
Nomogram and Carotid Risk Score for Predicting Moderate or High Carotid Atherosclerosis among Asymptomatic Elderly Recycling Volunteers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Instruments and Measurements
2.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Measurement Results
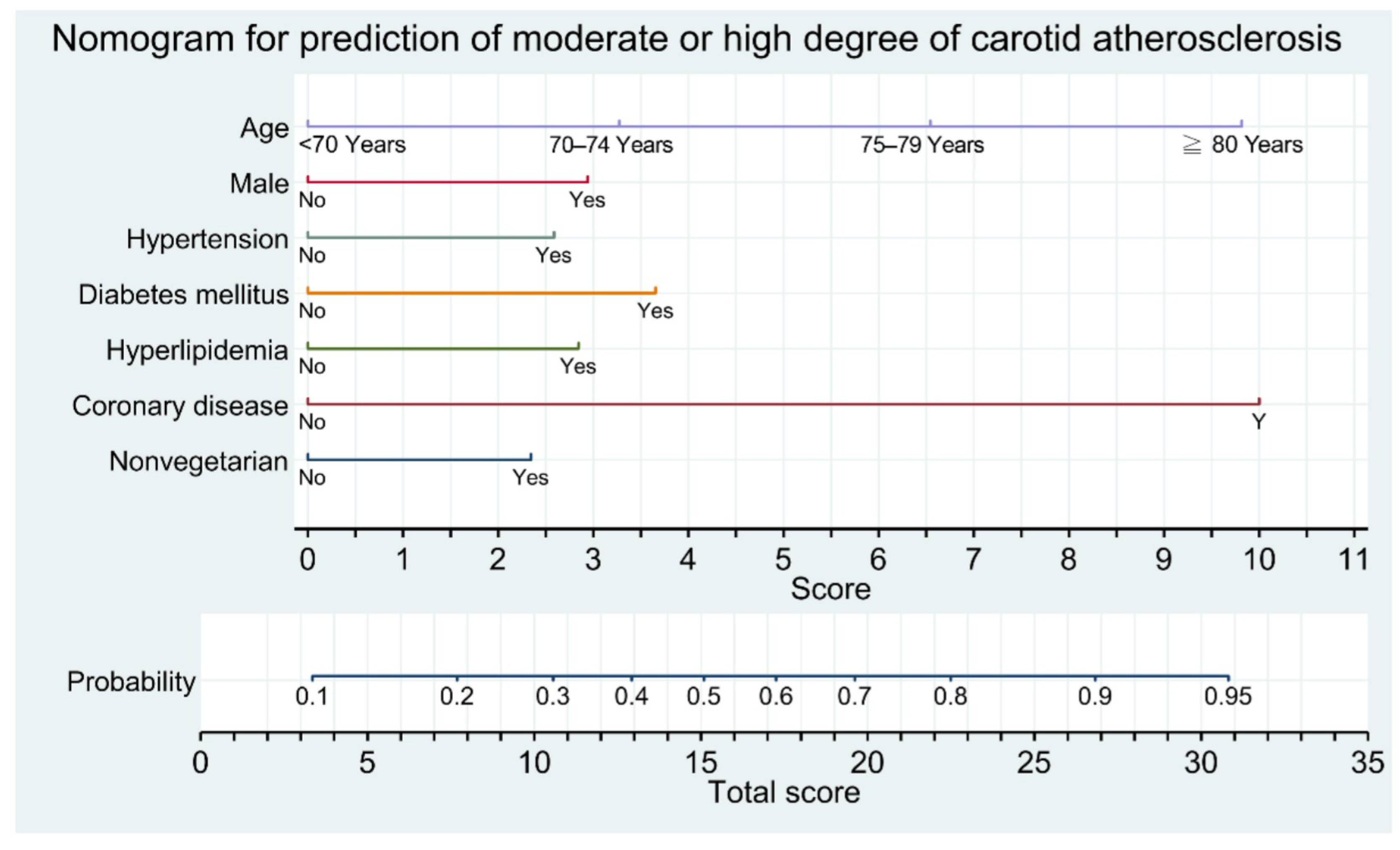
3.3. Development of Nomogram and Flowchart Table
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Boehme, A.K.; Esenwa, C.; Elkind, M.S.V. Stroke risk factors, genetics, and prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Simons, L.A.; McCallum, J.; Friedlander, Y.; Simons, J. Risk factors for ischemic stroke: Dubbo Study of the elderly. Stroke 1998, 29, 1341–1346. [Google Scholar] [CrossRef] [Green Version]
- Baber, U.; Mehran, R.; Sartori, S.; Schoos, M.; Sillesen, H.; Muntendam, P.; Garcia, M.J.; Gregson, J.; Pocock, S.; Falk, E.; et al. Prevalence, impact, and predictive value of detecting subclinical coronary and carotid atherosclerosis in asymptomatic adults: The BioImage study. J. Am. Coll. Cardiol. 2015, 65, 1065–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.; Kim, H.K.; Kwon, S.U.; Lee, S.W.; Kim, M.J.; Park, J.W.; Noh, M.; Han, Y.; Kwon, T.W.; Cho, Y.P. Risk of major adverse cardiovascular events in subjects with asymptomatic mild carotid artery stenosis. Sci. Rep. 2018, 8, 4700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, P.; Fang, Z.; Wang, H.; Cai, Y.; Rahimi, K.; Zhu, Y.; Fowkes, F.G.; Fowkes, F.J.; Rudan, I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: A systematic review, meta-analysis, and modelling study. Lancet Glob. Health 2020, 8, e721–e729. [Google Scholar] [CrossRef]
- Sillesen, H.; Falk, E. Why not screen for subclinical atherosclerosis? Lancet 2011, 378, 645–646. [Google Scholar] [CrossRef]
- Sturlaugsdottir, R.; Aspelund, T.; Bjornsdottir, G.; Sigurdsson, S.; Thorsson, B.; Eiriksdottir, G.; Gudnason, V. Prevalence and determinants of carotid plaque in the cross-sectional REFINEReykjavik study. BMJ Open 2016, 6, e012457. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.-C.; Chen, P.-Y.; Su, Y.-C.; Hsiao, C.-L.; Yang, F.-Y.; Hsu, P.-J.; Lin, S.-K. Vascular, cognitive, and psychomental survey on elderly recycling volunteers in Northern Taiwan. Front. Neurol. 2019, 9, 1176. [Google Scholar] [CrossRef] [Green Version]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Midlife cardiovascular health and 20-year cognitive decline: Atherosclerosis Risk in Communities Study results. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.W.; Lin, C.T.; Lin, Y.L.; Lin, T.K.; Lin, C.L. Taiwanese female vegetarians have lower lipoprotein-associated phospholipase A2 compared with omnivores. Yonsei Med. J. 2011, 52, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.-Y.; Zhang, H.-J.; Sun, S.-Y.; Wang, L.-Y.; Yan, B.; Liu, C.-Q.; Zhang, W.; Li, X.-J. Relationship of carotid intima-media thickness and duration of vegetarian diet in Chinese male vegetarians. Nutr. Metab. 2011, 8, 63. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the society for vascular medicine. J. Am. Soc. Echocardiogr. 2008, 21, 376. [Google Scholar] [CrossRef]
- Touboul, P.-J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez, R.H.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011): An update on behalf of the advisory board of the 3rd and 4th Watching the Risk Symposium 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Handa, N.; Matsumoto, M.; Maeda, H.; Hougaku, H.; Kamada, T. Ischemic stroke events and carotid atherosclerosis: Results of the Osaka Follow-up Study for Ultrasonographic Assessment of Carotid Atherosclerosis (the OSACA Study). Stroke 1995, 26, 1781–1786. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.W.; Kim, Y.K.; Kim, K.H.; Chiara, A.; Lee, M.S.; Bae, J.H. Predictors for high-risk carotid plaque in asymptomatic Korean population. Cardiovasc. Ther. 2020, 2020, 6617506. [Google Scholar] [CrossRef]
- Demšar, J.; Curk, T.; Erjavec, A.; Gorup, Č.; Hočevar, T.; Milutinovič, M.; Možina, M.; Polajnar, M.; Toplak, M.; Starič, A.; et al. Orange: Data mining toolbox in Python. J. Mach. Learn. Res. 2013, 14, 2349–2353. [Google Scholar]
- Sillesen, H.; Muntendam, P.; Adourian, A.; Entrekin, R.; Garcia, M.; Falk, E.; Fuster, V. Carotid plaque burden as a measure of subclinical atherosclerosis: Comparison with other tests for subclinical arterial disease in the high risk plaque BioImage study. JACC Cardiovasc. Imag. 2012, 5, 681–689. [Google Scholar] [CrossRef] [Green Version]
- Sillesen, H.; Sartori, S.; Sandholt, B.; Baber, U.; Mehran, R.; Fuster, V. Carotid plaque thickness and carotid plaque burden predict future cardiovascular events in asymptomatic adult Americans. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Handa, N.; Matsumoto, M.; Maeda, H.; Hougaku, H.; Ogawa, S.; Fukunaga, R.; Yoneda, S.; Kimura, K.; Kamada, T. Ultrasonic evaluation of early carotid atherosclerosis. Stroke 1990, 21, 1567–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Meer, I.M.; Bots, M.L.; Hofman, A.; del Sol, A.I.; van der Kuip, D.A.; Witteman, J.C. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: The Rotterdam Study. Circulation 2004, 109, 1089–1094. [Google Scholar] [CrossRef] [Green Version]
