
Psychological Aspect and Quality of Life in Porphyrias: A Review

 , and
, and
Abstract
:1. Introduction
2. Methods
3. Acute Hepatic Porphyrias (AHPs)
3.1. Questionnaire Assessment of Psychological Aspect of AHPs
3.2. Qualitative Approach of the Psychological Aspect of AHPs
4. Porphyria Cutanea Tarda (PCT)
5. Erythropoietic Protoporphyria (EPP)
5.1. Questionnaire Assessment of Psychological Aspect of EPP
5.2. The Qualitative Approach of the Psychological Aspect of EPP
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Phillips, J.D. Heme biosynthesis and the porphyrias. Mol. Genet. Metab. 2019, 128, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Ramanujam, V.M.; Anderson, K.E. Porphyria Diagnostics-Part 1: A Brief Overview of the Porphyrias. Curr. Protoc. Hum. Genet. 2015, 86, 17–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawe, R. An overview of the cutaneous porphyrias. F1000Research 2017, 6, 1906. [Google Scholar] [CrossRef] [PubMed]
- Di Pierro, E.; Brancaleoni, V.; Granata, F. Advances in understanding the pathogenesis of congenital erythropoietic porphyria. Br. J. Haematol. 2016, 173, 365–379. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Rudnick, S.; Cengia, B.; Bonkovsky, H.L. Acute Hepatic Porphyrias: Review and Recent Progress. Hepatol. Commun. 2019, 3, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Tian, Y.; Peng, C.; Zhang, Y.; Zhang, S. Recent advances in the epidemiology and genetics of acute intermittent porphyria. Intractable Rare Dis. Res. 2020, 9, 196–204. [Google Scholar] [CrossRef]
- Saadi, T. Porphyria: The Neglected Diagnosis. Isr. Med. Assoc. J. 2019, 21, 283–284. [Google Scholar]
- Ventura, P.; Brancaleoni, V.; Di Pierro, E.; Graziadei, G.; Macrì, A.; Carmine Guida, C.; Nicolli, A.; Rossi, M.T.; Granata, F.; Fiorentino, V.; et al. Clinical and molecular epidemiology of erythropoietic protoporphyria in Italy. Eur. J. Dermatol. 2020, 30, 532–540. [Google Scholar] [CrossRef]
- Di Pierro, E.; De Canio, M.; Mercadante, R.; Savino, M.; Granata, F.; Tavazzi, D.; Nicolli, A.M.; Trevisan, A.; Marchini, S.; Fustinoni, S. Laboratory Diagnosis of Porphyria. Diagnostics 2021, 11, 1343. [Google Scholar] [CrossRef]
- Pischik, E.; Kauppinen, R. An update of clinical management of acute intermittent porphyria. Appl. Clin. Genet. 2015, 8, 201–214. [Google Scholar] [CrossRef] [Green Version]
- Millward, L.M.; Kelly, P.; Deacon, A.; Senior, V.; Peters, T.J. Self-rated psychosocial consequences and quality of life in the acute porphyrias. J. Inherit. Metab. Dis. 2001, 24, 733–747. [Google Scholar] [CrossRef] [PubMed]
- Wikberg, A.; Jansson, L.; Lithner, F. Women’s experience of suffering repeated severe attacks of acute intermittent porphyria. J. Adv. Nurs. 2000, 32, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Edel, Y.; Mamet, R. Porphyria: What Is It and Who Should Be Evaluated? Rambam Maimonides Med. J. 2018, 9, e0013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sassa, S. Modern diagnosis and management of the porphyrias. Br. J. Haematol. 2006, 135, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Kaftory, R.; Edel, Y.; Snast, I.; Lapidoth, M.; Mamet, R.; Elis, A.; Hodak, E.; Levi, A. Greater disease burden of variegate porphyria than hereditary coproporphyria: An Israeli nationwide study of neurocutaneous porphyrias. Mol. Genet. Metab. Rep. 2021, 26, 100707. [Google Scholar] [CrossRef]
