
A Literature Review on the Use of Artificial Intelligence for the Diagnosis of COVID-19 on CT and Chest X-ray




Abstract
:1. Introduction
2. Materials and Methods
- Clinical relevance uncertain.
- Potentially clinically relevant but not evaluated against a relevant comparator and lacks independent testing.
- Potentially clinically relevant and has demonstrated value against a relevant comparator but lacks independent testing.
- Potentially clinically relevant and has demonstrated value against a relevant comparator and has been independently tested.
- 1–4 fulfilled and ready for implementation.

{kind=link}
{kind=link}
| Lead Author | Year | Country | Study Type | Aim | Dataset | Reference Standard | Comparator | Validation | External Testing | Main Findings | CRS | Funding |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [17] | 2020 | United States of America | Case control | Detection of COVID-19 from X-ray | Training: 103 COVID-19 images (GitHub COVID image dataset), 500 non-COVID but pathological, 500 normal (Kaggle RSNA Pneumonia Detection Challenge dataset). Validation: 10 COVID-19, 10 pneumonia, 10 normal (Veteran’s administration) | X-ray pre-annotated by Radiographer | No | Cross-validation | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from Chest X-ray. | 2 | Not disclosed |
| [7] | 2020 | United States of America | Case control | Detection of COVID-19 from X-ray | Training: 4698, Validation 523, Testing 580. 269 of the images COVID-19 (GitHub COVID image dataset), 3949 non-COVID pneumonia, 1583 normal. | X-ray pre-annotated by Radiographer | No | K-fold cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | No external funding |
| [18] | 2020 | Israel | Retrospective | Detection of COVID-19 from X-ray | Training: 2076 Testing: 350 | X-ray annotated by Radiographer and positive RT-PCR test. | No | Cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from a portable chest X-ray. | 2 | Not disclosed |
| [19] | 2020 | United States of America | Case control | Detection of COVID-19 from X-ray | Training: 6324, Validation: 1574, Test 1970. 34% of images healthy, 28% non-COVID viral, 27% bacterial, 5% COVID-19, 4% TB. | X-ray pre-annotated by Radiographer | No | Cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | No external funding |
| [20] | 2020 | United States of America | Retrospective | Detection of COVID-19 from X-ray | COVID = 455 (Cohen, 2020) Normal = 532 Bacterial pneumonia = 492 Viral non-COVID pneumonia = 552 (Kaggle RSNA Pneumonia Detection Challenge dataset) Split 75 training 25 validation | X-ray annotated by Radiographer | No | Epoch K-fold cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from a portable chest X-ray. | 2 | No external funding |
| [10] | 2020 | Bangladesh | Case control | Detection of COVID-19 from X-ray | Training: 17,749, of which 232 COVID-19. Validation: 1501, of which 51 COVID-19 positive. Dataset (GitHub Dr Cohen, RSNA pneumonia detection Kaggle, COVIDx). | X-ray pre-annotated by Radiographer | No | K-fold cross-validation (10-fold). | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | No external funding |
