
Maternal HPV Infection and the Estimated Risks for Adverse Pregnancy Outcomes—A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
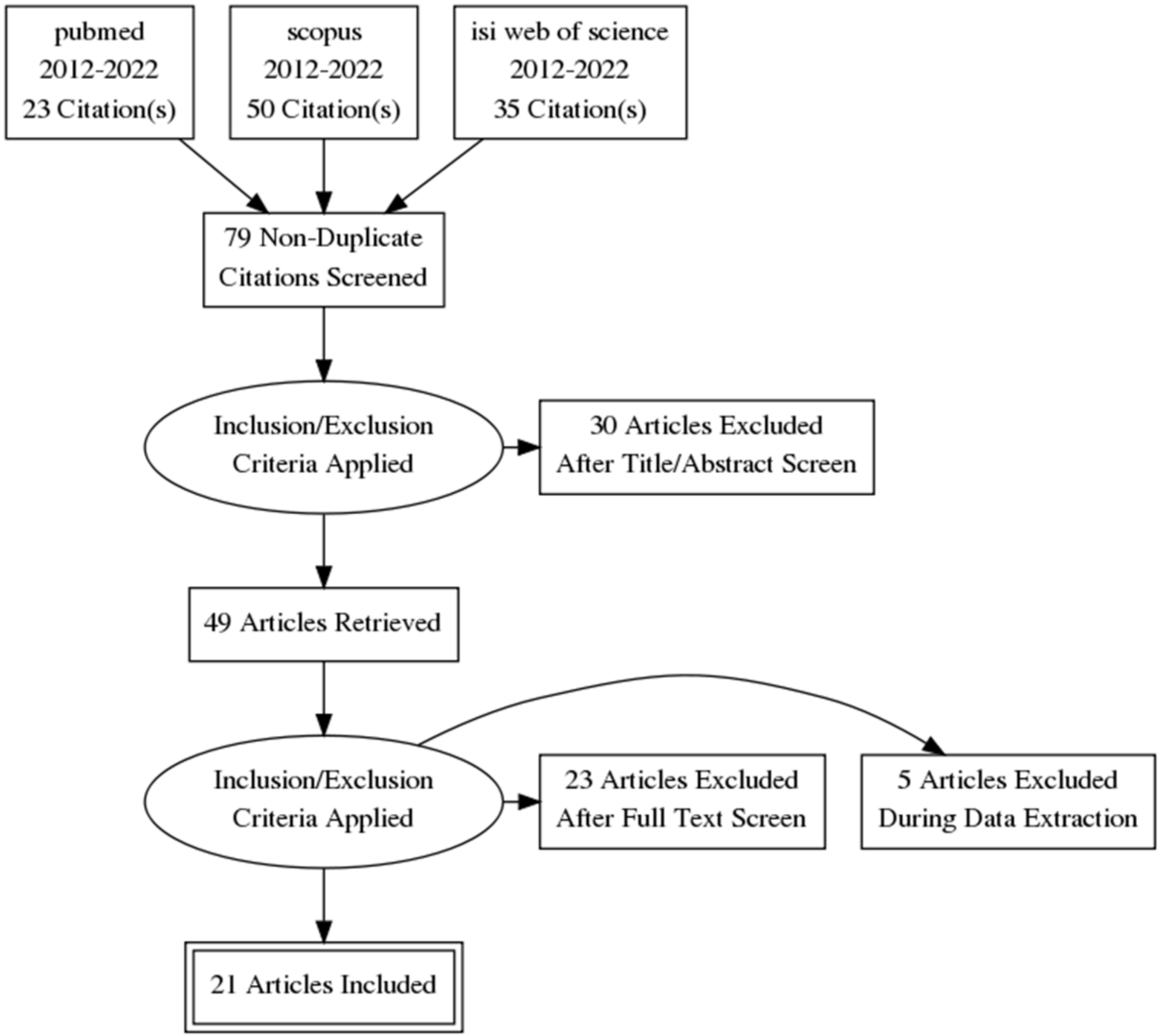
2.1. Search Strategy
2.2. Eligibility
2.3. Exposure
3. Results
3.1. Primary Outcome—Preterm Birth
3.2. Secondary Outcomes
3.2.1. Miscarriage
3.2.2. Premature Rupture of Membranes
3.2.3. Pregnancy-Induced Hypertensive Disorders
3.2.4. Fetal Growth Restriction (FGR)
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gheit, T. Mucosal and cutaneous human papillomavirus infections and cancer biology. Front. Oncol. 2019, 9, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). HPV and Cancer HPV-Associated Cancer Statistics; United States Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2020. [Google Scholar]
- Palefsky, J.M. Human Papillomavirus Infections: Epidemiology and Disease Associations. Available online: https://www.uptodate.com/contents/human-papillomavirus-infections-epidemiology-and-disease-associations?search=human-papillomavirus-infections-epidemiology-and-disease-associations%20January%202022&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 16 March 2022).