- Singal, A.K. Porphyria cutanea tarda: Recent update. Mol. Genet. Metab. 2019, 128, 271–281. [Google Scholar] [CrossRef]
- Vossen, A.R.; Boesten, L.S.; Siersema, P.D.; Nellen, R.G. Porphyria cutanea tarda: The benefit of additional diagnostics. Ned. Tijdschr. Voor Geneeskd. 2016, 160, A9166. [Google Scholar]
- Di Pierro, E.; Granata, F.; De Canio, M.; Rossi, M.; Ricci, A.; Marcacci, M.; De Luca, G.; Sarno, L.; Barbieri, L.; Ventura, P.; et al. Recognized and Emerging Features of Erythropoietic and X-Linked Protoporphyria. Diagnostics 2022, 12, 151. [Google Scholar] [CrossRef]
- Granata, F.; Duca, L.; Graziadei, G.; Brancaleoni, V.; Missineo, P.; De Luca, G.; Fustinoni, S.; Di Pierro, E. Inflammatory involvement into phototoxic reaction in erythropoietic protoporphyria (EPP) patients. Immunol. Res. 2019, 67, 382–389. [Google Scholar] [CrossRef]
- Parajuli, N.; Jha, H.K.; Jonkman, M.F. Porphyria Cutanea Tarda Presenting as Erythema-multiforme Like Lesions. J. Nepal. Health Res. Counc. 2019, 17, 119–121. [Google Scholar] [CrossRef]
- Granata, F.; Duca, L.; Brancaleoni, V.; Fustinoni, S.; De Luca, G.; Motta, I.; Graziadei, G.; Di Pierro, E. Alternative Pathway Involvement in Protoporphyria Patients Related to Sun Exposure. Front. Immunol. 2021, 12, 615620. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.; Gjengedal, E.; Sandberg, S.; Råheim, M. A skin disease, a blood disease or something in between? An exploratory focus group study of patients’ experiences with porphyria cutanea tarda. Br. J. Dermatol. 2015, 172, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balwani, M. Erythropoietic Protoporphyria and X-Linked Protoporphyria: Pathophysiology, genetics, clinical manifestations, and management. Mol. Genet. Metab. 2019, 128, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Genovese, G.; Maronese, C.A.; Moltrasio, C.; Piccinno, R.; Marletta, D.A.; De Luca, G.; Graziadei, G.; Granata, F.; Di Pierro, E.; Cappellini, M.D.; et al. Ultraviolet A phototest positivity is associated with higher free erythrocyte protoporphyrin IX concentration and lower transferrin saturation values in erythropoietic protoporphyria. Photodermatol. Photoimmunol. Photomed. 2021, 38, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Biolcati, G.; Hanneken, S.; Minder, E.I.; Neumann, N.J.; Wilson, J.H.P.; Wolgen, P.J.; Wright, D.J.; Lloyd, A.J. Correction to: Validation of a novel patient reported tool to assess the impact of treatment in erythropoietic protoporphyria: The EPP-QoL. J. Patient Rep. Outcomes 2021, 5, 73. [Google Scholar] [CrossRef] [PubMed]
- Honor, A.; Rudnick, S.R.; Bonkovsky, H.L. Givosiran to treat acute porphyria. Drugs Today 2021, 57, 47–59. [Google Scholar] [CrossRef]
- Barman-Aksözen, J.; Nydegger, M.; Schneider-Yin, X.; Minder, A.E. Increased phototoxic burn tolerance time and quality of life in patients with erythropoietic protoporphyria treated with afamelanotide—A three years observational study. Orphanet. J. Rare Dis. 2020, 15, 213. [Google Scholar] [CrossRef]
- Wensink, D.; Wagenmakers, M.A.E.M.; Langendonk, J.G. Afamelanotide for prevention of phototoxicity in erythropoietic protoporphyria. Expert Rev. Clin. Pharmacol. 2021, 14, 151–160. [Google Scholar] [CrossRef]