| [21] | 2020 | United States of America | Retrospective | Detection of COVID-19 from X-ray | Training and Testing split 75:25 randomly. In total: 455 = COVID-19 positive (GitHub Dr Cohen, Kaggle). 532 = Normal. 492 = Bacterial pneumonia. 552 = Non-COVID viral pneumonia. | X-ray pre-annotated by Radiographer and/or a positive RT-PCR test. | No | K-fold cross-validation (5-fold). | No | Machine-learning algorithm can diagnose cases of COVID-19 from a portable chest X-ray. | 2 | No external funding |
| [22] | 2020 | Brazil | Case control | Detection of COVID-19 from X-ray | Training: 5715 Validation: 653 6309 images in total. Non-COVID (Kaggle RSNA Pneumonia Detection Challenge dataset) COVID-19 (25 GitHub Dr Cohen), 180 Societa Italiana di Radiologia Medica, 248 Peshmerga Hospital Erbil. | Positive RT-PCR. | No | K-fold Cross-validation (10-fold) | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray and a full clinical history/examination. | 2 | No external funding |
| [23] | 2020 | Turkey | Case control | Detection of COVID-19 from X-ray | Training: 80% Validation: 20% 125 COVID-19 (GitHub Dr Cohen), 500 normal, 500 pneumonias (chestX-ray8) | X-ray in recovered patients, pre-annotated by Radiographer. | No | K-fold Cross-validation (5-fold) | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | Not disclosed |
| [8] | 2020 | Japan | Case control | Detection of COVID-19 from X-ray | Training: 410 COVID-19 (GitHub, Dr Cohen), 500 non-COVID (NIH, ChexPert) Validation: 62 COVID-19, | X-ray pre-annotated by Radiographer | No | K-fold Cross-validation (10-fold) | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | No external funding |
| [24] | 2020 | United States of America | Case control | Detection of COVID-19 from X-ray | Training: 84 COVID-19 (Radiopaedia, Societa Italiana di Radiologia Medica, GitHub Dr Cohen), 83 Normal (Mooney et al.). Testing: 25 COVID-19, 25 Normal. Validation: 11 COVID-19, 11 Normal. | X-ray pre- annotated by Radiographer. | No | Cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest X-ray. | 2 | Not disclosed |
| Lead Author | Year | Country | Study Type | Aim | Dataset | Reference Standard | Comparator | Validation | External Testing | Main Findings | CRS | Funding |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [25] | 2020 | United States of America | Case control | Detection of COVID-19 from chest CT, by discriminating between Ground Glass Opacities in COVID-19 and Milliary Tuberculosis. | 606 COVID-19 303 Normal (datasets not named) Tested an external dataset: 112 images. | CT slides pre-annotated by Radiographer | No | Cross-validation | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | Veteran Affairs Research Career Scientist Award, VA COVID Rapid Response Support, University of South Florida Strategic Investment Program Fund, Department of Health, Simons Foundation, Microsoft and Google. |
