
Development of a Fully Automated Graf Standard Plane and Angle Evaluation Method for Infant Hip Ultrasound Scans

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.2. The Fully Automated DDH Diagnosis Framework
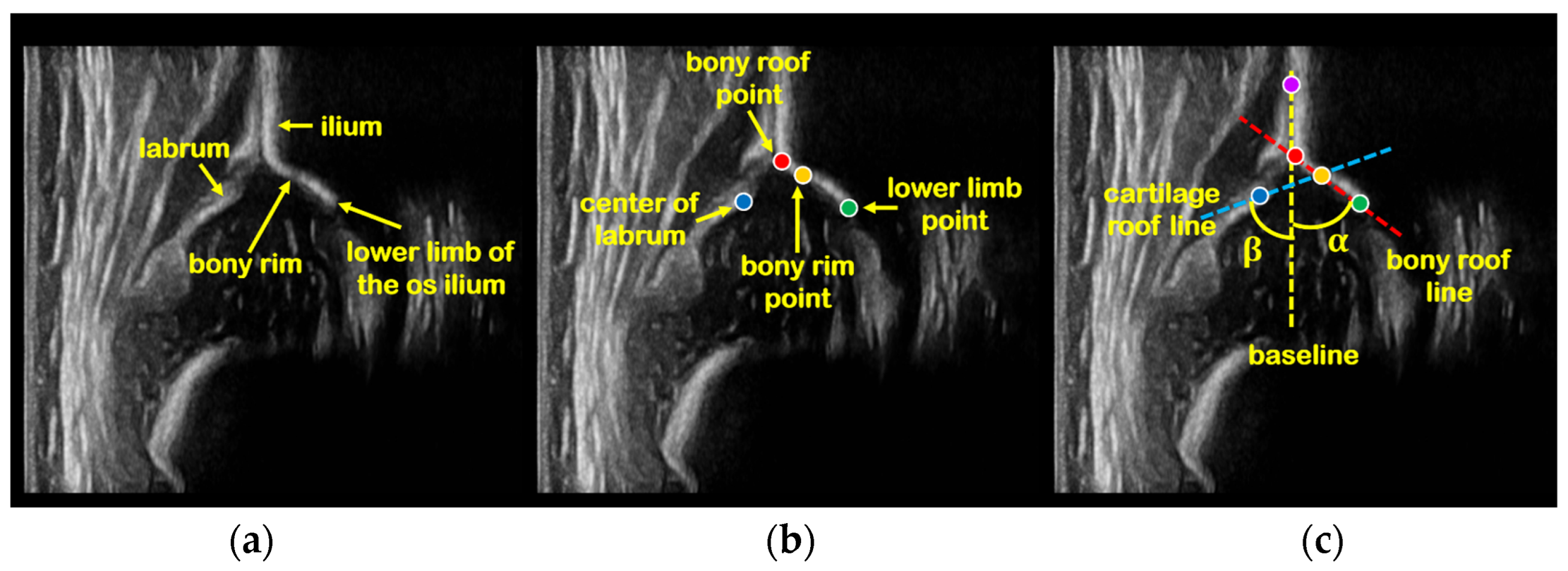
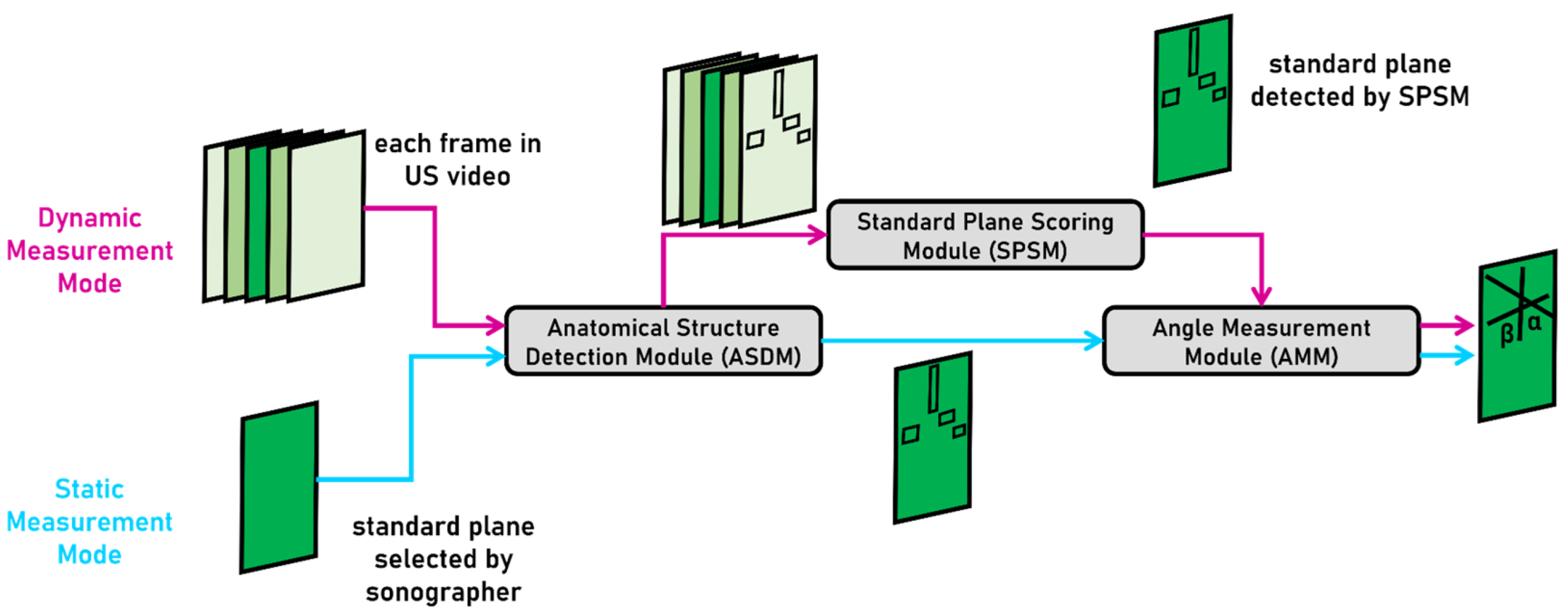
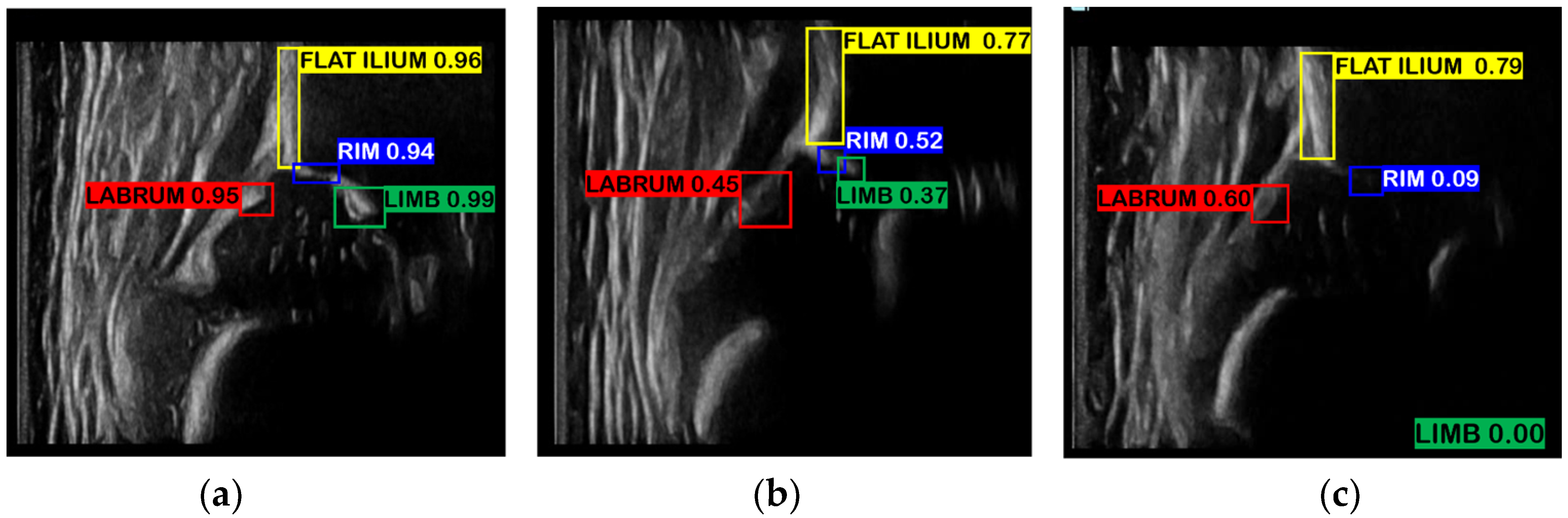
- Static measurement mode (SM mode): Based on the standard plane US image selected by sonographer, ASDM is first used to detect four key anatomical structures in this image: ilium, labrum, bony rim, and lower limb of the os ilium. AMM is then used to generate landmarks followed by measurement of α, β angles.
- Dynamic measurement mode (DM mode): ASDM is first used to detect the four key anatomical structures in each frame of a hip US video, and SPSM is then used to quantify the quality of each frame according to the scoring formula we designed, and finally, AMM is used to measure α, β angles of the highest-scoring frame.
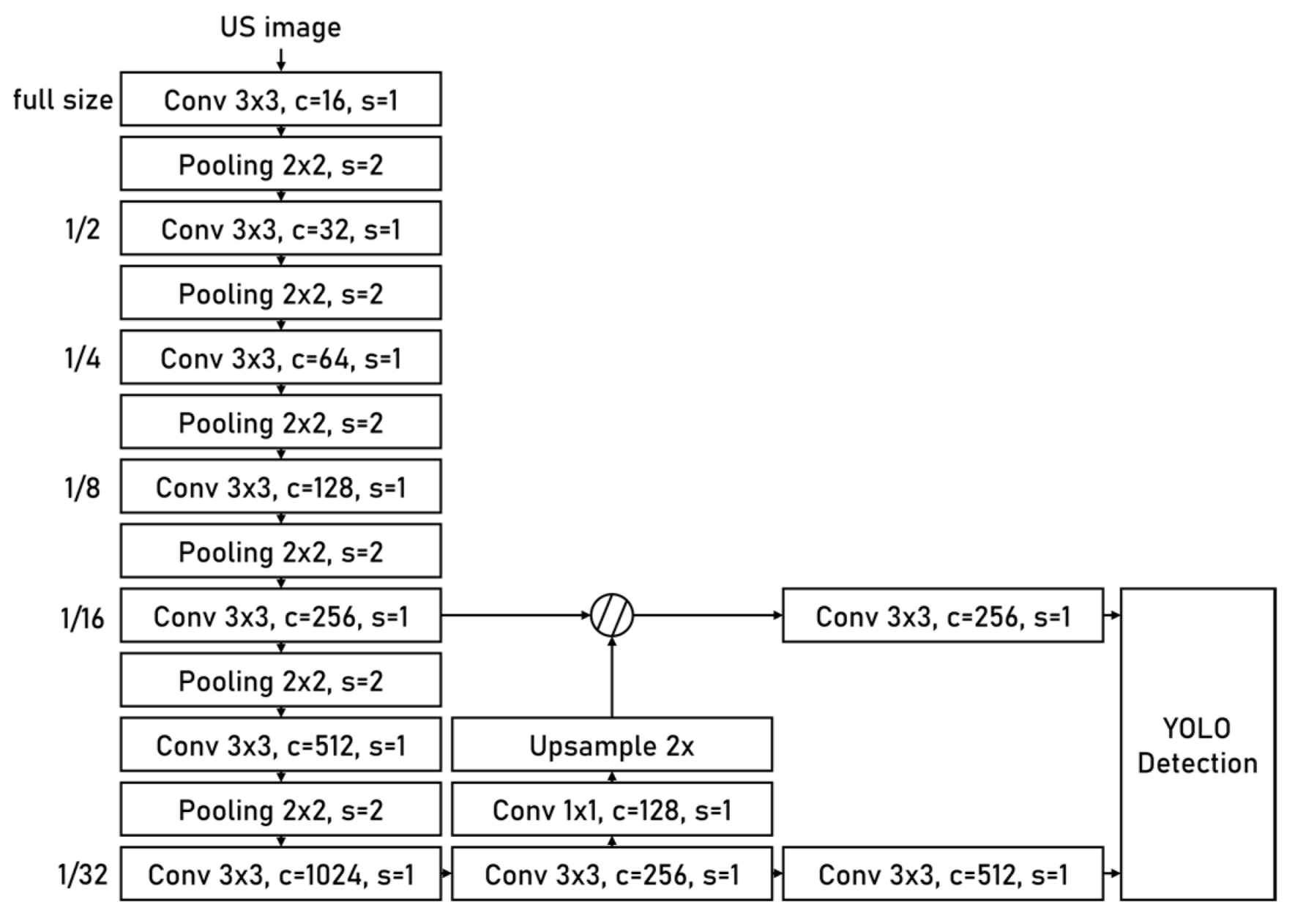
2.2.1. Anatomical Structure Detection Module
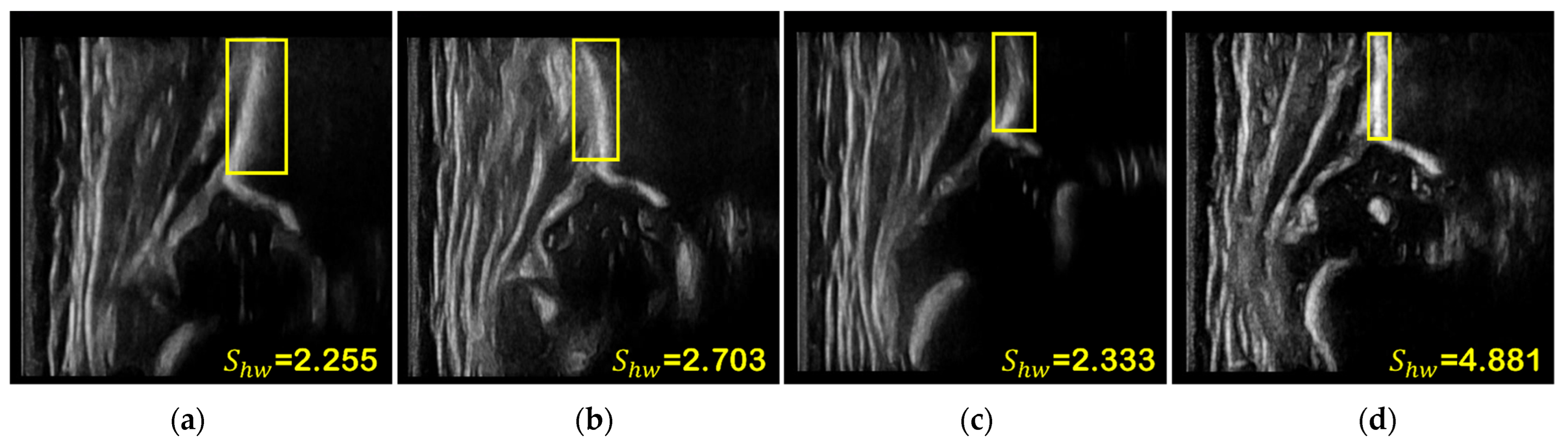
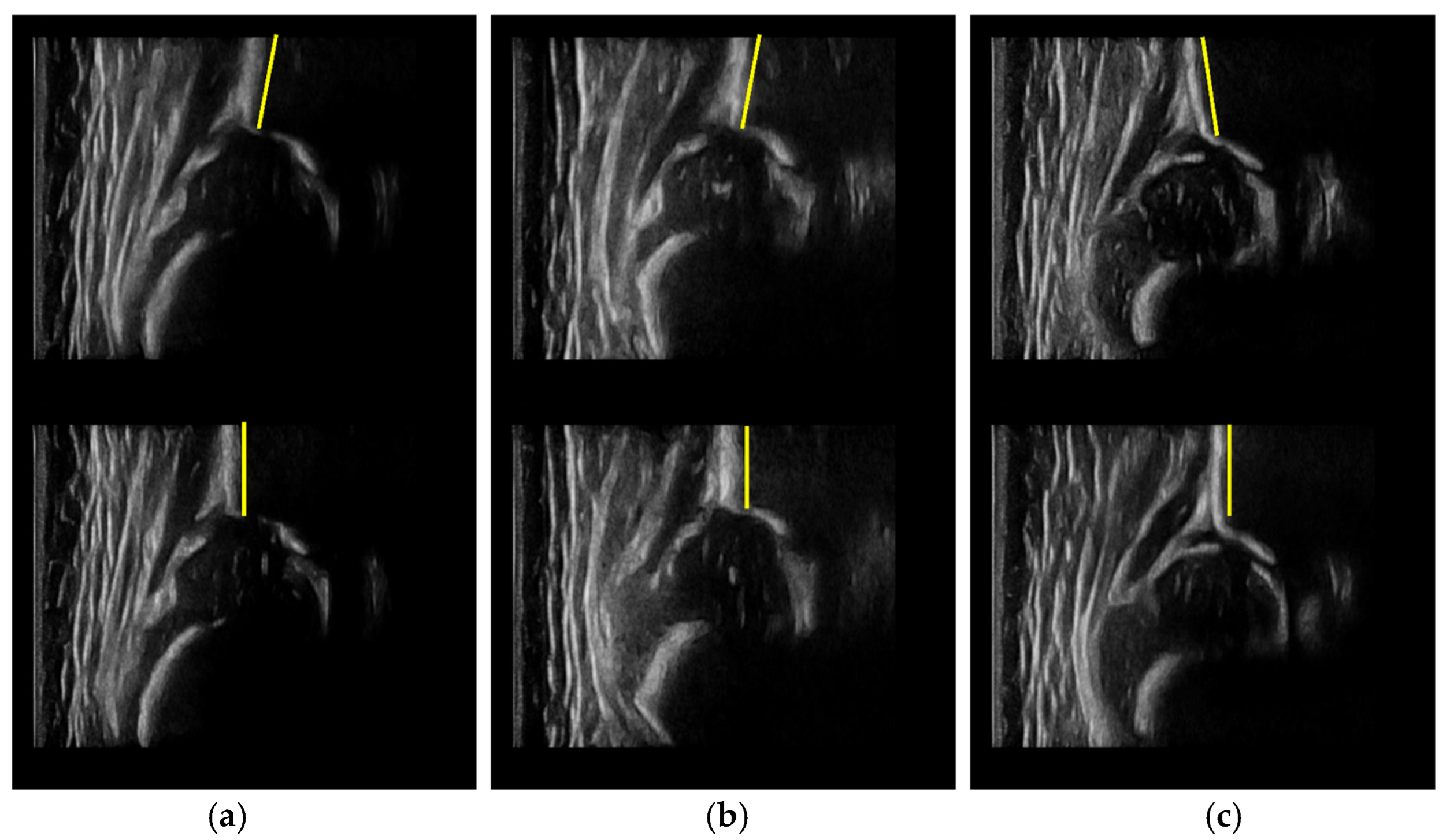
2.2.2. Standard Plane Scoring Module
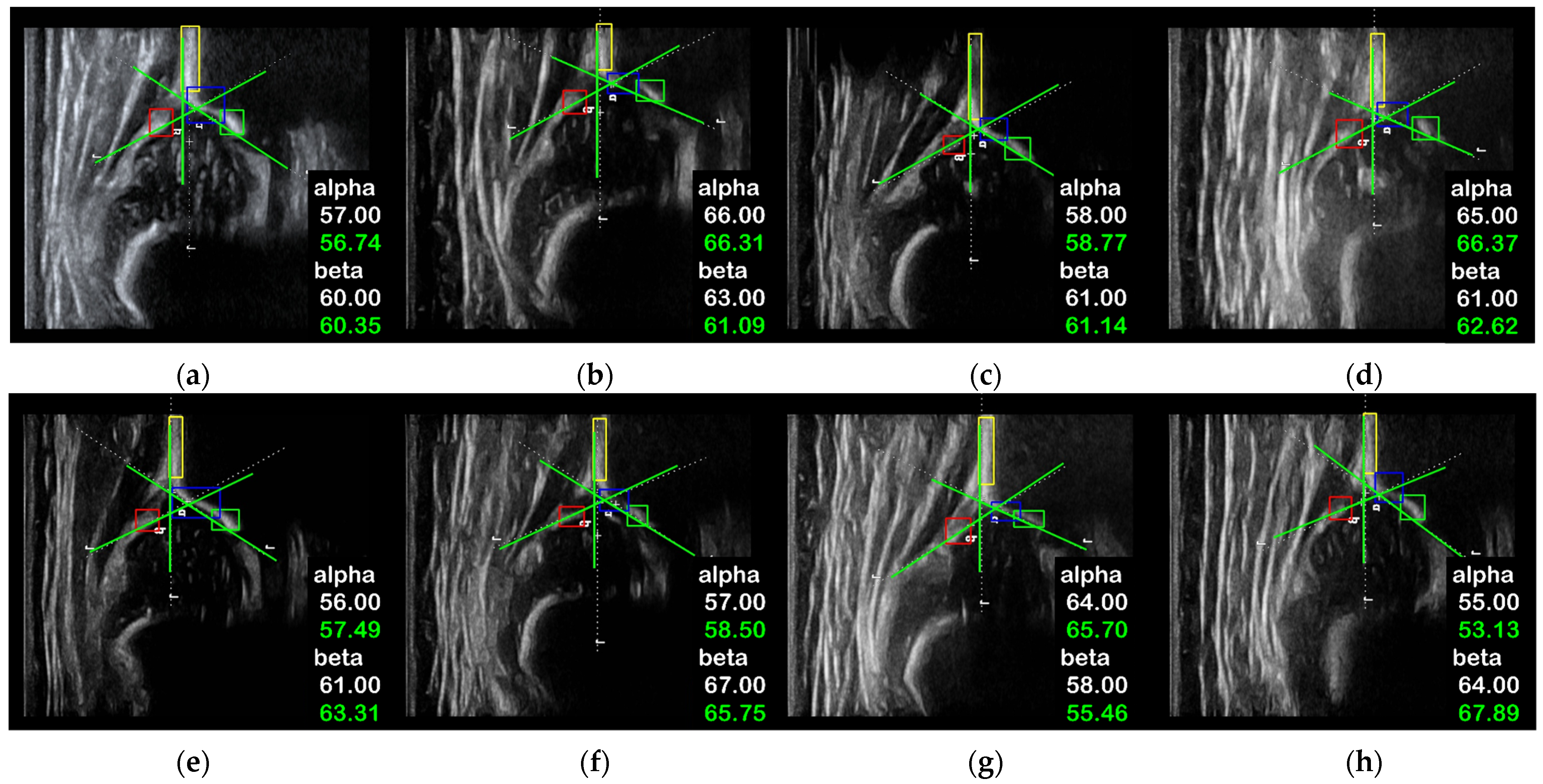
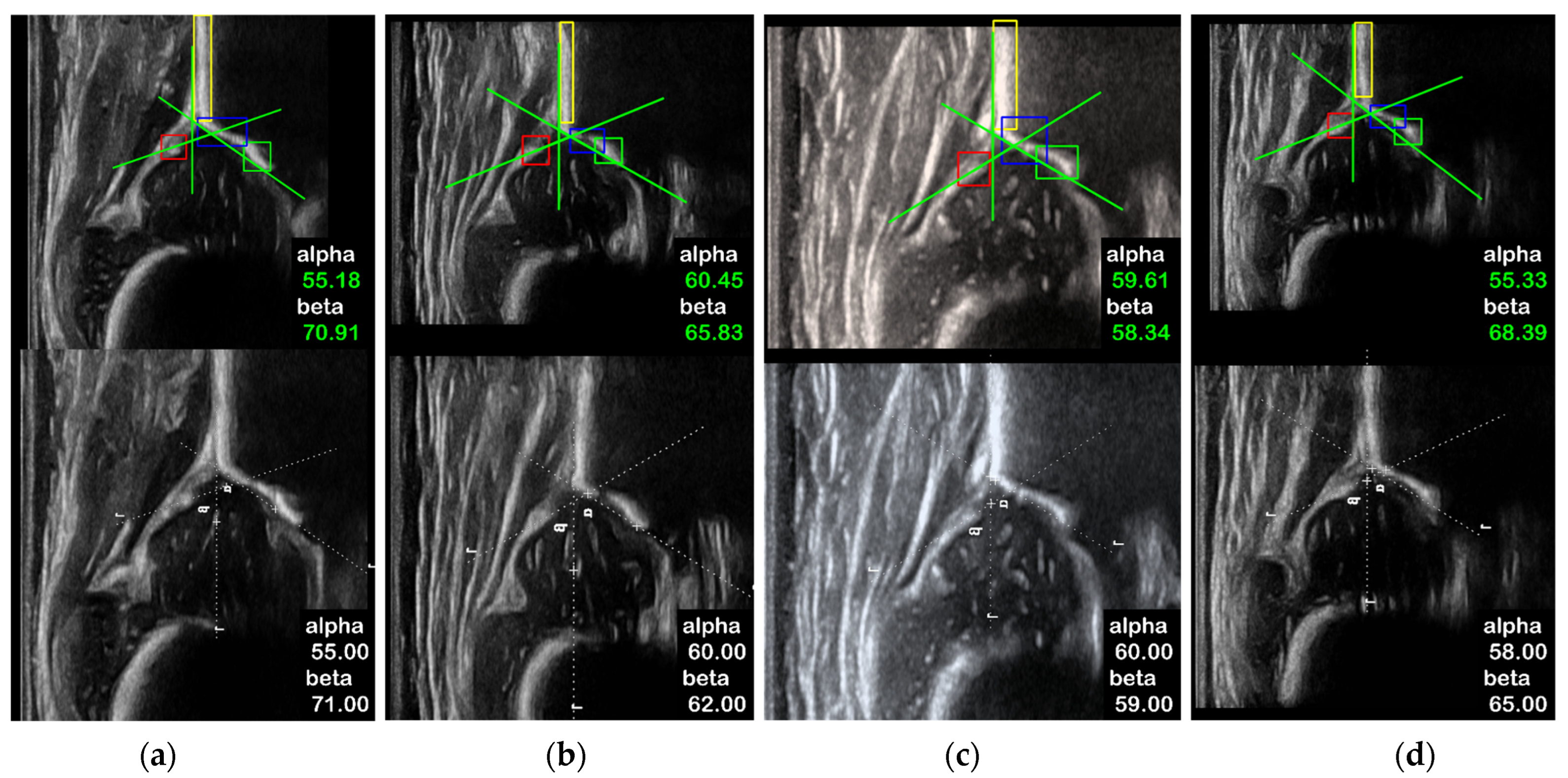
2.2.3. Angle Measurement Module
2.3. Experiment Design
3. Results
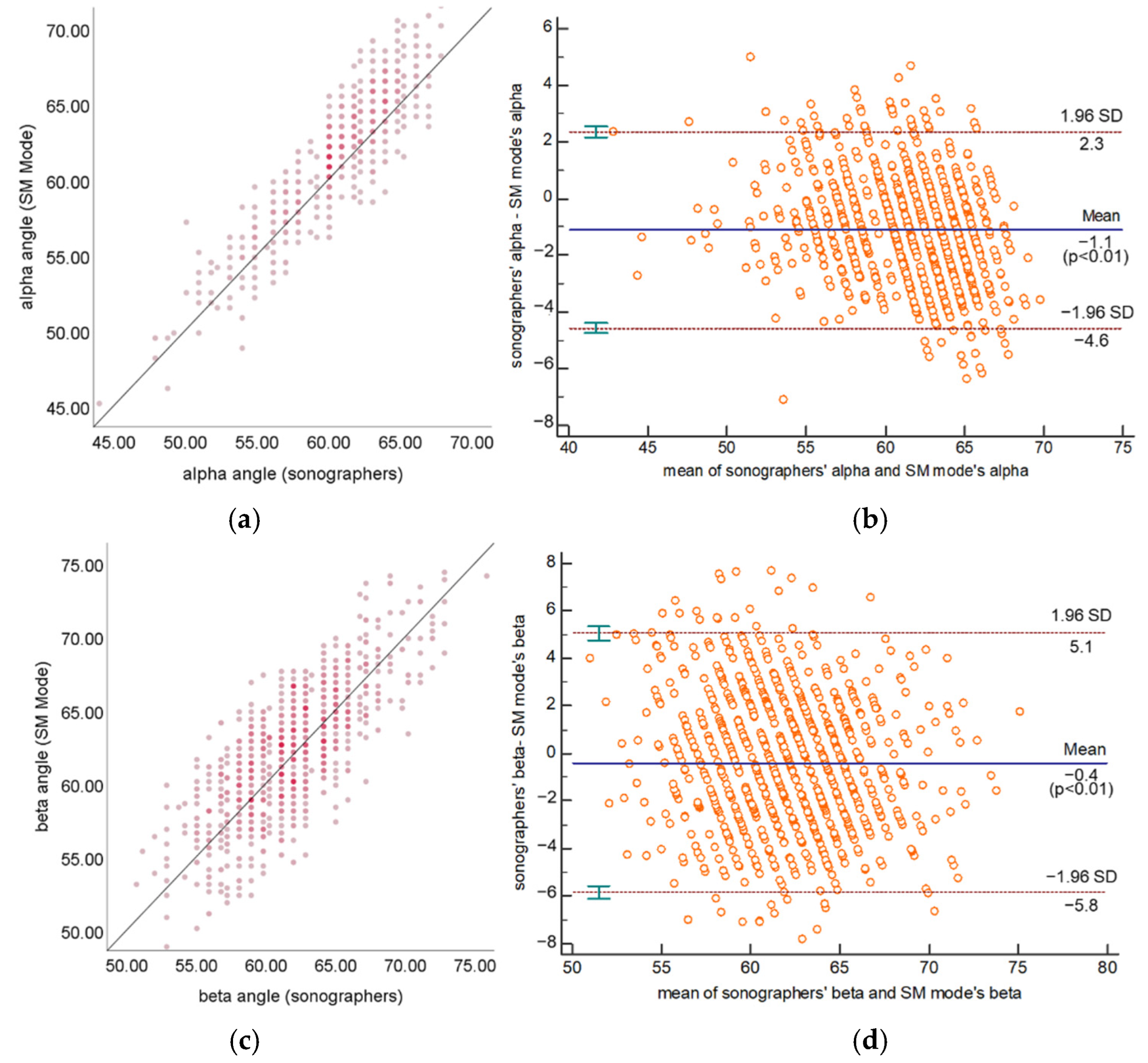
3.1. Statistical Results of Static Measurement Mode
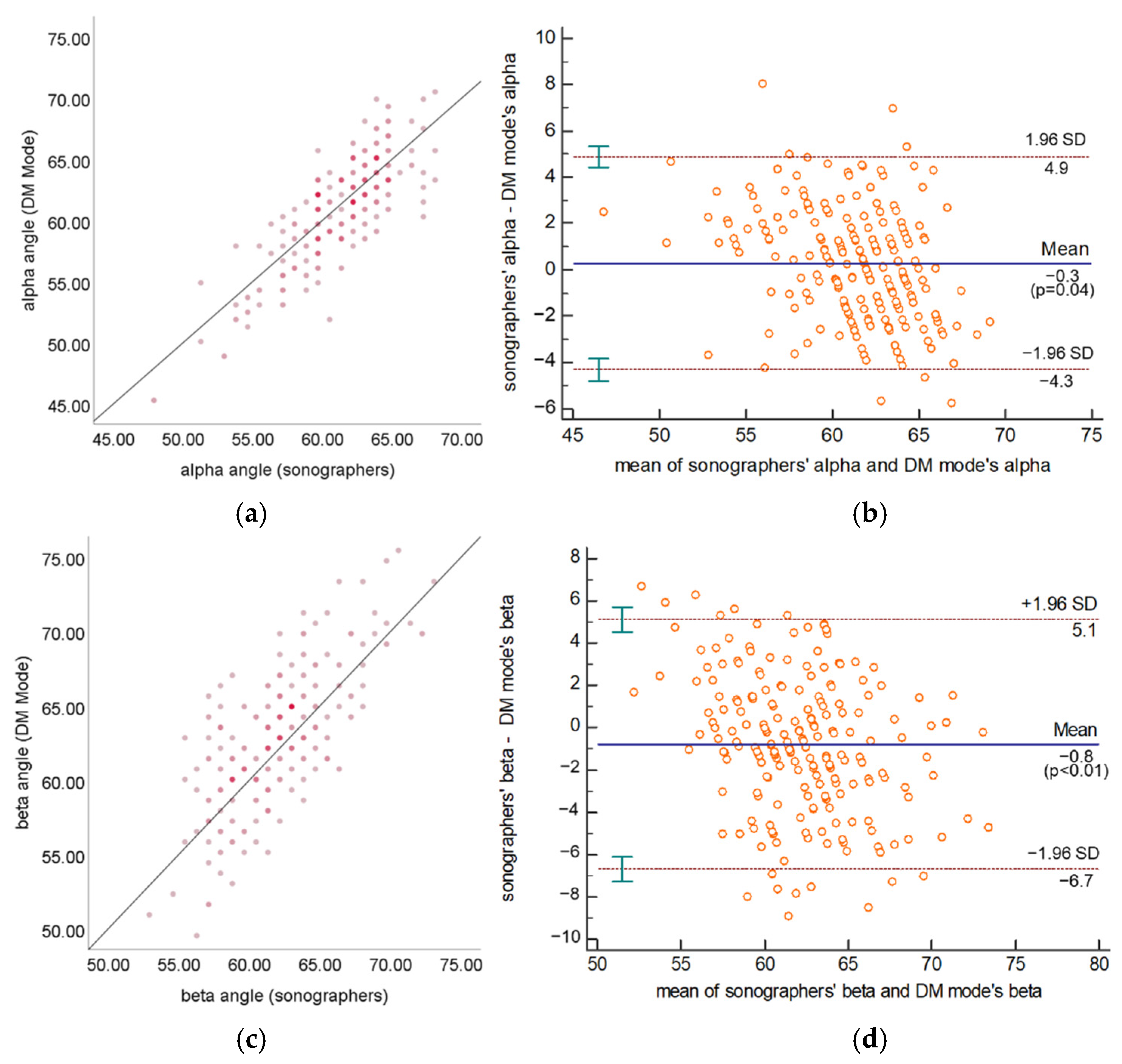
3.2. Statistical Results of Dynamic Measurement Mode
3.3. Running Speed of Dynamic Measurement Mode
