
Medical Radiation Exposure Reduction in PET via Super-Resolution Deep Learning Model

 , , and
, , and
Abstract
:1. Introduction
2. Related Works
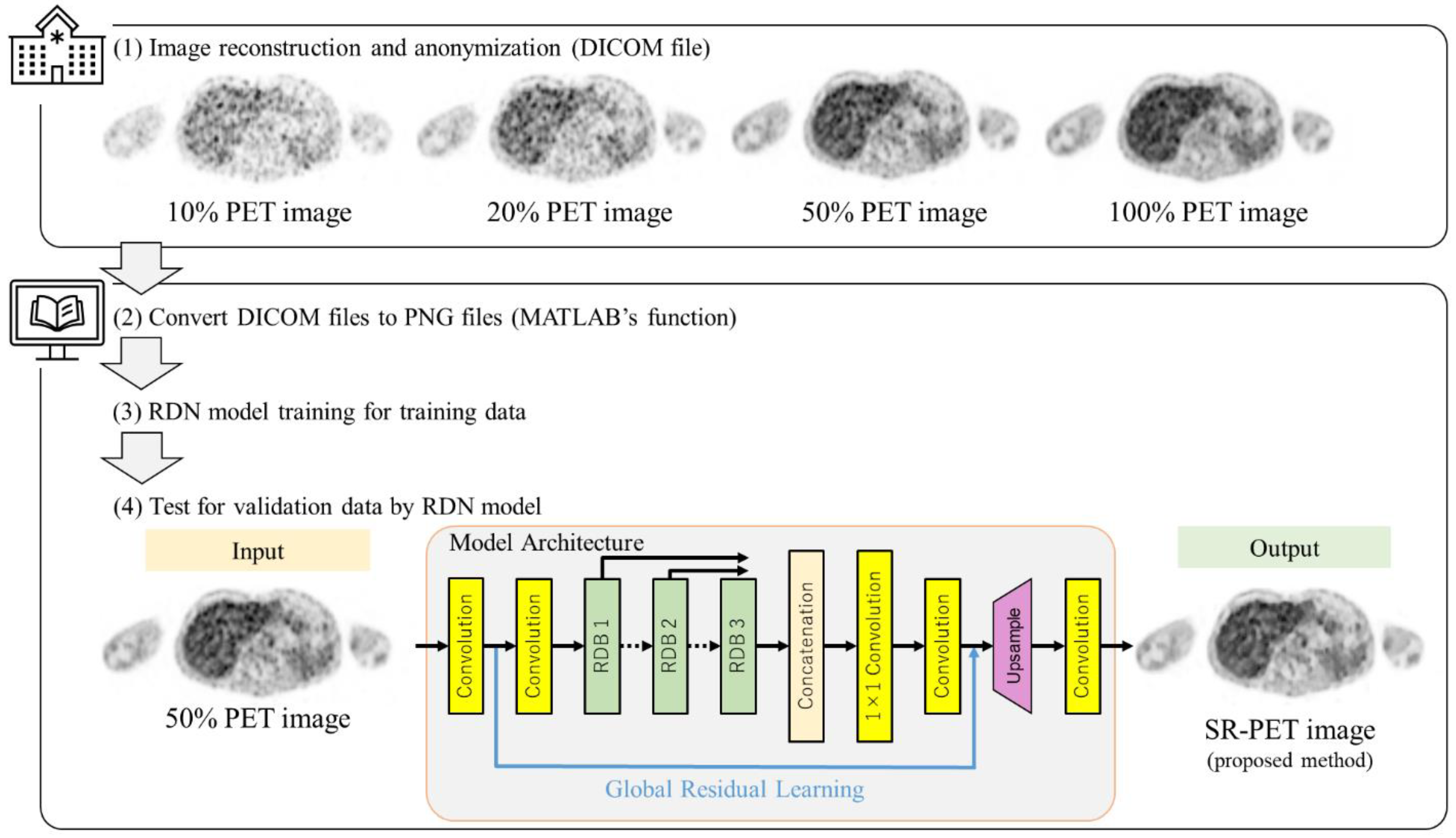
3. Materials and Methods
3.1. Patients and Image Acquisition
3.2. Super Resolution
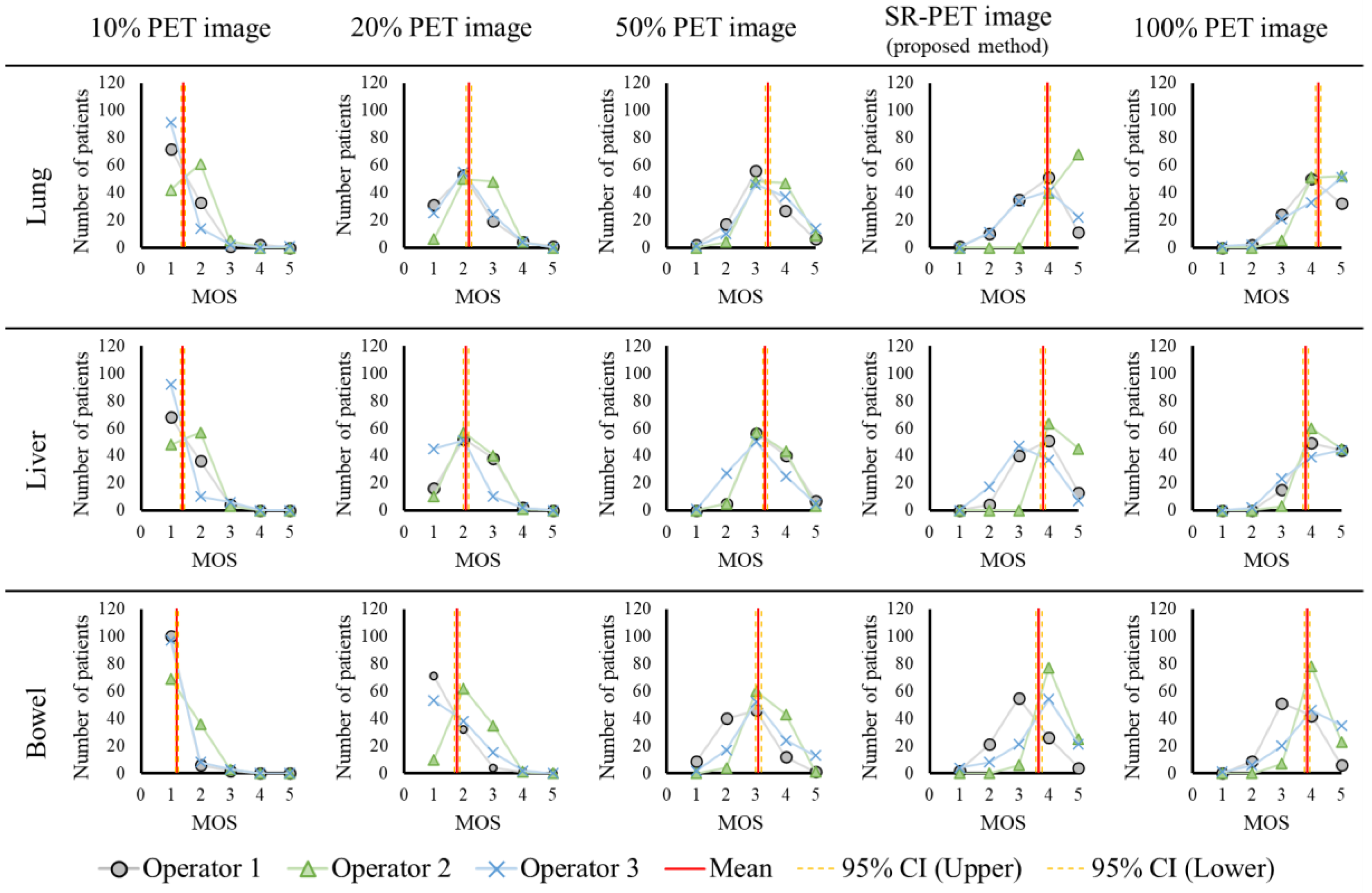
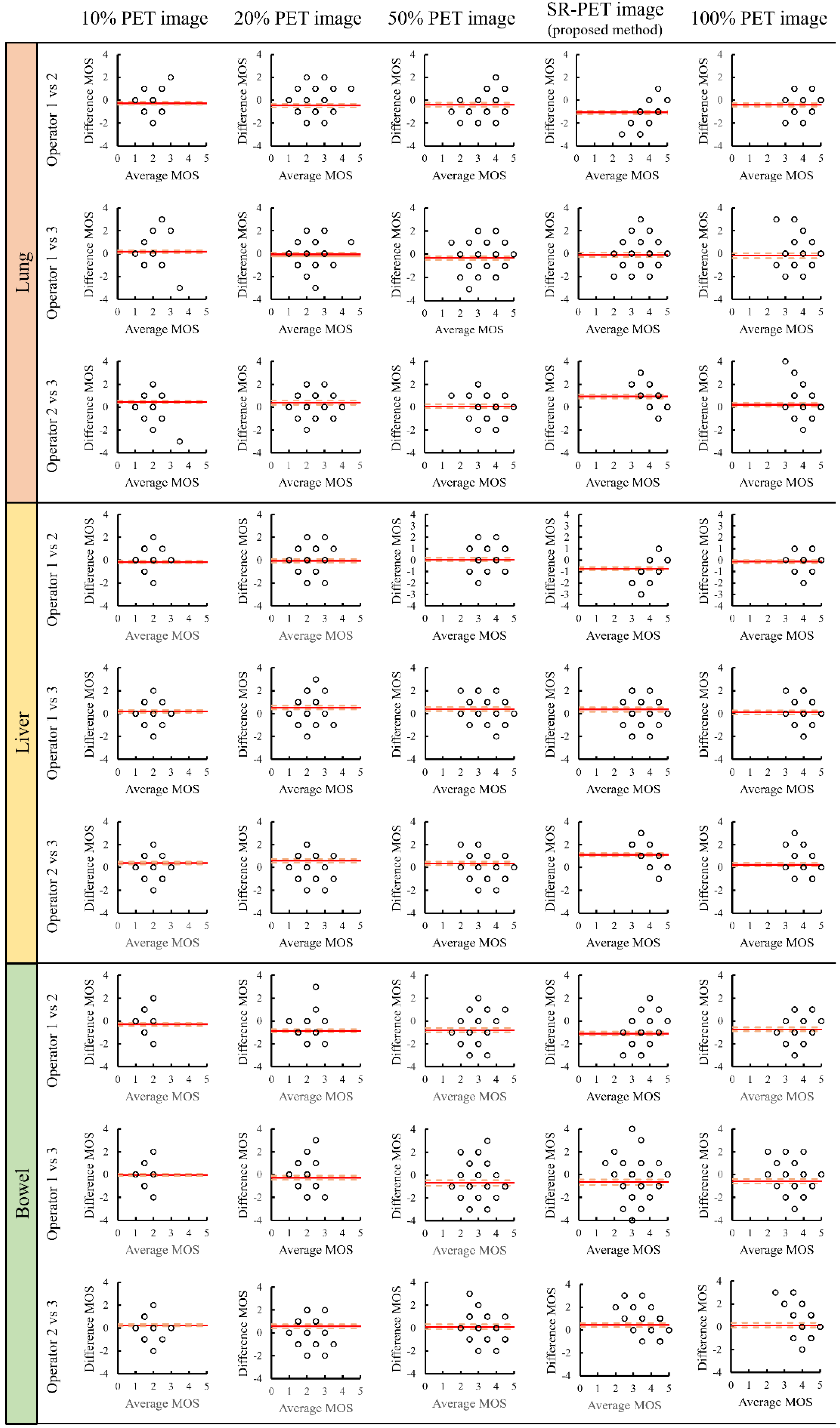
3.3. Evaluation
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, C.; Loy, C.C.; He, K.; Tang, X. Learning a Deep Convolutional Network for Image Super-Resolution. Cham 2014, 8692, 184–199. [Google Scholar]
