1. Introduction
Cervical cancer currently occupies second place as the most common cancer in young women between 15 and 44 years old. It is responsible for more than 500 thousand cases every year worldwide [
1], ranking as the third most common cancer type [
2]. Globally, around 200 thousand women die every year from cervical cancer, and both the mortality rates and incidence rates are highest in developing sub-Saharan countries [
3]. Women in the 35–66-years-old age group account for two-thirds of all cervical cancers, with a median age at diagnosis of 49 years [
4]. The prognosis in developed countries such as the UK is excellent, where more than 60% of women survive ten years after diagnosis. The 5-year relative survival for the International Federation of Obstetrics and Gynecology (FIGO) stage I is 96% in the United Kingdom and 92% in the United States of America [
5]. On the other side, 87% of all deaths caused by cervical cancer happen in developing countries [
3].
Intensive screening for cervical cancer allows for early detection by performing the widely used Pap smear with microscopic evaluation. The most frequently observed cancer histology is squamous-cell carcinoma (SCC), accounting for 90% of all cervical cancers, while the remaining part is caused by adenocarcinomas (ADC) in around 9% of cases and other histology variants in 1% [
6]. The sexually transmitted human papillomavirus (HPV) is the main cause of the development of SCC of the cervix [
7,
8]; it is classified into low-risk and high-risk types, with the latter also known as oncogenic HPV type. If the viral infection is not cleared within 12 to 24 months, it will tend to progress to a precancerous state [
9], starting as cervical intraepithelial neoplasia (CIN) and evolving to invasive cancer through biochemical and molecular alterations, such as down-regulating e-cadherins [
10,
11], histidine phosphatase [
12], the nucleotide-binding oligomerization domain protein-1 (NOD1) [
13], and other proteins. According to the VIVIANE study [
14], the highest-risk strains are, in descending order, HPV33, HPV16, HPV18, HPV31, and HPV45. High-risk HPV is found in 99.7% of cervical cancers [
15], but other risk factors such as chlamydia trachomatis have been discovered in 40% of SCC cases [
16], while the human immunodeficiency virus (HIV) and herpes simplex virus 2 (HSV-2) infections are also associated with cervical cancer [
17]. Nutritional behavior, use of oral contraceptive pills, smoking, obesity, and inflammatory diseases are also correlated with a higher chance of developing cervical cancer [
18].
Since the start of the coronavirus disease 2019 (COVID-19) pandemic, health services have made steps to expand their admission capacity for COVID-19 patients while decreasing the circulation of non-COVID-19 patients. This objective has been accomplished by minimizing outpatient visits and deferring tests, treatments, and elective surgery. These measures may disproportionately impact cancer patients, since the period between diagnosis and treatment commencement might negatively affect results. National screening programs were temporarily discontinued in certain areas to relieve pressure on health systems by urging the deferral of non-emergency visits, examinations, and treatments during quarantine [
19]. Additionally, the medical management of new cases was delayed due to the reorganization of health facilities and patients’ fear of interaction with COVID-19 [
20]. In countries such as the United States, a considerable decline in the frequency of screening tests and, subsequently, in the number of malignant and precursor lesions diagnosed has already been documented. In a conservative analysis of the effect of COVID-19 on breast and colorectal cancer screening and treatment in the United States, it is estimated that nearly 10,000 additional deaths will occur over the next decade, representing an increase of approximately 1% in the total number of deaths during a period when we would expect nearly 1 million deaths from the two most common tumors affecting women [
21].
Similarly to other European Union countries, the Romanian national screening programs were temporarily put on hold during the lockdown at the pandemic’s peak as a governmental measure to prevent SARS-CoV-2 infection. This program allowed women aged 21 to 65 years old to benefit from free annual Pap smears for the early detection of cervical lesions [
22]. Although official statistics regarding the cases of cancer diagnosed during the COVID-19 pandemic have not yet been released, we observed an important decrease in the number of newly diagnosed cases of cervical cancer, as well as a decrease in women requesting investigations for cervical cancer in our clinical practice during the past 24 months of the ongoing pandemic. This raised concerns about the number of cases of cervical cancer that had been missed. Considering this hypothesis, we developed a study that aimed to determine the influence of the first 24 months of the COVID-19 pandemic on the delivery of cervical cancer tests, the stage at which new cervical cancer patients were diagnosed, and their access to cancer care.