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Furnes, O.; Lie, S.A.; Espehaug, B.; Vollset, S.E.; Engesaeter, L.B.; Havelin, L.I. Hip disease and the prognosis of total hip replacements: A review of 53,698 primary total hip replacements reported to the Norwegian arthroplasty register 1987–1999. J. Bone Jt. Surg. 2001, 83, 579. [Google Scholar] [CrossRef]
- Kang, Y.R.; Koo, J. Ultrasonography of the pediatric hip and spine. Ultrasonography 2017, 36, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Pediatrics. Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip. Clinical practice guideline: Early detection of developmental dysplasia of the hip. Pediatrics 2000, 105, 896–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canavese, F.; Castañeda, P.; Hui, J.; Li, L.; Li, Y.; Roposch, A. Developmental dysplasia of the hip: Promoting global exchanges to enable understanding the disease and improve patient care. Orthop. Traumatol. Surg. Res. 2020, 106, 1243–1244. [Google Scholar] [CrossRef] [PubMed]
- Wenger, D.; Düppe, H.; Nilsson, J.Å.; Tiderius, C.J. Incidence of late-diagnosed hip dislocation after universal clinical screening in Sweden. JAMA Netw. Open 2019, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavone, V.; de Cristo, C.; Vescio, A.; Lucenti, L.; Sapienza, M.; Sessa, G.; Pavone, P.; Testa, G. Dynamic and Static Splinting for Treatment of Developmental Dysplasia of the Hip: A Systematic Review. Children 2021, 8, 104. [Google Scholar] [CrossRef]
- Cashman, J.P.; Round, J.; Taylor, G.; Clarke, N.M.P. The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness: A prospective, longitudinal follow-up. J. Bone Jt. Surg. 2002, 84, 418–425. [Google Scholar] [CrossRef]