- Bonkovsky, H.L.; Dixon, N.; Rudnick, S. Pathogenesis and clinical features of the acute hepatic porphyrias (AHPs). Mol. Genet. Metab. 2019, 128, 213–218. [Google Scholar] [CrossRef]
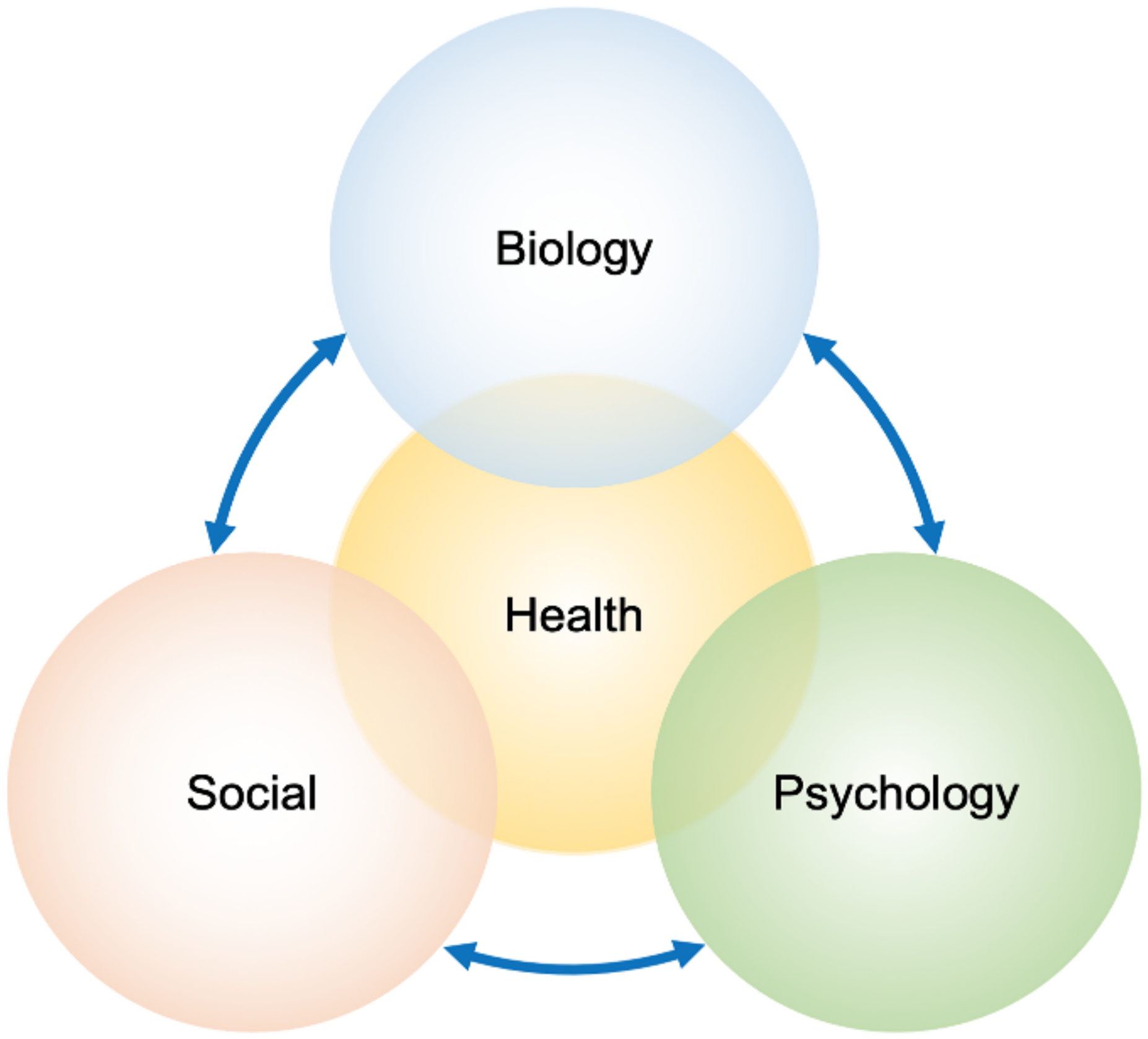
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Adler, R.H. Engel’s biopsychosocial model is still relevant today. J. Psychosom. Res. 2009, 67, 607–611. [Google Scholar] [CrossRef]
- Kusnanto, H.; Agustian, D.; Hilmanto, D. Biopsychosocial model of illnesses in primary care: A hermeneutic literature review. J. Family Med. Prim. Care 2018, 7, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Millward, L.M.; Kelly, P.; King, A.; Peters, T.J. Anxiety and depression in the acute porphyrias. J. Inherit. Metab. Dis. 2005, 28, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Tsang, A.; Von Korff, M.; Lee, S.; Alonso, J.; Karam, E.; Angermeyer, M.C.; Borges, G.L.; Bromet, E.J.; Demytteneare, K.; de Girolamo, G.; et al. Common chronic pain conditions in developed and developing countries: Gender and age differences and comorbidity with depression-anxiety disorders. J. Pain 2008, 9, 883–891. [Google Scholar] [CrossRef]
- Bannon, S.; Greenberg, J.; Mace, R.A.; Locascio, J.J.; Vranceanu, A.M. The role of social isolation in physical and emotional outcomes among patients with chronic pain. Gen. Hosp. Psychiatry 2021, 69, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Monreal, A.M.; Murcia, M.; Gómez-Murcia, V.; Bibiloni, M.D.M.; Pons, A.; Tur, J.A.; Martínez-Tomé, M. Anthropometric and Quality-of-Life Parameters in Acute Intermittent Porphyria Patients. Medicine 2015, 94, e1023. [Google Scholar] [CrossRef]
- Yang, J.; Zhu, T.; Zhao, Y.; Yu, X.; Zhu, H.; Jiang, Y.; Li, X. Acute Intermittent Porphyria in the North of China: The Acute Attack Effect on Quality of Life and Psychological Condition. BioMed Res. Int. 2018, 2018, 3216802. [Google Scholar] [CrossRef] [Green Version]
- Bronisch, O.; Stauch, T.; Haverkamp, T.; Beykirch, M.K.; Petrides, P.E. Acute porphyrias: A German monocentric study of the biochemical, molecular genetic, and clinical data of 62 families. Ann. Hematol. 2019, 98, 2683–2691. [Google Scholar] [CrossRef]
- Gerber, L.H.; Weinstein, A.A.; Mehta, R.; Younossi, Z.M. Importance of fatigue and its measurement in chronic liver disease. World J. Gastroenterol. 2019, 25, 3669–3683. [Google Scholar] [CrossRef]
- Bathen, T.; Johansen, H.; Strømme, H.; Velvin, G. Experienced fatigue in people with rare disorders: A scoping review on characteristics of existing research. Orphanet. J. Rare Dis. 2022, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Gouya, L.; Ventura, P.; Balwani, M.; Bissell, D.M.; Rees, D.C.; Stölzel, U.; Phillips, J.D.; Kauppinen, R.; Langendonk, J.G.; Desnick, R.J.; et al. EXPLORE: A Prospective, Multinational, Natural History Study of Patients with Acute Hepatic Porphyria with Recurrent Attacks. Hepatology 2020, 71, 1546–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naik, H.; Stoecker, M.; Sanderson, S.C.; Balwani, M.; Desnick, R.J. Experiences and concerns of patients with recurrent attacks of acute hepatic porphyria: A qualitative study. Mol. Genet. Metab. 2016, 119, 278–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, A.; Pompilus, F.; Querbes, W.; Wei, A.; Strzok, S.; Penz, C.; Howe, D.L.; Hungate, J.R.; Kim, J.B.; Agarwal, S.; et al. Patient Perspective on Acute Intermittent Porphyria with Frequent Attacks: A Disease with Intermittent and Chronic Manifestations. Patient 2018, 11, 527–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, L.; Burrell, S.; Chamberlayne, J.; Lombardelli, S.; Mora, J.; Mason, N.; Schurer, M.; Merkel, M.; Meninger, S.; Ko, J.J. Patient and caregiver experiences of living with acute hepatic porphyria in the UK: A mixed-methods study. Orphanet. J. Rare Dis. 2021, 16, 187. [Google Scholar] [CrossRef]