- Timofte, R.; Agustsson, E.; Gool, L.V.; Yang, M.-H.; Zhang, L.; Lim, B.; Son, S.; Kim, H.; Nah, S.; Lee, K.M.; et al. NTIRE 2017 Challenge on Single Image Super-Resolution: Methods and Results. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 1110–1121. [Google Scholar] [CrossRef]
- Agustsson, E.; Timofte, R. NTIRE 2017 Challenge on Single Image Super-Resolution: Dataset and Study. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 1122–1131. [Google Scholar] [CrossRef]
- Timofte, R.; Gu, S.; Wu, J.; Gool, L.V.; Zhang, L.; Yang, M.H.; Haris, M.; Shakhnarovich, G.; Ukita, N.; Hu, S.; et al. NTIRE 2018 Challenge on Single Image Super-Resolution: Methods and Results. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Salt Lake City, UT, USA, 18–22 June 2018; pp. 965–976. [Google Scholar]
- Cai, J.; Gu, S.; Radu, T.; Lei, Z. NTIRE 2019 Challenge on Real Image Super-Resolution: Methods and Results. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR) Workshops 2019, Long Beach, CA, USA, 15–20 June 2019. [Google Scholar]
- Andreas, L.; Martin, D.; Radu, T. NTIRE 2020 Challenge on Real-World Image Super-Resolution: Methods and Results. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR) Workshops 2020, Seattle, WA, USA, 14–19 June 2020. [Google Scholar]
- Browse State-of-the-Art. Available online: https://paperswithcode.com/sota (accessed on 1 April 2020).
