T.; Patel, P.; Yang, X. CT-based multi-organ segmentation using a 3D self-attention U-net network for pancreatic radiotherapy. Med. Phys. 2020, 47, 4316–4324. [Google Scholar] [CrossRef]
- Wang, W.; Sheng, Y.; Palta, M.; Czito, B.; Willett, C.; Hito, M.; Yin, F.F.; Wu, Q.; Ge, Y.; Wu, Q.J. Deep Learning–Based Fluence Map Prediction for Pancreas Stereotactic Body Radiation Therapy With Simultaneous Integrated Boost. Adv. Radiat. Oncol. 2021, 6, 100672. [Google Scholar] [CrossRef]
- Arabi, H.; Dowling, J.A.; Burgos, N.; Han, X.; Greer, P.B.; Koutsouvelis, N.; Zaidi, H. Comparative study of algorithms for synthetic CT generation from MRI: Consequences for MRI-guided radiation planning in the pelvic region. Med. Phys. 2018, 45, 5218–5233. [Google Scholar] [CrossRef]
- Maspero, M.; Savenije, M.H.; Dinkla, A.M.; Seevinck, P.R.; Intven, M.P.; Jurgenliemk-Schulz, I.M.; Kerkmeijer, L.G.; van den Berg, C.A. Dose evaluation of fast synthetic-CT generation using a generative adversarial network for general pelvis MR-only radiotherapy. Phys. Med. Biol. 2018, 63, 185001. [Google Scholar] [CrossRef]
- Ju, Z.; Wu, Q.; Yang, W.; Gu, S.; Guo, W.; Wang, J.; Ge, R.; Quan, H.; Liu, J.; Qu, B. Automatic segmentation of pelvic organs-at-risk using a fusion network model based on limited training samples. Acta Oncol. 2020, 59, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Bohara, G.; Sadeghnejad Barkousaraie, A.; Jiang, S.; Nguyen, D. Using deep learning to predict beam-tunable Pareto optimal dose distribution for intensity-modulated radiation therapy. Med. Phys. 2020, 47, 3898–3912. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Qin, A.; Zhou, D.; Yan, D. U-net-generated synthetic CT images for magnetic resonance imaging-only prostate intensity-modulated radiation therapy treatment planning. Med. Phys. 2018, 45, 5659–5665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savenije, M.H.; Maspero, M.; Sikkes, G.G.; van der Voort van Zyp, J.; Kotte, T.; Alexis, N.; Bol, G.H.; van den Berg, T.; Cornelis, A. Clinical implementation of MRI-based organs-at-risk auto-segmentation with convolutional networks for prostate radiotherapy. Radiat. Oncol. 2020, 15, 104. [Google Scholar] [CrossRef]
- Elmahdy, M.S.; Jagt, T.; Zinkstok, R.T.; Qiao, Y.; Shahzad, R.; Sokooti, H.; Yousefi, S.; Incrocci, L.; Marijnen, C.; Hoogeman, M.; et al. Robust contour propagation using deep learning and image registration for online adaptive proton therapy of prostate cancer. Med. Phys. 2019, 46, 3329–3343. [Google Scholar] [CrossRef] [Green Version]
- Elmahdy, M.S.; Ahuja, T.; van der Heide, U.A.; Staring, M. Patient-specific finetuning of deep-learning models for adaptive radiotherapy in prostate CT. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; pp. 577–580. [Google Scholar]
- Kajikawa, T.; Kadoya, N.; Ito, K.; Takayama, Y.; Chiba, T.; Tomori, S.; Takeda, K.; Jingu, K. Automated prediction of dosimetric eligibility of patients with prostate cancer undergoing intensity-modulated radiation therapy using a convolutional neural network. Radiol. Phys. Technol. 2018, 11, 320–327. [Google Scholar] [CrossRef]
- Kajikawa, T.; Kadoya, N.; Ito, K.; Takayama, Y.; Chiba, T.; Tomori, S.; Nemoto, H.; Dobashi, S.; Takeda, K.; Jingu, K. A convolutional neural network approach for IMRT dose distribution prediction in prostate cancer patients. J. Radiat. Res. 2019, 60, 685–693. [Google Scholar] [CrossRef]
- Kandalan, R.N.; Nguyen, D.; Rezaeian, N.H.; Barragán-Montero, A.M.; Breedveld, S.; Namuduri, K.; Jiang, S.; Lin, M.H. Dose prediction with deep learning for prostate cancer radiation therapy: Model adaptation to different treatment planning practices. Radiother. Oncol. 2020, 153, 228–235. [Google Scholar] [CrossRef]
- Kearney, V.; Chan, J.W.; Wang, T.; Perry, A.; Descovich, M.; Morin, O.; Yom, S.S.; Solberg, T.D. DoseGAN: A generative adversarial network for synthetic dose prediction using attention-gated discrimination and generation. Sci. Rep. 2020, 10, 11073. [Google Scholar]
- Kiljunen, T.; Akram, S.; Niemelä, J.; Löyttyniemi, E.; Seppälä, J.; Heikkilä, J.; Vuolukka, K.; Kääriäinen, O.S.; Heikkilä, V.P.; Lehtiö, K.; et al. A deep-learning-based automated CT segmentation of prostate cancer anatomy for radiation therapy planning-a retrospective multicenter study. Diagnostics 2020, 10, 959. [Google Scholar] [CrossRef]
- Kontaxis, C.; Bol, G.; Lagendijk, J.; Raaymakers, B. DeepDose: Towards a fast dose calculation engine for radiation therapy using deep learning. Phys. Med. Biol. 2020, 65, 075013. [Google Scholar] [CrossRef] [PubMed]