| [26] | 2020 | China | Case control | Detection of COVID-19 from chest CT. | Training: 1210 COVID-19, 1985 Non-COVID. Testing: 303 COVID-19, 495 Non-COVID. All images from CC-CCII (China Consortium of chest CT Image). | CT slides pre- annotated by Radiographer | No | Epoch (200) cross-validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | Not disclosed |
| [27] | 2020 | India | Case control | Detection of COVID-19 from chest CT. | Training: 1984 Testing: 497 2482 CT scans, 1252 COVID-19 (Kaggle—Eduardo), 1230 for other pulmonary disease | CT slides pre-annotated by Radiographer | No | Epoch (30) Cross validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | No external funding |
| [9] | 2021 (newest version) | Iran | Case control | Detection of COVID-19 from chest CT. | Training: 3023 Non-COVID, 1773 COVID-19. Validation: 336 Non-COVID, 190 COVID-19. Testing: 744 Non-COVID, 3081 COVID-19. | CT slides pre-annotated by Radiographer, confirmed by 2 pulmonologists, correct clinical presentation, positive RT-PCR report. | Yes, 4 experienced radiologists. | Cross validation | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 4 | No external funding |
| [28] | 2020 | China | Case control | Detection of COVID-19 from chest CT. | Training: 499 COVID-19 Validation: 131 COVID-19 | CT slides annotated by Radiographer | No | (100 epoch’s) cross validation. | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | No external funding. |
| [29] | 2020 | United States of America | Case control | Detection of COVID-19 from chest CT. | Training: 657 COVID-19, 2628 Non-COVID.Validation: 120 COVID-19, 477 Non-COVID. Test: 266 COVID-19, 1064 Non-COVID. Mixed data obtained from GitHub and private Indian Hospital. | CT slides annotated based off RT-PCR reporting. | No | (50 epoch’s) cross validation | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | Not disclosed |
| [30] | 2020 | China | Case control | Detection of COVID-19 from chest CT. | Training: 642 COVID-19, 674 Non-COVID. Validation: 124 COVID-19, 181 Non-COVID. Test: 154 COVID-19: 218 Non-COVID. | CT slides pre-annotated by 2 Radiographers (with 30+ years experience) | Yes, 8 radiologists (4 from COVID-19 hospitals, 4 from non-covid hospitals). | Cross Validation | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 4 | Not disclosed |
| [31] | 2020 | Belgium | Case Cotnrol | Detection of COVID-19 from chest CT. | Training: 80% Testing: 20% (CHU Sart-Tilman, CHU Notre Dame des Bruyeres). | CT slides annotated based off RT-PCR reporting | No (restrospectively assessed radiologists performance but not simultaneously with the algorithm). | K-Fold cross-validation (10-fold). | No | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | Interreg V-A Euregio Meuse-Rhine, ERC grant, European Marie Curie Grant. |