2. Materials and Methods
An observational study was organized at the University Clinic of Obstetrics and Gynecology “Bega” of the Timis County Emergency Clinical Hospital “Pius Brinzeu” from Timisoara, Romania, affiliated with the “Victor Babes” University of Medicine and Pharmacy. The research population and characteristics of interest were identified using a population-based administrative database on patients that presented during the study period in the outpatient setting of the same clinic. Our centralized database included patient medical records kept under privacy protection and patient consent, including their medical history, cervical cytology tests, and surgical and oncological data.
In Timis County, a region served by our clinic, approximately 300 thousand women are eligible to undergo cervical cytology tests annually. Women that are diagnosed with a high-grade cytology result following our analysis are advised to undergo a colposcopy, while those with a low-grade cytology result are advised to repeat cytology in six months. Colposcopy enables a doctor to detect a cervical lesion, confirm the diagnosis by biopsy, and recommend therapy for cervical cancer precursors or conservative care in the absence of cancer precursors. The research included all women aged 21 to 65 years old who had cervical screening cytology, colposcopy, or cancer therapy between January 2018 and January 2022. Individuals under the age of 21 were omitted, as were those 65 years and older.
The variables considered for evaluation comprised patient background data; the number of cervical cytology tests, HPV tests, and colposcopies performed; tumor staging; the interval from biopsy to first cancer center visit; and cancer therapy between the pre-pandemic and pandemic period. Cervical cancer staging was based on the 2018 International Federation of Gynecology and Obstetrics (FIGO) staging system [
23]. The pre-pandemic period was considered as the 24 months period from January 2018 until January 2020, while the pandemic period comprised the time frame between January 2020 and January 2022.
The Local Commission of Ethics for Scientific Research from the Timis County Emergency Clinical Hospital “Pius Brinzeu” from Timisoara, Romania, operates under article 167 provisions of Law no. 95/2006, art. 28, chapter VIII of order 904/2006; with EU GCP Directives 2005/28/EC, International Conference of Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH); and with the Declaration of Helsinki—Recommendations Guiding Medical Doctors in Biomedical Research Involving Human Subjects. The current study was approved on 10 January 2022, with approval number 17.
Statistical analysis was performed using the IBM SPSS software version 26.0. Categorical variables were represented as absolute and percentage values. Student’s t-test and Mann–Whitney U-test were used for continuous and discrete variables, respectively. The χ2 and Fisher’s exact tests were used for the statistical analysis of proportions. The significance threshold was set at α = 0.05. The patient loss ratio (PLR) was computed to offer comparative measures of change in patients presenting for cervical cancer investigations across subpopulations. The PLR = (PP-DP)/MA, and it was determined by dividing the difference between the pre-pandemic yearly average by subpopulation (PP) and the during-pandemic yearly number of patients by subpopulation (DP) by the monthly average during the pandemic (MA). Positive PLR levels imply a drop in investigations, while negative PLR values indicate an increase. The size of the PLR value indicates the relative degree of the investigation’s decrease or growth.
3. Results
Since the beginning of the COVID-19 pandemic in Romania in February 2020, and the subsequent lockdown measures implemented to delay the spread of SARS-CoV-2, we have seen a considerable drop in the number of cervical cancer screening tests and newly diagnosed cervical cancer patients. This decline was notably different from the pattern in the preceding two years (2018 and 2019), despite the absence of any reason to anticipate an abrupt epidemiological shift. Thus, the fundamental assumption backed by existing cancer burden data [
24] is that cervical cancer typically takes between ten and twenty years to develop [
25]; thus, the number of new cervical cancer cases did not naturally decrease or remained equivalent to the year previous to the start of the COVID-19 pandemic, but fewer of these new cases were effectively identified throughout the follow-up period.
Figure 1 presents a detailed description of the women presenting for cervical cancer investigation at our outpatient clinic before and during the COVID-19 pandemic.