- Largent, A.; Barateau, A.; Nunes, J.C.; Mylona, E.; Castelli, J.; Lafond, C.; Greer, P.B.; Dowling, J.A.; Baxter, J.; Saint-Jalmes, H.; et al. Comparison of deep-learning-based and patch-based methods for pseudo-CT generation in MRI-based prostate dose planning. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 1137–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhang, J.; Sheng, Y.; Chang, Y.; Yin, F.F.; Ge, Y.; Wu, Q.J.; Wang, C. Automatic IMRT planning via static field fluence prediction (AIP-SFFP): A deep learning algorithm for real-time prostate treatment planning. Phys. Med. Biol. 2020, 65, 175014. [Google Scholar] [CrossRef]
- Ma, M.; Buyyounouski, M.K.; Vasudevan, V.; Xing, L.; Yang, Y. Dose distribution prediction in isodose feature-preserving voxelization domain using deep convolutional neural network. Med. Phys. 2019, 46, 2978–2987. [Google Scholar] [CrossRef]
- Ma, M.; Kovalchuk, N.; Buyyounouski, M.K.; Xing, L.; Yang, Y. Incorporating dosimetric features into the prediction of 3D VMAT dose distributions using deep convolutional neural network. Phys. Med. Biol. 2019, 64, 125017. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Nguyen, D.; Bai, T.; Folkerts, M.; Jia, X.; Lu, W.; Zhou, L.; Jiang, S. A feasibility study on deep-learning-based individualized 3D dose distribution prediction. Med. Phys. 2021, 48, 4438–4447. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Magome, T.; Matsumoto, K.; Sato, T.; Yoshioka, Y.; Oguchi, M. Fully automated dose prediction using generative adversarial networks in prostate cancer patients. PLoS ONE 2020, 15, e0232697. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, T.; Futakami, N.; Yagi, M.; Kunieda, E.; Akiba, T.; Takeda, A.; Shigematsu, N. Simple low-cost approaches to semantic segmentation in radiation therapy planning for prostate cancer using deep learning with non-contrast planning CT images. Phys. Med. 2020, 78, 93–100. [Google Scholar] [CrossRef]
- Nguyen, D.; Long, T.; Jia, X.; Lu, W.; Gu, X.; Iqbal, Z.; Jiang, S. A feasibility study for predicting optimal radiation therapy dose distributions of prostate cancer patients from patient anatomy using deep learning. Sci. Rep. 2019, 9, 1076. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, D.; McBeth, R.; Sadeghnejad Barkousaraie, A.; Bohara, G.; Shen, C.; Jia, X.; Jiang, S. Incorporating human and learned domain knowledge into training deep neural networks: A differentiable dose-volume histogram and adversarial inspired framework for generating Pareto optimal dose distributions in radiation therapy. Med. Phys. 2020, 47, 837–849. [Google Scholar] [CrossRef]
- Sadeghnejad Barkousaraie, A.; Ogunmolu, O.; Jiang, S.; Nguyen, D. A fast deep-learning approach for beam orientation optimization for prostate cancer treated with intensity-modulated radiation therapy. Med. Phys. 2020, 47, 880–897. [Google Scholar] [CrossRef] [PubMed]
- Shao, W.; Banh, L.; Kunder, C.A.; Fan, R.E.; Soerensen, S.J.; Wang, J.B.; Teslovich, N.C.; Madhuripan, N.; Jawahar, A.; Ghanouni, P.; et al. ProsRegNet: A deep learning framework for registration of MRI and histopathology images of the prostate. Med. Image Anal. 2021, 68, 101919. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.S.; Kim, K.H.; Kang, S.W.; Kang, S.H.; Kim, J.S.; Kim, T.H.; Kim, D.S.; Cho, W.; Suh, T.S.; Chung, J.B. Dose Super-Resolution in Prostate Volumetric Modulated Arc Therapy Using Cascaded Deep Learning Networks. Front. Oncol. 2020, 10, 2443. [Google Scholar] [CrossRef] [PubMed]
- Sumida, I.; Magome, T.; Das, I.J.; Yamaguchi, H.; Kizaki, H.; Aboshi, K.; Yamaguchi, H.; Seo, Y.; Isohashi, F.; Ogawa, K. A convolution neural network for higher resolution dose prediction in prostate volumetric modulated arc therapy. Phys. Med. 2020, 72, 88–95. [Google Scholar] [CrossRef]
- Xing, Y.; Nguyen, D.; Lu, W.; Yang, M.; Jiang, S. A feasibility study on deep-learning-based radiotherapy dose calculation. Med. Phys. 2020, 47, 753–758. [Google Scholar] [CrossRef]
- Bibault, J.E.; Giraud, P.; Housset, M.; Durdux, C.; Taieb, J.; Berger, A.; Coriat, R.; Chaussade, S.; Dousset, B.; Nordlinger, B.; et al. Deep learning and radiomics predict complete response after neo-adjuvant chemoradiation for locally advanced rectal cancer. Sci. Rep. 2018, 8, 12611. [Google Scholar]
- Bird, D.; Nix, M.G.; McCallum, H.; Teo, M.; Gilbert, A.; Casanova, N.; Cooper, R.; Buckley, D.L.; Sebag-Montefiore, D.; Speight, R.; et al. Multicentre, deep learning, synthetic-CT generation for ano-rectal MR-only radiotherapy treatment planning. Radiother. Oncol. 2021, 156, 23–28. [Google Scholar] [CrossRef]
