
Acute Eosinophilic Pneumonia Complicated with Venous Thromboembolic Disease—Diagnostic and Therapeutic Considerations

 ,
,
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suzuki, Y.; Suda, T. Eosinophilic Pneumonia: A Review of the Previous Literature, Causes, Diagnosis, and Management. Allergol. Int. 2019, 68, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Chaaban, T. Acute Eosinophilic Pneumonia Associated with Non-Cigarette Smoking Products: A Systematic Review. Adv. Respir. Med. 2020, 88, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.; Correia, S.; Lima, A.L.; Costa, M.; Neves, I. SARS-CoV-2 as a Trigger of Eosinophilic Pneumonia. Pulmonology 2022, 28, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Carlicchi, E.; Gemma, P.; Poerio, A.; Caminati, A.; Vanzulli, A.; Zompatori, M. Chest-CT Mimics of COVID-19 Pneumonia-a Review Article. Emerg. Radiol. 2021, 28, 507–518. [Google Scholar] [CrossRef]
- Samoszuk, M.; Corwin, M.; Hazen, S.L. Effects of Human Mast Cell Tryptase and Eosinophil Granule Proteins on the Kinetics of Blood Clotting. Am. J. Hematol. 2003, 73, 18–25. [Google Scholar] [CrossRef]
