
An Evaluation of Choroidal and Retinal Nerve Fiber Layer Thicknesses Using SD-OCT in Children with Childhood IgA Vasculitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Ophthalmological Examinations
2.2. Data Acquisition
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trnka, P. Henoch–Schönlein Purpura in Children. J. Paediatr. Child Health 2013, 49, 995–1003. [Google Scholar] [CrossRef]
- Ozen, S.; Pistorio, A.; Iusan, S.M.; Bakkaloglu, A.; Herlin, T.; Brik, R.; Buoncompagni, A.; Lazar, C.; Bilge, I.; Uziel, Y.; et al. EULAR/PRINTO/PRES Criteria for Henoch-Schönlein Purpura, Childhood Polyarteritis Nodosa, Childhood Wegener Granulomatosis and Childhood Takayasu Arteritis: Ankara 2008. Part II: Final Classification Criteria. Ann. Rheum. Dis 2010, 69, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulur, I.; Onder, M. Behcet Disease: New Aspects. Clin. Dermatol. 2017, 35, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, S.; Taguchi, M.; Muraoka, T.; Sakurai, Y.; Kanda, T.; Takeuchi, M. Changes in Subfoveal Choroidal Thickness Associated with Uveitis Activity in Patients with Behçet’s Disease. Br. J. Ophthalmol. 2014, 98, 1508–1513. [Google Scholar] [CrossRef] [PubMed]
- Mittal, A.; Velaga, S.B.; Falavarjani, K.G.; Nittala, M.G.; Sadda, S.R. Choroidal Thickness in Non-Ocular Behçet’s Disease—A Spectral-Domain OCT Study. J. Curr. Ophthalmol. 2017, 29, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Baytaroğlu, A.; Kadayifçilar, S.; Ağin, A.; Deliktaş, Ö.; Demir, S.; Bilginer, Y.; Karakaya, J.; Özen, S.; Eldem, B. Choroidal Vascularity Index as A Biomarker of Systemic Inflammation in Childhood Polyarteritis Nodosa and Adenosine Deaminase-2 Deficiency. Pediatr. Rheumatol. Online J. 2020, 18, 29. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Sarraf, D.; Freund, K.B.; Sadda, S.R. OCT Angiography and Evaluation of the Choroid and Choroidal Vascular Disorders. Prog. Retin. Eye Res. 2018, 67, 30–55. [Google Scholar] [CrossRef] [PubMed]
- Hassenstein, A.; Meyer, C.H. Clinical Use and Research Applications of Heidelberg Retinal Angiography and Spectral-Domain Optical Coherence Tomography—A Review. Clin. Exp. Ophthalmol. 2009, 37, 130–143. [Google Scholar] [CrossRef]
