
Inflammatory Tumor Microenvironment in Cranial Meningiomas: Clinical Implications and Intraindividual Reproducibility

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
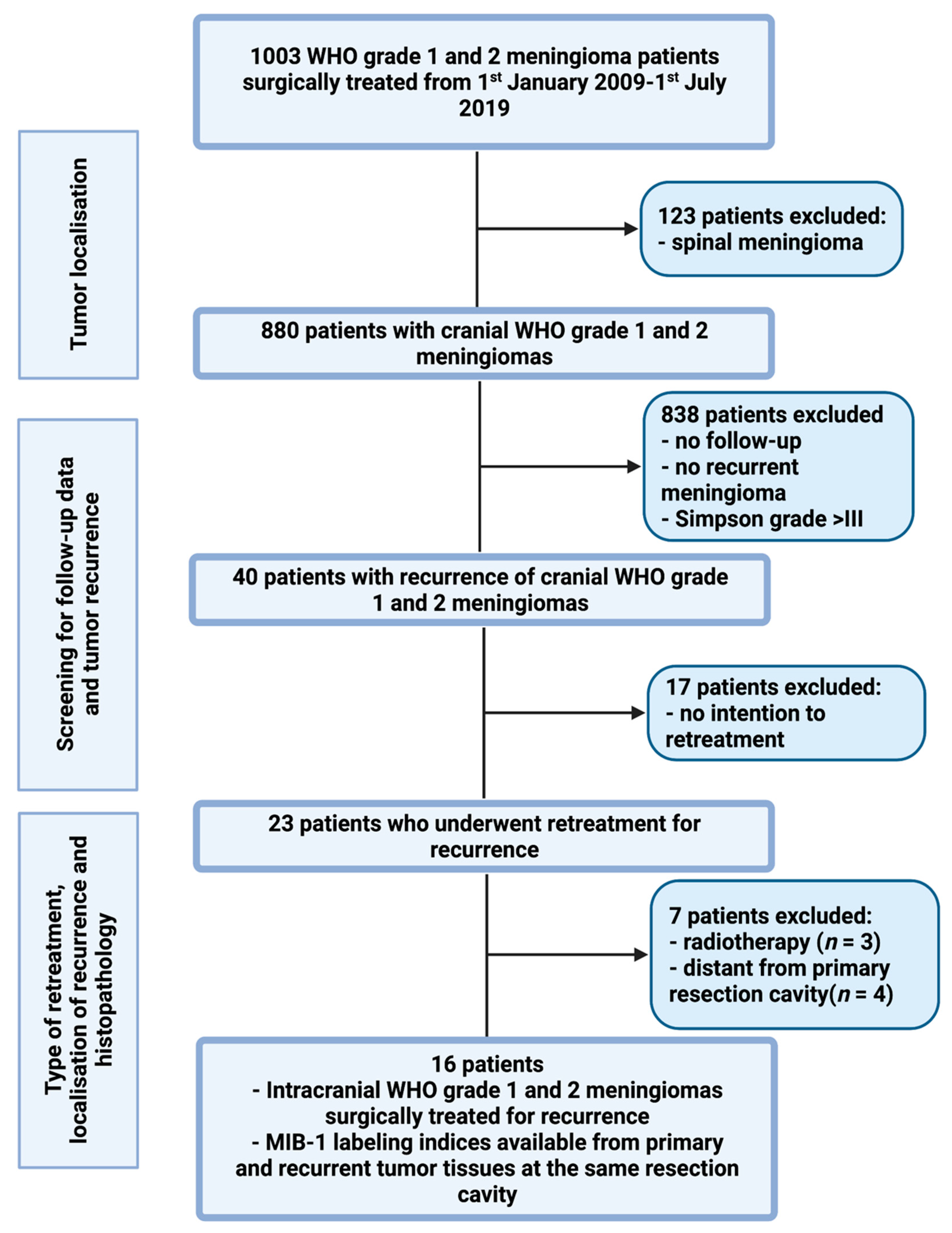
2.1. Study Design and Patient Characteristics
2.2. Data Recording
2.3. Histopathology
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
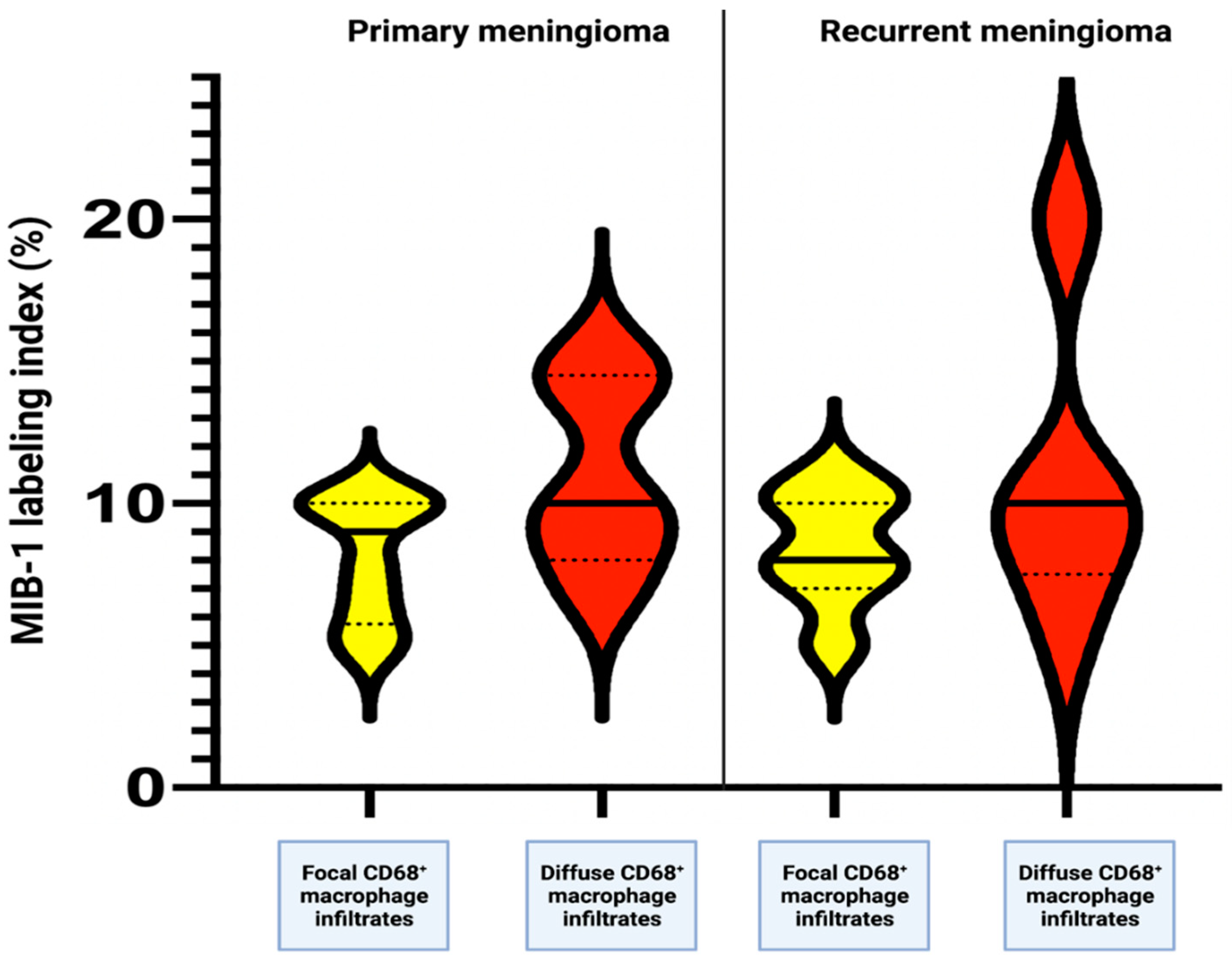
3.2. Increased MIB-1 Labeling Index
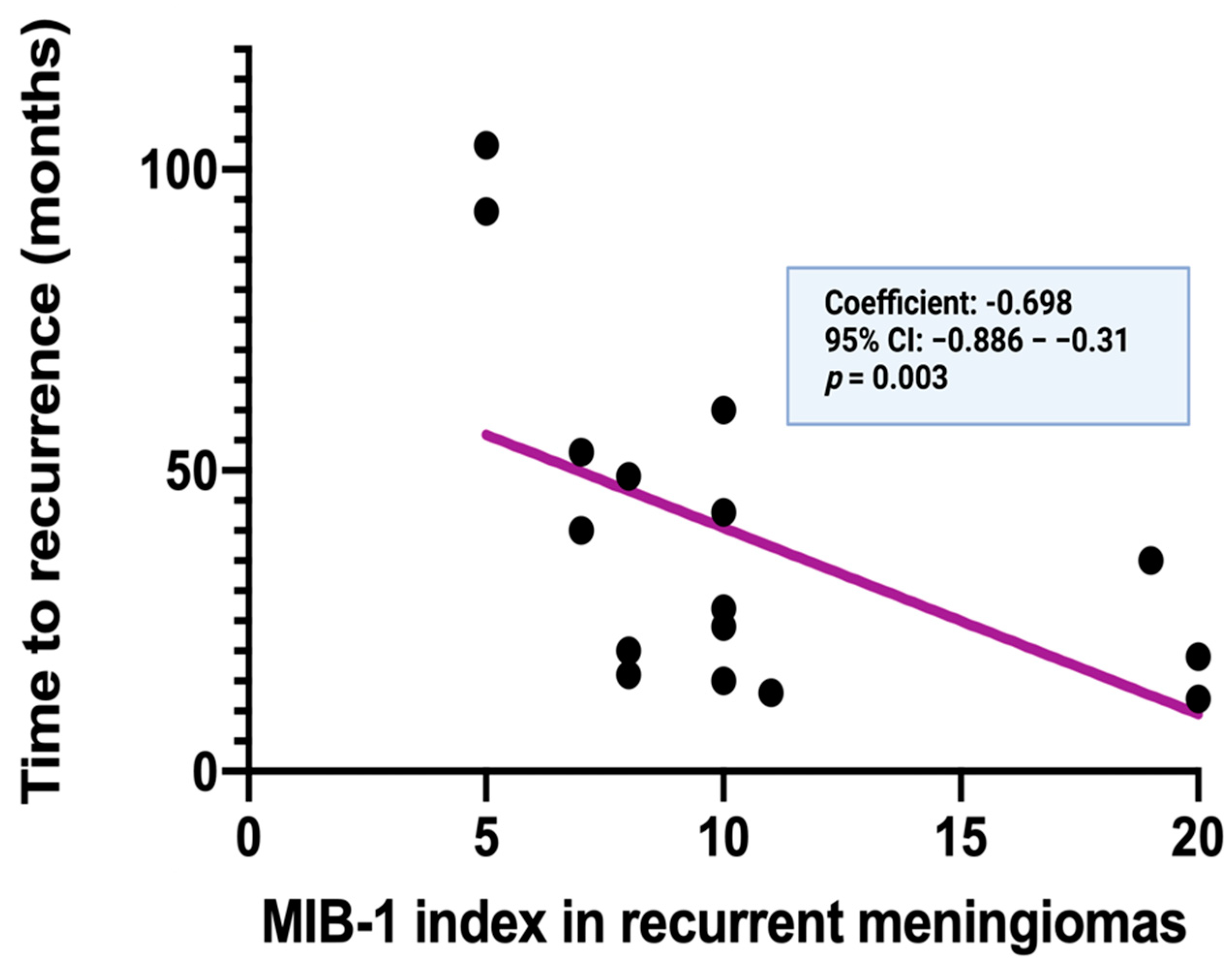
3.3. Time to Recurrence
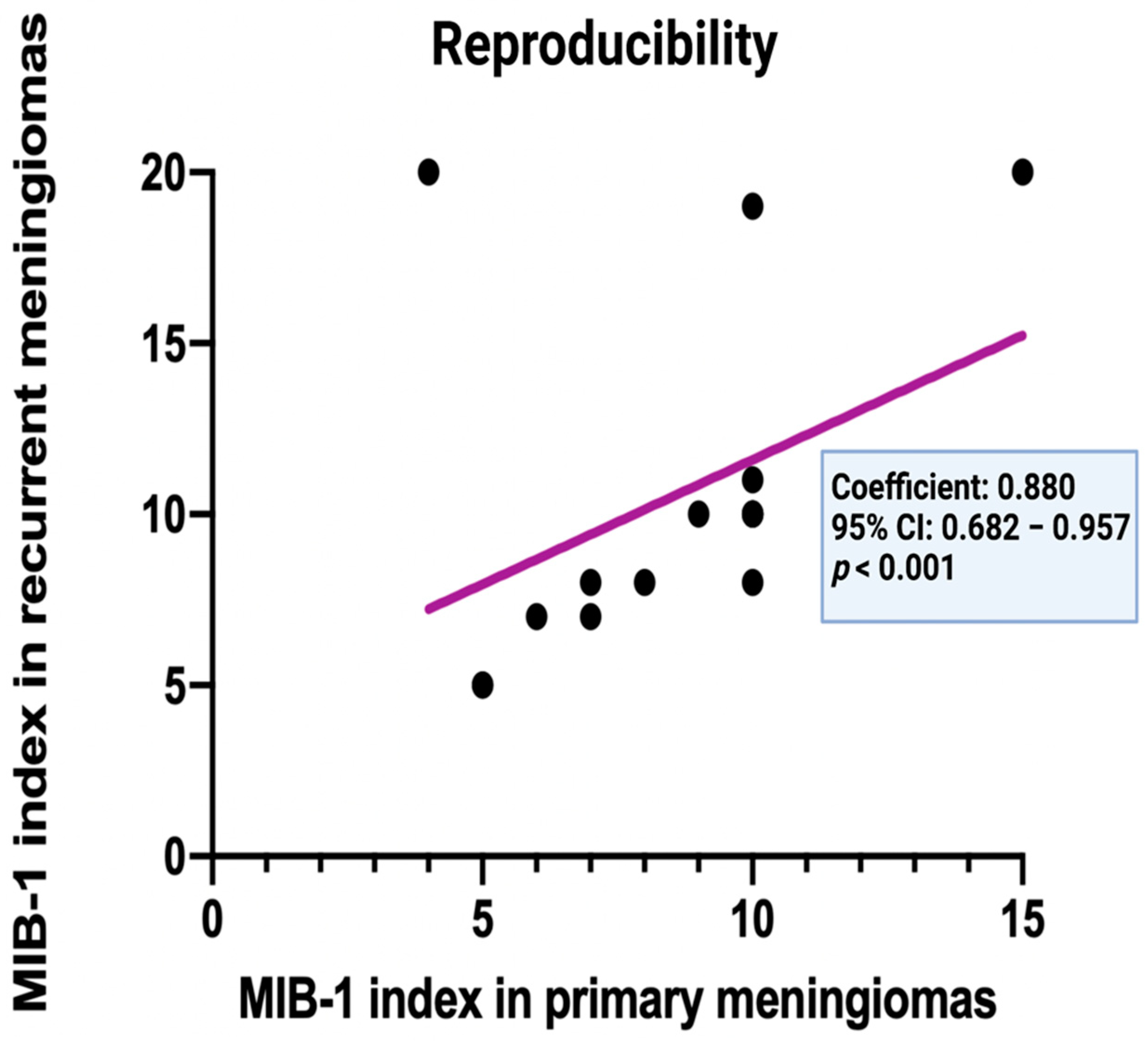
3.4. Intraindividual Reproducibility of the MIB-1 Labeling Index in Primary and Recurrent Cranial Meningiomas