- Jin, C.; Yu, H.; Ke, J.; Ding, P.; Yi, Y.; Jiang, X.; Duan, X.; Tang, J.; Chang, D.T.; Wu, X.; et al. Predicting treatment response from longitudinal images using multi-task deep learning. Nat. Commun. 2021, 12, 1851. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, D.; Liu, Z.; Li, Z.; Xie, P.; Sun, K.; Wei, W.; Dai, W.; Tang, Z.; Ding, Y.; et al. Deep learning radiomics-based prediction of distant metastasis in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy: A multicentre study. EBioMedicine 2021, 69, 103442. [Google Scholar] [CrossRef]
- Men, K.; Dai, J.; Li, Y. Automatic segmentation of the clinical target volume and organs at risk in the planning CT for rectal cancer using deep dilated convolutional neural networks. Med. Phys. 2017, 44, 6377–6389. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, Y.; Nie, K.; Sun, X.; Niu, T.; Yue, N.; Kwong, T.; Chang, P.; Chow, D.; Chen, J.H.; et al. Machine learning for prediction of chemoradiation therapy response in rectal cancer using pre-treatment and mid-radiation multi-parametric MRI. Magn. Reson. Imaging 2019, 61, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Hu, J.; Wu, Q.; Xu, F.; Nie, S.; Zhao, Y.; Bai, S.; Yi, Z. Automatic delineation of the clinical target volume and organs at risk by deep learning for rectal cancer postoperative radiotherapy. Radiother. Oncol. 2020, 145, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, J.; Qin, G.; Shen, L.; Sun, Y.; Ying, H.; Zhang, Z.; Hu, W. A deep-learning-based autosegmentation of rectal tumors in MR images. Med. Phys. 2018, 45, 2560–2564. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhou, X.; Ma, J.; Liu, S.; Zhang, M.; Zheng, X.; Zhang, X.; Liu, G.; Zhang, X.; Lu, Y.; et al. Application of convolutional neural network to risk evaluation of positive circumferential resection margin of rectal cancer by magnetic resonance imaging. Zhonghua Wei Chang. Wai Zhi = Chin. J. Gastrointest. Surg. 2020, 23, 572–577. [Google Scholar]
- Zhang, X.Y.; Wang, L.; Zhu, H.T.; Li, Z.W.; Ye, M.; Li, X.T.; Shi, Y.J.; Zhu, H.C.; Sun, Y.S. Predicting rectal cancer response to neoadjuvant chemoradiotherapy using deep learning of diffusion kurtosis MRI. Radiology 2020, 296, 56–64. [Google Scholar] [CrossRef]
- Zhou, J.; Peng, Z.; Song, Y.; Chang, Y.; Pei, X.; Sheng, L.; Xu, X.G. A method of using deep learning to predict three-dimensional dose distributions for intensity-modulated radiotherapy of rectal cancer. J. Appl. Clin. Med. Phys. 2020, 21, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.W.; Lee, Y.C.; Chang, C.C.; Lin, Y.J.; Liou, Y.A.; Hsu, P.C.; Chang, C.C.; Sai, A.K.O.; Wang, C.H.; Chao, T.K. A Weakly Supervised Deep Learning Method for Guiding Ovarian Cancer Treatment and Identifying an Effective Biomarker. Cancers 2022, 14, 1651. [Google Scholar] [CrossRef]
- Lin, Y.J.; Chao, T.K.; Khalil, M.A.; Lee, Y.C.; Hong, D.Z.; Wu, J.J.; Wang, C.W. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers 2021, 13, 3891. [Google Scholar] [CrossRef]
- Shelhamer, E.; Long, J.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2016, 39, 640–651. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25. [Google Scholar] [CrossRef]
- Liu, S.; Deng, W. Very deep convolutional neural network based image classification using small training sample size. In Proceedings of the 2015 third IAPR Asian Conference on Pattern Recognition (ACPR), Kuala Lampur, Malaysia, 3–6 November 2015; pp. 730–734. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Hedden, N.; Xu, H. Radiation therapy dose prediction for left-sided breast cancers using two-dimensional and three-dimensional deep-learning models. Phys. Med. 2021, 83, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar] [CrossRef] [Green Version]
- Sabour, S.; Frosst, N.; Hinton, G.E. Dynamic Routing between Capsules. In Proceedings of the 31st International Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; pp. 3859–3869. [Google Scholar] [CrossRef]
- Chen, L.C.; Papandreou, G.; Kokkinos, I.; Murphy, K.; Yuille, A. Semantic Image Segmentation with Deep Convolutional Nets and Fully Connected CRFs. arXiv 2015, arXiv:1412.7062. [Google Scholar]