- Adhi, M.; Duker, J.S. Optical coherence tomography—Current and future applications. Curr. Opin. Ophthalmol. 2013, 24, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steiner, M.; Esteban-Ortega, M.; Muñoz-Fernández, S. Choroidal and retinal thickness in systemic autoimmune and inflammatory diseases: A review. Surv. Ophthalmol. 2019, 64, 757–769. [Google Scholar] [CrossRef]
- Prousali, E.; Dastiridou, A.; Ziakas, N.; Androudi, S.; Mataftsi, A. Choroidal thickness and ocular growth in childhood. Surv. Ophthalmol. 2021, 66, 261–275. [Google Scholar] [CrossRef]
- Barteselli, G.; Chhablani, J.; El-Emam, S.; Wang, H.; Chuang, J.; Kozak, I.; Cheng, L.; Bartsch, D.U.; Freeman, W.R. Choroidal volume variations with age, axial length, and sex in healthy subjects: A three-dimensional analysis. Ophthalmol. 2012, 119, 2572–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Miara, H.; Ouyang, P.; Jiang, B. The Comparison of Regional RNFL and Fundus Vasculature by OCTA in Chinese Myopia Population. J. Ophthalmol. 2018, 2018, 3490962. [Google Scholar] [CrossRef] [PubMed]
- Ratheesh, K.M.; Seah, L.K.; Murukeshan, V.M. Spectral phase-based automatic calibration scheme for swept source-based optical coherence tomography systems. Phys. Med. Biol. 2016, 61, 7652–7663. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.S.; Ouyang, Y.; Ruiz, H.; Sadda, S.R. Diurnal Variation of Choroidal Thickness in Normal, Healthy Subjects Measured by Spectral Domain Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Chhablani, J.; Barteselli, G.; Wang, H.; El-Emam, S.; Kozak, I.; Doede, A.L.; Bartsch, D.U.; Cheng, L.; Freeman, W.R. Repeatability and reproducibility of manual choroidal volume measurements using enhanced depth imaging optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2274–2280. [Google Scholar] [CrossRef] [Green Version]
- Pillebout, E.; Sunderkötter, C. IgA vasculitis. Semin. Immunopathol. 2021, 43, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.A.; Gupta, P.; Agarwal, A.; Chhablani, J.; Cheng, C.Y.; Keane, P.A.; Agrawal, R. State of science: Choroidal thickness and systemic health. Surv. Ophthalmol. 2016, 61, 566–581. [Google Scholar] [CrossRef]
- Inoue, R.; Sawa, M.; Tsujikawa, M.; Gomi, F. Association between the efficacy of photodynamic therapy and indocyanine green angiography findings for central serous chorioretinopathy. Am. J. Ophthalmol. 2010, 149, 441–446.e2. [Google Scholar] [CrossRef]