- Bruni, L.; Barrionuevo-Rosas, L.; Albero, G.; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World: Summary Report. Available online: https://hpvcentre.net/statistics/reports/XWX.pdf (accessed on 16 March 2022).
- Mandell, G.L.; John, J.E.; Bennett, E.; Dolin, R. (Eds.) Papillomaviruses. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 6th ed.; Elsevier—Health Sciences Division: New York, NY, USA, 2010. [Google Scholar]
- Franco, E.L.; Duarte-Franco, E.; Ferenczy, A. Cervical cancer: Epidemiology, prevention and the role of human papillomavirus infection. CMAJ 2001, 164, 7. [Google Scholar]
- Tilston, P. Anal human papillomavirus and anal cancer. J. Clin. Pathol. 1997, 50, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De San José, S.; Alemany, L.; Ordi, J.; Tous, S.; Alejo, M.; Bigby, S.M.; Joura, E.A.; Maldonado, P.; Laco, J.; Bravo, I.G.; et al. Worldwide human papillomavirus genotype attribution in over 2000 cases of intraepithelial and invasive lesions of the vulva. Eur. J. Cancer 2013, 49, 16. [Google Scholar] [CrossRef]
- Beckmann, A.M.; Daling, J.R.; Sherman, K.J.; Maden, C.; Miller, B.A.; Coates, R.J.; Kiviat, N.B.; Myerson, D.; Weiss, N.S.; Hislop, T.G.; et al. Human papillomavirus infection and anal cancer. Int. J. Cancer 1989, 43, 6. [Google Scholar] [CrossRef]
- Gu, W.; Zhang, P.; Zhang, G.; Zhou, J.; Ding, X.; Wang, Q.; Wang, B.; Wei, Y.; Jin, S.; Ye, D.; et al. Importance of HPV in Chinese Penile Cancer: A Contemporary Multicenter Study. Front. Oncol. 2020, 10, 1521. [Google Scholar] [CrossRef]
- Faber, M.T.; Duun-Henriksen, A.K.; Dehlendorff, C.; Tatla, M.K.; Munk, C.; Kjaer, S.K. Adverse pregnancy outcomes and infant mortality after quadrivalent HPV vaccination during pregnancy. Vaccine 2019, 37, 265–271. [Google Scholar] [CrossRef]
- Bober, L.; Guzowski, G.; Moczulska, H.; Sieroszewski, P. Influence of Human Papilloma Virus (HPV) infection on early pregnancy. Ginekol. Pol. 2019, 90, 72–75. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Chen, L.; Zhen, J.; Jin, X. Systematic review and meta-analysis on influence of human papillomavirus infection during pregnancy on premature rupture of membranes and premature delivery. Ann. Palliat. Med. 2021, 10, 10735–70743. [Google Scholar] [CrossRef]
- Smith, H.B. (Ed.) Handbook on Human Papillomavirus: Prevalence, Detection and Management; Nova Medicine and Health: Hauppauge, NY, USA, 2013; ISBN 978-1-62618-672-9. [Google Scholar]
- Chatzistamatiou, K.; Sotiriadis, A.; Agorastos, T. Effect of mode of delivery on vertical human papillomavirus transmission—A meta-analysis. J. Obstet. Gynaecol. 2016, 36, 10–14. [Google Scholar] [CrossRef]
- Armbruster-Moraes, E.; Ioshimoto, L.M.; Leão, E.; Zugaib, M. Presence of human papillomavirus DNA in amniotic fluids of pregnant women with cervical lesions. Gynecol. Oncol. 1994, 54, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Uribarren-Berrueta, O.; Sánchez-Corona, J.; Montoya-Fuentes, H.; Trujillo-Hernández, B.; Vásquez, C. Presence of HPV DNA in placenta and cervix of pregnant Mexican women. Arch. Gynecol. Obstet. 2012, 285, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Bodaghi, S.; Wood, L.V.; Roby, G.; Ryder, C.; Steinberg, S.M.; Zheng, Z.-M. Could human papillomaviruses be spread through blood? J. Clin. Microbiol. 2005, 43, 5428–5434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cladel, N.M.; Jiang, P.; Li, J.J.; Peng, X.; Cooper, T.K.; Majerciak, V.; Balogh, K.K.; Meyer, T.J.; Brendle, S.A.; Budgeon, L.R.; et al. Papillomavirus can be transmitted through the blood and produce infections in blood recipients: Evidence from two animal models. Emerg. Microbes Infect. 2019, 8, 1108–1121. [Google Scholar] [CrossRef] [Green Version]