- Chen, L.C.; Papandreou, G.; Kokkinos, I.; Murphy, K.; Yuille, A. DeepLab: Semantic Image Segmentation with Deep Convolutional Nets, Atrous Convolution, and Fully Connected CRFs. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 40, 834–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking atrous convolution for semantic image segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European conference on computer vision (ECCV), Glasgow, UK, 23–28 August 2018; pp. 801–818. [Google Scholar]
- Wang, L.; Xie, C.; Zeng, N. RP-Net: A 3D Convolutional Neural Network for Brain Segmentation From Magnetic Resonance Imaging. IEEE Access 2019, 7, 39670–39679. [Google Scholar] [CrossRef]
- Gibson, E.; Giganti, F.; Hu, Y.; Bonmati, E.; Bandula, S.; Gurusamy, K.; Davidson, B.; Pereira, S.P.; Clarkson, M.J.; Barratt, D.C. Automatic Multi-Organ Segmentation on Abdominal CT With Dense V-Networks. IEEE Trans. Med. Imaging 2018, 37, 1822–1834. [Google Scholar] [CrossRef] [Green Version]
- Kaur, M.; Mohta, A. A Review of Deep Learning with Recurrent Neural Network. In Proceedings of the 2019 International Conference on Smart Systems and Inventive Technology (ICSSIT), Tirunelveli, India, 27–29 November 2019; pp. 460–465. [Google Scholar] [CrossRef]
- Szegedy, C.; Toshev, A.; Erhan, D. Deep Neural Networks for Object Detection. Adv. Neural Inf. Process. Syst. 2013, 26, 2553–2561. [Google Scholar]
- Gulgec, N.; Takáč, M.; Pakzad, S. Structural damage detection using convolutional neural networks. In Model Validation and Uncertainty Quantification; Springer: Cham, Switzerland, 2017; pp. 331–337. [Google Scholar] [CrossRef]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Ser. (Methodol.) 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, QC, Canada, 8–13 December 2014; Ghahramani, Z., Welling, M., Cortes, C., Lawrence, N., Weinberger, K.Q., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2014; Volume 27. [Google Scholar]
- Li, X.; Yu, L.; Chen, H.; Fu, C.W.; Xing, L.; Heng, P.A. Transformation-consistent self-ensembling model for semisupervised medical image segmentation. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 523–534. [Google Scholar] [CrossRef]
- Hu, Y.; Modat, M.; Gibson, E.; Li, W.; Ghavami, N.; Bonmati, E.; Wang, G.; Bandula, S.; Moore, C.M.; Emberton, M.; et al. Weakly-supervised convolutional neural networks for multimodal image registration. Med. Image Anal. 2018, 49, 1–13. [Google Scholar] [CrossRef]
- Chen, C.L.; Chen, C.C.; Yu, W.H.; Chen, S.H.; Chang, Y.C.; Hsu, T.I.; Hsiao, M.; Yeh, C.Y.; Chen, C.Y. An annotation-free whole-slide training approach to pathological classification of lung cancer types using deep learning. Nat. Commun. 2021, 12, 1193. [Google Scholar] [CrossRef] [PubMed]
- Anghel, A.; Stanisavljevic, M.; Andani, S.; Papandreou, N.; Rüschoff, J.H.; Wild, P.; Gabrani, M.; Pozidis, H. A high-performance system for robust stain normalization of whole-slide images in histopathology. Front. Med. 2019, 6, 193. [Google Scholar] [CrossRef] [PubMed]
- Tellez, D.; Litjens, G.; Bándi, P.; Bulten, W.; Bokhorst, J.M.; Ciompi, F.; Van Der Laak, J. Quantifying the effects of data augmentation and stain color normalization in convolutional neural networks for computational pathology. Med. Image Anal. 2019, 58, 101544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazvinian Zanjani, F.; Zinger, S.; Bejnordi, B.E.; van der Laak, J.A.; de With, P.H.N. Histopathology stain-color normalization using deep generative models. In Proceedings of the 1st Conference on Medical Imaging with Deep Learning (MIDL), Amsterdam, The Netherlands, 4–6 July 2018. [Google Scholar]
- Shaban, M.T.; Baur, C.; Navab, N.; Albarqouni, S. Staingan: Stain style transfer for digital histological images. In Proceedings of the 2019 Ieee 16th international symposium on biomedical imaging (Isbi 2019), Venice, Italy, 8–11 April 2019; pp. 953–956. [Google Scholar]
- Kang, H.; Luo, D.; Feng, W.; Zeng, S.; Quan, T.; Hu, J.; Liu, X. Stainnet: A fast and robust stain normalization network. Front. Med. 2021, 8, 746307. [Google Scholar] [CrossRef]
- Stathopoulos, S.; Kalamboukis, T. Applying latent semantic analysis to large-scale medical image databases. Comput. Med. Imaging Graph. 2015, 39, 27–34. [Google Scholar] [CrossRef]
- Kye, H.; Sohn, B.S.; Lee, J. Interactive GPU-based maximum intensity projection of large medical data sets using visibility culling based on the initial occluder and the visible block classification. Comput. Med. Imaging Graph. 2012, 36, 366–374. [Google Scholar] [CrossRef]
- Xu, Y.; Li, Y.; Shen, Z.; Wu, Z.; Gao, T.; Fan, Y.; Lai, M.; Eric, I.; Chang, C. Parallel multiple instance learning for extremely large histopathology image analysis. BMC Bioinform. 2017, 18, 360. [Google Scholar] [CrossRef]