- Laviers, H.; Zambarakji, H. Enhanced depth imaging-OCT of the choroid: A review of the current literature. Graefes. Arch. Clin. Exp. Ophthalmol. 2014, 252, 1871–1883. [Google Scholar] [CrossRef]
- Deuter, C.M.; Kötter, I.; Wallace, G.R.; Murray, P.I.; Stübiger, N.; Zierhut, M. Behçet’s Disease: Ocular Effects and Treatment. Prog. Retin. Eye Res. 2008, 27, 111–136. [Google Scholar] [CrossRef] [PubMed]
- Evereklioglu, C. Current Concepts in the Etiology and Treatment of Behçet Disease. Surv. Ophthalmol. 2005, 50, 297–350. [Google Scholar] [CrossRef] [PubMed]
- Aristodemou, P.; Stanford, M. Therapy insight: The Recognition and Treatment of Retinal Manifestations of Systemic Vasculitis. Nat. Clin. Pract. Rheumatol. 2006, 2, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Shiari, R.; Jari, M.; Karimi, S.; Salehpour, O.; Rahmani, K.; Yeganeh, M.H.; Parvaneh, V.J.; Hajian, S.; Ghasemi, L.; Safi, S. Relationship between Ocular Involvement and Clinical Manifestations, Laboratory Findings, and Coronary Artery Dilatation in Kawasaki Disease. Eye 2020, 34, 1883–1887. [Google Scholar] [CrossRef]
- De Andrade, F.A.; Balbi, G.M.; de Azevedo, L.G.B.; Sá, G.P.; Junior, H.V.M.; Klumb, E.M.; Levy, R.A. Neuro-Ophthalmologic Manifestations in Systemic Lupus Erythematosus. Lupus 2017, 26, 522–528. [Google Scholar] [CrossRef]
- Chuah, J.; Meaney, T. Anterior Ischaemic Optic Neuropathy Secondary to Henoch–Schönlein Purpura. Eye 2005, 19, 1028. [Google Scholar] [CrossRef] [Green Version]
- Chung, Y.R.; Cho, E.H.; Jang, S.; Lee, S.Y.; Lee, E.S.; Lee, K. Choroidal Thickness Indicates Subclinical Ocular and Systemic Inflammation in Eyes with Behçet Disease without Active Inflammation. Korean J. Ophthalmol. 2018, 32, 290–295. [Google Scholar] [CrossRef]
- Tetikoglu, M.; Temizturk, F.; Sagdik, H.M.; Aktas, S.; Ozcura, F.; Ozkan, Y.; Temizturk, S. Evaluation of the Choroid, Fovea, and Retinal Nerve Fiber Layer in Patients with Rheumatoid Arthritis. Ocul. Immunol. Inflamm. 2017, 25, 210–214. [Google Scholar] [CrossRef]