A relatively linear trend in the number of cervical cancer screening tests was observed between 2018 and 2020, with insignificant seasonal changes. However, when the pandemic started at the beginning of 2020, we observed a dramatic decrease in tests performed, dropping from −17% and −62% in January and February, respectively, down to −75% in April and May, as compared with the same months before the pandemic (
Figure 1). A slight but constant uptrend continued since that period, with several months of decreased testing, consistent with the pandemic waves and government restrictions. In the last month of 2021, the numbers recovered up to −36.1% from the same pre-pandemic period, but were still significantly lower than what was considered normal before. Overall, cervical cancer investigations were significantly affected by an average percent change of 49% decrease in the volume of tests during the two years of pandemic (CI [−31.7; −68.6],
p-value < 0.001).
The general characteristics and background of patients requesting cervical cancer investigations are presented in
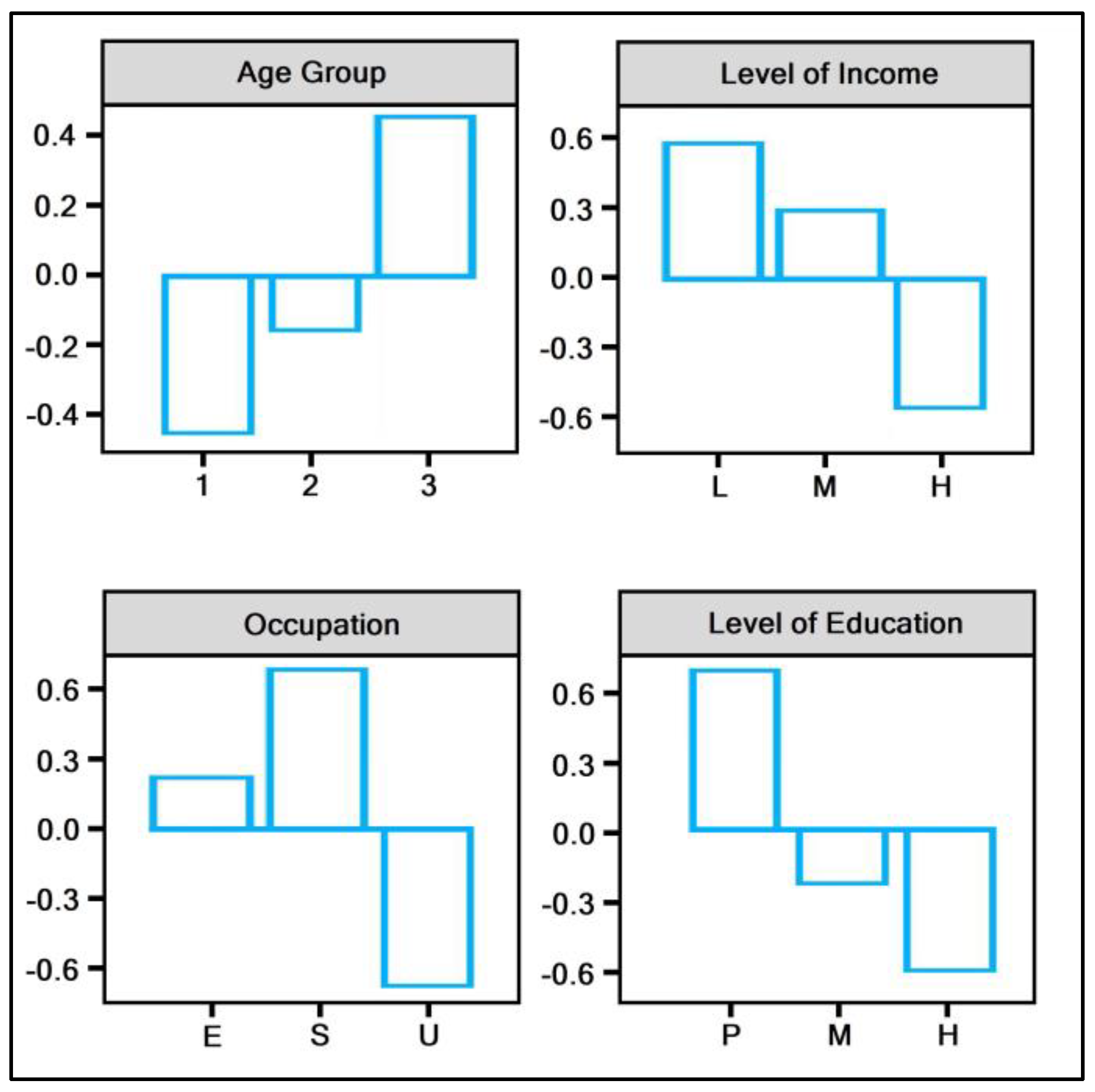
Table 1. There was a statistically significant age difference between the two study periods, both by average age of patients and by age group. The mean difference was 33.6 years before the pandemic and 32.4 years during the pandemic (
p-value = 0.002). The majority of patients presenting for investigations before and during the pandemic was in the 21–35 years age group (53.4%, respectively, 56.8%,
p-value = 0.003). The biggest patient loss ratio identified by age group was in the 50–65 years, as seen in
Figure 2. Other significant findings were identified in the level of income, where most patients were in the medium income range (53.4% pre-pandemic vs. 51.3% during the pandemic), with the biggest patient loss ratio observed in the low-income group (from 24.3% to 19.4%,
p-value < 0.001). There was an important decrease in the numbers of employed and self-employed patients during the COVID-19 pandemic, with the biggest PLR seen in the self-employed group (
p-value < 0.001). Lastly, we identified a statistically significant decrease in the level of education of patients requesting cervical cancer investigations during the pandemic, where those with primary education accounted for only 7.7% of investigations compared with 13.9% before the pandemic (
p-value < 0.001). This group was also represented by the biggest patient loss ratio (−0.6), as seen in
Figure 2.
Overall, the number of individual tests for cervical cancer was significantly decreased during the pandemic by the percentage of Pap smears, HPV tests, and colposcopies. The percentage of individuals awaiting more than four weeks of test results was statistically significantly higher during the pandemic (5.5% vs. 14.7%,
p-value < 0.001). The number of newly diagnosed cervical cancers was significantly lower from the baseline, with a 45% drop (CI [−31.6; −53.3],
p-value < 0.001). Similar concerning findings were in the stage of cancers newly diagnosed, with a significant difference in stage III cancers of 21.4% more during the pandemic (