- Pinckaers, H.; Bulten, W.; van der Laak, J.; Litjens, G. Detection of prostate cancer in whole-slide images through end-to-end training with image-level labels. IEEE Trans. Med. Imaging 2021, 40, 1817–1826. [Google Scholar] [CrossRef]
- Cruz-Roa, A.; Gilmore, H.; Basavanhally, A.; Feldman, M.; Ganesan, S.; Shih, N.; Tomaszewski, J.; Madabhushi, A.; González, F. High-throughput adaptive sampling for whole-slide histopathology image analysis (HASHI) via convolutional neural networks: Application to invasive breast cancer detection. PLoS ONE 2018, 13, e0196828. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Reference | Deep Learning Methods | Dataset | Modality | Treatment Methods |
|---|---|---|---|---|---|
| Bladder | Cha et al. [12] | CNN | 62 patients (65000 regions training; Leave-one-case-out cross-validation; 29 testing) | CT | Chemotherapy |
| Cha et al. [13] | CNN | 123 patients (82 training; 41 testing) | CT | Chemotherapy | |
| Wu et al. [14] | AlexNet | 123 patients (73 training; 41 testing) | CT | Chemotherapy | |
| Brain | Andreas et al. [15] | U-Net and HighResNet | 402 patients (242 training; 81 validation; 79 testing) | MRI + CT | Radiotherapy |
| Han et al. [16] | DeepLabV3+ | 520 patients (312 training; 104 validation; 104 testing) | CT | Radiotherapy : WBRT | |
| Jalalifar et al. [17] | U-Net | 106 patients (90 training; 6 validation; 10 testing) | MRI | Radiotherapy : SRT | |
| Kazemifar et al. [18] | GAN | 77 patients with 5-fold cross validation (70% training; 12% validation; 18% testing) | MRI + CT | Radiotherapy : VMAT | |
| Kazemifar et al. [19] | GAN | 77 patients (54 training; 12 validation; 11 testing) | MRI + CT | Radiotherapy : IMPT | |
| Li et al. [20] | Cycle GAN | 34 patients (28 training; 6 testing) | MRI + CT | Radiotherapy | |
| Liu et al. [10] | CNN | 505 patients data with 5-fold cross validation (490 training and validation) | MRI | Radiosurgery | |
| Maspero et al. [21] | cGANs | 60 patients (30 training; 10 validation; 20 testing) | MRI + CT | Radiotherapy : proton and photon therapy | |
| Wang et al. [22] | V-Net | 80 patients (75 training; 5 testing) | CT | Radiosurgery : SRS | |
| Yoon et al. [23] | CNN | 118 patients (88 training; 30 testing) | MRI | Surgery + Chemoradiotherapy : CCRT | |
| Yu et al. [4] | U-Net | 55 patients (40 training; 5 validation; 10 testing) | CT | Radiotherapy | |
| Breast | Bakx et al. [24] | U-Net | 115 patients (72 training; 18 validation; 15 testing) | CT | Radiotherapy : IMRT |
| Byra et al. [25] | Inception-ResNet-V2 | 30 patients with 251 breast masses (212 training; 39 validation) | US | Chemotherapy : NAC | |
| Chen et al. [26] | VGG-16 | 40 patients with 900 ROI for each patients (30 training; 10 testing) | CT | Radiotherapy | |
| Adoui et al. [27] | CNN | 42 patients (42 training; 14 external cases testing) | MRI | Chemotherapy | |
| Gernaat et al. [28] | CNN | 2289 patients (803 trainning and validation; 240 testing) | CT | Radiotherapy | |
| Ha et al. [29] | VGG-16 | 141 patients with 5-fold cross validation (80% validation; 20% testing) | MRI | Chemotherapy : NAC | |
| Hedden and Xu [4] | U-Net | 145 patients (120 training; 5-fold cross validation; 25 testing) | CT | Radiotherapy : 3D-CRT | |
| Jiang et al. [30] | CNN | 592 patients (356 training; 236 validation) | US | Chemotherapy : NAC | |
| Qu et al. [31] | CNN | 302 patients (244 training; 58 validation) | MRI | Chemotherapy : NAC | |
| Schreier et al. [32] | BibNet | 251 patients (149 training; 50 validation; 52 scans | CT | Radiotherapy | |
| Bone | He et al. [9] | Inception V3 | 56 patients (28 training; 28 testing) | MRI | Surgery |
| Wang et al. [33] | Cascade R-CNN | 12426 Cells (10 fold cross validation); 300 Cells image (testing) | Phatology | Bone marrow smear | |
| Cervix | Jihong et al. [34] | CNN | 140 patients (100 training; 20 validation; 20 testing) | CT | Radiotherapy : IMRT |
| Rigaud et al. [35] | DeepLabV3 + U-Net | 408 patients (255 training; 61 validation; 92 testing) | CT | Radiotherapy : IMRT | |
| Zaffino et al. [36] | U-Net | 50 patients (70% training; 30% testing) | MRI | Radiotherapy : Brachytherapy | |
| Wang et al. [37] | FCN | 143 patients (68% training; 32% testing) | Pathology: Pap-smear images | Surgery : cervical biopsy | |
| Esophagus | Hu et al. [38] | CNN | 231 patients (161 training; 70 testing) | CT | Chemoradiation + Surgery |
| Jiang et al. [39] | Autoencoder + DBN | 80 patients with 8-fold cross validation | CT | Radiotherapy | |