- Hirata, K.; Sugimori, H.; Fujima, N.; Toyonaga, T.; Kudo, K. Artificial intelligence for nuclear medicine in oncology. Ann. Nucl. Med. 2022, 36, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Farwell, M.D.; Pryma, D.A.; Mankoff, D.A. PET/CT imaging in cancer: Current applications and future directions. Cancer 2014, 120, 3433–3445. [Google Scholar] [CrossRef] [PubMed]
- Sotoudeh, H.; Sharma, A.; Fowler, K.J.; McConathy, J.; Dehdashti, F. Clinical application of PET/MRI in oncology. J. Magn. Reson. Imaging 2016, 44, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Law, M.W.-M.; Khong, P.-L. Whole-Body PET/CT Scanning: Estimation of Radiation Dose and Cancer Risk. Radiology 2009, 251, 166–174. [Google Scholar] [CrossRef]
- Grant, A.M.; Deller, T.W.; Khalighi, M.M.; Maramraju, S.H.; Delso, G.; Levin, C.S. NEMA NU 2-2012 performance studies for the SiPM-based ToF-PET component of the GE SIGNA PET/MR system. Med. Phys. 2016, 43, 2334–2343. [Google Scholar] [CrossRef] [Green Version]
- Hsu, D.F.C.; Ilan, E.; Peterson, W.T.; Uribe, J.; Lubberink, M.; Levin, C.S. Studies of a Next-Generation Silicon-Photomultiplier-Based Time-of-Flight PET/CT System. J. Nucl. Med. 2017, 58, 1511–1518. [Google Scholar] [CrossRef]
- van Sluis, J.; de Jong, J.; Schaar, J.; Noordzij, W.; van Snick, P.; Dierckx, R.; Borra, R.; Willemsen, A.; Boellaard, R. Performance Characteristics of the Digital Biograph Vision PET/CT System. J. Nucl. Med. 2019, 60, 1031–1036. [Google Scholar] [CrossRef]
- Rausch, I.; Ruiz, A.; Valverde-Pascual, I.; Cal-Gonzalez, J.; Beyer, T.; Carrio, I. Performance Evaluation of the Vereos PET/CT System According to the NEMA NU2-2012 Standard. J. Nucl. Med. 2019, 60, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, P.A.; Houdu, B.; Cesaire, L.; Nakouri, I.; De Pontville, M.; Lasnon, C.; Aide, N. Revisiting detection of in-transit metastases in melanoma patients using digital (18) F-FDG PET/CT with small-voxel reconstruction. Ann. Nucl. Med. 2021, 35, 669–679. [Google Scholar] [CrossRef]
- Alberts, I.; Sachpekidis, C.; Prenosil, G.; Viscione, M.; Bohn, K.P.; Mingels, C.; Shi, K.; Ashar-Oromieh, A.; Rominger, A. Digital PET/CT allows for shorter acquisition protocols or reduced radiopharmaceutical dose in [(18).F]-FDG PET/CT. Ann. Nucl. Med. 2021, 35, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Japan Network for Research and Information on Medical Exposure (J-RIME), National Diagnostic Reference Levels in Japan (2020)-Japan DRLs 2020. Available online: http://www.radher.jp/J-RIME/report/DRL2020_Engver.pdf (accessed on 20 April 2020).