| [32] | 2020 | South Korea | Case Control | Detection of COVID-10 from chest CT. | Training: 1194 COVID-19 (Wonkwang Hospital, Chonnam Hospital, Societa Italiana di Radiologia Medica), 2799 Non-COVID (inc. pneumonia, normal lung, lung cancer, non-pneumonia pathology—all from Wonkwang Hospital) External testing: 264 COVID-19(images of COVID-19 from recently published papers) | CT slides pre-annotated by Radiographer | No | K-Fold cross-validation (5-fold). | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | National Research Foundation of Korea, Ministry of Science, ICT and Future Planning via Basic Science Research Program. |
| [33] | 2020 | United States of America | Case Control | Detection of COVID-19 from chest CT. | Training: 526 COVID-19, 533 Non-COVID Validation: 177 COVID-19, 151 Non-COVID. Testing: 326 COVID-19, 1011 N0n-COVID.COVID-19 data from single lefts: Hubei, 2 lefts in Milan, Tokyo, Syracuse. Non-COVID data: Lung image database consortium, Syracuse, National institute of health USA. | CT slides annotated based off RT-PCR reporting | No | Cross validation | Yes | Machine-learning algorithm can diagnose cases of COVID-19 from chest CT. | 2 | NIH Centre for Intervential Oncology, Intramural Research Program of the National Institutes of Health and the NIH Intramural Targeted Anti-COVID-19 Program. |
| [34] | 2020 | United States of America. | Case Control | Detection of COVID-19 from chest CT. | Training: 242 COVID-19, 292 Non-COVID. Tuning: 43 COVID-19, 49 Non-COVID. Testing: 134 COVID-19, 145 Non-COVID. All data obtained from 18 medical lefts in 12 provinces in China. | CT slides annotated based off 2 × RT-PCR reporting. | Yes, 2 radiologists. | Cross Validation | No | Demographical information (travel, exposure, patient age, sex, WBC count and symptoms) combined with output from machine-learning algorithm can diagnose cases of COVID-19. | 3 | US NIH grant. |
| [35] | 2020 | China | Retrospective | Detection of COVID-19 from chest CT. | Training: 1294 COVID-19, 1969 Non-COVID. Testing: 1235 COVID-19, 1964 Non-COVID. External testing: 2113 COVID-19, 2861 Non-COVID. | CT slides annotated by 5 radiographers. | Yes, 5 radiologists. | Cross validation | Yes | Not disclosed. | 4 | Not disclosed |
3. Results
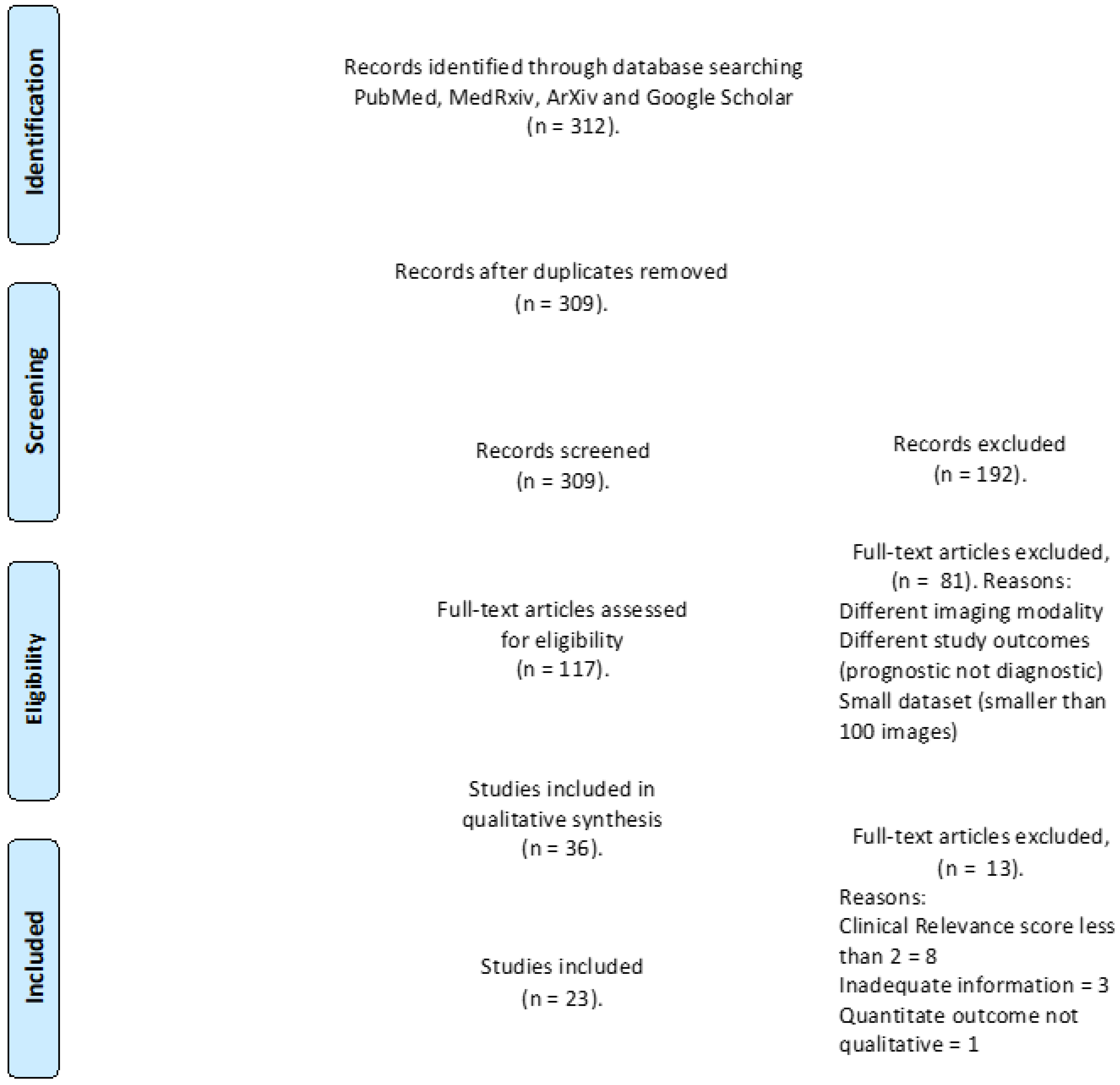
3.1. Study Selection
3.2. General Characteristics
3.3. Aim and Methodology
- The detection of and screening for COVID-19 (binary classification)
- Forming a differential diagnosis between COVID-19 pneumonia and other viral or bacterial pneumonia (multiclass classification).
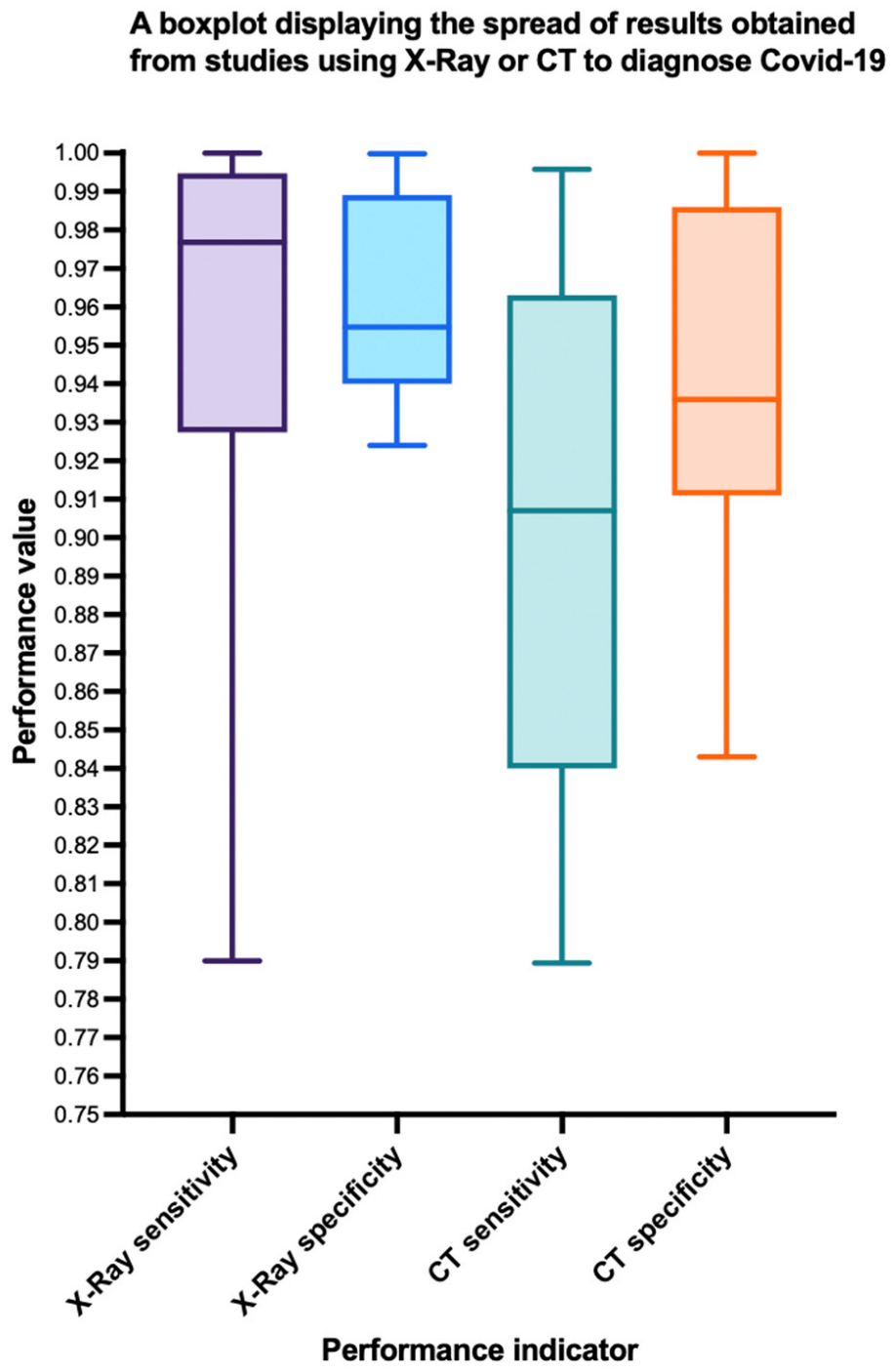
3.4. Reference Standard and Comparator
3.5. Validation and Testing
3.6. Clinical Relevance and Main Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Zhong, N.S.; Zheng, B.J.; Li, Y.M.; Poon, L.L.M.; Xie, Z.H.; Chan, K.H.; Li, P.H.; Tan, S.Y.; Chang, Q.; Xie, J.P.; et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet 2003, 362, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- WorldOMeter. Coronavirus Live Statistics. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 2 December 2020).