- Jong, C.T.; Finlay, A.Y.; Pearse, A.D.; Kerr, A.C.; Ferguson, J.; Benton, E.C.; Hawk, J.L.; Sarkany, R.P.; McMullen, E.; Rhodes, L.E.; et al. The quality of life of 790 patients with photodermatoses. Br. J. Dermatol. 2008, 159, 192–197. [Google Scholar] [CrossRef]
- Yasuda, M.; Chen, B.; Desnick, R.J. Recent advances on porphyria genetics: Inheritance, penetrance & molecular heterogeneity, including new modifying/causative genes. Mol. Genet. Metab. 2019, 128, 320–331. [Google Scholar] [CrossRef]
- Andersen, J.; Nordin, K.; Sandberg, S. Illness Perception and Psychological Distress in Persons with Porphyria Cutanea Tarda. Acta Derm. Venereol. 2016, 96, 674–678. [Google Scholar] [CrossRef] [Green Version]
- Andersen, J.; Thomsen, J.; Enes, Å.; Sandberg, S.; Aarsand, A.K. Health-related quality of life in porphyria cutanea tarda: A cross-sectional registry based study. Health Qual. Life Outcomes 2020, 18, 84. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Turk, D.C.; Angst, M.S.; Dionne, R.; Freeman, R.; Hansson, P.; Haroutounian, S.; Arendt-Nielsen, L.; Attal, N.; et al. Patient phenotyping in clinical trials of chronic pain treatments: IMMPACT recommendations. Pain 2016, 157, 1851–1871. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.C.; Pearce, S.A.; Turner-Stokes, L.; Jones, A. The Pain Beliefs Questionnaire: An investigation of beliefs in the causes and consequences of pain. Pain 1992, 51, 267–272. [Google Scholar] [CrossRef]
- Kim, E.S.; Garnock-Jones, K.P. Afamelanotide: A Review in Erythropoietic Protoporphyria. Am. J. Clin. Dermatol. 2016, 17, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Minder, E.I. Afamelanotide, an agonistic analog of α-melanocyte-stimulating hormone, in dermal phototoxicity of erythropoietic protoporphyria. Expert Opin. Investig. Drugs 2010, 19, 1591–1602. [Google Scholar] [CrossRef]
- Langendonk, J.G.; Balwani, M.; Anderson, K.E.; Bonkovsky, H.L.; Anstey, A.V.; Bissell, D.M.; Bloomer, J.; Edwards, C.; Neumann, N.J.; Parker, C.; et al. Afamelanotide for Erythropoietic Protoporphyria. N. Engl. J. Med. 2015, 373, 48–59. [Google Scholar] [CrossRef]
- O’Neill, T.A. An Overview of Interrater Agreement on Likert Scales for Researchers and Practitioners. Front. Psychol. 2017, 8, 777. [Google Scholar] [CrossRef] [Green Version]
- Biolcati, G.; Marchesini, E.; Sorge, F.; Barbieri, L.; Schneider-Yin, X.; Minder, E.I. Long-term observational study of afamelanotide in 115 patients with erythropoietic protoporphyria. Br. J. Dermatol. 2015, 172, 1601–1612. [Google Scholar] [CrossRef]
- Wakefield, E.O.; Zempsky, W.T.; Puhl, R.M.; Litt, M.D. Conceptualizing pain-related stigma in adolescent chronic pain: A literature review and preliminary focus group findings. Pain Rep. 2018, 3, e679. [Google Scholar] [CrossRef]