- Kirin, M.; Nagy, R.; MacGillivray, T.J.; Polašek, O.; Hayward, C.; Rudan, I.; Campbell, H.; Wild, S.; Wright, A.F.; Wilson, J.F.; et al. Determinants of retinal microvascular features and their relationships in two European populations. J. Hypertens. 2017, 35, 1646–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnould, L.; Seydou, A.; Gabrielle, P.H.; Guenancia, C.; Tzourio, C.; Bourredjem, A.; El Alami, Y.; Daien, V.; Binquet, C.; Bron, A.M.; et al. Subfoveal Choroidal Thickness, Cardiovascular History, and Risk Factors in the Elderly: The Montrachet Study. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2431–2437. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.Y.; Utset, T.O.; Bernard, J.T. Retinal nerve fiber layer and macular thinning in systemic lupus erythematosus: An optical coherence tomography study comparing SLE and neuropsychiatric SLE. Lupus. 2015, 24, 1169–1176. [Google Scholar] [CrossRef] [Green Version]
- Bayram, N.; Gundogan, M.; Ozsaygılı, C.; Adelman, R.A. Posterior ocular structural and vascular alterations in severe COVID-19 patients. Graefes. Arch. Clin. Exp. Ophthalmol. 2022, 260, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Arnould, L.; Guillemin, M.; Seydou, A.; Gabrielle, P.H.; Bourredjem, A.; Kawasaki, R.; Binquet, C.; Bron, A.M.; Creuzot-Garcher, C. Association between the retinal vascular network and retinal nerve fiber layer in the elderly: The Montrachet study. PLoS ONE 2020, 15, e0241055. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| IgAV Group (n = 52) | Control Group (n = 54) | p | |
|---|---|---|---|
| Gender (F/M) # | 24/28 | 25/29 | 0.571 |
| Age (year) † | 7.1 ± 2.4 | 7.8 ± 2.3 | 0.154 |
| Hemoglobin (g/dL) † | 11.9 ± 0.9 | 11.8 ± 0.8 | 0.676 |
| CRP (mg/dL) ¶ | 3.20 (0.01–15.30) | 0.40 (0.01–3.50) | <0.001 * |
| ESR (mm/h) ¶ | 16 (5–32) | 7 (3–15) | <0.001 * |
| Creatinine (mg/dL) † | 0.60 ± 0.18 | 0.57 ± 0.14 | 0.390 |
| Albumin (mg/dL) † | 3.54 ± 0.30 | 3.48 ± 0.28 | 0.334 |
| IOP (mmHg) † | 14.2 ± 1.3 | 13.7 ± 1.2 | 0.054 |
| Visual acuity (Snellen chart, in decimal) † | 1.14 ± 0.12 | 1.17 ± 0.09 | 0.147 |
| CCT (μm) † | 532.4 ± 20.4 | 530.7 ± 26.0 | 0.704 |
| Axial length (mm) † | 22.02 ± 0.78 | 22.06 ± 0.83 | 0.817 |
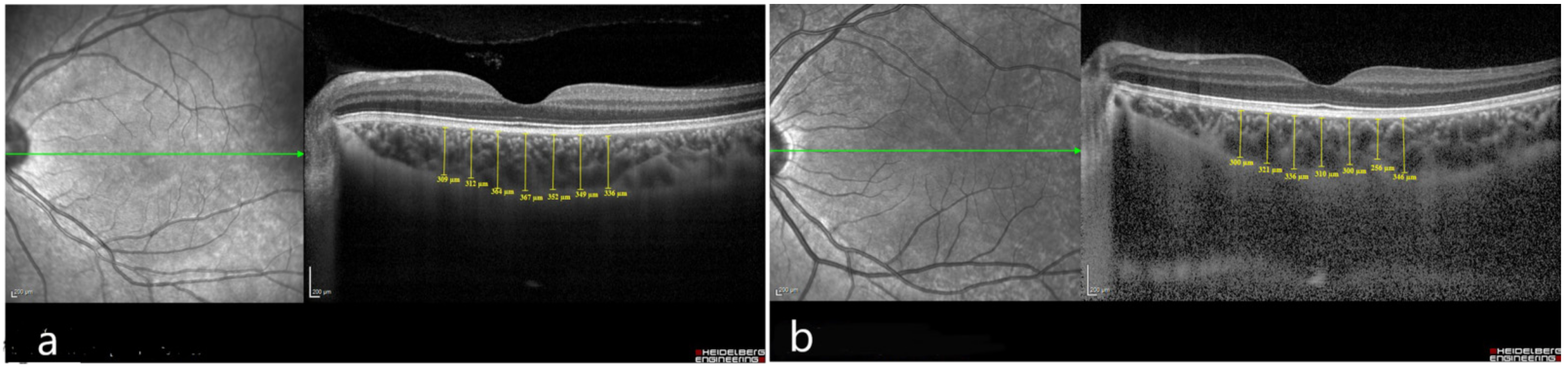
| IgAV Group (n = 52) | Control Group (n = 54) | p | |
|---|---|---|---|
| Foveal center, µm | 374.0 (315.0–452.0) | 349.5 (285.0–442.0) | 0.001 * |