- Réau, V.; Vallée, A.; Terrier, B.; Plessier, A.; Abisror, N.; Ackermann, F.; Benainous, R.; Bohelay, G.; Chabi-Charvillat, M.-L.; Cornec, D.; et al. Venous Thrombosis and Predictors of Relapse in Eosinophil-Related Diseases. Sci. Rep. 2021, 11, 6388. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism Developed in Collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- De Giacomi, F.; Vassallo, R.; Yi, E.S.; Ryu, J.H. Acute Eosinophilic Pneumonia. Causes, Diagnosis, and Management. Am. J. Respir. Crit. Care Med. 2018, 197, 728–736. [Google Scholar] [CrossRef]
- Leurs, A.; Chenivesse, C.; Lopez, B.; Gibier, J.B.; Clément, G.; Groh, M.; Copin, M.C.; Staumont-Sallé, D.; Mortuaire, G.; Balquet, M.H.; et al. C-Reactive protein as a diagnostic tool in differential diagnosis of hypereosinophilic syndrome and antineutrophil cytoplasmic antibody-negative eosinophilic granulomatosis with polyangiitis. J. Allergy Clin. Immunol. Pract. 2019, 7, 1347–1351.e3. [Google Scholar] [CrossRef]
- Liu, X.; Sun, W.; Meng, W.; Xiao, Y.; Feng, G.; Shi, B. Cigarette Smoking-Induced Acute Eosinophilic Pneumonia: A Case Report. Medicine 2019, 98, e14704. [Google Scholar] [CrossRef]
- Nakajima, M.; Matsushima, T. Acute Eosinophilic Pneumonia Following Cigarette Smoking. Intern. Med. 2000, 39, 759–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagome, K.; Nagata, M. Possible Mechanisms of Eosinophil Accumulation in Eosinophilic Pneumonia. Biomolecules 2020, 10, 638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, T.L.; Rada, B.; Tandon, E.; Gestal, M.C. NETs and EETs, a Whole Web of Mess. Microorganisms 2020, 8, 1925. [Google Scholar] [CrossRef] [PubMed]