- Gulati, V.; Eseonu, K.; Sayani, J.; Ismail, N.; Uzoigwe, C.; Choudhury, M.Z.; Gulati, P.; Aqil, A.; Tibrewal, S. Developmental dysplasia of the hip in the newborn: A systematic review. World J. Orthop. 2013, 4, 32. [Google Scholar] [CrossRef]
- Graf, R. Hip sonography: Background; technique and common mistakes; results; debate and politics; challenges. Hip Int. 2017, 27, 215–219. [Google Scholar] [CrossRef]
- Barrera, C.A.; Cohen, S.A.; Sankar, W.N.; Ho-Fung, V.M.; Sze, R.W.; Nguyen, J.C. Imaging of developmental dysplasia of the hip: Ultrasound, radiography and magnetic resonance imaging. Pediatr. Radiol. 2019, 49, 1652–1668. [Google Scholar] [CrossRef]
- Graf, R. Fundamentals of sonographic diagnosis of infant hip dysplasia. J. Pediatr. Orthop. 1984, 4, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Graf, R. Hip Sonography: Diagnosis and Management of Infant Hip Dysplasia; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Tschauner, C.; Matthissen, H. Hip Sonography with Graf-method in Newborns: Checklists help to avoid mistakes. OUB 2012, 1, 7–8. [Google Scholar]
- Jaremko, J.L.; Mabee, M.; Swami, V.G.; Jamieson, L.; Chow, K.; Thompson, R.B. Potential for change in US diagnosis of hip dysplasia solely caused by changes in probe orientation: Patterns of alpha-angle variation revealed by using three-dimensional US. Radiology 2014, 273, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Quader, N.; Hodgson, A.J.; Mulpuri, K.; Schaeffer, E.; Abugharbieh, R. Automatic evaluation of scan adequacy and dysplasia metrics in 2-D ultrasound images of the neonatal hip. Ultrasound Med. Biol. 2017, 43, 1252–1262. [Google Scholar] [CrossRef] [PubMed]
- Orak, M.M.; Onay, T.; Çağırmaz, T.; Elibol, C.; Elibol, F.D.; Centel, T. The reliability of ultrasonography in developmental dysplasia of the hip: How reliable is it in different hands? Indian J. Orthop. 2015, 49, 610. [Google Scholar] [CrossRef]