- MacLeod, J.S.; Austin, J.K. Stigma in the lives of adolescents with epilepsy: A review of the literature. Epilepsy Behav. 2003, 4, 112–117. [Google Scholar] [CrossRef]
- Martin, S.R.; Cohen, L.L.; Mougianis, I.; Griffin, A.; Sil, S.; Dampier, C. Stigma and Pain in Adolescents Hospitalized for Sickle Cell Vasoocclusive Pain Episodes. Clin. J. Pain 2018, 34, 438–444. [Google Scholar] [CrossRef]
- Sartorius, N. Depression and diabetes. Dialogues Clin. Neurosci. 2018, 20, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Toumi, M.L.; Merzoug, S.; Boulassel, M.R. Does sickle cell disease have a psychosomatic component? A particular focus on anxiety and depression. Life Sci. 2018, 210, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Bartkowska, W.; Samborski, W.; Mojs, E. Cognitive functions, emotions and personality in woman with fibromyalgia. Anthropol. Anz. 2018, 75, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T.; Halligan, P.W. The biopsychosocial model of illness: A model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef]
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Naik, H.; Overbey, J.R.; Desnick, R.J.; Anderson, K.E.; Bissell, D.M.; Bloomer, J.; Bonkovsky, H.L.; Phillips, J.D.; Wang, B.; Singal, A.; et al. Evaluating quality of life tools in North American patients with erythropoietic protoporphyria and X-linked protoporphyria. JIMD Rep. 2019, 50, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Wensink, D.; Wagenmakers, M.A.E.M.; Barman-Aksözen, J.; Friesema, E.C.H.; Wilson, J.H.P.; van Rosmalen, J.; Langendonk, J.G. Association of Afamelanotide with Improved Outcomes in Patients With Erythropoietic Protoporphyria in Clinical Practice. JAMA Dermatol. 2020, 156, 570–575. [Google Scholar] [CrossRef]
- Rutter, K.J.; Ashraf, I.; Cordingley, L.; Rhodes, L.E. A review of studies looking at quality of life and psychological impact in people with photodermatoses—Skin diseases triggered by sunlight. Br. J. Dermatol. 2020, 182, e161–e182. [Google Scholar] [CrossRef]
- Rutter, K.J.; Ashraf, I.; Cordingley, L.; Rhodes, L.E. Quality of life and psychological impact in the photodermatoses: A systematic review. Br. J. Dermatol. 2020, 182, 1092–1102. [Google Scholar] [CrossRef]
- Eccleston, C.; Crombez, G. Worry and chronic pain: A misdirected problem solving model. Pain 2007, 132, 233–236. [Google Scholar] [CrossRef]
- Rufener, E.A. Erythropoietic protoporphyria: A study of its psychosocial aspects. Br. J. Dermatol. 1987, 116, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Kao, G.S. The Pain of Invisibility: A Perspective on the Treatment of Pediatric Chronic Pain. J. Patient Exp. 2020, 7, 845–847. [Google Scholar] [CrossRef] [PubMed]
- Uhlenbusch, N.; Löwe, B.; Härter, M.; Schramm, C.; Weiler-Normann, C.; Depping, M.K. Depression and anxiety in patients with different rare chronic diseases: A cross-sectional study. PLoS ONE 2019, 14, e0211343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von der Lippe, C.; Diesen, P.S.; Feragen, K.B. Living with a rare disorder: A systematic review of the qualitative literature. Mol Genet. Genomic. Med. 2017, 5, 758–773. [Google Scholar] [CrossRef]
- Naik, H.; Shenbagam, S.; Go, A.M.; Balwani, M. Psychosocial issues in erythropoietic protoporphyria—The perspective of parents, children, and young adults: A qualitative study. Mol. Genet. Metab. 2019, 128, 314–319. [Google Scholar] [CrossRef]