- Rosvall, M.; Janzon, L.; Berglund, G.; Engström, G.; Hedblad, B. Incident coronary events and case fatality in relation to common carotid intima-media thickness. J. Intern. Med. 2005, 257, 430–437. [Google Scholar] [CrossRef]
- Chien, K.-L.; Su, T.-C.; Jeng, J.-S.; Hsu, H.-C.; Chang, W.-T.; Chen, M.-F.; Lee, Y.-T.; Hu, F.B. Carotid artery intima-media thickness, carotid plaque and coronary heart disease and stroke in Chinese. PLoS ONE 2008, 3, e3435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prati, P.; Tosetto, A.; Casaroli, M.; Bignamini, A.; Canciani, L.; Bornstein, N.; Prati, G.; Touboul, P.-J.T. Carotid plaque morphology improves stroke risk prediction: Usefulness of a new ultrasonographic score. Cerebrovasc. Dis. 2011, 31, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xu, X.; Luo, B.; Zhang, Y. The predictive value of carotid ultrasonography with cardiovascular risk factors—A “SPIDER” promoting atherosclerosis. Front. Cardiovasc. Med. 2021, 8, 706490. [Google Scholar] [CrossRef]
- Ikeda, N.; Kogame, N.; Iijima, R.; Nakamura, M.; Sugi, K. Carotid artery intima-media thickness and plaque score can predict the SYNTAX score. Eur. Heart J. 2012, 33, 113–119. [Google Scholar] [CrossRef]
- Sun, Y.; Lin, C.H.; Lu, C.J.; Yip, P.K.; Chen, R.C. Carotid atherosclerosis, intima-media thickness and risk factors: An analysis of 1781 asymptomatic subjects in Taiwan. Atherosclerosis 2002, 164, 89–94. [Google Scholar] [CrossRef]
- Su, T.C.; Jeng, J.S.; Chien, K.L.; Sung, F.C.; Hsu, H.C.; Lee, Y.T. Hypertension status is the major determinant of carotid atherosclerosis: A community-based study in Taiwan. Stroke 2001, 32, 2265–2271. [Google Scholar] [CrossRef]
- Yan, Z.; Liang, Y.; Shi, J.; Cai, C.; Jiang, H.; Song, A.; Qiu, C. Carotid stenosis and cognitive impairment amongst older Chinese adults living in a rural area: A population-based study. Eur. J. Neurol. 2016, 23, 201–204. [Google Scholar] [CrossRef]
- Spence, J.D.; Eliasziw, M.; DiCicco, M.; Hackam, D.G.; Galil, R.; Lohmann, T. Carotid plaque area: A tool for targeting and evaluating vascular preventive therapy. Stroke 2002, 33, 2916–2922. [Google Scholar] [CrossRef]
- Spence, J.D. Measurement of carotid plaque burden. JAMA Neurol. 2015, 72, 383–384. [Google Scholar] [CrossRef]