p-value = 0.018), as shown in
Figure 3. Lastly, we observed that patients newly diagnosed with cervical cancer took significantly more time to their first cancer center visit (4.1 months vs. 6.4 months,
p-value < 0.001), and they had significantly more missed appointments than pre-pandemic times (16.1% vs. 7.6%,
p-value < 0.001), as described in
Table 2.
4. Discussion
Cervical cancer tests performed using Pap smears, HPV testing, and colposcopies, as well as treatment volumes decreased significantly during the first 24 months of the COVID-19 pandemic compared with the pre-pandemic period. The most significant decrease was observed within the March 2020 to December 2020 period, after which the numbers began to show a slight but consistent recovery. Consistent with the drop in cervical cancer investigation, each month between March and December 2020 saw an average of 49 percent fewer high-grade cytological abnormalities diagnosed. Although cervical screening, colposcopy, and treatment volumes had begun to rebound in area of study by January 2021, they had not yet recovered to pre-pandemic levels. As the pandemic progresses, it is expected that these services will continue to be reduced for a while due to a variety of factors, including rigorous infection prevention and control measures that limit the volume of human interactions that primary care providers can engage in. Additionally, depending on pandemic peaks, some primary care providers, such as our clinic, have varied between resuming in-person preventative care appointments and cancelling in-person visits.
Our findings indicated that individuals diagnosed with advanced-stage cervical malignancies during the pandemic compared with the same period prior to the pandemic. The percentage of late-stage cervical cancers (III–IV) rose significantly by 17%. During the pandemic era, the total number of new cervical cancer cases presenting at tertiary cancer centers was also lower. An intriguing discovery was that the percentage of cervical cancer cases detected during the pandemic dropped as a result of screening testing. Following a cancer diagnosis, the delay between the first visit to a cancer center reduced during the pandemic compared to the preceding era. Taking this into account, the primary effect of the COVID-19 pandemic on delaying cancer patients’ treatment seems to be a drop in the number of screening appointments and diagnostic procedures. The primary explanation for the reduction in the time between initial visits to a cancer center is that fewer patients were referred during the pandemic, improving access for those who were referred. Nonetheless, our cancer center is a tertiary care facility dedicated exclusively to oncologic patients. Less specialized centers that also serve non-oncologic patients may have needed a bigger shift in health care priorities to accommodate COVID-19 patients. Therefore, in such instances, the likelihood of delays in initiating cancer therapy after diagnosis cannot be ruled out.