| Temporal, 1500 µm | 320.5 (290.0–400.0) | 300.0 (251.0–400.0) | 0.016 * |
| Nasal, 1500 µm | 302.5 (233.0–433.0) | 290.0 (220.0–370.0) | 0.003 * |
| Temporal, 1000 µm | 342.5 (234.0–420.0) | 319.0 (254.0–420.0) | 0.009 * |
| Nasal, 1000 µm | 324.0 (261.0–418.0) | 300.0 (231.0–398.0) | 0.002 * |
| Temporal, 500 µm | 359.0 (301.0–437.0) | 332.5 (258.0–437.0) | 0.004 * |
| Nasal, 500 µm | 345.0 (250.0–493.0) | 316.0 (245.0–410.0) | 0.003 * |
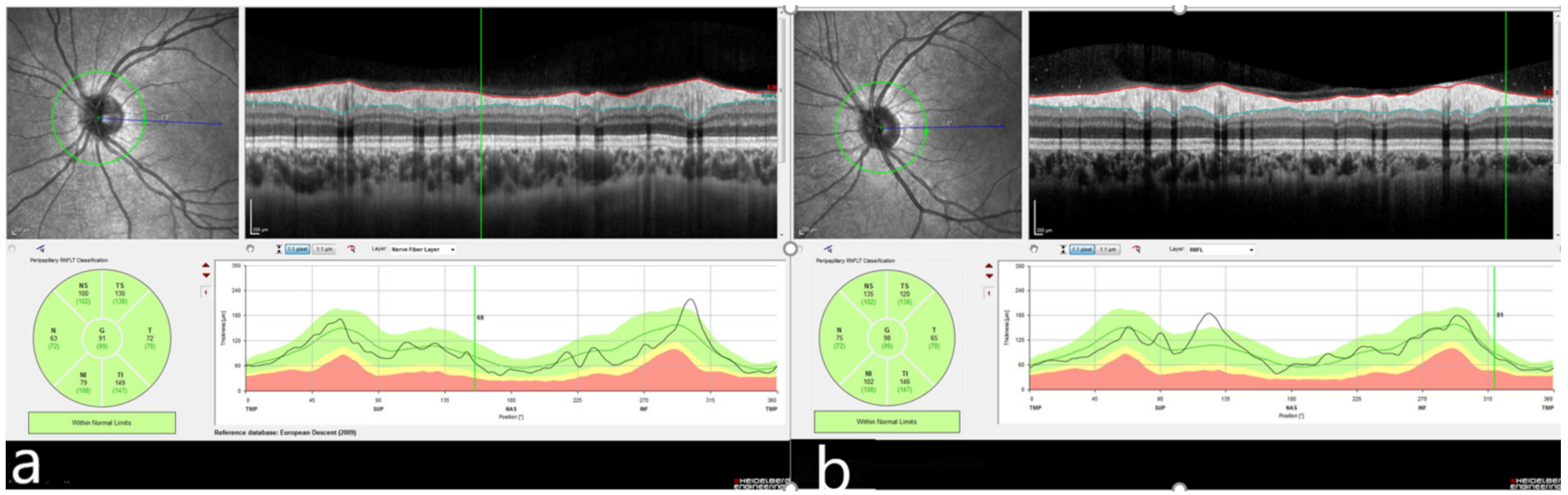
| IgAV Group (n = 52) | Control Group (n = 54) | p | |
|---|---|---|---|
| Nasal inferior RNFL, µm | 124.0 (115.0–170.0) | 113.0 (97.0–127.0) | <0.001 * |
| Nasal superior RNFL, µm | 116.0 (108.0–153.0) | 106.0 (94.0–122.0) | <0.001 * |
| Nasal RNFL, µm | 86.0 (67.0–116.0) | 75.0 (67.0–98.0) | <0.001 * |
| Temporal inferior RNFL, µm | 162.5 (135.0–189.0) | 147.0 (129.0–175.0) | <0.001 * |
| Temporal superior RNFL, µm | 149.5 (123.0–179.0) | 137.0 (115.0–165.0) | 0.001 * |
| Temporal RNFL, µm | 89.0 (70.0–117.0) | 82.5 (59.0–107.0) | 0.001 * |
| Average RNFL, µm | 110.0 (92.0–134.0) | 104.0 (89.0–117.0) | <0.001 * |
| r | R2 | Estimated Equation | 95% CI | p | |
|---|---|---|---|---|---|
| ESR-Foveal center CT | −0.12 | 1.551E−4 | y = 3.75E2 − 0.06 * x | −0.213 to +0.198 | 0.930 |
| ESR-Average RNFL | 0.126 | 0.016 | y = 1.08E2 + 0.18 * x | −0.203 to +0.425 | 0.372 |
| CRP-Foveal center CT | −0.013 | 1.773E−4 | y = 3.75E2 − 0.12 * x | −0.282 to +0.232 | 0.925 |
| CRP-Average RNFL | −0.260 | 0.068 | y = 1.14E2 − 0.67 * x | −0.463 to +0.013 | 0.062 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simsek, A.; Tekin, M. An Evaluation of Choroidal and Retinal Nerve Fiber Layer Thicknesses Using SD-OCT in Children with Childhood IgA Vasculitis. Diagnostics 2022, 12, 901. https://doi.org/10.3390/diagnostics12040901
Simsek A, Tekin M. An Evaluation of Choroidal and Retinal Nerve Fiber Layer Thicknesses Using SD-OCT in Children with Childhood IgA Vasculitis. Diagnostics. 2022; 12(4):901. https://doi.org/10.3390/diagnostics12040901
Chicago/Turabian StyleSimsek, Ali, and Mehmet Tekin. 2022. "An Evaluation of Choroidal and Retinal Nerve Fiber Layer Thicknesses Using SD-OCT in Children with Childhood IgA Vasculitis" Diagnostics 12, no. 4: 901. https://doi.org/10.3390/diagnostics12040901