- Rando, R.F.; Lindheim, S.; Hasty, L.; Sedlacek, T.V.; Woodland, M.; Eder, C. Increased frequency of detection of human papillomavirus deoxyribonucleic acid in exfoliated cervical cells during pregnancy. Am. J. Obstet. Gynecol. 1989, 161, 50–55. [Google Scholar] [CrossRef]
- Liu, Y.; You, H.; Chiriva-Internati, M.; Korourian, S.; Lowery, C.L.; Carey, M.J.; Smith, C.V.; Hermonat, P.L. Display of complete life cycle of human papillomavirus type 16 in cultured placental trophoblasts. Virology 2001, 290, 99–105. [Google Scholar] [CrossRef] [Green Version]
- You, H.; Liu, Y.; Agrawal, N.; Prasad, C.; Edwards, J.; Osborne, A.; Korourian, S.; Lowery, C.; Hermonat, P. Multiple Human Papillomavirus Types Replicate in 3A Trophoblasts. Placenta 2008, 29, 30–38. [Google Scholar] [CrossRef]
- Pandey, D.; Solleti, V.; Jain, G.; Das, A.; Prasada, K.S.; Acharya, S.; Satyamoorthy, K. Human Papillomavirus (HPV) infection in early pregnancy: Prevalence and implications. Infect. Dis. Obstet. Gynecol. 2019, 2019, 4376902. [Google Scholar] [CrossRef] [Green Version]
- Hornychova, H.; Kacerovsky, M.; Musilova, I.; Pliskova, L.; Zemlickova, H.; Matejkova, A.; Vosmikova, H.; Rozkosova, K.; Cermakova, P.; Bolehovska, R.; et al. Cervical human papillomavirus infection in women with preterm prelabor rupture of membranes. PLoS ONE 2018, 13, e0207896. [Google Scholar] [CrossRef]
- Wiik, J.; Nilsson, S.; Kärrberg, C.; Strander, B.; Jacobsson, B.; Sengpiel, V. Associations of treated and untreated human papillomavirus infection with preterm delivery and neonatal mortality: A Swedish population-based study. PLoS Med. 2021, 18, e1003641. [Google Scholar] [CrossRef]
- Zuo, Z.; Goel, S.; Carter, J.E. Association of cervical cytology and HPV DNA status during pregnancy with placental abnormalities and preterm birth. Am. J. Clin. Pathol. 2011, 136, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Giambanco, L.; Iannone, V.; Borriello, M.; Montalto, A. Papillomavirus infection and preterm birth. Chronicle of a broken relationship? case series and review of the literature. PAMJ Clin. Med. 2020, 3, 133. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Xiong, Y.-Q.; Mo, Y.; Luo, Q.-M.; Huo, S.-T.; He, W.-Q.; Chen, Q. The risk of human papillomavirus infection for spontaneous abortion, spontaneous preterm birth, and pregnancy rate of assisted reproductive technologies: A systematic review and meta-analysis. Gynecol. Obstet. Investig. 2018, 83, 417–427. [Google Scholar] [CrossRef]
- Niyibizi, J.; Zanré, N.; Mayrand, M.-H.; Trottier, H. Association between Maternal Human Papillomavirus Infection and Adverse Pregnancy Outcomes: Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 221, 1925–1937. [Google Scholar] [CrossRef]
- Ambühl, L.M.M.; Baandrup, U.; Dybkær, K.; Blaakær, J.; Uldbjerg, N.; Sørensen, S. Human Papillomavirus Infection as a Possible Cause of Spontaneous Abortion and Spontaneous Preterm Delivery. Infect. Dis. Obstet. Gynecol. 2016, 2016, 3086036. [Google Scholar] [CrossRef] [Green Version]
- Chilaka, V.N.; Navti, O.B.; Al Beloushi, M.; Ahmed, B.; Konje, J.C. Human papillomavirus (HPV) in pregnancy—An update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 264, 340–348. [Google Scholar] [CrossRef]