- Sherer, Y.; Salomon, O.; Livneh, A.; Pras, M.; Langevitz, P. Thromboembolism in a Patient with Transient Eosinophilia and Thrombocytopenia. Clin. Lab. Haematol. 2000, 22, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Sakamoto, S.; Ueki, S.; Miyabe, Y.; Fukuchi, M.; Okuda, Y.; Asano, M.; Sato, K.; Nakayama, K. Eosinophil Extracellular Traps in a Patient with Chronic Eosinophilic Pneumonia. Asia Pac. Allergy 2021, 11, e24. [Google Scholar] [CrossRef] [PubMed]
- Francischetti, I.M.B.; Alejo, J.C.; Sivanandham, R.; Davies-Hill, T.; Fetsch, P.; Pandrea, I.; Jaffe, E.S.; Pittaluga, S. Neutrophil and Eosinophil Extracellular Traps in Hodgkin Lymphoma. Hemasphere 2021, 5, e633. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.D.; Moll, S.; Dellon, E.S. Pulmonary Embolism in a Patient with Eosinophilic Esophagitis: Causal or Coincidental? Case Rep. Gastroenterol. 2013, 7, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Ghaffar, T.Y.A.; Elfaramawy, A.A.M.; El Saied, S.; El Adawy, M.; Sakr, M.A.; Zalata, K. Hepatic Venous Outflow Obstruction Complicating Churg-Strauss Syndrome in a 5-Year-Old Child. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 217–218. [Google Scholar] [CrossRef]