- Quader, N.; Hodgson, A.J.; Mulpuri, K.; Cooper, A.; Garbi, R. 3-d ultrasound imaging reliability of measuring dysplasia metrics in infants. Ultrasound Med. Biol. 2021, 47, 139–153. [Google Scholar] [CrossRef]
- Hareendranathan, A.R.; Chahal, B.; Ghasseminia, S.; Zonoobi, D.; Jaremko, J.L. Impact of scan quality on AI assessment of hip dysplasia ultrasound. J. Ultrasound 2022, 25, 145–153. [Google Scholar] [CrossRef]
- Paserin, O.; Mulpuri, K.; Cooper, A.; Hodgson, A.J.; Abugharbieh, R. Automatic near real-time evaluation of 3D ultrasound scan adequacy for developmental dysplasia of the hip. In Computer Assisted and Robotic Endoscopy and Clinical Image-Based Procedures; Springer: Cham, Switzerland, 2017; pp. 124–132. [Google Scholar]
- Paserin, O.; Mulpuri, K.; Cooper, A.; Abugharbieh, R.; Hodgson, A.J. Improving 3D ultrasound scan adequacy classification using a three-slice convolutional neural network architecture. CAOS 2018, 2, 152–156. [Google Scholar]
- Paserin, O.; Mulpuri, K.; Cooper, A.; Hodgson, A.J.; Garbi, R. Real time RNN based 3D ultrasound scan adequacy for developmental dysplasia of the hip. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2018; pp. 365–373. [Google Scholar]
- El-Hariri, H.; Hodgson, A.J.; Mulpuri, K.; Garbi, R. Automatically Delineating Key Anatomy in 3-D Ultrasound Volumes for Hip Dysplasia Screening. Ultrasound Med. Biol. 2021, 47, 2713–2722. [Google Scholar] [CrossRef]
- Liu, R.; Liu, M.; Sheng, B.; Li, H.; Song, H.; Zhang, P.; Jiang, L.; Shen, D. NHBS-Net: A Feature Fusion Attention Network for Ultrasound Neonatal Hip Bone Segmentation. IEEE Trans. Med. Imaging 2021, 40, 3446–3458. [Google Scholar] [CrossRef]