- Condrat, C.E.; Filip, L.; Gherghe, M.; Cretoiu, D.; Suciu, N. Maternal HPV infection: Effects on pregnancy outcome. Viruses 2021, 13, 2455. [Google Scholar] [CrossRef]
- Basonidis, A.; Liberis, A.; Daniilidis, A.; Petousis, S.; Dinas, K. Human papilloma virus infection and miscarriage: Is there an association? Taiwan. J. Obstet. Gynecol. 2020, 59, 656–659. [Google Scholar] [CrossRef]
- Caballero, A.; Dudley, D.; Ferguson, J.; Pettit, K.; Boyle, A. Maternal Human Papillomavirus and Preterm Premature Rupture of Membranes: A Retrospective Cohort Study. J. Women’s Health 2019, 28, 606–611. [Google Scholar] [CrossRef]
- Reily-Bell, A.L.; Fisher, A.; Harrison, B.; Bowie, S.; Ray, S.; Hawkes, M.; Wise, L.M.; Fukuzawa, R.; Macaulay, E.C.; Devenish, C.J.; et al. Human papillomavirus E6/E7 expression in preeclampsia-affected placentae. Pathogens 2020, 9, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ticconi, C.; Pietropolli, A.; Fabbri, G.; Capogna, M.V.; Perno, C.F.; Piccione, E. Recurrent miscarriage and cervical human papillomavirus infection. Am. J. Reprod. Immunol. 2013, 70, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, A.; Lees, B.F.; Becker, D.A.; Tang, Y.; Khan, M.J.; Edwards, R.K. Evaluation of Human Papillomavirus as a Risk Factor for Preterm Birth or Pregnancy-Related Hypertension. Obstet. Gynecol. 2016, 127, 233–240. [Google Scholar] [CrossRef] [PubMed]
- McDonnold, M.; Dunn, H.; Hester, A.; Pacheco, L.D.; Hankins, G.D.; Saade, G.R.; Costantine, M.M. High risk human papillomavirus at entry to prenatal care and risk of preeclampsia. Am. J. Obstet. Gynecol. 2014, 210, 138.e1–138.e5. [Google Scholar] [CrossRef]
- Mosbah, A.; Barakat, R.; Nabiel, Y.; Barakat, G. High-risk and low-risk human papilloma virus in association to spontaneous preterm labor: A case-control study in a tertiary center, Egypt. J. Matern.-Fetal Neonatal Med. 2018, 31, 720–725. [Google Scholar] [CrossRef]
- Conde-Ferráez, L.; May, A.D.A.C.; Carrillo-Martínez, J.R.; Ayora-Talavera, G.; González-Losa, M.D.R. Human papillomavirus infection and spontaneous abortion: A case-control study performed in Mexico. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 468–473. [Google Scholar] [CrossRef]
- Cho, G.; Min, K.-J.; Hong, H.-R.; Kim, S.; Hong, J.-H.; Lee, J.-K.; Oh, M.-J.; Kim, H. High-risk human papillomavirus infection is associated with premature rupture of membranes. BMC Pregnancy Childbirth 2013, 13, 173. [Google Scholar] [CrossRef] [Green Version]
- Slatter, T.L.; Hung, N.G.; Clow, W.M.; Royds, J.A.; Devenish, C.J.; Hung, N.A. A clinicopathological study of episomal papillomavirus infection of the human placenta and pregnancy complications. Mod. Pathol. 2015, 28, 1369–1382. [Google Scholar] [CrossRef] [Green Version]
- Aldhous, M.C.; Bhatia, R.; Pollock, R.; Vragkos, D.; Cuschieri, K.; Cubie, H.A.; Norman, J.E.; Stock, S.J. HPV infection and pre-term birth: A data-linkage study using Scottish Health Data [version 1; peer review: 3 approved]. Wellcome Open Res. 2019, 4, 48. [Google Scholar] [CrossRef] [Green Version]
- Ambühl, L.M.M.; Leonhard, A.K.; Zakhary, C.W.; Jørgensen, A.; Blaakaer, J.; Dybkaer, K.; Baandrup, U.; Uldbjerg, N.; Sørensen, S. Human papillomavirus infects placental trophoblast and Hofbauer cells, but appears not to play a causal role in miscarriage and preterm labor. Acta Obstet. Gynecol. Scand. 2017, 96, 1188–1196. [Google Scholar] [CrossRef] [Green Version]