- Moon, C.-J.; Kwon, T.H.; Lee, H.-S. Portal Vein Thrombosis and Food Protein-Induced Allergic Proctocolitis in a Premature Newborn with Hypereosinophilia: A Case Report. BMC Pediatr. 2021, 21, 49. [Google Scholar] [CrossRef]
- Leiva, O.; Baker, O.; Jenkins, A.; Brunner, A.M.; Al-Samkari, H.; Leaf, R.K.; Rosovsky, R.P.; Fathi, A.T.; Weitzman, J.; Bornikova, L.; et al. Association of Thrombosis with Hypereosinophilic Syndrome in Patients with Genetic Alterations. JAMA Netw. Open. 2021, 4, e2119812. [Google Scholar] [CrossRef]
- Li, D.; Xu, L.; Lin, D.; Jiang, S.; Feng, S.; Zhu, L. Acute Pulmonary Embolism and Deep Vein Thrombosis Secondary to Idiopathic Hypereosinophilic Syndrome. Respir. Med. Case Rep. 2018, 25, 213–215. [Google Scholar] [CrossRef]
- Ding, F.; Wu, C.; Li, Y.; Mukherjee, S.; Ghosh, S.; Arrossi, A.V.; Krishnan, S. A Case of Hypereosinophilic Syndrome with STAT5b N642H Mutation. Oxf. Med. Case Rep. 2021, 2021, omaa129. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.K.; Min, K.H.; Yim, N.Y.; Lee, J.E.; Lee, N.R.; Chung, M.P.; Jeon, K. Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia. Eur. Respir. J. 2013, 41, 402–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zöller, B.; Svensson, P.J.; Dahlbäck, B.; Lind-Hallden, C.; Hallden, C.; Elf, J. Genetic Risk Factors for Venous Thromboembolism. Expert Rev. Hematol. 