
Role of Cardiac Imaging Modalities in the Evaluation of COVID-19-Related Cardiomyopathy

 , ,
, ,
Abstract
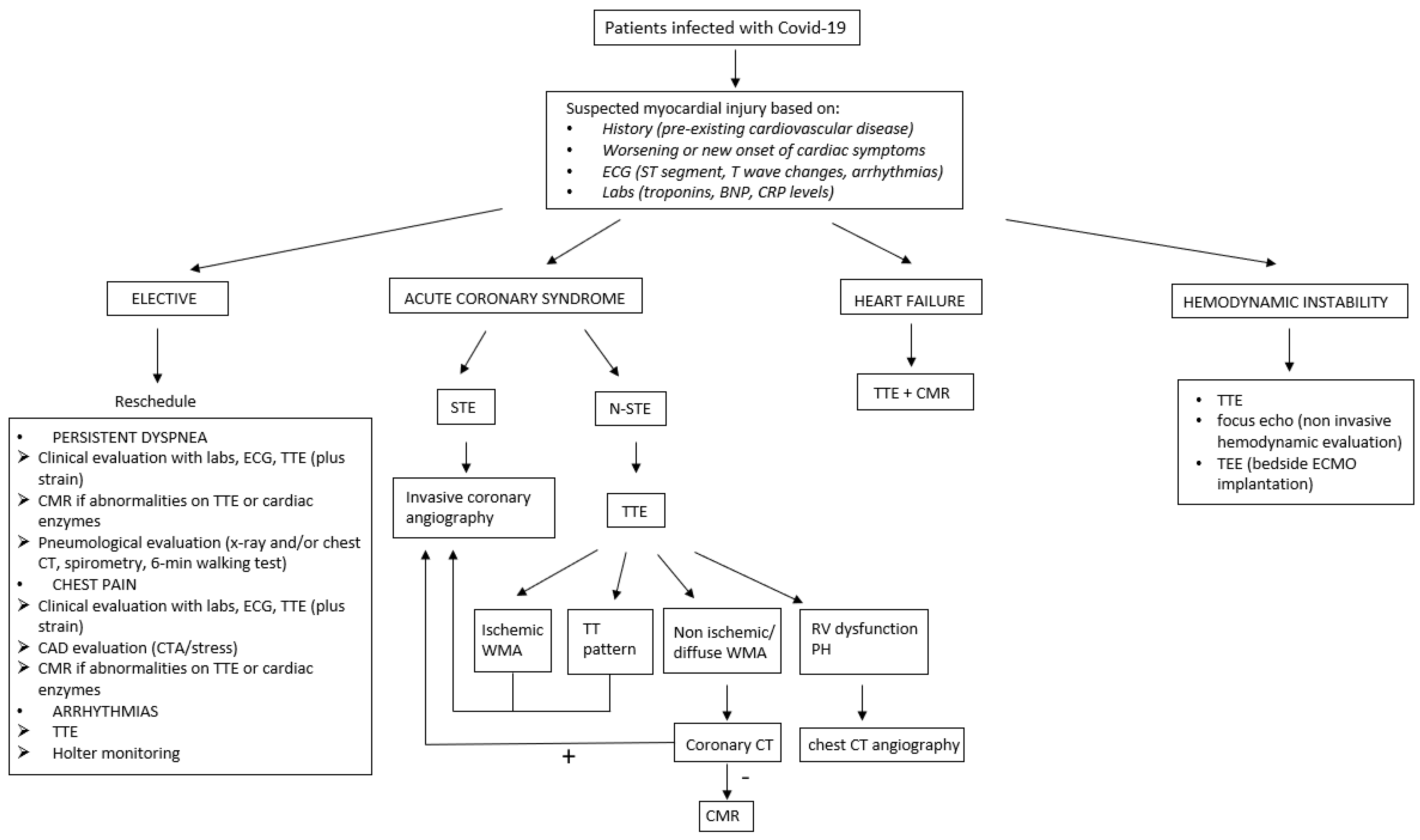
:1. Introduction
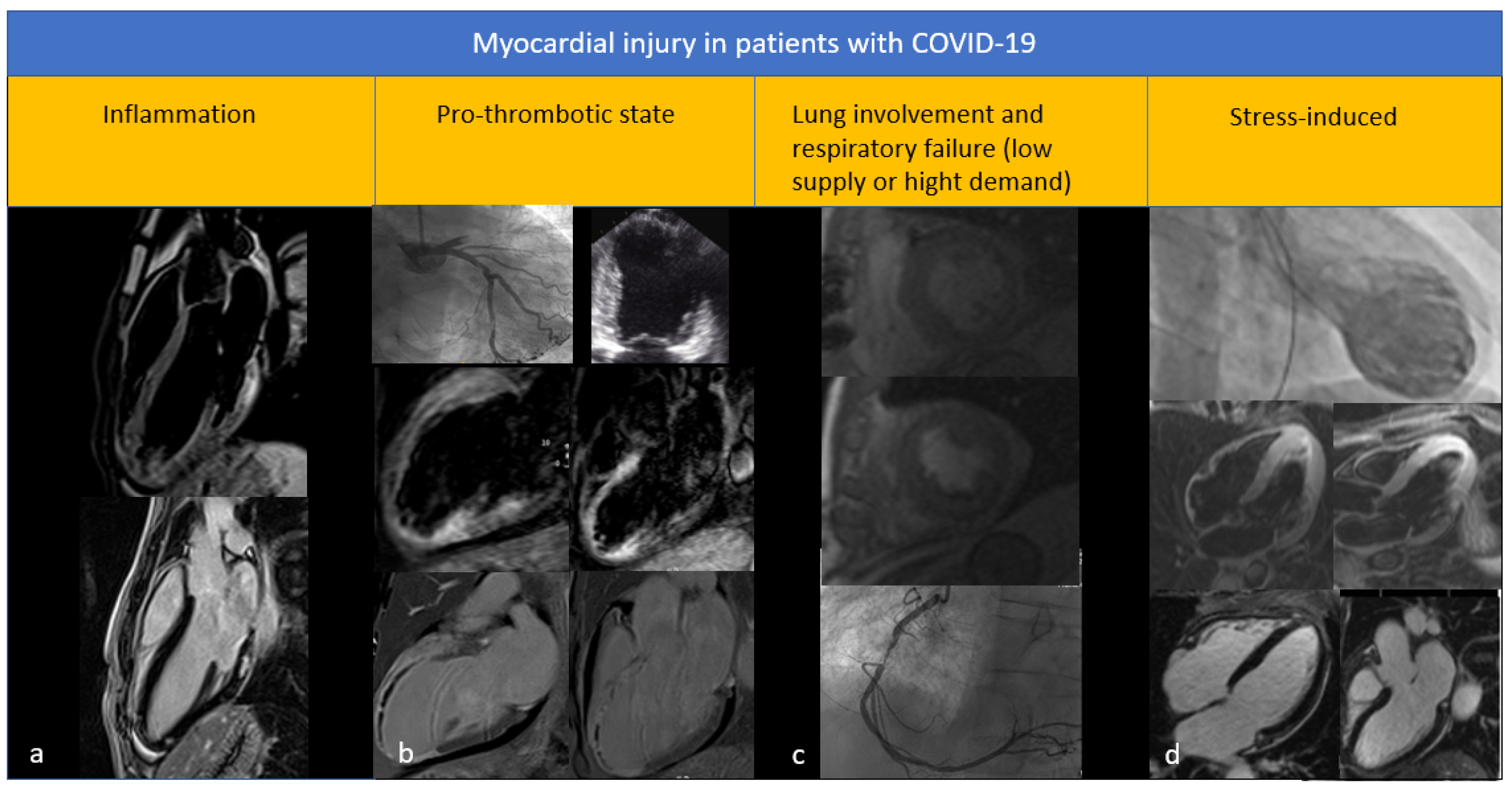
2. Myocardial Damage in COVID-19 Patients
3. The Left Ventricle in COVID-19 Patients
3.1. Types of Left Ventricular Disfunction
3.2. Findings from Speckle Tracking Echocardiography

{kind=link}
{kind=link}
| Study | N Patients | Time to Echo from Admission | GLS Abnormal Value (% of Patients) | Stratification by Comorbidity | Correlation with | ||
|---|---|---|---|---|---|---|---|
| Tn | CPR | PS | |||||
| Kocas et al. [33] | 38 | 1 week | >−18% (28.9%) | + | - | - | NK |
| Ozer et al. [32] | 28 | 1 month | >−18% (37.8%) | + | + | + | NK |
| Baykiz et al. [34] | 75 | 6 months | >−16% | + | - | + | + |
| Li et al. [36] | 218 | average of 24 days | >−21% (83%) | + | + | + | - |
| Hayama et al. [37] | 209 | average of 56 days | >−20% (29.7%) | + | + | NK | NK |
| Bathia et al. [35] | 67 | 1 week | >−18% (91%) | + | - | NK | - |
| Baycan et al. [28] | 100 | 1 day | NK | + | + | - | + |
3.3. Findings from Cardiac Magnetic Resonance
4. The Right Ventricle in COVID-19 Patients
4.1. Characteristics and Importance of Right Ventricular Dysfunction
4.2. Information from Speckle Tracking Echocardiography
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Giustino, G.; Croft, L.B.; Stefanini, G.G.; Bragato, R.; Silbiger, J.J.; Vicenzi, M.; Danilov, T.; Kukar, N.; Shaban, N.; Kini, A.; et al. Characterization of myocardial injury in patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2043–2055. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goerlich, E.; Minhas, A.S.; Mukherjee, M.; Sheikh, F.H.; Gilotra, N.A.; Sharma, G.; Michos, E.D.; Hays, A.G. Multimodality Imaging for Cardiac Evaluation in Patients with COVID-19. Curr. Cardiol. Rep. 2021, 23, 44. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Deng, Q.; Hu, B.; Zhang, Y.; Wang, H.; Zhou, X.; Hu, W.; Cheng, Y.; Yan, J.; Ping, H.; Zhou, Q. Suspected myocardial injury in patients with COVID-19: Evidence from front-line clinical observation in Wuhan, China. Int. J. Cardiol. 2020, 311, 116–121. [Google Scholar] [CrossRef]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353 . [Google Scholar] [CrossRef]