Similar findings were confirmed by a study taking place in the US [
26], where an observed reduction of more than 70% in Pap smears during the lockdown period triggered an alarm sign for oncologists. Additionally, it was reported that HPV test screening rates per 100 person-months declined by more than 80 percent among women aged 30–65 years. After the lockdown was removed, screening rates in the United States rebounded to near baseline levels, in contrast to persistent declines in our area in Romania. Other studies focused on different cancer types that are dependent on screening programs to preserve good curative results, such as breast cancer and colorectal cancer. All observations converged to the same concerning fact that the COVID-19 pandemic caused a steep decline in screening and diagnosis availability, with a negative forecast in long-term cancer outcomes [
27,
28,
29]. As the pandemic persists, priority should be given to individuals at increased risk of acquiring cervical malignancies and pre-cancer. It is critical to continue to ensure that women obtain preventative services, such as cancer screening and adequate follow-up, in a safe and timely manner.
Although it is not yet possible to quantify the impact of COVID-19-related service reductions on cervical cancer outcomes and make long-term projections in Romania, a study conducted by Smith et al. [
30] suggests that disruptions to routine cervical cancer screening in 2020 could result in an increase of 1.1–3.6 percent in cervical cancer diagnoses. The researchers assessed the effect of a variety of standardized screening interruption situations in four countries with varying cervical cancer prevention strategies. Additionally, it was expected that between 2020 and 2022, there would be a 60% increase in cervical cancers, resulting in an increase in cervical cancer mortality, morbidity, or both over the long run [
31]. In addition, Gupta et al. [
32] determined a 2.52% to 3.80% increase in cervical cancer related deaths with treatment delays ranging from 9 weeks to 6 months. Davies et al. [
33] estimated that over the next 3 years there would be considerable rise in the number of newly diagnosed cervical cancer cases, while Kregting et al. [
34] forecasted a two-fold increase in cervical cancer deaths per 100,000 individuals in 10 years. Several other studies by Matsuo et al. determined that a waiting time of between 6.1 and 9.8 weeks for cervical cancer treatment was not associated with increased risk of all-cause mortality compared to a waiting time of 6 weeks [
35,
36]. Additionally, in women with early-stage cervical cancer, an 8-week delay for hysterectomy may not be related with short-term disease recurrence and shorter disease-free survival [
37].
Several limitations of the current study comprise the single-center design and data availability from patient records. Data collection from a single-center may not be representative for the entire Romanian population, as proportions of patient background characteristics may vary with large differences across the country. As a single-center that partially dealt with women infected with SARS-CoV-2 in the region, the significant decrease in patients that was observed during the COVID-19 pandemic might also have been influenced by physician overload and availability. Therefore, this single-center study may lack external validity. Additionally, population estimates might be different and patient migration from the area of study should also be taken into consideration. Above the aforementioned limitations, our study is the first in the region to describe in detail the variation in cervical cancer diagnosis and management, as well as providing detailed patient characteristics. It gives a first insight into the effects of the COVID-19 pandemic on this group of patients and provides valuable evidence to help prevent and further manage cervical cancer screening and newly diagnosed patients during a pandemic.
The careful monitoring of the downstream effects of COVID-19-related service interruptions on cervical pre-cancer and cancer outcomes will be important to help service providers plan and minimize adverse consequences. Based on these data, we anticipate similar future results in our area, and future priority measures for catch-up should be created that balance prospective resource limits with clinical needs.
5. Conclusions
The COVID-19 pandemic had a considerable detrimental influence on investigations performed to detect cervical cancer, as well as cervical cancer care in the first 24 months of the pandemic, compared to the pre-pandemic period. Although the figures are steadily improving, there is still a significant gap that might result in the missed detection of many cervical cancer cases. Not only are we missing these cases, but patients newly diagnosed with the disease are often found to have more advanced stages, and the pandemic conditions make it harder to access cancer care. We urge the implementation of further measures to close the gap between the pre- and post-pandemic periods for cervical cancer diagnosis and management.