2020, 13, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Zuk, J.; Papuga-Szela, E.; Zareba, L.; Undas, A. Direct Oral Anticoagulants in Patients with Severe Inherited Thrombophilia: A Single-Center Cohort Study. Int. J. Hematol. 2021, 113, 190–198. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| On Admission | On Discharge | 4 Months Follow-Up | Reference Range | |
|---|---|---|---|---|
| Body temperature (°C) | 38–39 | Normal | Normal | Normal |
| White blood cell count (WBC) (×109/L) | 13.8 | 6.53 | 6.65 | 3.98–10.04 |
| Eosinophil count (×109/L) | 3.07 | 0.57 | 0.14 | 0.04–0.36 |
| Eosinophils (%) | 22 | 8.7 | 2.1 | 0.7–5.8 |
| C-reactive protein (CRP) (mg/L) | 81 | 28 | <5 | <5 |
| D-dimer (ng/mL) | 25,491 | 7567 | 176 | <500 |
| PaO2 (mmHg) | 62 | 71.5 | 102.2 | 65–90 |
| PaCO2 (mmHg) | 32 | 37.1 | 41.6 | 35–45 |
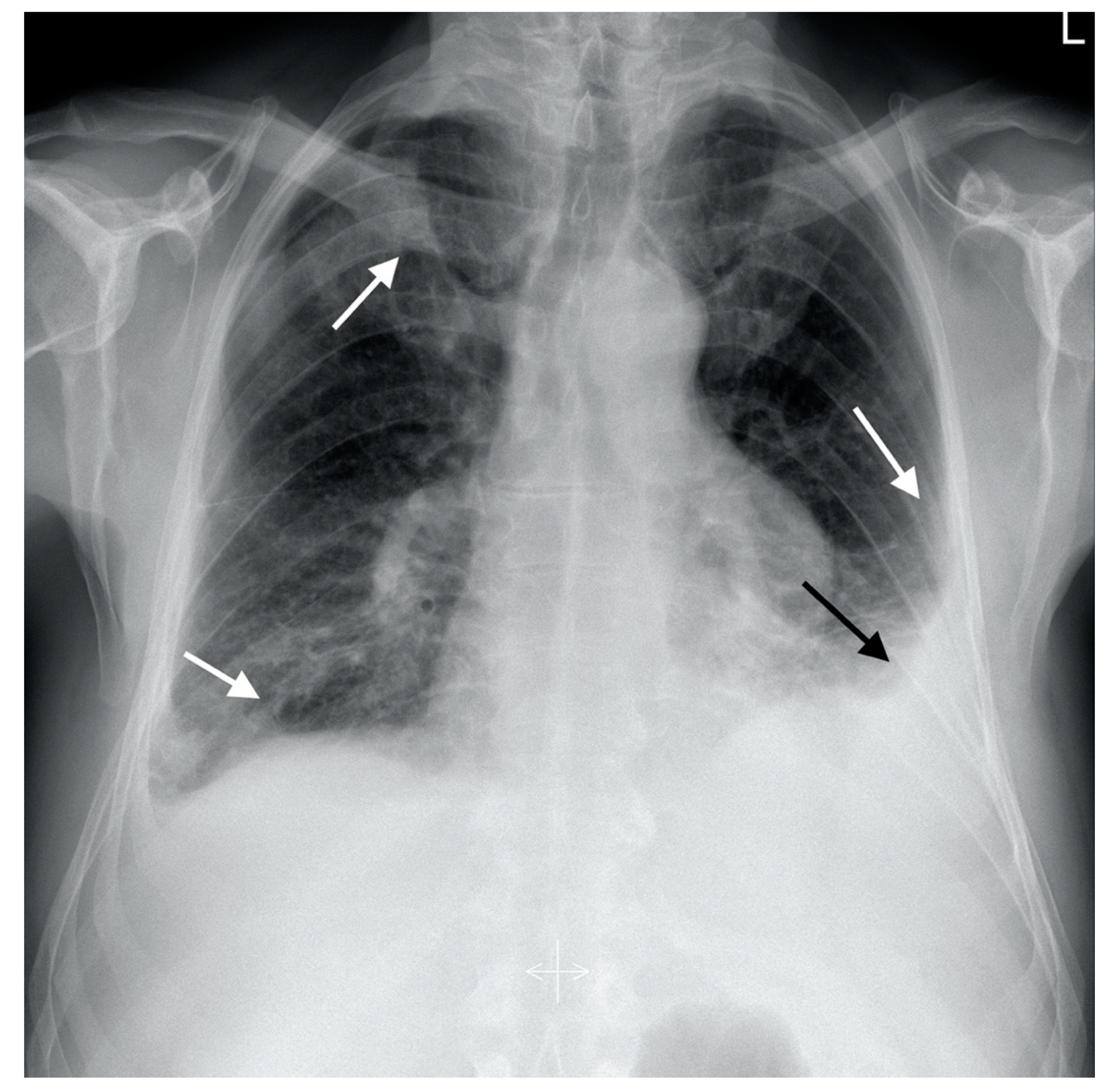
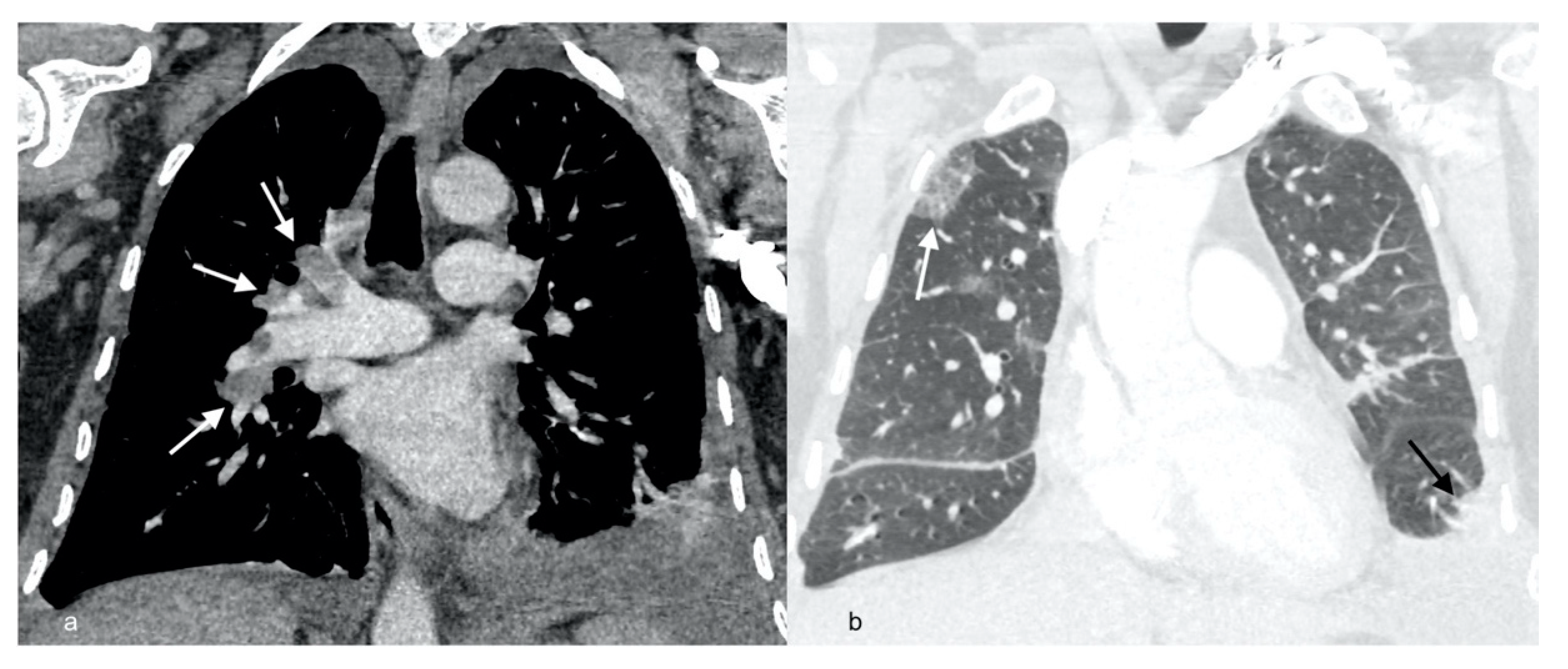
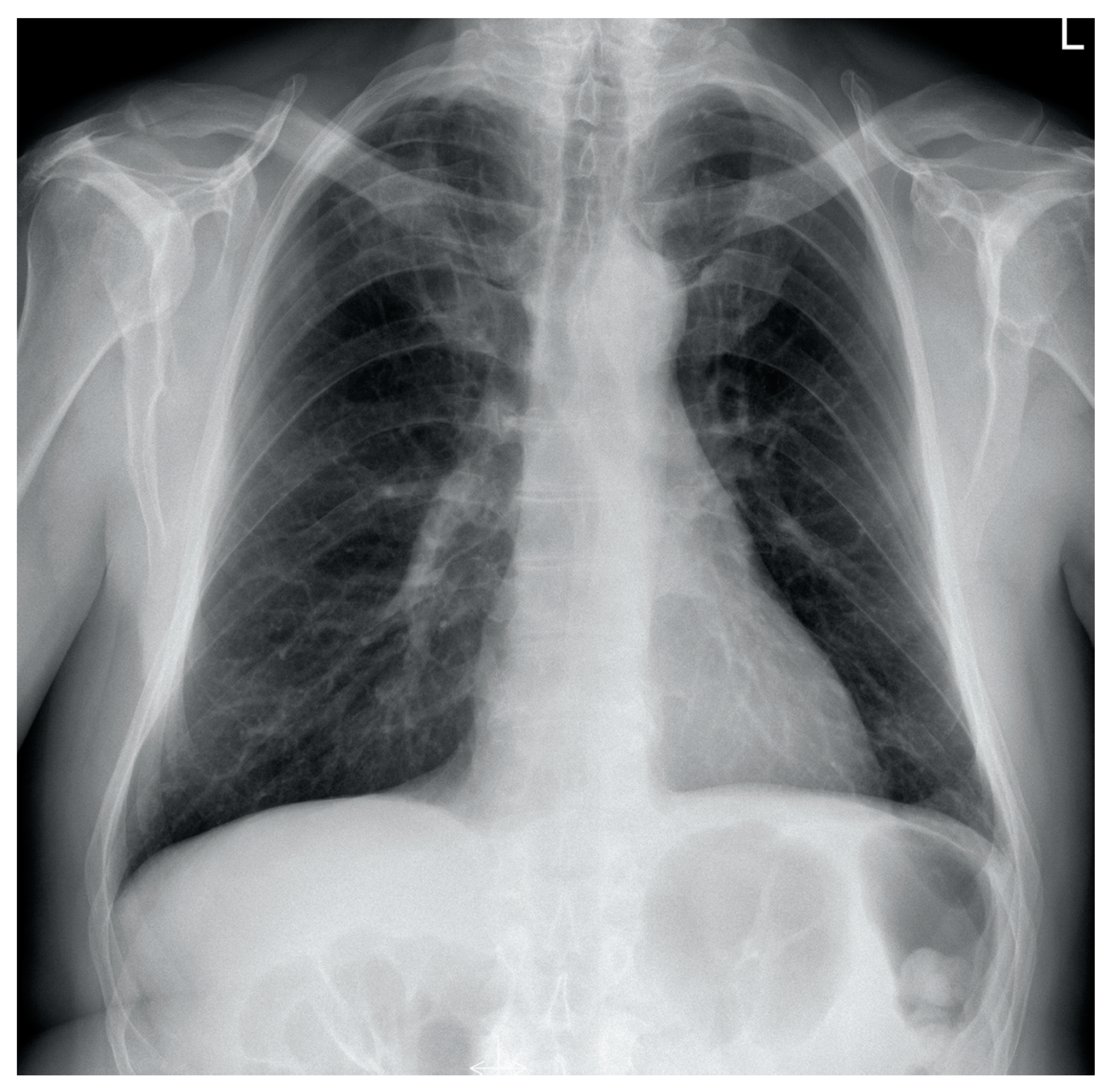
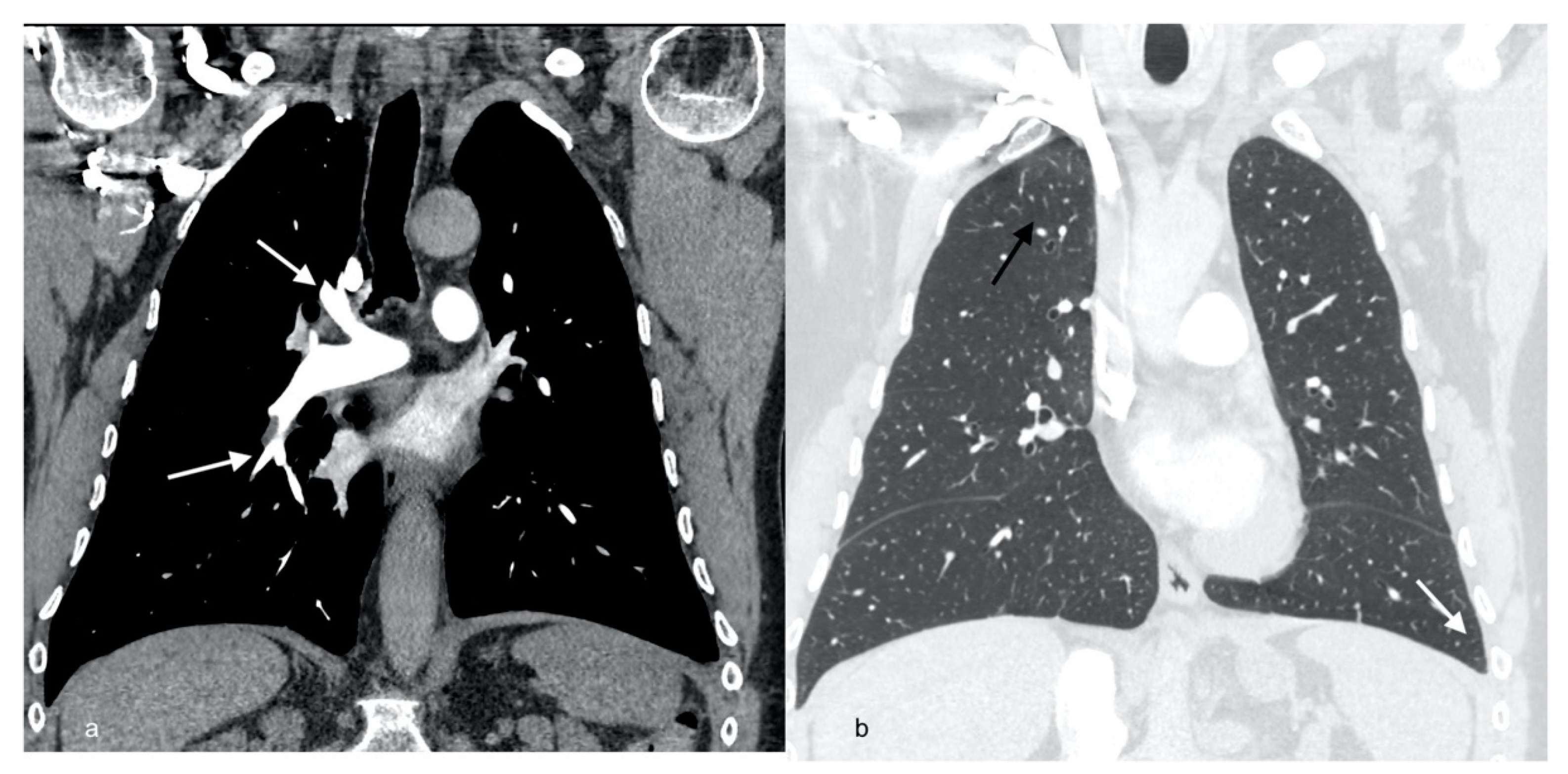
| Radiological picture | Pulmonary embolism, parenchymal infiltrates, bilateral pleural fluid | Regression of PA thrombi, pleural fluid and parenchymal consolidations | Complete resolution of PA thrombi, pleural fluid and lung consolidations | |