- Dweck, M.R.; Bularga, A.; Hahn, R.T.; Bing, R.; Lee, K.K.; Chapman, A.R.; White, A.; Di Salvo, G.; Sade, L.E.; Pearce, K.; et al. Global evaluation of echocardiography in patients with COVID-19. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Hendren, N.S.; Drazner, M.H.; Bozkurt, B.; Cooper, L.T., Jr. Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome. Circulation 2020, 141, 1903–1914. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.; Degrauwe, S.; Van Delden, C.; Ghadri, J.-R.; Templin, C. Typical takotsubo syndrome triggered by SARS-CoV-2 infection. Eur. Heart J. 2020, 41, 1860. [Google Scholar] [CrossRef] [PubMed]
- Moderato, L.; Monello, A.; Lazzeroni, D.; Binno, S.; Giacalone, R.; Ferraro, S.; Piepoli, M.F.; Villani, G.Q. Sindrome Takotsubo in corso di polmonite da SARS-CoV-2: Una possibile complicanza cardiovascolare. G. Ital. Cardiol. 2020, 21, 417–420. [Google Scholar] [CrossRef]
- Okura, H. Update of takotsubo syndrome in the era of COVID-19. J. Cardiol. 2021, 77, 361–369. [Google Scholar] [CrossRef]
- Hegde, S.; Khan, R.; Zordok, M.; Maysky, M. Characteristics and outcome of patients with COVID-19 complicated by Takotsubo cardiomyopathy: Case series with literature review. Open Heart 2020, 7, e001360. [Google Scholar] [CrossRef]
- Epstein, F.H.; Parrillo, J.E. Pathogenetic Mechanisms of Septic Shock. N. Engl. J. Med. 1993, 328, 1471–1477. [Google Scholar] [CrossRef]
- Van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O.; et al. Recognition and Initial Management of Fulminant Myocarditis: A scientific statement from the American Heart Association. Circulation 2020, 141, e69–e92. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Di Giannuario, G.; Marrazzo, G.; Riegler, L.; Mele, D.; Rizzo, M.; Campana, M.; Gimelli, A.; Khoury, G.; Moreo, A. L’imaging integrato nel percorso del paziente con COVID-19: Dalla diagnosi, al monitoraggio clinico, alla prognosi. G. Ital. Cardiol. 2020, 21, 345–353. [Google Scholar] [CrossRef]
- Mele, D.; Flamigni, F.; Rapezzi, C.; Ferrari, R. Myocarditis in COVID-19 patients: Current problems. Intern. Emerg. Med. 2021, 16, 1123–1129. [Google Scholar] [CrossRef]
- Sala, S.; Peretto, G.; Gramegna, M.; Palmisano, A.; Villatore, A.; Vignale, D.; De Cobelli, F.; Tresoldi, M.; Cappelletti, A.M.; Basso, C.; et al. Acute myocarditis presenting as a reverse Tako-Tsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur. Heart J. 2020, 41, 1861–1862. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Heuvel, F.M.A.V.D.; Vos, J.L.; Koop, Y.; van Dijk, A.P.J.; Duijnhouwer, A.L.; de Mast, Q.; van de Veerdonk, F.L.; Bosch, F.; Kok, B.; Netea, M.G.; et al. Cardiac function in relation to myocardial injury in hospitalised patients with COVID-19. Neth. Heart J. 2020, 28, 410–417. [Google Scholar] [CrossRef]