- Harari, A.; Chen, Z.; Burk, R.D. Human papillomavirus genomics: Past, present and future. Curr. Probl. Dermatol. 2014, 45, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, L.; Ma, Y.; Ho, C.; McGrath, C.; Nelson, D.; Parry, S. Placental infection with human papillomavirus is associated with spontaneous preterm delivery. Hum. Reprod. 2008, 23, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- León-Juárez, M.; Martínez–Castillo, M.; González-García, L.D.; Helguera-Repetto, A.C.; Zaga-Clavellina, V.; García-Cordero, J.; Flores-Pliego, A.; Herrera-Salazar, A.; Vázquez-Martínez, E.R.; Reyes-Muñoz, E. Cellular and molecular mechanisms of viral infection in the human placenta. Pathog. Dis. 2017, 75, ftx093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on spontaneous abortion and human papillomavirus infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Meis, P.J.; Ernest, J.; Moore, M.L. Causes of low birth weight births in public and private patients. Am. J. Obstet. Gynecol. 1987, 156, 1165–1168. [Google Scholar] [CrossRef]
- Roccella, E.J. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am. J. Obstet. Gynecol. 2000, 183, s1–s22. [Google Scholar] [CrossRef]
- Sharma, D.; Shastri, S.; Sharma, P. Intrauterine Growth Restriction: Antenatal and Postnatal Aspects. Clin. Med. Insights Pediatrics 2016, 10, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference, Author, Year | Title | Journal | Study Design | No. of Patient | HPV Detection Tissue | Preterm Birth | Premature Rupture of Membranes (PROM) | Miscarriage | Pregnancy Induced Hypertensive Disease | Fetal Growth Restriction | Fetal Death | Study Limitation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bober, 2019 [12] | Influence of human Papilloma Virus (hPV) infection on early pregnancy | Ginekol Pol | Case-control | 143 | Cervical, trophoblast, placenta | HR-HPV more prevalent among study group; p = 0.02 | Limited sample size, limited statistical power | |||||
| Wu, 2021 [13] | Systematic review and meta-analysis on influence of human papillomavirus infection during pregnancy on premature rupture of membranes and premature delivery | Ann Palliat Med | Systematic review and meta-analysis—7 studies included | 45,603 22,799 = control group 22,799 = study group | Cervical, placenta | OR = 1.81, p < 0.05 | OR =1.74, p < 0.05 | Contradictory treatments and no randomization reports among the studies included, different retrieval mechanisms | ||||
| Hornychova, 2018 [24] | Cervical human papillomavirus infection in women with preterm prelabor rupture of membranes | PLoS ONE | Case-control | 100 | Cervical, placenta | p = 1.00 HPV infection is not a risk factor | Limited sample size, no HPV detecting thru the amniotic fluid | |||||
| Pandey, 2019 [23] | Human Papillomavirus (HPV) Infection in Early Pregnancy: Prevalence and Implications | Infect Dis Obstet Gynecol | Prospective study | 104 | cervical | p = 0.324 | p = 0.026 | p = 0.100 | p = 0.470 | p = 0.100 | Limited sample size, only one time testing in the first trimester: new infection? And clearance during pregnancy? | |
