
Automatic Classification for Sagittal Craniofacial Patterns Based on Different Convolutional Neural Networks


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Labeling and Dataset
2.3. Data Processing
2.4. Data Augmentation
2.5. Convolutional Neural Network Constriction
2.6. Training Details and Strategy
2.7. Model Testing and Evaluation Metrics
2.8. Model Visualization
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Samek, W.; Krois, J. Artificial Intelligence in Dentistry: Chances and Challenges. J. Dent. Res. 2020, 99, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Golla, T.; Dreher, M.; Krois, J. Convolutional neural networks for dental image diagnostics: A scoping review. J. Dent. 2019, 91, 103226. [Google Scholar] [CrossRef] [PubMed]
- Allareddy, V.; Rengasamy Venugopalan, S.; Nalliah, R.P.; Caplin, J.L.; Lee, M.K.; Allareddy, V. Orthodontics in the era of big data analytics. Orthod. Craniofac. Res. 2019, 22 (Suppl. S1), 8–13. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Seo, H.; Hwang, J.; Jeong, T.; Shin, J. Comparison of Deep Learning Models for Cervical Vertebral Maturation Stage Classification on Lateral Cephalometric Radiographs. J. Clin. Med. 2021, 10, 3591. [Google Scholar] [CrossRef]
- Yoon, H.-J.; Kim, D.-R.; Gwon, E.; Kim, N.; Baek, S.-H.; Ahn, H.-W.; Kim, K.-A.; Kim, S.-J. Fully automated identification of cephalometric landmarks for upper airway assessment using cascaded convolutional neural networks. Eur. J. Orthod. 2021, 44, 66–77. [Google Scholar] [CrossRef]
- Monill-González, A.; Rovira-Calatayud, L.; d’Oliveira, N.G.; Ustrell-Torrent, J.M. Artificial intelligence in orthodontics: Where are we now? A scoping review. Orthod. Craniofac. Res. 2021, 24 (Suppl. S2), 6–15. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields, H.W.; Larson, B.; Sarver, D.M. Contemporary Orthodontics-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Freeman, R.S. Adjusting A-N-B angles to reflect the effect of maxillary position. Angle Orthod. 1981, 51, 162–171. [Google Scholar] [CrossRef]
- Jacobson, A. The “Wits” appraisal of jaw disharmony. Am. J. Orthod. 1975, 67, 125–138. [Google Scholar] [CrossRef]
- Kim, Y.H.; Vietas, J.J. Anteroposterior dysplasia indicator: An adjunct to cephalometric differential diagnosis. Am. J. Orthod. 1978, 73, 619–633. [Google Scholar] [CrossRef]
- Baik, C.Y.; Ververidou, M. A new approach of assessing sagittal discrepancies: The Beta angle. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 100–105. [Google Scholar] [CrossRef]