- Baycan, O.F.; Barman, H.A.; Atici, A.; Tatlisu, A.; Bolen, F.; Ergen, P.; Icten, S.; Gungor, B.; Caliskan, M. Evaluation of biventricular function in patients with COVID-19 using speckle tracking echocardiography. Int. J. Cardiovasc. Imaging 2021, 37, 135–144. [Google Scholar] [CrossRef]
- Chang, W.-T.; Lee, W.-H.; Lee, W.-T.; Chen, P.-S.; Su, Y.-R.; Liu, P.-Y.; Liu, Y.-W.; Tsai, W.-C. Left ventricular global longitudinal strain is independently associated with mortality in septic shock patients. Intensive Care Med. 2015, 41, 1791–1799. [Google Scholar] [CrossRef]
- Goerlich, E.; Gilotra, N.A.; Minhas, A.S.; Bavaro, N.; Hays, A.G.; Cingolani, O.H. Prominent Longitudinal Strain Reduction of Basal Left Ventricular Segments in Patients with Coronavirus Disease-19. J. Card. Fail. 2021, 27, 100–104. [Google Scholar] [CrossRef]
- Stöbe, S.; Richter, S.; Seige, M.; Stehr, S.; Laufs, U.; Hagendorff, A. Echocardiographic characteristics of patients with SARS-CoV-2 infection. Clin. Res. Cardiol. 2020, 109, 1549–1566. [Google Scholar] [CrossRef] [PubMed]
- Özer, S.; Candan, L.; Özyıldız, A.G.; Turan, O.E. Evaluation of left ventricular global functions with speckle tracking echocardiography in patients recovered from COVID-19. Int. J. Cardiovasc. Imaging 2021, 37, 2227–2233. [Google Scholar] [CrossRef] [PubMed]
- Kocas, B.B.; Cetinkal, G.; Ser, O.S.; Kilci, H.; Keskin, K.; Ozcan, S.N.; Verdi, Y.; Zeren, M.I.; Kilickesmez, K. The relation between left ventricular global longitudinal strain and troponin levels in patients hospitalized with COVID-19 pneumonia. Int. J. Cardiovasc. Imaging 2021, 37, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Baykiz, D.; Govdeli, E.A.; Ozer, P.K.; Karaayvaz, E.B.; Catma, Y.; Medetalibeyoglu, A.; Cagatay, A.; Umman, B.; Tukek, T.; Bugra, Z. Evaluation the relationship of left ventricular global longitudinal strain and laboratory parameters in discharged patients with COVID-19: A follow-up study. Int. J. Cardiovasc. Imaging 2021, 37, 2451–2464. [Google Scholar] [CrossRef]
- Bhatia, H.S.; Bui, Q.M.; King, K.; DeMaria, A.; Daniels, L.B. Subclinical left ventricular dysfunction in COVID-19. IJC Heart Vasc. 2021, 34, 100770. [Google Scholar] [CrossRef]
- Li, R.; Wang, H.; Ma, F.; Cui, G.-L.; Peng, L.-Y.; Li, C.-Z.; Zeng, H.-S.; Marian, A.J.; Wang, D.-W. Widespread myocardial dysfunction in COVID-19 patients detected by myocardial strain imaging using 2-D speckle-tracking echocardiography. Acta Pharmacol. Sin. 2021, 42, 1567–1574. [Google Scholar] [CrossRef]