- Meints, S.M.; Edwards, R.R. Evaluating psychosocial contributions to chronic pain outcomes. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 87, 168–182. [Google Scholar] [CrossRef]
- Hussein, S.; Sadeh, Y.; Dekel, R.; Shadmi, E.; Brezner, A.; Landa, J.; Silberg, T. Using a biopsychosocial approach to examine differences in post-traumatic stress symptoms between Arab and Jewish Israeli mothers following a child’s traumatic medical event. Int. J. Equity Health 2021, 20, 89. [Google Scholar] [CrossRef]
- Turk, D.C.; Fillingim, R.B.; Ohrbach, R.; Patel, K.V. Assessment of Psychosocial and Functional Impact of Chronic Pain. J. Pain 2016, 17, T21–T49. [Google Scholar] [CrossRef]
- Dicicco-Bloom, B.; Crabtree, B.F. The qualitative research interview. Med. Educ. 2006, 40, 314–321. [Google Scholar] [CrossRef]
- Buendía-Martínez, J.; Barreda-Sánchez, M.; Rodríguez-Peña, L.; Ballesta-Martínez, M.J.; López-González, V.; Sánchez-Soler, M.J.; Serrano-Antón, A.T.; Pérez-Tomás, M.E.; Gil-Ferrer, R.; Avilés-Plaza, F.; et al. Health impact of acute intermittent porphyria in latent and non-recurrent attacks patients. Orphanet. J. Rare Dis. 2021, 16, 106. [Google Scholar] [CrossRef]
- Bustad, H.J.; Kallio, J.P.; Vorland, M.; Fiorentino, V.; Sandberg, S.; Schmitt, C.; Aarsand, A.K.; Martinez, A. Acute Intermittent Porphyria: An Overview of Therapy Developments and Future Perspectives Focusing on Stabilisation of HMBS and Proteostasis Regulators. Int. J. Mol. Sci. 2021, 22, 675. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef] [PubMed]
- Hylands-White, N.; Duarte, R.V.; Raphael, J.H. An overview of treatment approaches for chronic pain management. Rheumatol. Int. 2017, 37, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Romm, M.J.; Ahn, S.; Fiebert, I.; Cahalin, L.P. A Meta-Analysis of Group-Based Pain Management Programs: Overall Effect on Quality of Life and Other Chronic Pain Outcome Measures, with an Exploration into Moderator Variables that Influence the Efficacy of Such Interventions. Pain Med. 2021, 22, 407–429. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [Green Version]
- De Ridder, D.; Geenen, R.; Kuijer, R.; van Middendorp, H. Psychological adjustment to chronic disease. Lancet 2008, 372, 246–255. [Google Scholar] [CrossRef]
- Weermeijer, J.D.; Meulders, A. Clinimetrics: Tampa Scale for Kinesiophobia. J. Physiother. 2018, 64, 126. [Google Scholar] [CrossRef]
- Ansari, A.H.; Pal, A.; Ramamurthy, A.; Kabat, M.; Jain, S.; Kumar, S. Fibromyalgia Pain and Depression: An Update on the Role of Repetitive Transcranial Magnetic Stimulation. ACS Chem. Neurosci. 2021, 12, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Adami, G.; Gerratana, E.; Atzeni, F.; Benini, C.; Vantaggiato, E.; Rotta, D.; Idolazzi, L.; Rossini, M.; Gatti, D.; Fassio, A. Is central sensitization an important determinant of functional disability in patients with chronic inflammatory arthritides? Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X21993252. [Google Scholar] [CrossRef]
- Aich, A.; Jones, M.K.; Gupta, K. Pain and sickle cell disease. Curr. Opin. Hematol. 2019, 26, 131–138. [Google Scholar] [CrossRef]
- Williams, A.C.C.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2020, 8, CD007407. [Google Scholar] [CrossRef] [PubMed]