| Xiong, 2018 [29] | The Risk of Human Papillomavirus Infection for Spontaneous Abortion, Spontaneous Preterm Birth, and Pregnancy Rate of Assisted Reproductive Technologies: A Systematic Review and Meta-Analysis | Gynecol Obstet Invest | Systematic review and meta-analysis—18 studies included | 6116 | Cervical, placenta, amniotic fluid | HR-HPV OR: 2.84 | indiscriminate genotype HPV infection OR: 2.24 meanwhile HR-HPV OR: 0.65 | significant heterogeneity among the included studies; not report other adverse pregnancy outcomes risk factors | ||||
| Niyibizi, 2020 [30] | Association Between Maternal Human Papillomavirus Infection and Adverse Pregnancy Outcomes: Systematic Review and Meta-Analysis | J Infect Dis | Systematic review and meta-analysis—36 studies included | 342,796 | Cervical, placental, amniotic fluid | aOR: 1.50 | aOR: 1.96 | aOR: 1.14 | aOR: 1.24 | aOR: 1.17 | aOR: 2.23 | significant heterogeneity among the included studies, no standardization among HPV testing, no clear identification of possible negative cofactors, misclassification of pregnancy outcomes |
| Ambühl, 2016 [31] | Human Papillomavirus Infection as a Possible Cause of Spontaneous Abortion and Spontaneous Preterm Delivery | Infect Dis Obstet Gynecol | Review 45 studies included | 15,868 | Cervical, placental, ombilical, amniotic fluid | p < 0.01 | p < 0.05 | significant heterogeneity among the included studies, inaccurate and inhomogeneous inclusion and exclusion criteria used, no cofactors investigated, different time of HPV testing | ||||
| Chilaka, 2021 [32] | Human papillomavirus (HPV) in pregnancy—An update | Eur J Obstet Gynecol Reprod Biol | review | aOR: 1.5 | aOR: 1.42 | No association | No association | aOR: 1.17 | aOR: 2.23 | Heterogenic data, insufficient documentation of correlation between infection and adverse pregnancy outcomes | ||
| Condrat, 2021 [33] | Maternal HPV Infection: Effects on Pregnancy Outcome | Viruses | Systematic review 17 studies included | 479,204 | Cervical, placenta, amniotic fluid | x | x | x | x | x | x | Heterogenic data report, no statistical analyses only descriptive study |
| Basonidis, 2020 [34] | Human papilloma virus infection and miscarriage: is there an association? | Taiwanese Journal of Obstetrics and Gynecology | review | 45,373 | Unclear if there is any association | Descriptive study, no statistical analyses, heterogenic data, no cofactors investigated | ||||||
| Caballero, 2019 [35] | Maternal Human Papillomavirus and Preterm Premature Rupture of Membranes: A Retrospective Cohort Study | J Womens Health (Larchmt) | Retrospective Cohort Study | 2153 829 HPV positive 1324 HPV negative | cervical | OR: 1.35, p = 0.04 | OR: 2.07, p = 0.16 | OR: 5.76, p < 0.001 | interaction between HPV and other pathogenic organisms was not assessed in the study, limited population | |||
| Subramaniam, 2016 [38] | Evaluation of Human Papillomavirus as a Risk Factor for Preterm Birth or Pregnancy-Related Hypertension | Obstet Gynecol | retrospective cohort study | 2321 242 HPV positive, 2079 HPV negative | cervical | OR: 1.3 | OR: 1.7 | OR: 1.0 | Retrospective study, HPV testing identifying only HR-HPV, no data about HPV clearance, 3 years interval for HPV testing positive | |||
| Reily-Bell, 2020 [36] | Human Papillomavirus E6/E7 Expression in Preeclampsia-Affected Placentae | Pathogens | Case control | 96 | placenta | HR-HPV, p = 0.017; LR-HPV, p = 0.033 | No other sexually transmitted disease detected into the placenta | |||||
| McDonnold, 2014 [39] | High risk human papillomavirus at entry to prenatal care and risk of preeclampsia | Am J Obstet Gynecol | Retrospective cohort study | 942 | cervical | aOR:1.83, p = 0.04 | HR-HPV aOR: 2.18, p = 0.004 | Retrospective study, does not study causality, does not evaluate proteinuria or other co-factors involved in pathogenesis | ||||