| Jiang et al. [40] | CNN + Autoencoder | 245 patients (182 training; 63 testing) | CT | Radiotherapy : IMRT | |
| Gastric | Lee et al. [7] | RNN-Surv | 1190 patients (80% training; 20% testing) | Pathology | Chemotherapy |
| Zhang et al. [41] | CNN | 640 patients (518 training; 122 validation) | CT | Chemotherapy | |
| Chen et al. [42] | ResNet | 147 patients (80 training; 35 internal validation; 32 external validation) | CT | Surgery | |
| Head and neck | Cardenas et al. [43] | U-Net | 71 patients (51 training; 10 validation; 10 testing) | CT | Radiotherapy |
| Chen et al. [44] | ResNet-101 | 80 patients (70 training; 10 testing) | CT | Radiotherapy : IMRT | |
| Diamant et al. [45] | CNN | 300 patients with 5-fold cross validation (194 training; 106 testing) | CT | Chemoradiation | |
| Dinkla et al. [46] | U-Net | 34 patients (22 training; 12 testing) | MRI + CT | Radiotherapy | |
| Fan et al. [47] | ResNet-50 | 270 patients (195 training; 25 validation; 50 testing) | CT | Radiotherapy : IMRT | |
| Fujima et al. [48] | ResNet-101 | 113 patients (83 training; 30 testing) | CT + PET | Surgery + Chemoradiation | |
| Gronberg et al. [49] | Dense Dilated U-Net | 340 patients (200 training; 40 validation; 100 testing) | CT | Radiotherapy : IMRT | |
| Gurney-Champion et al. [50] | U-Net | 48 patients with 8-fold cross validation (80% training; 20% validation; 6 testing) | MRI | Radiotherapy | |
| Ibragimov and Xing [51] | CNN | 50 patients with 5-fold cross validation (40 training; 10 testing) | CT | Radiotherapy | |
| Kim et al. [52] | DeepSurv | 255 patients (183 training; 72 testing) | Patients record: oral SCC | Surgery | |
| Kim et al. [53] | DenseNet | 100 patients (80 training; 20 testing) | CT | Radiotherapy | |
| Koike et al. [54] | GAN | 107 patients with 5-fold cross validation (92 training; 15 testing) | CT | Radiotherapy : IMRT | |
| Koike et al. [55] | DenseNet | 61 patients (45 training; 16 testing) | CT | Radiotherapy : VMAT | |
| Lalonde et al. [56] | U-Net | 48 patients (29 training; 9 validation; 10 testing) | CT | Radiotherapy : proton therapy (APT) | |
| Liang et al. [57] | CNN | 185 patients with 4-fold cross-validation | CT | Radiotherapy | |
| Li et al. [58] | cGAN | 231 patients (200 training; 16 validation; 15 testing) | CT | Radiotherapy : IMRT | |
| Lin et al. [59] | CNN | 1021 patients (715 training; 103 validation; 203 testing) | MRI | Radiotherapy | |
| Liu et al. [60] | U-ResNet-D | 190 patients (136 training; 34 validation; 20 testing) | CT | Radiotherapy : HT | |
| Liu et al. [61] | DeepSurv | 1055 patients (843 training; 212 validation) | Pathology | Chemotherapy | |
| Liu et al. [62] | GAN | 164 patients (117 training; 18 validation; 29 testing) | CT + MRI | Radiotherapy | |
| Men et al. [63] | CNN casacades | 100 patients with 5-fold cross validation (80% training; 20% testing) | CT | Radiotherapy | |
| Neppl et al. [64] | U-Net | 81 patients (57 training; 28 validation; 4 testing) | MRI + CT | Radiotherapy : proton and photon therapy | |
| Nguyen et al. [65] | U-Net + DenseNet | 120 patients (80 training; 20 validation; 20 testing) | Planning data : VMAT | Radiotherapy : VMAT | |
| Nikolov et al. [66] | U-Net | 486 patients (389 training; 51 validation; 46 testing) | CT | Radiotherapy | |
| Peng et al. [67] | CNN | 707 patients (470 training; 237 testing) | PET + CT | Chemotherapy | |
| Qi et al. [68] | GAN + U-Net | 45 patients (30 training; 15 testing) | MRI + CT | Radiotherapy | |
| Tong et al. [69] | FCNN | 32 patients (22 training; 10 testing) | CT | Radiotherapy : IMRT | |
| van Rooij et al. [70] | U-Net | 157 patients (142 training; 15 testing) | CT | Radiotherapy | |
| Wang et al. [71] | CNN | 61 patients (61 training; 5 testing) | CT + PET | Radiotherapy | |
| Zhu et al. [72] | U-Net | 271 patients (261 training; 10 testing) | CT | Radiotherapy | |
| Zhong et al. [73] | SE-ResNeXt | 638 patients (447 training; 191 testing) | MRI | Chemotherapy | |
| Kidneys | Florkow et al. [74] | U-Net | 66 patients (54 training; 12 testing) | MRI + CT | Radiotherapy : proton and photon therapy |
| Guerreiro et al. [75] | U-Net | 80 patients (48 training; 12 validation; 20 testing) | CT | Radiotherapy : proton and photon therapy | |
| Jackson et al. [76] | CNN | 113 patients (89 training; 24 testing) | CT | Radiotherapy | |
| Liver | He et al. [77] | CapsNet | 109 patients (87 training; 22 testing) | MRI + Pathology | Surgery : liver transplantation |