- Abe, K.; Hosono, M.; Igarashi, T.; Iimori, T.; Ishiguro, M.; Ito, T.; Nagahata, T.; Tsushima, H.; Watanabe, H. The 2020 national diagnostic reference levels for nuclear medicine in Japan. Ann. Nucl. Med. 2020, 34, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Karakatsanis, N.A.; Fokou, E.; Tsoumpas, C. Dosage optimization in positron emission tomography: State-of-the-art methods and future prospects. Am. J. Nucl. Med. Mol. Imaging. 2015, 5, 527–547. [Google Scholar] [PubMed]
- Queiroz, M.A.; Delso, G.; Wollenweber, S.; Deller, T.; Zeimpekis, K.; Huellner, M.; de Galiza Barbosa, F.; von Schulthess, G.; Veit-Haibach, P. Dose Optimization in TOF-PET/MR Compared to TOF-PET/CT. PLoS ONE 2015, 10, e0128842. [Google Scholar] [CrossRef] [Green Version]
- Sekine, T.; Delso, G.; Zeimpekis, K.G.; de Galiza Barbosa, F.; Ter Voert, E.; Huellner, M.; Veit-Haibach, P. Reduction of (18)F-FDG Dose in Clinical PET/MR Imaging by Using Silicon Photomultiplier Detectors. Radiology 2018, 286, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Dilsizian, V.; Bacharach, S.L.; Beanlands, R.S.; Bergmann, S.R.; Delbeke, D.; Dorbala, S.; Gropler, R.J.; Knuuti, J.; Schelbert, H.R.; Travin, M.I. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J. Nucl. Cardiol. 2016, 23, 1187–1226. [Google Scholar] [CrossRef] [Green Version]
- Ooi, Y.K.; Ibrahim, H. Deep Learning Algorithms for Single Image Super-Resolution: A Systematic Review. Electronics 2021, 10, 867. [Google Scholar] [CrossRef]
- Ledig, C.; Theis, L.; Huszar, F.; Caballero, J.; Cunningham, A.; Acosta, A.; Aitken, A.; Tejani, A.; Totz, J.; Wang, Z.; et al. Photo-Realistic Single Image Super-Resolution Using a Generative Adversarial Network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 4681–4690. [Google Scholar]
- Lei, Y.; Dong, X.; Wang, T.; Higgins, K.; Liu, T.; Curran, W.J.; Mao, H.; Nye, J.A.; Yang, X. Whole-body PET estimation from low count statistics using cycle-consistent generative adversarial networks. Phys. Med. Biol. 2019, 64, 215017. [Google Scholar] [CrossRef]
- Ouyang, J.; Chen, K.T.; Gong, E.; Pauly, J.; Zaharchuk, G. Ultra-low-dose PET reconstruction using generative adversarial network with feature matching and task-specific perceptual loss. Med. Phys. 2019, 46, 3555–3564. [Google Scholar] [CrossRef]
- Radiation Dose to Patients from Radiopharmaceuticals (Addendum to ICRP Publication 53). ICRP Publication 80. Ann. ICRP 1998, 28, 1–143. [Google Scholar]
- Zhang, Y.; Tian, Y.; Kong, Y.; Zhong, B.; Fu, Y. Residual Dense Network for Image Super-Resolution. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018. [Google Scholar]
- Vabalas, A.; Gowen, E.; Poliakoff, E.; Casson, A.J. Machine learning algorithm validation with a limited sample size. PLoS ONE 2019, 14, e0224365. [Google Scholar] [CrossRef] [PubMed]
- Hore, A.; Ziou, D. Image quality metrics: PSNR vs. SSIM. In Proceedings of the 2010 20th International Conference on Pattern Recognition, Istanbul, Turkey, 23–26 August 2010; pp. 2366–2369. [Google Scholar]
- Wang, Z.; Bovik, A.C.; Sheikh, H.R.; Simoncelli, E.P. Image quality assessment: From error visibility to structural similarity. IEEE Trans. Image Process. 2004, 13, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 5-Point Likert Scale. Handbook of Disease Burdens and Quality of Life Measures; Preedy, V.R., Watson, R.R., Eds.; Springer New York: New York, NY, USA, 2010; p. 4288. [Google Scholar]