- Barman-Aksözen, J. Patient empowerment and access to medicines: Insights from a scientist-patient suffering from erythropoietic protoporphyria. Med. Access Point Care 2019, 3, 2399202619865167. [Google Scholar] [CrossRef] [Green Version]
- Perestelo-Pérez, L.; Rivero-Santana, A.; Abt-Sacks, A.; Toledo-Chavarri, A.; Brito, N.; Álvarez-Pérez, Y.; González-Hernández, N.; Serrano-Aguilar, P. Patient Empowerment and Involvement in Research. Adv. Exp. Med. Biol. 2017, 1031, 249–264. [Google Scholar] [CrossRef] [PubMed]
- Babić, R.; Babić, M.; Rastović, P.; Ćurlin, M.; Šimić, J.; Mandić, K.; Pavlović, K. Resilience in Health and Illness. Psychiatr. Danub. 2020, 32, 226–232. [Google Scholar]
- Jafferany, M.; Pastolero, P. Psychiatric and Psychological Impact of Chronic Skin Disease. Prim. Care Companion CNS Disord. 2018, 20. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Bassi, M.; Cilia, S.; Falautano, M.; Grobberio, M.; Niccolai, C.; Pattini, M.; Pietrolongo, E.; Quartuccio, M.E.; Viterbo, R.G.; Allegri, B.; et al. Illness perceptions and psychological adjustment among persons with multiple sclerosis: The mediating role of coping strategies and social support. Disabil. Rehabil. 2020, 42, 3780–3792. [Google Scholar] [CrossRef]
- Hagger, M.S.; Koch, S.; Chatzisarantis, N.L.D.; Orbell, S. The common sense model of self-regulation: Meta-analysis and test of a process model. Psychol. Bull. 2017, 143, 1117–1154. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Authors | Assessment Method | Age (Years) | Patients (n) | Item (n) | Score | Score Max |
|---|---|---|---|---|---|---|
| Quantitative methods by using questionnaires | ||||||
| Millward LM, et al., 2001 | Medical Outcomes Study (MOS) | >18 | 81 AIP: 51 VP: 25 HCP 5 | 20 item | Health Perception 54.1 (±2.4) | 100 |
| EuroQoL Questionnaire (EuroQoL) | NR | M 70–79 yrs = 0.10 F 60–69 yrs = 0.63 | 1 | |||
| Hospital Anxiety and Depression Scale (HADS) | 14 item | Anxiety 7.1 ± 4.9 Depression 4.6 ± 4.7 | 21 | |||
| Illness Perceptions Questionnaire (IPQ) | NR | NR | NR | |||
| Millward LM, et al., 2005 | Beck Anxiety Inventory (BAI) | >18 | 90 58 AIP 32 VP | 21 item | 10.3 ± 9.4 | 63 |
| Beck Depression Inventory (BDI) | 21 item | 8.5 ± 8.5 | 63 | |||
| State Trait Anxiety Inventory (STAI) | 20 item | 80 | ||||
| Hospital Anxiety and Depression Scale (HADS) | 14 item | NR | 21 | |||
| General Health Questionnaire (GHQ12) | 12 item | 2.21 ± 3.42 | 1 | |||
| Jiménez-Monreal AM, et al., 2015 | Health-related Quality of Life Questionnaire (EQ-5D) | >18 | 32 (AIP) | 5 domains | VAS 61.60 | 100 |
| Activities of Daily Living (Katz-ADL and Barthal Index) | 10 item | 81.5% independent | 100 | |||
| Yang J, et al., 2018 | SF-36 Health Survey (Chinese version 1.0) | mean 29 | 27 | 36 item | 85.74 | 100 |
| Event Scale-Revised Questionnaire (IES-R) | 22 item | 36.7 ± 11.8 | > 26 | |||
| Bronisch O, et al., 2019 | Porphyria-oriented Quality of Life Questionnaire | >18 | 62 | 9 item | 5 | 10 |
| Gouya L, et al., 2020 | EuroQoL 5–Dimensions Questionnaire 5–Levels (EQ–5D–5L) | ≥18 | 112 104 AIP 3 HCP 5 VP | 5 item | 0.78 | 1 |
| Qualitative descriptive approaches | ||||||
| Wikberg A, et al., 2000 | Qualitative approach (interwiew) | mean 55 | 5 | 20 ± 45 min | NR | NR |
| Naik H, et al., 2016 | Focus group with interactive discussion | >18 | 16 15 AIP 1 VP | 1.5–2 h interview | No score | NR |