- Hayama, H.; Ide, S.; Moroi, M.; Kitami, Y.; Bekki, N.; Kubota, S.; Uemura, Y.; Hara, H.; Kutsuna, S.; Ohmagari, N.; et al. Elevated high-sensitivity troponin is associated with subclinical cardiac dysfunction in patients recovered from coronavirus disease 2019. Glob. Health Med. 2021, 3, 95–101. [Google Scholar] [CrossRef]
- Jaglan, A.; Roemer, S.; Jan, M.F.; Khandheria, B.K. Myocardial work index: A glimmer of hope in COVID-19. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 228. [Google Scholar] [CrossRef]
- Minhas, A.; A Gilotra, N.; Goerlich, E.; Garibaldi, B.T.; Metkus, T.S.; Sharma, G.; Bavaro, N.; Phillip, S.; Michos, E.D.; Hays, A.G. Abstract 15455: Prevalence of Subclinical Myocardial Dysfunction in Hospitalized Patients with Covid-19 and Association with In-hospital Mortality. Circulation 2020, 142, A15455. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef]
- Schultheiss, H.-P.; Fairweather, D.; Caforio, A.L.P.; Escher, F.; Hershberger, R.; Lipshultz, S.E.; Liu, P.P.; Matsumori, A.; Mazzanti, A.; McMurray, J.; et al. Dilated cardiomyopathy. Nat. Rev. Dis. Prim. 2019, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Habtemicael, Y.G.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Lanzillo, C.; Scatteia, A.; Di Roma, M.; Pontone, G.; et al. Prognostic Value of Repeating Cardiac Magnetic Resonance in Patients with Acute Myocarditis. J. Am. Coll. Cardiol. 2019, 74, 2439–2448. [Google Scholar] [CrossRef] [PubMed]
- Knight, D.S.; Kotecha, T.; Razvi, Y.; Chacko, L.; Brown, J.T.; Jeetley, P.S.; Goldring, J.; Jacobs, M.; Lamb, L.E.; Negus, R.; et al. COVID-19 Myocardial Injury in Survivors. Circulation 2020, 142, 1120–1122. [Google Scholar] [CrossRef] [PubMed]
- Salamanca, J.; Díez-Villanueva, P.; Martínez, P.; Cecconi, A.; de Marcos, B.G.; Reyes, G.; Salas, C.; Segovia, J.; Jiménez-Borreguero, L.J.; Alfonso, F. COVID-19 “Fulminant Myocarditis&rdquo” Successfully Treated with Temporary Mechanical Circulatory Support. JACC Cardiovasc. Imaging 2020, 13, 2457–2459. [Google Scholar] [CrossRef] [PubMed]
- Augusto, J.B.; Johner, N.; Shah, D.; Nordin, S.; Knott, K.D.; Rosmini, S.; Lau, C.; Alfarih, M.; Hughes, R.; Seraphim, A.; et al. The myocardial phenotype of Fabry disease pre-hypertrophy and pre-detectable storage. Eur. Heart J.-Cardiovasc. Imaging 2021, 22, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Pan, C.; Zhang, Z.; Luo, L.; Wu, W.; Jia, T.; Lu, L.; Liu, W.V.; Qin, Y.; Hu, F.; Bs, X.D.; et al. Cardiac T1 and T2 Mapping Showed Myocardial Involvement in Recovered COVID -19 Patients Initially Considered Devoid of Cardiac Damage. J. Magn. Reson. Imaging 2021, 54, 421–428. [Google Scholar] [CrossRef]