- Spence, J.D.; Coates, V.; Li, H.; Tamayo, A.; Munoz, C.; Hackam, D.G.; DiCicco, M.; DesRoches, J.; Bogiatzi, C.; Klein, J.; et al. Effects of intensive medical therapy on microemboli and cardiovascular risk in asymptomatic carotid stenosis. Arch. Neurol. 2010, 67, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Paraskevas, K.I.; Veith, F.J.; Eckstein, H.H.; Ricco, J.B.; Mikhailidis, D.P. Cholesterol, carotid artery disease and stroke: What the vascular specialist needs to know. Ann. Transl. Med. 2020, 8, 1265. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, G.; Toth, P.P.; Bungau, S.; Behl, T.; Ilie, M.; Stoian, A.P.; Bratu, O.G.; Bacalbasa, N.; Rus, M.; Diaconu, C.C. Cardiovascular risk and statin therapy considerations in women. Diagnostics 2020, 10, 483. [Google Scholar] [CrossRef] [PubMed]
- Näslund, U.; Ng, N.; Lundgren, A.; Fhärm, E.; Grönlund, C.; Johansson, H.; Lindahl, B.; Lindahl, B.; Lindvall, K.; Nilsson, S.K.; et al. Visualization of asymptomatic atherosclerotic disease for optimum cardiovascular prevention (VIPVIZA): A pragmatic, open-label, randomised controlled trial. Lancet. 2019, 393, 133–142. [Google Scholar] [CrossRef]
- Kiriyama, H.; Kaneko, H.; Itoh, H.; Yoshida, Y.; Nakanishi, K.; Mizuno, Y.; Daimon, M.; Morita, H.; Yamamichi, N.; Komuro, I. Effect of cigarette smoking on carotid artery atherosclerosis: A community-based cohort study. Heart Vessels 2020, 35, 22–29. [Google Scholar] [CrossRef]
- Hisamatsu, T.; Miura, K.; Arima, H.; Kadota, A.; Kadowaki, S.; Torii, S.; Suzuki, S.; Miyagawa, N.; Sato, A.; Yamazoe, M.; et al. Smoking, smoking cessation, and measures of subclinical atherosclerosis in multiple vascular beds in Japanese men. J. Am. Heart Assoc. 2016, 5, e003738. [Google Scholar] [CrossRef]
- Peace, A.; Van Mil, A.; Jones, H.; Thijssen, D.H.J. Similarities and differences between carotid artery and coronary artery function. Curr. Cardiol. Rev. 2018, 14, 254–263. [Google Scholar] [CrossRef]
- Tada, H.; Kawashiri, M.-A.; Okada, H.; Nakahashi, T.; Sakata, K.; Nohara, A.; Inazu, A.; Mabuchi, H.; Yamagishi, M.; Hayashi, K. Assessments of carotid artery plaque burden in patients with familial hypercholesterolemia. Am. J. Cardiol. 2017, 120, 1955–1960. [Google Scholar] [CrossRef]
- Nakahashi, T.; Tada, H.; Sakata, K.; Nomura, A.; Ohira, M.; Mori, M.; Takamura, M.; Hayashi, K.; Yamagishi, M.; Kawashiri, M.-A. Additive prognostic value of carotid plaque score to enhance the age, creatinine, and ejection fraction score in patients with acute coronary syndrome. J. Atheroscler. Thromb. 2018, 25, 709–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mostaza, J.M.; Lahoz, C.; Salinero-Fort, M.A.; de Burgos-Lunar, C.; Laguna, F.; Estirado, E.; García-Iglesias, F.; González-Alegre, T.; Cornejo-Del-Río, V.; Sabín, C.; et al. Carotid atherosclerosis severity in relation to glycemic status: A cross-sectional population study. Atherosclerosis 2015, 242, 377–382. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 7, 255–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettersen, B.J.; Anousheh, R.; Fan, J.; Jaceldo-Siegl, K.; Fraser, G.E. Vegetarian diets and blood pressure among white subjects: Results from the Adventist Health Study-2 (AHS-2). Public Health Nutr. 2012, 15, 1909–1916. [Google Scholar] [CrossRef] [Green Version]
- Tonstad, S.; Stewart, K.; Oda, K.; Batech, M.; Herring, R.P.; Fraser, G.E. Vegetarian diets and incidence of diabetes in the Adventist Health Study-2. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 292–299. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian diets and blood pressure: A meta-analysis. JAMA Intern. Med. 2004, 174, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Saxhaug, L.M.; Graven, T.; Olsen, Ø.; Kleinau, J.O.; Skjetne, K.; Ellekjær, H.; Dalen, H. Reliability and agreement of point-ofcare carotid artery examinations by experts using hand-held ultrasound devices in patients with ischaemic stroke or transitory ischaemic attack. Open Heart 2022, 9, e001917. [Google Scholar] [CrossRef]
- Ohara, T.; Kokubo, Y.; Toyoda, K.; Watanabe, M.; Koga, M.; Nakamura, S.; Nagatsuka, K.; Minematsu, K.; Nakagawa, M.; Miyamoto, Y. Impact of chronic kidney disease on carotid atherosclerosis according to blood pressure category: The Suita Study. Stroke 2013, 44, 3537–3539. [Google Scholar] [CrossRef] [Green Version]
- Moisi, M.I.; Bungau, S.G.; Vesa, C.M.; Diaconu, C.C.; Behl, T.; Stoicescu, M.; Toma, M.M.; Bustea, C.; Sava, C.; Popescu, M.I. Framing cause-effect relationship of acute coronary syndrome in patients with chronic kidney disease. Diagnostics 2021, 11, 1518. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total n = 956 (%) | Women n = 778 (%) | Men n = 178 (%) | p Value |
|---|---|---|---|---|
| Hypertension | 379 (40) | 314 (40) | 65 (37) | 0.352 |
| Diabetes | 122 (13) | 100 (13) | 22 (12) | 0.999 |
| Heart disease | 169 (18) | 140 (18) | 29 (16) | 0.663 |
| Coronary artery disease | 27 (3) | 18 (2) | 9 (5) | 0.074 |
| Hyperlipidemia | 186 (19) | 162 (21) | 24 (13) | 0.027 |
| Smoking | 72 (8) | 13 (2) | 59 (33) | <0.001 |
| Alcohol consumption | 77 (8) | 43 (6) | 34 (19) | <0.001 |
| Vegetarian diets | 495 (52) | 406 (52) | 89 (50) | 0.619 |
| Characteristics | Total (n = 956) | Sex | Vegetarian Diet | ||||
|---|---|---|---|---|---|---|---|
| Women (n = 778) | Men (n = 178) | p Value | Yes (n = 495) | No (n = 461) | p Value | ||