- Sezer, H.B.; Sezer, A. Automatic segmentation and classification of neonatal hips according to Graf’s sonographic method: A computer-aided diagnosis system. Appl. Soft Comput. 2019, 82, 105–516. [Google Scholar] [CrossRef]
- Golan, D.; Donner, Y.; Mansi, C.; Jaremko, J.; Ramachandran, M. Fully automating Graf’s method for DDH diagnosis using deep convolutional neural networks. In Deep Learning and Data Labeling for Medical Applications; Springer: Cham, Switzerland, 2016; pp. 130–141. [Google Scholar]
- Hareendranathan, A.R.; Zonoobi, D.; Mabee, M.; Cobzas, D.; Punithakumar, K.; Noga, M.; Jaremko, J.L. Toward automatic diagnosis of hip dysplasia from 2D ultrasound. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 982–985. [Google Scholar]
- El-Hariri, H.; Mulpuri, K.; Hodgson, A.; Garbi, R. Comparative evaluation of hand-engineered and deep-learned features for neonatal hip bone segmentation in ultrasound. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2019; pp. 12–20. [Google Scholar]
- Hu, X.; Wang, L.; Yang, X.; Zhou, X.; Xue, W.; Cao, Y.; Liu, S.; Huang, Y.; Guo, S.; Shang, N.; et al. Joint Landmark and Structure Learning for Automatic Evaluation of Developmental Dysplasia of the Hip. IEEE J. Biomed. Health Inform. 2021, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Ye, H.U.; Lee, K.J.; Jang, W.Y.; Lee, J.H.; Hwang, S.M.; Heo, Y.R. Accuracy of New Deep Learning Model-Based Segmentation and Key-Point Multi-Detection Method for Ultrasonographic Developmental Dysplasia of the Hip (DDH) Screening. Diagnostics 2021, 11, 1174. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Sezer, H.B. Deep convolutional neural network-based automatic classification of neonatal hip ultrasound images: A novel data augmentation approach with speckle noise reduction. Ultrasound Med. Biol. 2020, 46, 735–749. [Google Scholar] [CrossRef]
- Gong, B.; Shi, J.; Han, X.; Zhang, H.; Huang, Y.; Hu, L.; Wang, J.; Du, J.; Shi, J. Diagnosis of Infantile Hip Dysplasia with B-mode Ultrasound via Two-stage Meta-learning Based Deep Exclusivity Regularized Machine. IEEE J. Biomed. Health Inform. 2021, 26, 334–344. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Hu, M.-K. Visual pattern recognition by moment invariants. IRE Trans. Inf. Theory 1962, 8, 179–187. [Google Scholar]
- Kapur, J.N.; Sahoo, P.K.; Wong, A.K. A new method for gray-level picture thresholding using the entropy of the histogram. Comput. Vis. Graph. Image Process. 1985, 29, 273–285. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Li, F.-F. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 22–24 June 2009. [Google Scholar] [CrossRef] [Green Version]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Roovers, E.A.; Boere-Boonekamp, M.M.; Geertsma, T.S.A.; Zielhuis, G.A.; Kerkhoff, A.H.M. Ultrasonographic screening for developmental dysplasia of the hip in infants: Reproducibility of assessments made by radiographers. J. Bone Jt. Surg. 2003, 85, 726–730. [Google Scholar] [CrossRef] [Green Version]
- Simon, E.A.; Saur, F.; Buerge, M.; Glaab, R.; Roos, M.; Kohler, G. Inter-observer agreement of ultrasonographic measurement of alpha and beta angles and the final type classification based on the Graf method. Swiss Med. Wkly. 2004, 134, 671–677. [Google Scholar] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aim | Type of CAD | Author | Year | Algorithm | Applicable Data |