- Clark, D.E.; Parikh, A.; Dendy, J.M.; Diamond, A.B.; George-Durrett, K.; Fish, F.A.; Slaughter, J.C.; Fitch, W.; Hughes, S.G.; Soslow, J.H. COVID-19 Myocardial Pathology Evaluation in Athletes with Cardiac Magnetic Resonance (COMPETE CMR). Circulation 2021, 143, 609–612. [Google Scholar] [CrossRef]
- Ojha, V.; Verma, M.; Pandey, N.N.; Mani, A.; Malhi, A.S.; Kumar, S.; Jagia, P.; Roy, A.; Sharma, S. Cardiac Magnetic Resonance Imaging in Coronavirus Disease 2019 (COVID-19). J. Thorac. Imaging 2021, 36, 73–83. [Google Scholar] [CrossRef]
- Wang, H.; Li, R.; Zhou, Z.; Jiang, H.; Yan, Z.; Tao, X.; Li, H.; Xu, L. Cardiac involvement in COVID-19 patients: Mid-term follow up by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 14. [Google Scholar] [CrossRef]
- Fu, H.; Zhang, N.; Zheng, Y.; Jiang, N.; Xu, H.; Xu, R.; Xie, L.; Zhou, Z.; Kang, B.; Li, T.; et al. Risk stratification of cardiac sequelae detected using cardiac magnetic resonance in late convalescence at the six-month follow-up of recovered COVID-19 patients. J. Infect. 2021, 83, 119–145. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, H.; Zhao, R.; Wang, T.; Zhu, Y.; Qian, Y.; Liu, B.; Yu, Y.; Han, Y. Elevated Extracellular Volume Fraction and Reduced Global Longitudinal Strains in Participants Recovered from COVID-19 without Clinical Cardiac Findings. Radiology 2021, 299, E230–E240. [Google Scholar] [CrossRef] [PubMed]
- Himebauch, A.S.; Yehya, N.; Wang, Y.; McGowan, F.X.; Mercer-Rosa, L. New or Persistent Right Ventricular Systolic Dysfunction Is Associated with Worse Outcomes in Pediatric Acute Respiratory Distress Syndrome. Pediatr. Crit. Care Med. 2020, 21, e121–e128. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, C.; Bonizzoli, M.; Cozzolino, M.; Verdi, C.; Cianchi, G.; Batacchi, S.; Franci, A.; Gensini, G.F.; Peris, A. Serial measurements of troponin and echocardiography in patients with moderate-to-severe acute respiratory distress syndrome. J. Crit. Care 2016, 33, 132–136. [Google Scholar] [CrossRef]
- Argulian, E.; Sud, K.; Vogel, B.; Bohra, C.; Garg, V.P.; Talebi, S.; Lerakis, S.; Narula, J. Right Ventricular Dilation in Hospitalized Patients with COVID-19 Infection. JACC Cardiovasc. Imaging 2020, 13, 2459–2461. [Google Scholar] [CrossRef]