| Ticconi, 2013 [37] | Recurrent miscarriage and cervical human papillomavirus infection | Am J Reprod Immunol | Retrospective case-control study | 524 | cervical | Lower HPV infection prevalence in patients with recurrent miscarriage: 26.53% vs. 61.89%, p < 0.001 | Retrospective study, different method of HPV detection | |||||
| Ambühl, 2017 [45] | Human papillomavirus infects placental trophoblast and Hofbauer cells, but appears not to play a causal role in miscarriage and preterm labor | Acta Obstet Gynecol Scand | prospective case-control study | 270 | placenta | HPV prevalence in study group vs. control group:8.8%vs. 8.7%, p = 0.98 | HPV prevalence in study group vs. control group: 10.9% vs. 20.4%, p = 0.19 | Elective abortion as a control group | ||||
| Mosbah, 2017 [40] | High-risk and low-risk human papilloma virus in association to spontaneous preterm labor: a case-control study in a tertiary center, Egypt | J Matern Fetal Neonatal Med | observational comparative case-control study | 103 | placenta | HPV prevalence in study group vs. control group 18.1% vs. 4%, p = 0.019 | Limited sample size | |||||
| Conde-Ferráez, 2013 [41] | Human papillomavirus infection and spontaneous abortion: a case-control study performed in Mexico | Eur J Obstet Gynecol Reprod Biol | Case control study | 281 | cervical | OR: 1.80, p = 0.0538 | Limited sample size, no standardization regarding the moment of HPV detection | |||||
| Cho, 2013 [42] | High-risk human papillomavirus infection is associated with premature rupture of membranes | BMC Pregnancy Childbirth | cross-sectional study | 311 | cervical | p = 0.718 | OR: 2.380, p = 0.029 | p = 0.054 | Cross-sectional study, limited sample size, no cofactors investigated | |||
| Slatter, 2015 [43] | A clinicopathological study of episomal papillomavirus infection of the human placenta and pregnancy complications | Mod Pathol | Case control | 339 253 HPV positive vs. 86 HPV negative | placenta | s.d 29.2% vs. 16.3%, OR: (odds ratio 2.13, p = 0.018 | 7.9% vs. 0%; OR: 8.4, p < 0.05 | 22.4% vs. 19.8%, p = 0.02 | 5.1% vs. 3.5% | no possible cofactors were identified, limited sample size heterogenous data | ||
| Aldhous, 2019 [44] | HPV infection and pre-term birth: a data-linkage study using Scottish Health Data | Wellcome Open Res | data-linkage study | 5598 | cervical | OR: 1.843, p = 0.020 | No data about HPV treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popescu, S.D.; Boiangiu, A.G.; Sima, R.-M.; Bilteanu, L.; Vladareanu, S.; Vladareanu, R. Maternal HPV Infection and the Estimated Risks for Adverse Pregnancy Outcomes—A Systematic Review. Diagnostics 2022, 12, 1471. https://doi.org/10.3390/diagnostics12061471
Popescu SD, Boiangiu AG, Sima R-M, Bilteanu L, Vladareanu S, Vladareanu R. Maternal HPV Infection and the Estimated Risks for Adverse Pregnancy Outcomes—A Systematic Review. Diagnostics. 2022; 12(6):1471. https://doi.org/10.3390/diagnostics12061471
Chicago/Turabian StylePopescu, Simona Daniela, Andreea Gratiana Boiangiu, Romina-Marina Sima, Liviu Bilteanu, Simona Vladareanu, and Radu Vladareanu. 2022. "Maternal HPV Infection and the Estimated Risks for Adverse Pregnancy Outcomes—A Systematic Review" Diagnostics 12, no. 6: 1471. https://doi.org/10.3390/diagnostics12061471