Author Contributions
A.P. and F.B. contributed equally to this article. Conceptualization, A.P., A.G., and S.P.; methodology, A.P., A.G., and S.P.; software, C.P. and I.M.; validation, C.P. and I.M.; formal analysis, F.B. and I.B.; investigation, F.B. and I.B.; resources, S.H. and C.C.; data curation, S.H. and C.C.; writing—original draft preparation, E.B., A.G.M., and R.N.; writing—review and editing, C.A. and V.D.C.; visualization, E.B. and R.N.; supervision, A.G.M. and M.C.; project administration, C.D. and M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Local Commission of Ethics for Scientific Research from the Timis County Emergency Clinical Hospital “Pius Brinzeu” from Timisoara, Romania, operates under article 167 provisions of Law no. 95/2006, art. 28, chapter VIII of order 904/2006; with EU GCP Directives 2005/28/EC, International Conference of Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH); and with the Declaration of Helsinki—Recommendations Guiding Medical Doctors in Biomedical Research Involving Human Subjects. The current study was approved on 10 January 2022, with the approval number 17.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Escobar, N.; Plugge, E. Prevalence of human papillomavirus infection, cervical intraepithelial neoplasia and cervical cancer in imprisoned women worldwide: A systematic review and meta-analysis. J. Epidemiol. Community Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Sherris, J.; Herdman, C.; Elias, C. Cervical cancer in the developing world. West J. Med. 2001, 175, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memon, A.; Bannister, P. Epidemiology of Cervical Cancer. In Uterine Cervical Cancer; Farghaly, S., Ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- The Surveillance, Epidemiology, and End Results (SEER) Program. Available online: http://seer.cancer.gov (accessed on 21 January 2022).
- Cancer Research UK. Available online: http://info.cancerresearchuk.org (accessed on 21 January 2022).
- Nowakowski, A.; Cybulski, M.; Buda, I.; Janosz, I.; Olszak-Wąsik, K.; Bodzek, P.; Śliwczyński, A.; Teter, Z.; Olejek, A.; Baranowski, W. Cervical Cancer Histology, Staging and Survival before and after Implementation of Organised Cervical Screening Programme in Poland. PLoS ONE 2016, 11, e0155849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, M. Pathology and epidemiology of HPV infection in females. Gynecol. Oncol. 2010, 117, S5–S10. [Google Scholar] [CrossRef] [PubMed]
- Gorun, F.; Motoi, S.; Malita, D.; Navolan, D.B.; Nemescu, D.; Olariu, T.R.; Craina, M.; Vilibic-Cavlek, T.; Ciohat, I.; Boda, D.; et al. Cytomegalovirus seroprevalence in pregnant women in the western region of Romania: A large-scale study. Exp. Ther. Med. 2020, 20, 2439–2443. [Google Scholar] [CrossRef]
- Reid, R.; Stanhope, C.R.; Herschman, B.R.; Booth, E.; Phibbs, G.D.; Smith, J.P. Genital warts and cervical cancer. I. Evidence of an association between subclinical pap-illomavirus infection and cervical malignancy. Cancer 1982, 50, 377–387. [Google Scholar] [CrossRef] [Green Version]
- Branca, M.; Giorgi, C.; Ciotti, M.; Santini, D.; Di Bonito, L.; Costa, S.; Benedetto, A.; Bonifacio, D.; Di Bonito, P.; Paba, P.; et al. Down-regulation of E-cadherin is closely associated with progression of cervical intraepithelial neoplasia (CIN), but not with high-risk human papillomavirus (HPV) or disease outcome in cervical cancer. Eur. J. Gynaecol. Oncol. 2006, 27, 215–223. [Google Scholar]