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction-Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: Innova lateral flow test is not fit for “test and release” strategy, say experts. BMJ 2020, 371, m4469. [Google Scholar] [CrossRef]
- Zokaeinikoo, M.; Kazemian, P.; Mitra, P.; Kumara, S. AIDCOV: An Interpretable Artificial Intelligence Model for Detection of COVID-19 from Chest Radiography Images. ACM Trans. Manag. Inf. Syst. 2021, 12, 1–20. [Google Scholar] [CrossRef]
- Ahmed, S.; Hossain, T.; Hoque, O.B.; Sarker, S.; Rahman, S.; Shah, F.M. Automated COVID-19 Detection from Chest X-Ray Images: A High Resolution Network (HRNet)Approach. SN Comput. Sci. 2021, 2, 1–17. [Google Scholar] [CrossRef]
- Yousefzadeh, M.; Esfahanian, P.; Movahed, S.M.S.; Gorgin, S.; Lashgari, R.; Rahmati, D.; Kiani, A.; Nadji, S.A.; Haseli, S.; Hoseinyazdi, M.; et al. Ai-corona: Radiologist-Assistant Deep Learning Framework for COVID-19 Diagnosis in Chest CT Scans. PLoS ONE 2021, 16, e0250952. [Google Scholar]
- Shibly, K.H.; Dey, S.K.; Islam, M.T.U.; Rahman, M.M. COVID Faster R-CNN: A Novel Framework to Diagnose Novel Coronavirus Disease (COVID-19) in X-Ray Images. Inform. Med. Unlocked 2020, 20, 100405. [Google Scholar] [CrossRef]
- Pesapane, F.; Codari, M.; Sardanelli, F. Artificial intelligence in medical imaging: Threat or opportunity? Radiologists again at the forefront of innovation in medicine. Eur. Radiol. Exp. 2018, 2, 35. [Google Scholar] [CrossRef] [Green Version]
- Duda, R.O.; Hart, P.E.; Education, I.C. Machine Learning Artificial Intelligence, Data Scienc. In Pattern Classification and Scene Analysis; Wiley: New York, NY, USA, 1973; Volume 3. [Google Scholar]
- Schmidhuber, J. Deep learning in neural networks: An overview. Neural Netw. 2015, 61, 85–117. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.C.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.S.; Maruthappu, M. Artificial intelligence versus clinicians: Systematic review of design, reporting standards, and claims of deep learning studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef] [Green Version]
- Krarup, M.M.K.; Krokos, G.; Subesinghe, M.; Nair, A.; Fischer, B.M. Artificial Intelligence for the Characterization of Pulmonary Nodules, Lung Tumors and Mediastinal Nodes on PET/CT. Semin. Nucl. Med. 2021, 51, 143–156. [Google Scholar] [CrossRef]
- Borkowski, A.A.; Viswanadham, N.A.; Thomas, L.B.; Guzman, R.D.; Deland, L.A.; Mastorides, S.M. Using Artificial Intelligence for COVID-19 Chest X-ray Diagnosis. Fed. Pract. 2020, 37, 398–404. [Google Scholar] [CrossRef]
- Keidar, D.; Yaron, D.; Goldstein, E.; Shachar, Y.; Blass, A.; Charbinsky, L.; Aharony, I.; Lifshitz, L.; Lumelsky, D.; Neeman, Z.; et al. COVID-19 Classification of X-ray Images Using Deep Neural Networks. Eur. Radiol. 2021, 31, 9654–9663. [Google Scholar] [CrossRef]
- Li, A.C.; Lee, D.T.; Misquitta, K.K.; Uno, K.; Wald, S. COVID-19 Detection From Chest Radiographs Using Machine Learning and Convolutional Neural Networks. medRxiv 2020. [Google Scholar] [CrossRef]
- Taresh, M.M.; Zhu, N.; Ali, T.A.A.; Hameed, A.S.; Mutar, M.L. Transfer learning to detect COVID-19 automatically from X-ray images, using convolutional neural networks. Int. J. Biomed. Imaging 2021, 2021. [Google Scholar] [CrossRef]