- Yu, H.J.; Cho, S.R.; Kim, M.J.; Kim, W.H.; Kim, J.W.; Choi, J. Automated Skeletal Classification with Lateral Cephalometry Based on Artificial Intelligence. J. Dent. Res. 2020, 99, 249–256. [Google Scholar] [CrossRef]
- So, L.L.; Davis, P.J.; King, N.M. “Wits” appraisal in Southern Chinese children. Angle Orthod. 1990, 60, 43–48. [Google Scholar]
- Cooke, M.S.; Wei, S.H. An improved method for the assessment of the sagittal skeletal pattern and its correlation to previous methods. Eur. J. Orthod. 1988, 10, 122–127. [Google Scholar] [CrossRef]
- Nalepa, J.; Marcinkiewicz, M.; Kawulok, M. Data Augmentation for Brain-Tumor Segmentation: A Review. Front. Comput. Neurosci. 2019, 13, 83. [Google Scholar] [CrossRef] [Green Version]
- Morid, M.A.; Borjali, A.; Del Fiol, G. A scoping review of transfer learning research on medical image analysis using ImageNet. Comput. Biol. Med. 2021, 128, 104115. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Kensert, A.; Harrison, P.J.; Spjuth, O. Transfer Learning with Deep Convolutional Neural Networks for Classifying Cellular Morphological Changes. SLAS Discov. 2019, 24, 466–475. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Mohammad-Rahimi, H.; Nadimi, M.; Rohban, M.H.; Shamsoddin, E.; Lee, V.Y.; Motamedian, S.R. Machine learning and orthodontics, current trends and the future opportunities: A scoping review. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 170–192.e4. [Google Scholar] [CrossRef]
- Moyers, R.E.; Bookstein, F.L.; Guire, K.E. The concept of pattern in craniofacial growth. Am. J. Orthod. 1979, 76, 136–148. [Google Scholar] [CrossRef] [Green Version]
- Hou, D.; Capote, R.; Bayirli, B.; Chan, D.C.N.; Huang, G. The effect of digital diagnostic setups on orthodontic treatment planning. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Sengupta, S.; Lakshminarayanan, V. Explainable Deep Learning Models in Medical Image Analysis. J. Imaging 2020, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Molina-Berlanga, N.; Llopis-Perez, J.; Flores-Mir, C.; Puigdollers, A. Lower incisor dentoalveolar compensation and symphysis dimensions among Class I and III malocclusion patients with different facial vertical skeletal patterns. Angle Orthod. 2013, 83, 948–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleall, J.F.; BeGole, E.A. Diagnosis and treatment of class II division 2 malocclusion. Angle Orthod. 1982, 52, 38–60. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class I | Class II | Class III | Total | |
|---|---|---|---|---|
| Training set | 642 | 525 | 534 | 1701 |
| Validation set | 138 | 113 | 115 | 366 |
| Test set | 138 | 112 | 115 | 365 |
| Total | 918 | 750 | 764 | 2432 |