- Grigoraş, M.L.; Arghirescu, T.S.; Folescu, R.; Talpoş, I.C.; Gîndac, C.M.; Zamfir, C.L.; Cornianu, M.; Anghel, M.D.; Levai, C.M. Expression of E-cadherin in lung carcinoma, other than those with small cells (NSCLC). Rom. J. Morphol. Embryol. 2017, 58, 1317–1325. [Google Scholar] [PubMed]
- Zheng, J.; Dai, X.; Chen, H.; Fang, C.; Chen, J.; Sun, L. Down-regulation of LHPP in cervical cancer influences cell proliferation, metastasis and apoptosis by modulating AKT. Biochem. Biophys. Res. Commun. 2018, 503, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Ma, H.; Fei, L.; Jiang, M.; Xia, M.; Bai, L.; Pi, X.; Chen, S.; Yu, L. HPV-mediated down-regulation of NOD1 inhibits apoptosis in cervical cancer. Infect Agents Cancer 2020, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Skinner, R.S.; Wheeler, C.M.; Romanowski, B.; Castellsagué, X.; Lazcano-Ponce, E.; Del Rosario-Raymundo, R.M.; Vallejos, C.; Minkina, G.; da Silva, D.P.; McNeil, S.; et al. Progression of HPV infection to detectable cervical lesions or clearance in adult women: Analysis of the control arm of the VIVIANE study. Int. J. Cancer 2016, 138, 2428–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin-Drubin, M.E.; Munger, K. Viruses associated with human cancer. Biochim. Et Biophys. Acta (BBA)-Mol. Basis Dis. 2008, 1782, 127–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskela, P.; Anttila, T.; Bjørge, T.; Brunsvig, A.; Dillner, J.; Hakama, M.; Lenner, P. Chlamydia trachomatis infection as a risk factor for invasive cervical cancer. Int. J. Cancer 2000, 85, 35–39. [Google Scholar] [CrossRef]
- Smith, J.S.; Herrero, R.; Bosetti, C.; Munoz, N.; Bosch, F.X.; Eluf-Neto, J.; Castellsagué, X.; Meijer, C.J.; Van den Brule, A.J.; Franceschi, S.; et al. Herpes simplex virus-2 as a human papillomavirus cofactor in the etiology of invasive cervical cancer. J. Natl. Cancer Inst. 2002, 94, 1604–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momenimovahed, Z.; Salehiniya, H. Incidence, mortality and risk factors of cervical cancer in the world. Biomed. Res. Ther. 2017, 4, 1795–1811. [Google Scholar] [CrossRef]
- Del Pilar Estevez-Diz, M.; Bonadio, R.C.; Miranda, V.C.; Carvalho, J.P. Management of cervical cancer patients during the COVID-19 pandemic: A challenge for developing countries. Ecancermedicalscience 2020, 14, 1060. [Google Scholar] [CrossRef] [PubMed]
- Bakouny, Z.; Paciotti, M.; Schmidt, A.L.; Lipsitz, S.R.; Choueiri, T.K.; Trinh, Q.D. Cancer screening tests and cancer diagnoses during the COVID-19 pandemic. J. Am. Med. Assoc. Oncol. 2021, 7, 458–460. [Google Scholar] [CrossRef]
- Sharpless, N.E. COVID-19 and cancer. Science 2020, 368, 1290. [Google Scholar] [CrossRef]
- “Alessandrescu-Rusescu” National Institute for Maternal and Child Health. Active Early Detection of Cervical Cancer by Papanicolau Testing. Available online: https://www.insmc.ro/programe-de-sanatate/programe-de-sanatate-finantate-de-ms/programele-nationale-de-sanatate-privind-bolile-netransmisibile/programul-national-de-depistare-activa-precoce-a-cancerului-de-col-uterin/ (accessed on 21 January 2022).