- Müller, R.; Büttner, P. A critical discussion of intraclass correlation coefficients. Stat. Med. 1994, 13, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleiss, J.L.; Cohen, J. The Equivalence of Weighted Kappa and the Intraclass Correlation Coefficient as Measures of Reliability. Educ. Psychol. Meas. 1973, 33, 613–619. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.J.; Baratto, L.; Hawk, K.E.; Theruvath, A.J.; Pribnow, A.; Thakor, A.S.; Gatidis, S.; Lu, R.; Gummidipundi, S.E.; Garcia-Diaz, J.; et al. Artificial intelligence enables whole-body positron emission tomography scans with minimal radiation exposure. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2771–2781. [Google Scholar] [CrossRef]
- Fahlstrom, M.; Appel, L.; Kumlien, E.; Danfors, T.; Engstrom, M.; Wikstrom, J.; Antoni, G.; Larsson, E.M.; Lubberink, M. Evaluation of Arterial Spin Labeling MRI-Comparison with (15) O-Water PET on an Integrated PET/MR Scanner. Diagnostics 2021, 11, 821. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Hicks, R.J.; Siva, S.; Hofman, M.S. PET/CT Lung Ventilation and Perfusion Scanning using Galligas and Gallium-68-MAA. Semin. Nucl. Med. 2019, 49, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Sim, K.S.; Sammani, F. Deep convolutional networks for magnification of DICOM brain images. Int. J. Innov. Comput. Inf. Control. 2019, 15, 725–739. [Google Scholar]
- Hirata, K.; Manabe, O.; Magota, K.; Furuya, S.; Shiga, T.; Kudo, K. A Preliminary Study to Use SUVmax of FDG PET-CT as an Identifier of Lesion for Artificial Intelligence. Front Med. Lausanne 2021, 8, 647562. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Kobayashi, K.; Wong, K.P.; Manabe, O.; Surmak, A.; Tamaki, N.; Huang, S.C. A semi-automated technique determining the liver standardized uptake value reference for tumor delineation in FDG PET-CT. PLoS ONE 2014, 9, e105682. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median | Range | |||
|---|---|---|---|---|
| Age | (years) | 66.5 | 20.0 | 86.0 |
| BMI | (kg/m2) | 22.4 | 12.3 | 34.7 |
| Weight | (kg) | 57.6 | 30.0 | 91.3 |
| Height | (m) | 1.60 | 1.40 | 1.78 |
| Injection dose | (MBq) | 258.7 | 124.0 | 400.7 |
| Emission time | (s) | 90 | 90 | 180 |
| Uptake time | (min) | 63 | 54 | 118 |
| Exposure dose from PET | (mSv) | 4.9 | 2.3 | 7.6 |
| Number of images per patient | 241 | 191 | 291 | |
| 10% PET Image Set | 20% PET Image Set | 50% PET Image Set | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (95% CI) | Mean | (95% CI) | Mean | (95% CI) | |||||
| MOS | Lung | 1.41 | 1.35 | 1.48 | 2.17 | 2.09 | 2.26 | 3.41 | 3.32 | 3.49 |
| Liver | 1.40 | 1.34 | 1.46 | 2.08 | 2.00 | 2.16 | 3.31 | 3.22 | 3.39 | |
| Bowel | 1.20 | 1.15 | 1.25 | 1.78 | 1.69 | 1.86 | 3.08 | 2.99 | 3.17 | |
| ICC (3,3) | Lung | 0.48 | 0.28 | 0.63 | 0.53 | 0.36 | 0.67 | 0.62 | 0.48 | 0.73 |
| Liver | 0.55 | 0.38 | 0.68 | 0.43 | 0.21 | 0.59 | 0.56 | 0.39 | 0.69 | |
| Bowel | 0.06 | −0.29 | 0.33 | 0.35 | 0.10 | 0.54 | 0.14 | −0.18 | 0.39 | |
| SR-PET Image (Proposed Method) | 100% PET Image Set | |||||||||