- Kikkisetti, S.; Zhu, J.; Shen, B.; Li, H.; Duong, T. Deep-learning convolutional neural networks with transfer learning accurately classify COVID19 lung infection on portable chest radiographs. PeerJ 2020, 8, e10309. [Google Scholar] [CrossRef]
- Gomes, J.C.; Barbosa, V.A.d.F.; de Santana, M.A.; Bandeira, J.; Valenca, M.J.S.; de Souza, R.E.; Ismael, A.M.; dos Santos, W.P. IKONOS: An intelligent tool to support diagnosis of COVID-19 by texture analysis of x-ray images. Res. Biomed. Eng. 2020, 1–14. [Google Scholar]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef]
- Sharma, V.; Dyreson, C. COVID-19 Screening Using Residual Attention Network an Artificial Intelligence Approach. arXiv 2020, arXiv:2006.16106. Available online: https://ui.adsabs.harvard.edu/abs/2020arXiv200616106S (accessed on 1 June 2020).
- Warman, A.; Warman, P.; Sharma, A.; Parikh, P.; Warman, R.; Viswanadhan, N.; Chen, L.; Mohapatra, S.; Mohapatra, S.S.; Sapiro, G. Interpretable Artificial Intelligence for COVID-19 Diagnosis from Chest CT Reveals Specificity of Ground-Glass Opacities. medRxiv 2020. [Google Scholar] [CrossRef]
- He, X.; Wang, S.; Shi, S.; Chu, X.; Tang, J.; Liu, X.; Yan, C.; Zhang, J.; Ding, G. Benchmarking Deep Learning Models and Automated Model Design for COVID-19 Detection with Chest CT Scans. medRxiv 2020. [Google Scholar] [CrossRef]
- Goel, C.; Kumar, A.; Dubey, S.K.; Srivastava, V. Efficient Deep Network Architecture for COVID-19 Detection Using Computed Tomography Images. medRxiv 2020. [Google Scholar] [CrossRef]
- Zheng, C.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Wang, X. Deep Learning-based Detection for COVID-19 from Chest CT using Weak Label. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Lokwani, R.; Gaikwad, A.; Kulkarni, V.; Pant, A.; Kharat, A. Automated Detection of COVID-19 from CT Scans Using Convolutional Neural Networks. arXiv 2020, arXiv:2006.13212. [Google Scholar]
- Liu, B.; Liu, P.; Dai, L.; Yang, Y.; Xie, P.; Tan, Y.; Du, J.; Shan, W.; Zhao, C.; Zhong, Q. Assisting Scalable Diagnosis Automatically via CT Images in the Combat against COVID-19. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Guiot, J.; Vaidyanathan, A.; Deprez, L.; Zerka, F.; Danthine, D.; Frix, A.-N.; Thys, M.; Henket, M.; Canivet, G.; Mathieu, S.; et al. Development and validation of an automated radiomic CT signature for detecting COVID-19. Diagnostics 2020, 11, 41. [Google Scholar] [CrossRef]
- Ko, H.; Chung, H.; Kang, W.S.; Kim, K.W.; Shin, Y.; Kang, S.J.; Lee, J.H.; Kim, Y.J.; Kim, N.Y.; Jung, H.; et al. COVID-19 Pneumonia Diagnosis Using a Simple 2D Deep Learning Framework With a Single Chest CT Image: Model Development and Validation. J. Med. Internet Res. 2020, 22, e19569. [Google Scholar] [CrossRef]
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 4080. [Google Scholar] [CrossRef]
- Mei, X.; Lee, H.-C.; Diao, K.-y.; Huang, M.; Lin, B.; Liu, C.; Xie, Z.; Ma, Y.; Robon, P.M.; Chung, M.; et al. Artificial intelligence—enabled rapid diagnosis of patients with COVID-19. Nat. Med. 2020, 26, 1224–1228. [Google Scholar] [CrossRef]
- Jin, C.; Chen, W.; Cao, Y.; Xu, Z.; Tan, Z.; Zhang, X.; Deng, L.; Zheng, C.; Zhou, J.; Shi, H.; et al. Development and evaluation of an artificial intelligence system for COVID-19 diagnosis. Nat. Commun. 2020, 11, 5088. [Google Scholar] [CrossRef]
- Futoma, J.; Simons, M.; Panch, T.; Doshi-Velez, F.; Celi, L.A. The myth of generalisability in clinical research and machine learning in health care. Lancet Digit. Health 2020, 2, e489–e492. [Google Scholar] [CrossRef]