| Age (years) | 71 (65–76) | 71 (65–76) | 70 (64–75) | 0.189 | 69 (64–75) | 72 (66–76) | <0.001 |
| Body mass index (kg/m2) | 24.0 (21.9–26.4) | 24.0 (21.8–26.4) | 24.1 (22.0–26.1) | 0.542 | 23.6 (21.5–26.0) | 24.5 (22.4–26.8) | <0.001 |
| Mean systolic blood pressure (mmHg) | 147 (133–160) | 146 (132–160) | 149 (137–161) | 0.218 | 145 (132–159) | 149 (135–162) | 0.007 |
| Right arm | 137 (125–149) | 137 (124–149) | 137 (127–148) | 0.734 | 134 (123–145) | 139 (127–150) | <0.001 |
| Left arm * | 156 (141–173) | 155 (139–173) | 159 (145–173) | 0.121 | 154 (139–172) | 158 (142–174) | 0.073 |
| Glucose (mg/dL) | 98 (92–105) | 98 (91–105) | 99 (95–106) | 0.025 | 97 (91–105) | 99 (92–106) | 0.185 |
| Cholesterol (mg/dL) | 187 (163–214) | 190 (166–216) | 172 (153–191) | <0.001 | 183 (161–207) | 190 (167–217) | 0.004 |
| Mean ankle-brachial index | 1.13 (1.08–1.19) | 1.13 (1.08–1.18) | 1.16 (1.09–1.21) | 0.001 | 1.14 (1.09–1.19) | 1.12 (1.07–1.19) | 0.014 |
| Right side | 1.13 1.07–1.19) | 1.13 (1.07–1.19) | 1.05 (1.19–1.21) | 0.005 | 1.14 (1.08–1.19) | 1.13 (1.06–1.19) | 0.031 |
| Left side | 1.13 (1.07–1.19) | 1.13 (1.07–1.19) | 1.16 (1.09–1.22) | <0.001 | 1.13 (1.08–1.19) | 1.12 (1.06–1.19) | 0.058 |
| Mean carotid intima-media thickness (mm) | 0.66 (0.57–0.75) | 0.65 (0.57–0.74) | 0.71 (0.61–0.79) | <0.001 | 0.64 (0.56–0.74) | 0.68 (0.59–0.76) | <0.001 |
| Right side (mm) | 0.66 (0.57–0.77) | 0.65 (0.56–0.76) | 0.70 (0.60–0.82) | <0.001 | 0.64 (0.55–0.76) | 0.68 (0.58–0.78) | <0.001 |
| Left side (mm) | 0.65 (0.56–0.75) | 0.63 (0.65–0.74) | 0.69 (0.59–0.79) | 0.004 | 0.63 (0.55–0.75) | 0.65 (0.57–0.76) | 0.016 |
| Carotid plaque score | 1.9 (0.0–4.7) | 1.8 (0.0–4.5) | 2.4 (1.2–6.1) | 0.020 | 1.5 (0.0–4.0) | 2.5 (0.0–5.4) | <0.001 |
| Right side | 1.3 (0.0–2.3) | 1.2 (0.0–2.1) | 1.4 (0.0–3.2) | 0.008 | 0.0 (0.0–2.0) | 1.3 (0.0–2.8) | 0.007 |
| Left side | 1.3 (0.0–2.3) | 1.3 (0.0–2.2) | 1.4 (0.0–2.8) | 0.218 | 0.0 (0.0–1.9) | 1.5 (0.0–2.8) | <0.001 |
| Degree of total carotid plaque score | 0.030 | <0.001 | |||||
| No plaque | 310 (33%) | 266 (34%) | 44 (25%) | 177 (36%) | 133 (29%) | ||
| Mild (total carotid plaque score 1.5–5.0) | 433 (45%) | 350 (45%) | 83 (47%) | 233 (47%) | 200 (44%) | ||
| Moderate (total carotid plaque score 5.1–10) | 152 (16%) | 118 (15%) | 34 (19%) | 58 (12%) | 94 (20%) | ||
| Severe (total carotid plaque score > 10) | 61 (6%) | 44 (6%) | 17 (9%) | 27 (5%) | 34 (7%) | ||
| Mean CIMT | Carotid Plaque Score | |||||
|---|---|---|---|---|---|---|
| Dependent Variables | Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