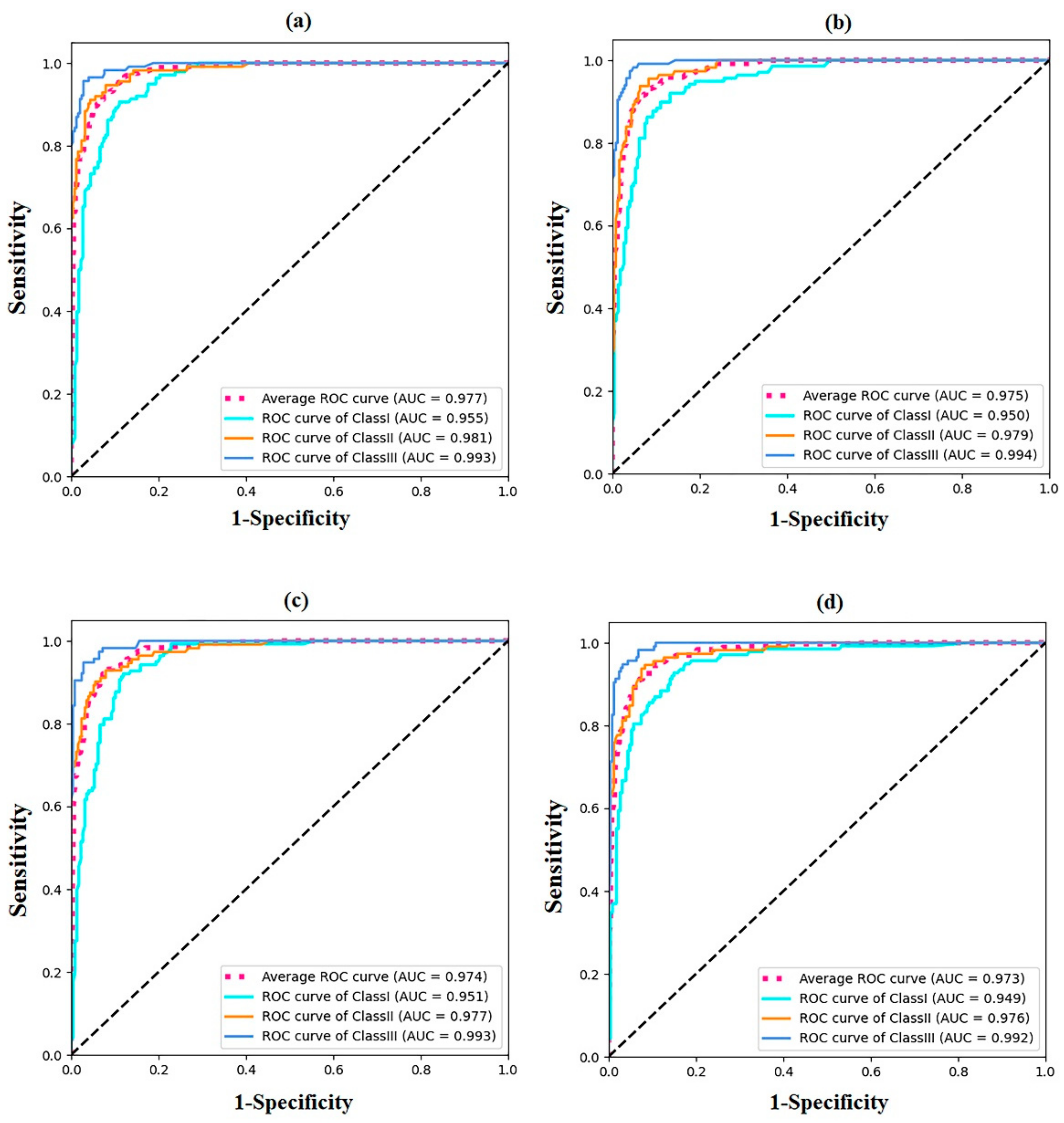
| Model Size | Training Time (min) | Accuracy | Inference Time (s/per Image) | AUC Value | |
|---|---|---|---|---|---|
| DenseNet161 | 102 | 40 | 89.58 | 0.32 | 0.977 |
| ResNet152 | 222 | 38 | 89.04 | 0.32 | 0.974 |
| VGG16 | 512 | 33 | 88.76 | 0.26 | 0.973 |
| GoogLeNet | 21.5 | 27 | 87.94 | 0.083 | 0.972 |
| Precision (95% CI) | Recall (95% CI) | F1 Score (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | I | II | III | I | II | III | |
| DenseNet161 | 0.83(0.77–0.88) | 0.93(0.86–0.96) | 0.95(0.90–0.98) | 0.91(0.85–0.94) | 0.88(0.81–0.93) | 0.90(0.83–0.94) | 0.87(0.81–0.691) | 0.90(0.83–0.94) | 0.92(0.86–0.96) |
| ResNet152 | 0.83(0.75–0.87) | 0.89(0.82–0.94) | 0.97(0.92–0.99) | 0.89(0.83–0.93) | 0.88(0.80–0.92) | 0.90(0.84–0.95) | 0.86(0.79–0.90) | 0.88(0.81–0.93) | 0.94(0.88–0.97) |
| VGG16 | 0.84(0.78–0.89) | 0.88(0.81–0.93) | 0.95(0.90–0.98) | 0.86(0.79–0.91) | 0.90(0.83–0.94) | 0.90(0.84–0.95) | 0.85(0.78–0.90) | 0.89(0.82–0.93) | 0.93(0.87–0.96) |
| GoogLeNet | 0.87(0.80–0.92) | 0.84(0.77–0.90) | 0.93(0.87–0.96) | 0.80(0.73–0.86) | 0.91(0.84–0.95) | 0.94(0.88–0.97) | 0.83(0.76–0.89) | 0.88(0.80–0.92) | 0.94(0.87–0.96) |
| DenseNet161 | ResNet152 | VGG16 | GoogLeNet | |||||
|---|---|---|---|---|---|---|---|---|
| ANB | Wits | ANB | Wits | ANB | Wits | ANB | Wits | |
| I–II * | 4.38 ± 0.34 | 1.63 ± 0.25 | 4.43 ± 0.31 | 1.45 ± 0.3 | 4.38 ± 0.29 | 1.51 ± 0.17 | 4.51 ± 0.29 | 1.48 ± 0.26 |
| II–I * | 5.61 ± 0.35 | 2.85 ± 0.48 | 5.45 ± 0.33 | 3.23 ± 0.57 | 5.57 ± 0.29 | 2.85 ± 0.61 | 5.63 ± 0.16 | 3.07 ± 0.61 |
| I–III * | 0.66 ± 0.34 | −1.92 ± 0.64 | 0.50 ± 0.20 | −1.83 ± 0.84 | 0.54 ± 0.30 | −1.94 ± 0.32 | 0.44 ± 0.32 | −1.79 ± 0.65 |
| III–I * | −0.38 ± 0.31 | −3.34 ± 0.32 | −0.42 ± 0.29 | −3.75 ± 0.29 | −0.55 ± 0.30 | −3.46 ± 0.22 | −0.33 ± 0.22 | −3.31 ± 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Xu, Y.; Lei, Y.; Wang, Q.; Gao, X. Automatic Classification for Sagittal Craniofacial Patterns Based on Different Convolutional Neural Networks. Diagnostics 2022, 12, 1359. https://doi.org/10.3390/diagnostics12061359
Li H, Xu Y, Lei Y, Wang Q, Gao X. Automatic Classification for Sagittal Craniofacial Patterns Based on Different Convolutional Neural Networks. Diagnostics. 2022; 12(6):1359. https://doi.org/10.3390/diagnostics12061359
Chicago/Turabian StyleLi, Haizhen, Ying Xu, Yi Lei, Qing Wang, and Xuemei Gao. 2022. "Automatic Classification for Sagittal Craniofacial Patterns Based on Different Convolutional Neural Networks" Diagnostics 12, no. 6: 1359. https://doi.org/10.3390/diagnostics12061359