| Simon A, et al., 2018 | Qualitative one-on-one interviews | mean 40 | 19 | 2 h interview | No score | NR |
| Gill L, et al., 2021 | Online survey | ≥18 | 38 28 AIP 9 VP 1 HCP | NR | No score | NR |
| Telephone interview | 10 on 38 were eligible | 1 h interview | ||||
| Authors | Assessment Method | Age (Years) | Patients (n) | Item (n) | Score | Score Max |
|---|---|---|---|---|---|---|
| Quantitative methods by using questionnaires | ||||||
| Jong CT, et al., 2008 | Dermatology Life Questionnaire Index (DLQI) | Mean 57 | 12 | 10 item | >10 | 30 |
| Andersen J, et al., 2016 | Brief Illness Perception Questionnaire (BIPQ) | 25–78 | 263 | 8 item | A group 39.6 (35.8–43.4) R group 29.7 (27.9–31.5) L group 27.2 (23.3–31.1) | Between group p < 0.01 |
| Self-reported Health Complaints (SHC) | 29 item | A group 20.5 (16.7–24.2) R group 14.1 (12.4–15.8) L group 10.7 (7.7–13.7) | ||||
| INTRUSION: Impact of Events Scale (IES) | 7/15 item | A group 11.7 (9.1–14.3) R group 6.1 (5.1–7.1) L group 3.0 (1.6–4.4) | ||||
| AVOIDANCE: Impact of Events Scale (IES) | 8/15 item | A group 12.1 (9.5–14.7) R group 6.1 (5.1–7.1) L group 4.3 (2.2–6.4) | ||||
| Andersen J, et al., 2020 | Short Form-12 Health Survey vs. 2 (SF-12) | 24–79 | 12 | 12 item | PCS mean 48 MCS mean 47 | Mean 50 |
| Qualitative descriptive approaches | ||||||
| Andersen J, et al., 2015 | Qualitative approach (interactive discussion) | 31–77 | 21 | 1.5 h of interview | Higher impact of disease | NR |
| Authors | Assessment Method | Age (Years) | Patients (n) | Item (n) | Score | Score Max |
|---|---|---|---|---|---|---|
| Quantitative methods by using questionnaires | ||||||
| Langendonk JG, et al., 2015 | EPP disease-specific Quality of Life Questionnaire (EPPQoL) | >18 | 167 | 12-item | 31% | 100% |
| Biolcati G, et al., 2015 | EPP—specific Quality of Life (QoL) Questionnaire by Clinuvel | >18 | 173 | 18/16-item | 4 | 10 |
| Naik H, et al., 2019 Apr. | PROMIS | >18 | 193 | NR | Higher for pain | NR |
| HADS | 103 | NR | Border line | NR | ||
| IPQR | 104 | NR | Higher | >20 | ||
| XLP/EPP-specific tools | 107 | 7 day recall | Higher | 100 | ||
| Barman-Aksözen J, et al., 2020 | EPP-QoL Questionnaire | >18 | 35 | 12 item | 49.10% | 100% |
| Qualitative descriptive approaches | ||||||
| Rufener AE. 1989 | EPP Questionnaire + Structurated interview | >18 | 10 | 25-item | NR | NR |
| Structurated interview | 7–11 >18 | 12 | 3–6 h of interview | |||
| Naik H, et al., 2019 Jan. | Qualitative approach (focus group with interactive discussion) | 10-nov | 6 | 17 open questions | NR | NR |
| 24–25 | 4 | |||||
| Parents 29–55 | 14 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francesca, G.; Nicolli, A.; Colaiocco, A.; Di Pierro, E.; Graziadei, G. Psychological Aspect and Quality of Life in Porphyrias: A Review. Diagnostics 2022, 12, 1193. https://doi.org/10.3390/diagnostics12051193
Francesca G, Nicolli A, Colaiocco A, Di Pierro E, Graziadei G. Psychological Aspect and Quality of Life in Porphyrias: A Review. Diagnostics. 2022; 12(5):1193. https://doi.org/10.3390/diagnostics12051193
Chicago/Turabian StyleFrancesca, Granata, Annamaria Nicolli, Alessia Colaiocco, Elena Di Pierro, and Giovanna Graziadei. 2022. "Psychological Aspect and Quality of Life in Porphyrias: A Review" Diagnostics 12, no. 5: 1193. https://doi.org/10.3390/diagnostics12051193