| Mean | (95% CI) | Mean | (95% CI) | |||||||
| MOS | Lung | 3.96 | 3.87 | 4.05 | 4.23 | 4.15 | 4.31 | |||
| Liver | 3.80 | 3.71 | 3.89 | 4.27 | 4.20 | 4.35 | ||||
| Bowel | 3.67 | 3.57 | 3.77 | 3.85 | 3.77 | 3.94 | ||||
| ICC (3,3) | Lung | 0.48 | 0.28 | 0.63 | 0.31 | 0.06 | 0.51 | |||
| Liver | 0.43 | 0.22 | 0.60 | 0.55 | 0.38 | 0.68 | ||||
| Bowel | 0.32 | 0.07 | 0.52 | 0.19 | −0.12 | 0.42 | ||||
| Operator | 10% PET Image | 20% PET Image | 50% PET Image | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| d | k | d | k | d | k | ||||||||
| Mean | (95% CI) | Mean | (95% CI) | Mean | (95% CI) | ||||||||
| 1 vs. 2 | Lung | −0.28 | −0.42 | −0.14 | 0.96 | −0.47 | −0.64 | −0.30 | 0.94 −0.40 | −0.57 | −0.23 | 0.94 | |
| Liver | −0.18 | −0.31 | −0.05 | 0.97 | −0.06 | −0.22 | 0.11 | 0.95 | 0.05 | −0.11 | 0.20 | 0.96 | |
| Bowel | −0.30 | −0.43 | −0.17 | 0.97 | −0.85 | −0.99 | −0.71 | 0.92 −0.79 | −0.97 | −0.61 | 0.91 | ||
| 1 vs. 3 | Lung | 0.18 | 0.04 | 0.31 | 0.97 | −0.07 | −0.26 | 0.11 | 0.94 −0.32 | −0.50 | −0.15 | 0.94 | |
| Liver | 0.20 | 0.08 | 0.32 | 0.97 | 0.53 | 0.36 | 0.69 | 0.94 | 0.40 | 0.22 | 0.57 | 0.94 | |
| Bowel | −0.04 | −0.14 | 0.06 | 0.98 | −0.29 | −0.47 | −0.10 | 0.94 −0.68 | −0.91 | −0.44 | 0.88 | ||
| 2 vs. 3 | Lung | 0.45 | 0.32 | 0.59 | 0.96 | 0.40 | 0.23 | 0.57 | 0.94 | 0.07 | −0.10 | 0.25 | 0.95 |
| Liver | 0.38 | 0.26 | 0.50 | 0.96 | 0.58 | 0.41 | 0.76 | 0.93 | 0.35 | 0.19 | 0.51 | 0.95 | |
| Bowel | 0.26 | 0.14 | 0.38 | 0.97 | 0.56 | 0.38 | 0.75 | 0.92 | 0.11 | −0.10 | 0.32 | 0.92 | |
| Operator | SR-PET Image (Proposed Method) | 100% PET Image | |||||||||||
| d | k | d | k | ||||||||||
| Mean | (95% CI) | Mean | (95% CI) | ||||||||||
| 1 vs. 2 | Lung | −1.06 | −1.22 | −0.91 | 0.86 | −0.40 | −0.56 | −0.24 | 0.92 | ||||
| Liver | −0.74 | −0.89 | −0.59 | 0.93 | −0.12 | −0.26 | 0.01 | 0.97 | |||||
| Bowel | −1.09 | −1.27 | −0.92 | 0.87 | −0.73 | −0.89 | −0.57 | 0.92 | |||||
| 1 vs. 3 | Lung | −0.12 | −0.32 | 0.08 | 0.93 | −0.18 | −0.39 | 0.04 | 0.92 | ||||
| Liver | 0.36 | 0.17 | 0.56 | 0.93 | 0.11 | −0.06 | 0.28 | 0.95 | |||||
| Bowel | −0.66 | −0.89 | −0.42 | 0.88 | −0.58 | −0.79 | −0.38 | 0.91 | |||||
| 2 vs. 3 | Lung | 0.94 | 0.76 | 1.13 | 0.89 | 0.22 | 0.03 | 0.41 | 0.94 | ||||
| Liver | 1.10 | 0.95 | 1.26 | 0.88 | 0.23 | 0.07 | 0.40 | 0.95 | |||||
| Bowel | 0.44 | 0.25 | 0.62 | 0.93 | 0.15 | −0.06 | 0.35 | 0.93 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimura, T.; Hasegawa, A.; Kogame, S.; Magota, K.; Kimura, R.; Watanabe, S.; Hirata, K.; Sugimori, H. Medical Radiation Exposure Reduction in PET via Super-Resolution Deep Learning Model. Diagnostics 2022, 12, 872. https://doi.org/10.3390/diagnostics12040872
Yoshimura T, Hasegawa A, Kogame S, Magota K, Kimura R, Watanabe S, Hirata K, Sugimori H. Medical Radiation Exposure Reduction in PET via Super-Resolution Deep Learning Model. Diagnostics. 2022; 12(4):872. https://doi.org/10.3390/diagnostics12040872
Chicago/Turabian StyleYoshimura, Takaaki, Atsushi Hasegawa, Shoki Kogame, Keiichi Magota, Rina Kimura, Shiro Watanabe, Kenji Hirata, and Hiroyuki Sugimori. 2022. "Medical Radiation Exposure Reduction in PET via Super-Resolution Deep Learning Model" Diagnostics 12, no. 4: 872. https://doi.org/10.3390/diagnostics12040872