| Age | 0.240 | 0.173–0.301 | <0.001 | 0.346 | 0.288–0.400 | <0.001 |
| Body mass index | −0.003 | −0.069–0.062 | 0.918 | 0.014 | −0.049–0.077 | 0.669 |
| Systolic blood pressure | 0.178 | 0.114–0.241 | <0.001 | 0.177 | 0.114–0.237 | <0.001 |
| Fasting glucose | 0.079 | 0.004–0.153 | 0.039 | 0.092 | 0.019–0.163 | 0.013 |
| Fasting cholesterol | 0.037 | −0.039–0.113 | 0.338 | 0.043 | −0.030–0.116 | 0.249 |
| Mean ankle-brachial index | 0.009 | −0.057–0.074 | 0.785 | −0.066 | −0.129–−0.002 | 0.042 |
| Mean CIMT | - | - | - | 0.301 | 0.240–0.359 | <0.001 |
| Carotid plaque score | 0.301 | 0.240–0.359 | <0.001 | - | - | - |
| Characteristics | MHCA (CPS > 5) * | MHCA (CPS > 5) ** | |||
|---|---|---|---|---|---|
| Yes/n = 213 (%) | No/n = 743 (%) | p Value | OR (95% CI) | p Value | |
| Age | <0.001 | ||||
| 60–69 years (n = 434) | 50 (12) | 384 (88) | - | - | |
| 70–74 years (n = 218) | 46 (21) | 172 (79) | 1.802 (1.134–2.863) | 0.013 | |
| 75–9 years (n = 197) | 72 (37) | 125 (63) | 3.828 (2.463–5.951) | <0.001 | |
| ≥80 years (n = 107) | 45 (42) | 62 (58) | 5.770 (3.447–9.661) | <0.001 | |
| Male sex (n = 178) | 51 (29) | 127 (17) | 0.028 | 1.718 (1.139–2.590) | 0.010 |
| Hypertension (n = 379) | 119 (56) | 260 (35) | <0.001 | 1.627 (1.153–2.297) | 0.006 |
| Diabetes mellitus (n = 122) | 46 (22) | 75 (10) | <0.001 | 2.080 (1.260–3.080) | 0.003 |
| Hyperlipidemia (n = 186) | 59 (28) | 127 (17) | <0.001 | 1.686 (1.128–2.521) | 0.011 |
| Heart disease (n = 169) | 55 (26) | 114 (15) | <0.001 | 0.986 (0.636–1.528) | 0.949 |
| Coronary artery disease (n = 27) | 19 (9) | 8 (1) | <0.001 | 6.525 (2.560–16.633) | <0.001 |
| Smoking (n = 72) | 21 (10) | 51 (7) | 0.143 | - | - |
| Alcohol consumption (n = 77) | 16 (8) | 61 (8) | 0.886 | - | - |
| Nonvegetarian diets (n = 461) | 128 (60) | 333 (45) | <0.001 | 1.544 (1.098–2.172) | 0.013 |
| ≥80 Years(9.8) | CAD(10): 19.8 | |||
| Male(3): 12.8 | Non-V(2.4): 15.2 | |||
| V(0): 12.8 | 1 RF(≥2.6): ≥15.4 | |||
| Female(0): 9.8 | Non-V(2.4): 12.2 | 1 RF(2.6~3.7): 14.8~15.9 | ||
| V(0): 9.8 | 2 RF(≥5.4): ≥15.2 | |||
| 1 RF(2.6~3.7): 12.4~13.5 (40%) | ||||
| 75–79 Years(6.5) | CAD(10): 16.5 | |||
| Male(3): 9.5 | Non-V(2.4): 11.9 | DM(3.7): 15.6 | ||
| 2 RF(≥5.4): ≥17.3 | ||||
| 1 RF(2.6~2.8): 14.5~14.7 (47%) | ||||
| V(0): 9.5 | 2 RF(5.4~6.5): 14.9~16.0 | |||
| 1 RF(2.6~3.7): 12.1~13.2 (39%) | ||||
| Female(0): 6.5 | Non-V(2.4): 8.9 | DM(3.7) + 1 RF(≥2.6): ≥15.2 | ||
| 2 RF(5.4): 14.3 (47%) | ||||
| 1 RF(2.6~2.8): 11.5~1.7 (33%) | ||||
| V(0): 6.5 | 3 RF(9.1): 15.6 | |||
| 2 RF(5.4~6.5): 11.9~13 (38%) | ||||