| Doppler ultrasonography | Massive venous thrombosis of left lower limb | Complete recanalization of femoral vein, organizing thrombi comprising up to 40% of femoral vein and 40–75% of popliteal vein | ||
| Echocardiography | Mild pulmonary hypertension (TRG 34 mmHg, AcT 90 ms) | No evidence of pulmonary hypertension (TRG 25 mmHg) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jankowska, E.; Bartoszuk, I.; Lewandowska, K.; Dybowska, M.; Opoka, L.; Tomkowski, W.; Szturmowicz, M. Acute Eosinophilic Pneumonia Complicated with Venous Thromboembolic Disease—Diagnostic and Therapeutic Considerations. Diagnostics 2022, 12, 1425. https://doi.org/10.3390/diagnostics12061425
Jankowska E, Bartoszuk I, Lewandowska K, Dybowska M, Opoka L, Tomkowski W, Szturmowicz M. Acute Eosinophilic Pneumonia Complicated with Venous Thromboembolic Disease—Diagnostic and Therapeutic Considerations. Diagnostics. 2022; 12(6):1425. https://doi.org/10.3390/diagnostics12061425
Chicago/Turabian StyleJankowska, Ewa, Iwona Bartoszuk, Katarzyna Lewandowska, Małgorzata Dybowska, Lucyna Opoka, Witold Tomkowski, and Monika Szturmowicz. 2022. "Acute Eosinophilic Pneumonia Complicated with Venous Thromboembolic Disease—Diagnostic and Therapeutic Considerations" Diagnostics 12, no. 6: 1425. https://doi.org/10.3390/diagnostics12061425