- Roberts, M.; Driggs, D.; Thorpe, M.; Gilbey, J.; Yeung, M.; Ursprung, S.; Aviles-Rivero, A.I.; Etmann, C.; McCague, C.; Beer, L.; et al. Common pitfalls and recommendations for using machine learning to detect and prognosticate for COVID-19 using chest radiographs and CT scans. Nat. Mach. Intell. 2021, 3, 199–217. [Google Scholar] [CrossRef]


| Author | Dataset | Deep Learning Model | 2D/3D | All Data | COVID Data | Train All/COVID | Validation All/COVID | TestAll/COVID | Sensitivity | Specificity | AUC | Dataset | Code URL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [17] | COVID-19/non-COVID pneumonia/normal | Microsoft CustomVision | 2d | 1000 | 500 | 970/474 | 30/10 | / | 100 | 95 | / | Public | / |
| [7] | COVID-19/non-COVID infection/normal | AIDCOV using VGG-16 | 2d | 5801 | 269 | 4698 | 523 | 580 | 99.3 | 99.98 | n/a | Public | / |
| [18] | COVID-19/normal | RetNet50 | 2d | 2427 | 360 | 2120/84 | 350/178 | n/a | 87.1 | 92.4 | 0.94 | Institutional dataset | / |
| [20] | COVID-19/viral pneumonia/normal | VGG-16 | 2d | 1034 | 274 | 724/192 | / | 310/82 | / | / | 0.9978 | Public | / |
| [19] | COVID-19/viral/bacterial pneumonia/TB | DenseNet-201 | 2d | 9868 | 494 | 6234/(n/a) | 1574/(n/a) | 1970/125 | 94.62 | / | / | Public | / |
| [8] | COVID/non-COVID | HRNet | 2d | 1410 | 410 | n/a | / | 1410/410 | 98.53 | 98.52 | Public | / | |
| [21] | COVID/bacterial pneumonia/viral pneumonia/normal | VGG-16 | 2d | 2031 | 445 | 1523/334/ | / | 508/111 | 79.0 | 93 | 0.85 | Public | / |
| [10] | COVID/non-COVID | Faster R-CNN | 2d | 19,250 | 283 | 17,749/232 | / | 1501/51 | 97.65 | 95.48 | / | Public | / |
| [22] | COVID-19/bacterial and viral pneumonia/normal | IKONOS | 2d | 6320 | 464 | / | / | 97.7 | 99.3 | / | Public | https://github.com/Biomedical-Computing-UFPE/Ikonos-X-Desktop | |
| [32] | COVID-19/pneumonia/normal | DarkNet-19 | 2d | 1125 | 125 | 900/100 | / | 225/25 | 95.13 | 95.3 | / | Public | https://github.com/muhammedtalo/COVID-19 |
| [24] | COVID-19/non COVID-19 | Residual Att Net | 2d | 239 | 120 | 167/84 | 50/25 | 22/11 | 100 | 96 | 1 | Public | https://github.com/vishalshar/COVID-19-screening-using-RAN-on-Xray-images |
| Author | Dataset | Deep Learning Model | 2D /3D | All Data | COVID Data | Train All/COVID | Validation All/COVID | Test All/COVID | Sensitivity | Specificity | AUC | Dataset | Code URL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [25] | COVID-19/non-COVID disease/normal | 2d | 904 | 606 | 2685/2116 | / | 34/34 | 97.06 | / | 0.9664 | Institutional dataset | / | |
| [26] | COVID-19/common pneumonia/normal | MNas3DNet41 | 3d | 3993 | 1515 | 3195/1213 | / | 798/302 | 86.09 | 93.15 | 0.957 | Public | / |
| [27] | COVID-19/non-COVID-19 disease | GLCM | 2d | 2483 | 1252 | 1986/1002 | / | 497/250 | / | 98.77 | 0.987 | Public | / |
| [9] | COVID-19/non-COVID pathological/normal | Ai-corona | 2d | 2121 | 720 | 1764/601 | / | 357/119 | 92.4 | 98.3 | 0.989 | Institutional dataset | https://ai-corona.com/ |
| [28] | COVID-19/normal | DeCoVNet | 3d | 630 | 630 | 499 | / | 131 | 90.7 | 91.1 | 0.976 | Institutional dataset | https://github.com/sydney0zq/COVID-19-detection |
| [30] | COVID/non-COVID | COVIDNet | 2d | 1993 | 920 | 1316/642 | 522/233 | 894/387 | 92.2 | 98.6 | 0.98 | Institutional dataset | / |