| 1 RF(2.6–3.7): 9.1~10.2 (27%) | ||||
| 70–74 Years(3.3) | CAD(10): 13.3 | Male(3): 16.3 | ||
| Female (0): 13.3 | Non-V(2.4): 15.9 | |||
| V(0): 13.3 | 1 RF(≥2.6): ≥15.9 | |||
| Male(3): 6.3 | Non-V(2.4): 8.7 | DM(3.7) + 1 RF(≥2.6): ≥15 | ||
| 2 RF(5.4): 14.1 (46%) | ||||
| 1 RF(2.6~3.7): 11.3~12.4 (36%) | ||||
| V(0): 6.3 | 3 RF(9.1): 15.4 | |||
| 2 RF(5.4~6.5): 11.7~12.8 (37%) | ||||
| 1 RF(2.6~3.7): 8.9~10 (26%) | ||||
| Female(0): 3.3 | Non-V(2.4): 5.7 | 3 RF(9.1): 14.8 (49%) | ||
| 2 RF(5.4–6.5): 11.1~12.2 (34%) | ||||
| 1 RF(2.6~3.7): 8.3~9.4 (24%) | ||||
| V(0): 3.3 | 3 RF(9.1): 12.4 (37%) | |||
| 2 RF(5.4~6.5): 8.7~9.8 (25%) | ||||
| 1 RF(2.6~3.7): 5.9~7 (19%) | ||||
| <70 Years(0) | CAD(10): 10 | Male(3): 13 | Non-V(2.4): 15.4 | |
| V(0): 13 | 1 RF(≥2.6): ≥15.6 | |||
| Female(0): 10 | Non-V(2.4): 12.4 | 1 RF(≥2.6): ≥15 | ||
| V(0): 10 | 2 RF(5.4~6.3): 15.4~16.3 | |||
| 1 RF(2.6~3.7): 12.6~13.7 (40%) | ||||
| Male(3): 3 | Non-V(2.4): 5.4 | 3 RF(9.1): 14.5 (47%) | ||
| 2 RF(5.4~6.5): 10.8~11.9 (33%) | ||||
| 1 RF(2.6~3.7): 8.0~9.1 (23%) | ||||
| V(0): 3 | 3 RF(9.1): 12.1 (37%) | |||
| 2 RF(5.4–6.5): 8.4~9.5 (24%) | ||||
| 1 RF(2.6~3.7): 5.6~6.7 (17%) | ||||
| Female(0): 0 | Non-V(2.4): 2.4 | 3 RF(9.1): 11.5 (33%) | ||
| 2 RF(5.4~6.6): 7.8~9 (22%) | ||||
| 1 RF(2.6~3.7): 5.0~6.1 (15%) | ||||
| V(0): 0 | 3 RF(9.1): 9.1 (25%) | |||
| 2 RF(5.4~6.5): 5.4~6.5 (16%) | ||||
| 1 RF(2.6~3.7): 2.6~3.7 (<10%) | ||||
| Items | Score |
|---|---|
| Age | |
| <70 years | 0 |
| 70–74 years | 1 |
| 75–79 years | 3 |
| ≥80 years | 5 |
| Male sex | 1 |
| Hypertension | 1 |
| Diabetes mellitus | 2 |
| Hyperlipidemia | 1 |
| Coronary artery disease | 6 |
| Nonvegetarian | 1 |
| Total score | 0–17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-L.; Chen, P.-Y.; Hsu, P.-J.; Lin, S.-K. Nomogram and Carotid Risk Score for Predicting Moderate or High Carotid Atherosclerosis among Asymptomatic Elderly Recycling Volunteers. Diagnostics 2022, 12, 1407. https://doi.org/10.3390/diagnostics12061407
Hsiao C-L, Chen P-Y, Hsu P-J, Lin S-K. Nomogram and Carotid Risk Score for Predicting Moderate or High Carotid Atherosclerosis among Asymptomatic Elderly Recycling Volunteers. Diagnostics. 2022; 12(6):1407. https://doi.org/10.3390/diagnostics12061407
Chicago/Turabian StyleHsiao, Cheng-Lun, Pei-Ya Chen, Po-Jen Hsu, and Shinn-Kuang Lin. 2022. "Nomogram and Carotid Risk Score for Predicting Moderate or High Carotid Atherosclerosis among Asymptomatic Elderly Recycling Volunteers" Diagnostics 12, no. 6: 1407. https://doi.org/10.3390/diagnostics12061407