- Bhatla, N.; Berek, J.; Cuello, M.; Denny, L.A.; Grenman, S.; Karunaratne, K. New revised FIGO staging of cervical cancer. Abstract S020.2. In In Proceedings of the FIGO XXII World Congress of Gynecology and Obstetrics, Rio de Janeiro, Brazil, 14–19 October 2018. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease 2019 Cancer Collaboration. Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef]
- Chan, C.K.; Aimagambetova, G.; Ukybassova, T.; Kongrtay, K.; Azizan, A. Human Papillomavirus Infection and Cervical Cancer: Epidemiology, Screening, and Vaccination-Review of Current Perspectives. J. Oncol. 2019, 2019, 3257939. [Google Scholar] [CrossRef]
- Miller, M.J.; Xu, L.; Qin, J.; Hahn, E.E.; Ngo-Metzger, Q.; Mittman, B.; Tewari, D.; Hodeib, M.; Wride, P.; Saraiya, M.; et al. Impact of COVID-19 on cervical cancer screening rates among women aged 21–65 years in a large integrated health care system-Southern California, 1 January–30 September 2019 and 1 January–30 September, 2020. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.; Olson, S.; Sharma, P.; Rajendra, S. A Review of the Impact of the COVID-19 Pandemic on Colorectal Cancer Screening: Implications and Solutions. Pathogens 2021, 10, 1508. [Google Scholar] [CrossRef] [PubMed]
- Ali, J.K.; Riches, J.C. The Impact of the COVID-19 Pandemic on Oncology Care and Clinical Trials. Cancers 2021, 13, 5924. [Google Scholar] [CrossRef] [PubMed]
- Harber, I.; Zeidan, D.; Aslam, M.N. Colorectal Cancer Screening: Impact of COVID-19 Pandemic and Possible Consequences. Life 2021, 11, 1297. [Google Scholar] [CrossRef]
- Smith, M.; Hall, M.; Simms, K.; Killen, J.; Sherrah, M.; O’Farrell, X.; Rebolj, M.; Jansen, E.E.; Killen, J.; Kim, J.J.; et al. Modelled Analysis of Hypothetical Impacts of COVID-19 Related Disruptions on the National Cervical Screening Program. Report to the Department of Health (May 2020). New South Wales: Cancer Research Division, Cancer Council NSW. 2020. Available online: https://www.health.gov.au/resources/publications/modelled-analysis-of-hypothetical-impacts-of-covid-19-related-disruptions-to-the-national-cervical-screening-program (accessed on 21 January 2022).
- Smith, M.A.; Burger, E.A.; Castanon, A.; de Kok, I.M.C.M.; Hanley, S.J.B.; Rebolj, M.; Hall, M.T.; Jansen, E.E.L.; Killen, J.; O’Farrell, X.; et al. Impact of disruptions and recovery for established cervical screening programs across a range of high-income country program designs, using COVID-19 as an example: A modelled analysis. Prev. Med. 2021, 151, 106623. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Chauhan, A.S.; Prinja, S.; Pandey, A.K. Impact of COVID-19 on Outcomes for Patients with Cervical Cancer in India. JCO Glob. Oncol. 2021, 7, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.M.; Spencer, A.; Macdonald, S.; Dobson, L.; Haydock, E.; Burton, H.; Angelopoulos, G.; Martin-Hirsch, P.; Wood, N.J.; Thangavelu, A.; et al. Cervical cancer and COVID-an assessment of the initial effect of the pandemic and subsequent projection of impact for women in England: A cohort study. BJOG 2022, 11, 17098. [Google Scholar] [CrossRef]
- Kregting, L.M.; Kaljouw, S.; de Jonge, L.; Jansen, E.E.L.; Peterse, E.F.P.; Heijnsdijk, E.A.M.; van Ravesteyn, N.T.; Lansdorp-Vogelaar, I.; de Kok, I.M.C.M. Effects of cancer screening restart strategies after COVID-19 disruption. Br J Cancer 2021, 124, 1516–1523. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Ragab, O.M.; Roman, L.D.; Wright, J.D. Association between definitive chemoradiotherapy wait-time and survival in locally-advanced cervical cancer: Implications during the coronavirus pandemic. Gynecol Oncol. 2021, 161, 414–421. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Deshpande, R.R.; Klar, M.; Roman, L.D.; Wright, J.D. Association between hysterectomy wait-time and all-cause mortality for micro-invasive cervical cancer: Treatment implications during the coronavirus pandemic. Arch. Gynecol. Obstet. 2021, 11, 1–5. [Google Scholar] [CrossRef]
- Matsuo, K.; Novatt, H.; Matsuzaki, S.; Hom, M.S.; Castaneda, A.V.; Licon, E.; Nusbaum, D.J.; Roman, L.D. Wait-time for hysterectomy and survival of women with early-stage cervical cancer: A clinical implication during the coronavirus pandemic. Gynecol Oncol. 2020, 158, 37–43. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 




{kind=link}
{kind=link}
{kind=link}