|---|---|---|---|---|---|
| Standard Plane Evaluation | Conventional CAD | Quader et al. [17] | 2021 | random forest classifier | 3D volume |
| Hareendranathan et al. [18] | 2021 | manual method | 2D standard plane | ||
| Deep Learning-based CAD | Paserin et al. [19,20] | 2017 | CNN | 3D volume | |
| Paserin et al. [21] | 2018 | LSTM | 3D volume | ||
| El-Hariri et al. [22] | 2021 | 3D U-Net | 3D volume | ||
| Liu et al. [23] | 2021 | NHBS-Net | 2D standard plane | ||
| Angle Measurement | Conventional CAD | Quader et al. [15] | 2017 | morphological and geometric features | 2D standard plane |
| Quader et al. [17] | 2021 | 3D volume | |||
| Sezer et al. [24] | 2019 | level set | 2D standard plane | ||
| Deep Learning-based CAD | Golan et al. [25] | 2016 | FCN | 2D standard plane | |
| Hareendranathan et al. [26] | 2016 | CNN | 2D standard plane | ||
| El-Hariri et al. [27] | 2019 | 2D U-Net | 2D standard plane | ||
| Hu et al. [28] | 2021 | multi-head Mask R-CNN | 2D standard plane | ||
| Lee et al. [29] | 2021 | Mask R-CNN + FCN | 2D standard plane | ||
| Graf Type Classification | Deep Learning-based CAD | Sezer et al. [30] | 2020 | CNN | 2D standard plane |
| Gong et al. [31] | 2021 | DNN + random forest classifier | 2D standard plane |
| Sonographers | Framework (SM Mode) | Framework-Sonographer | MAE | ICC (95% CI) | Agreement | |
|---|---|---|---|---|---|---|
| α | 60.94 ± 3.54 | 61.88 ± 4.08 | 1.09 ± 1.79 | 1.71 | 0.85 (0.84~0.87) | Good (>0.7) |
| β | 61.57 ± 3.82 | 62.20 ± 4.26 | 0.44 ± 2.97 | 2.40 | 0.73 (0.70~0.76) | Good (>0.7) |
| Angle Measurement | Difference | MAE | ICC (95% CI) | Agreement | ||