- Pagnesi, M.; Baldetti, L.; Beneduce, A.; Calvo, F.; Gramegna, M.; Pazzanese, V.; Ingallina, G.; Napolano, A.; Finazzi, R.; Ruggeri, A.; et al. Pulmonary hypertension and right ventricular involvement in hospitalised patients with COVID-19. Heart 2020, 106, 1324–1331. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Zhu, S.; Xie, Y.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; Wu, C.; et al. Prognostic Value of Right Ventricular Longitudinal Strain in Patients with COVID-19. JACC Cardiovasc. Imaging 2020, 13, 2287–2299. [Google Scholar] [CrossRef]
- Gibson, L.E.; Di Fenza, R.; Lang, M.; Capriles, M.I.; Li, M.D.; Kalpathy-Cramer, J.; Little, B.P.; Arora, P.; Mueller, A.L.; Ichinose, F.; et al. Right Ventricular Strain Is Common in Intubated COVID-19 Patients and Does Not Reflect Severity of Respiratory Illness. J. Intensive Care Med. 2021, 36, 900–909. [Google Scholar] [CrossRef]
- Günay, N.; Demiröz, Ö.; Kahyaoğlu, M.; Başlılar, Ş.; Aydın, M.; Özer, M.Ç.; Ileri, Ç.; Keskin, M.; Bayam, E.; Uyan, C. The effect of moderate and severe COVID-19 pneumonia on short-term right ventricular functions: A prospective observational single pandemic center analysis. Int. J. Cardiovasc. Imaging 2021, 37, 1883–1890. [Google Scholar] [CrossRef]
- Ozer, P.K.; Govdeli, E.A.; Baykiz, D.; Karaayvaz, E.B.; Medetalibeyoglu, A.; Catma, Y.; Elitok, A.; Cagatay, A.; Umman, B.; Oncul, A.; et al. Impairment of right ventricular longitudinal strain associated with severity of pneumonia in patients recovered from COVID-19. Int. J. Cardiovasc. Imaging 2021, 37, 2387–2397. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cecchetto, A.; Nistri, S.; Baroni, G.; Torreggiani, G.; Aruta, P.; Pergola, V.; Baritussio, A.; Previtero, M.; Palermo, C.; Iliceto, S.; et al. Role of Cardiac Imaging Modalities in the Evaluation of COVID-19-Related Cardiomyopathy. Diagnostics 2022, 12, 896. https://doi.org/10.3390/diagnostics12040896
Cecchetto A, Nistri S, Baroni G, Torreggiani G, Aruta P, Pergola V, Baritussio A, Previtero M, Palermo C, Iliceto S, et al. Role of Cardiac Imaging Modalities in the Evaluation of COVID-19-Related Cardiomyopathy. Diagnostics. 2022; 12(4):896. https://doi.org/10.3390/diagnostics12040896
Chicago/Turabian StyleCecchetto, Antonella, Stefano Nistri, Giulia Baroni, Gianpaolo Torreggiani, Patrizia Aruta, Valeria Pergola, Anna Baritussio, Marco Previtero, Chiara Palermo, Sabino Iliceto, and et al. 2022. "Role of Cardiac Imaging Modalities in the Evaluation of COVID-19-Related Cardiomyopathy" Diagnostics 12, no. 4: 896. https://doi.org/10.3390/diagnostics12040896