| [31] | COVID/non-COVID | RadiomiX | 2d | 1381 | 181 | 1104/145 | / | 276/36 | 78.94 | 91.09 | 0.9398 | Institutional dataset | / |
| [32] | COVID-19/bacterial/viral pneumonia | FCONet ft ResNet-50 | 2d | 4257 | 1194 | 3194/955 | / | 1063/239 | 99.58 | 100 | 1 | Institutional dataset e | / |
| [33] | COVID-19/non COVID-19 | Densenet-121 | 3d | 2724 | 1029 | 1059/526 | 328/177 | 1337/326 | 84.0 | 93.0 | 0.949 | Mixed | https://ngc.nvidia.com/catalog/containers/nvidia:clara:ai-COVID-19 |
| [34] | COVID-19/non-COVID-19 | Inception-ResNet-v2 | 3d | 905 | 419 | 534/242 | 92/43 | 279/134 | 82.8 | 84.3 | 0.92 | Institutional dataset | https://github.com/howchihlee/COVID19_CT |
| [35] | COVID-19/viral pneumonia/bacterial pneumonia/influenza | OpenCovidDetector | 2d | 11,356 | 3084 | 2688/751 | / | 6337/2333 | 87.03 | 96.60 | 0.9781 | Public | https://github.com/ChenWWWeixiang/diagnosis_covid19 |
| [29] | COVID-19/non COVID-19 | U-Net | 2d | 5212 (slices) | 275 | 3285/657 | 597/120 | 1330/266 | 96.3 | 93.6 | / | Public | / |
| Dataset Name | Study Used |
|---|---|
| Kaggle RSNA Pneumonia Detection challenge dataset | [8,17] |
| NIH | [33] |
| SUNY | [33] |
| LIDC | [33,35] |
| CC-CCII | [35] |
| Tianchi-Alibaba | [35] |
| MosMedData | [35] |
| Cohen database | [10,17,21] |
| Italian society of Medical and Interventional Radiology | [32] |
| WKUH (Wonkwang University hospital) | [32] |
| CNUH (Chonnam National University Hospital) | [32] |
| COVID-19-CT-dataset | [29] |
| MDH (MasihDaneshvari Hospital) | [9] |
| Peshmerga Hospital Erbil | [22] |
| Network Name | Study Used |
|---|---|
| HRNetHRNet | [8] |
| Microsoft CustomVisionMicrosoft CustomVision | [17] |
| GLCMGLCM | [27] |
| ResNetResNet | [18,24,32,34,35] |
| RadioMixRadioMix | [31] |
| UNetUNet | [28,29] |
| VGGVGG | [7,10,20,21,24] |
| DenseNetDenseNet | [19,26,30,33] |
| DarkNetDarkNet | [23,25] |
| EfficientNetEfficientNet | [9] |
| Study | AI Performance | Radiologist Performance | Additional Information | Experience of the Radiologist | ||
|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | |||
| [9] | 0.92 | 0.97 | 0.90 | 0.88 | Time taken to assess one image: AI→2.02 s. Radiologist→58.0 s. | 4 radiologists, average experience 9.25 years. |
| [30] | 0.92 | 0.99 | 0.77 | 0.90 | 4 radiologists, average experience 11.25 years. | |
| [35] | 0.98 | 0.91 | 0.96 | 0.72 | Time taken to assess one image: AI→2.73 s. Radiologist→390 s. All 5 radiologists had a n average of 8 years experience. | 5 radiologists, average experience of 8 years. |
| [34] | 0.84 | 0.83 | 0.75 | 0.94 | 2 radiologists, average experience of 6 years. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulrenan, C.; Rhode, K.; Fischer, B.M. A Literature Review on the Use of Artificial Intelligence for the Diagnosis of COVID-19 on CT and Chest X-ray. Diagnostics 2022, 12, 869. https://doi.org/10.3390/diagnostics12040869
Mulrenan C, Rhode K, Fischer BM. A Literature Review on the Use of Artificial Intelligence for the Diagnosis of COVID-19 on CT and Chest X-ray. Diagnostics. 2022; 12(4):869. https://doi.org/10.3390/diagnostics12040869
Chicago/Turabian StyleMulrenan, Ciara, Kawal Rhode, and Barbara Malene Fischer. 2022. "A Literature Review on the Use of Artificial Intelligence for the Diagnosis of COVID-19 on CT and Chest X-ray" Diagnostics 12, no. 4: 869. https://doi.org/10.3390/diagnostics12040869