|---|---|---|---|---|---|---|
| sonographers | α | 61.35 ± 3.26 | – | – | – | – |
| β | 61.52 ± 3.51 | – | – | – | – | |
| DM w/o. SPSM | α | 61.18 ± 3.41 | –0.37 ± 3.30 | 2.61 | 0.64 (0.59~0.69) | Moderate (0.5~0.7) |
| β | 61.57 ± 3.70 | 1.55 ± 4.29 | 3.64 | 0.44 (0.38~0.51) | Poor (<0.5) | |
| DM w. SPSM | α | 61.04 ± 4.17 | −0.31 ± 2.43 | 1.97 | 0.80 (0.75~0.84) | Good (>0.7) |
| β | 62.58 ± 4.35 | 0.80 ± 3.15 | 2.53 | 0.68 (0.61~0.74) | Moderate (0.5~0.7) | |
| SM mode | α | 62.31 ± 3.74 | 1.03 ± 1.66 | 1.59 | 0.85 (0.81~0.88) | Good (>0.7) |
| β | 61.95 ± 4.15 | 0.17 ± 2.91 | 2.28 | 0.71 (0.65~0.76) | Good (>0.7) | |
| Classification Agreement Rate (%) | Cohen’s Kappa | Agreement | |
|---|---|---|---|
| DM w/o. SPSM | 71.73 | 0.39 | Poor |
| DM w. SPSM | 89.51 | 0.76 | Good |
| SM mode | 95.80 | 0.89 | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.; Zhang, Y.; Wang, B.; Wang, J.; Cui, L.; He, J.; Cong, L. Development of a Fully Automated Graf Standard Plane and Angle Evaluation Method for Infant Hip Ultrasound Scans. Diagnostics 2022, 12, 1423. https://doi.org/10.3390/diagnostics12061423
Chen T, Zhang Y, Wang B, Wang J, Cui L, He J, Cong L. Development of a Fully Automated Graf Standard Plane and Angle Evaluation Method for Infant Hip Ultrasound Scans. Diagnostics. 2022; 12(6):1423. https://doi.org/10.3390/diagnostics12061423
Chicago/Turabian StyleChen, Tao, Yuxiao Zhang, Bo Wang, Jian Wang, Ligang Cui, Jingnan He, and Longfei Cong. 2022. "Development of a Fully Automated Graf Standard Plane and Angle Evaluation Method for Infant Hip Ultrasound Scans" Diagnostics 12, no. 6: 1423. https://doi.org/10.3390/diagnostics12061423