| Ibragimov et al. [78] | CNN | 72 patients with 8-fold cross validation | CT | Radiotherapy : SBRT | |
| Ibragimov et al. [78] | CNN | 125 patients with 20-fold cross validation | CT | Radiotherapy : SBRT | |
| Ibragimov et al. [79] | CNN | 125 patients with 10-fold cross validation | CT | Radiotherapy : SBRT | |
| Ibragimov et al. [80] | CNN | 122 patients with 20-fold cross validation | CT | Radiotherapy | |
| Peng et al. [81] | ResNet-50 | 789 patients (562 training; 89 validation; 138 testing) | CT | Chemotherapy : TACE therapy | |
| Wei et al. [5] | ResNet-10 | 192 patients (244 training; 48 validation) | CT | Chemotherapy | |
| Zhu et al. [82] | CNN | 155 patients (101 training; 54 testing) + 25 patients from external cohort | MRI | Chemotherapy | |
| Lung | Barragan-Montero et al. [83] | U-Net + DenseNet | 129 patients with 5-fold cross validation (80 training; 20 validation; 29 testing) | Pathology | Radiotherapy : IMRT |
| Cui et al. [84] | Dense V-Net | 192 patients (147 training, 26 validation; 19 testing) | CT | Radiotherapy : SBRT | |
| Haq et al. [85] | Deeplab V3+ | 241 patients (193 training; 24 validation; 24 testing) | CT | Radiotherapy | |
| He et al. [86] | DenseNet | 327 patients (236 training; 26 validation; 65 testing) | CT | Immunotherapy | |
| Huang et al. [8] | CNN + ResNet | 180 patients with 2-fold cross validation (1-fold training; 1-fold testing) | pathology : H&E | Targeted therapy | |
| Liang et al. [87] | CNN | 70 patients (1000 times bootstrap training; 70 validation) | CT | Radiotherapy : VMAT | |
| Lou et al. [88] | DNN : Deep profiler | 944 patients with 5-fold cross validation | CT | Radiotherapy | |
| Mu et al. [89] | CNN | 697 patients (284 training; 116 validation; 85 testing) | PET/CT | Immunotherapy | |
| Tian et al. [90] | Deep CNN | 939 patients (750 training; 93 validation; 96 training) | CT | Immunotherapy | |
| Tseng et al. [91] | DRL | 114 patients (114 training; 34 testing) | PET | Radiotherapy | |
| Xing et al. [92] | HD U-Net | 120 patients (72 training; 18 validation; 30 testing) | CT | Radiotherapy | |
| Xu et al. [93] | CNN + RNN | 268 patients (179 training; 89 testing) | CT + pathology | Chemoradiation + Surgery | |
| Yang et al. [94] | CNN + ResNet | 180 patients with 2-fold cross validation | Pathology | Immunotherapy + Targeted therapy | |
| Yang et al. [6] | DNN | 200 patients with 5-fold cross validation (5-folds training; 5-folds testing) | CT | Immunotherapy | |
| Multi cancer | Ding et al. [95] | Autoencoder | 624 cell lines (520 training; 104 testing) | Genomics data | Chemotherapy |
| Sakellaropoulos et al. [96] | DNN | 1001 cell lines + 251 drugs with 5-fold cross validation (1001 training; 1001 testing) | Genomics data | Chemotherapy | |
| Maspero et al. [97] | GAN | 99 patients (45 training; 24 validation; 30 testing) | CT | Radiotherapy | |
| Nyflot et al. [98] | CNN | 558 gamma images (303 training; 255 testing) | CT | Radiotherapy : IMRT | |
| Yang et al. [99] | U-Net | 60 patients (36 training; 24 testing) | CT | Radiotherapy : TRT | |
| Pancreas | Liu et al. [100] | U-Net | 100 patients with 5-fold cross validation (80 training; 20 testing) | CT | Radiotherapy |
| Wang et al. [101] | CNN | 100 patients (80 training; 20 testing) | SBRT | Radiotherapy : SBRT | |
| Pelvis | Arabi et al. [102] | Deep CNN | 39 patients with 4-fold cross validation (3-fold training; 1-fold testing) | MRI + sCT | Radiotherapy |
| Maspero et al. [103] | cGAN | 91 patients (32 training; 59 testing) | MRI + sCT | Radiotherapy | |
| Ju et al. [104] | Dense V-Net | 100 patients (80 taining, 20 testing) | CT | Radiotherapy | |
| Prostate | Bohara et al. [105] | U-Net | 70 patients (54 training; 6 validation; 10 testing) | CT | Radiotherapy : IMRT |
| Chen et al. [106] | U-Net | 51 patients (36 training; 15 testing) | MRI + CT | Radiotherapy : IMRT | |
| Elguindi et al. [107] | DeepLabV3+ + U-Net | 50 patients (40 training; 10 validation; 50 testing) | MRI | Radiotherapy | |
| Elmahdy et al. [108] | CNN | 450 patients (350 training; 68 validation; 32 testing) | CT | Radiotherapy : proton therapy (IMPT) | |
| Elmahdy et al. [109] | CNN | 379 patients + 18 patients (259 training; 111 validation; 18 testing) | CT | Radiotherapy | |
| Kajikawa et al. [110] | AlexNet | 60 patients with 5-fold cross validation (48 training; 12 testing) | CT + structure label | Radiotherapy : IMRT | |
| Kajikawa et al. [111] | U-Net | 95 patients with 5-fold cross validation (64 training; 16 validation; 15 testing) | CT | Radiotherapy : IMRT | |
| Kandalan et al. [112] | U-Net | 248 patients (188 training; 60 testing) | Planning data : VMAT | Radiotherapy : VMAT | |
| Kearney et al. [113] | GAN | 141 patients (126 training; 15 testing) | CT | Radiotherapy : SBRT | |
| Kiljunen et al. [114] | CNN | 900 patients (900 training; 900 testing) | CT | Radiotherapy | |
| Kontaxis et al. [115] | U-Net | 101 patients (80 training; 10 validation; 11 testing) | MRI | Radiotherapy | |
| Landry et al. [56] | U-Net | 42 patients (27 training; 7 validation; 8 testing) | CT | Radiotherapy : VMAT | |
| Largent et al. [116] | U-Net + GAN | 39 patients (25 training; 14 validation) | MRI + CT | Radiotherapy : VMAT | |
| Li et al. [117] | Dense-Res Hybrid Network | 106 patients (106 training; 14 testing) | IMRT planning | Radiotherapy : IMRT | |
| Ma et al. [118] | U-Net | 70 patients (60 training; 10 testing) | CT | Radiotherapy : VMAT | |
| Ma et al. [119] | U-Net | 70 patients (52 training; 8 validation; 10 testing) | CT | Radiotherapy : VMAT | |
| Ma et al. [120] | U-Net | 97 patients (69 taining; 8 validation; 20 testing) | CT : Patient anatomy | Radiotherapy | |
| Murakami et al. [121] | GAN | 90 patients (81 training; 9 testing) | CT | Radiotherapy : IMRT | |
| Nemoto et al. [122] | U-Net | 556 patients (400 training; 100 validation; 56 testing) | CT | Radiotherapy : IMRT | |
| Nguyen et al. [123] | U-Net | 88 patients (72 training; 8 validation; 8 testing) | IMRT | Radiotherapy : IMRT | |
| Nguyen et al. [124] | U-Net | 70 patients (54 training; 6 validation; 10 testing) | IMRT | Radiotherapy : IMRT | |
| Barkousaraie et al. [125] | DNN | 70 patients (50 training; 7 validation; 13 testing) | IMRT | Radiotherapy : IMRT | |
| Savenije et al. [107] | DenseV-Net | 150 patients (97 training; 53 testing) | MRI | Radiotherapy | |
| Shao et al. [126] | CNN | 152 patients (99 training; 53 testing) | MRI + Pathology | Radiotherapy | |
| Shin et al. [127] | HD U-Net + Residual DenseNet | 73 patients with 5-fold cross validation (80% training; 20% testing) | CT | Radiotherapy : VMAT | |
| Sumida et al. [128] | U-Net | 66 patients (50 training; 16 testing) | CT | Radiotherapy : VMAT | |
| Xing et al. [129] | HD U-net | 78 patients with 5-fold cross validation (70 training; 8 testing) | CT | Radiotherapy : IMRT | |
| Rectum | Bibault et al. [130] | DNN | 95 patients with 5-fold cross-validation (4-fold training; 1-fold testing) | CT | Chemoradiation |
| Bird et al. [131] | cGAN | 90 patients (46 training; 44 testing) | sCT + MRI | Radiotherapy | |
| Jin et al. [132] | RP-Net | 622 patients (321 training; 160 internal validation; 141 external validation) | MRI | Chemoradiation : NCRT | |
| Liu et al. [133] | ResNet-18 | 235 patients (170 training; 65 external validation) | MRI + Pathology | Chemoradiation : NCRT | |
| Men et al. [134] | CNN + U-Net | 278 patients (218 training; 60 testing) | CT | Radiotherapy | |
| Shi et al. [135] | CNN | 51 patients with 10-fold cross validation (90% training; 10% testing) | MRI | Chemoradiation : CRT | |
| Song et al. [136] | DeeplabV3+ + ResUNet + DDCNN | 199 patients (98 training; 38 validation; 63 testing) | CT | Radiotherapy | |
| Wang et al. [137] | U-Net | 93 patients (85 training; 8 validation) + 20 patients double contoured | MRI | Chemoradiotherapy : NACT + Surgery | |
| Xu et al. [138] | CNN | 350 patients (300 training; 50 validation) | MRI | Surgery | |
| Zhang et al. [139] | CNN | 383 patients (290 training; 93 testing) | MRI | Chemoradiation | |
| Zhou et al. [140] | ResNet | 122 patients with 5-fold cross validation (80 training; 20 validation; 22 testing) | CT | Radiotherapy : IMRT | |
| Ovarian | Wang et al. [141] | R-CNN + Weakly supervised learning + Inception model 2 and 3 | 72 Tissue core (66% training; 34%testing; 5 fold cross validation) | Pathology | Molecular target therapy : antiangiogenesis |
| Thyroid | Lin et al. [142] | VGG16 + UNet + SegNet | 131 WSIs (28 training; 103 testing) | Pathology | Surgery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-W.; Khalil, M.-A.; Firdi, N.P. A Survey on Deep Learning for Precision Oncology. Diagnostics 2022, 12, 1489. https://doi.org/10.3390/diagnostics12061489
Wang C-W, Khalil M-A, Firdi NP. A Survey on Deep Learning for Precision Oncology. Diagnostics. 2022; 12(6):1489. https://doi.org/10.3390/diagnostics12061489
Chicago/Turabian StyleWang, Ching-Wei, Muhammad-Adil Khalil, and Nabila Puspita Firdi. 2022. "A Survey on Deep Learning for Precision Oncology" Diagnostics 12, no. 6: 1489. https://doi.org/10.3390/diagnostics12061489