3.5. Factors Influencing the Intraindividual Course of the MIB-1 Labeling Indices in Primary and Their Corresponding Recurrent Meningiomas
3.6. Correlation between the Time to Recurrence, Volumetric Tumor Regrowth and Pattern of Recurrence with the MIB-1 Labeling Index in Simpson Grade IV or V Resected Meningiomas
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Fulop, J.; Liu, M.; Blanda, R.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008–2012. Neuro Oncol. 2015, 17 (Suppl. S4), iv1–iv62. [Google Scholar] [CrossRef]
- Domingues, P.H.; Sousa, P.; Otero, Á.; Gonçalves, J.M.; Ruiz, L.; de Oliveira, C.; Lopes, M.C.; Orfao, A.; Tabernero, M.D. Proposal for a new risk stratification classification for meningioma based on patient age, WHO tumor grade, size, localization, and karyotype. Neuro Oncol. 2014, 16, 735–747. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Alexiou, G.A.; Gogou, P.; Markoula, S.; Kyritsis, A.P. Management of meningiomas. Clin. Neurol. Neurosurg. 2010, 112, 177–182. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; Orrego, A.; Lönn, S.; Mathiesen, T. Long-term 25-year follow-up of surgically treated parasagittal meningiomas. World Neurosurg. 2011, 76, 564–571. [Google Scholar] [CrossRef]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [Green Version]
- Sumkovski, R.; Micunovic, M.; Kocevski, I.; Ilievski, I.; Ilievski, B.; Petrov, I. Surgical Treatment of Meningiomas—Outcome Associated With Type of Resection, Recurrence, Karnofsky Performance Score, Mitotic Count. Open Access Maced. J. Med. Sci. 2019, 7, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Vranic, A.; Popovic, M.; Cör, A.; Prestor, B.; Pizem, J. Mitotic count, brain invasion, and location are independent predictors of recurrence-free survival in primary atypical and malignant meningiomas: A study of 86 patients. Neurosurgery 2010, 67, 1124–1132. [Google Scholar] [CrossRef] [Green Version]
- Van Diest, P.J.; Brugal, G.; Baak, J.P. Proliferation markers in tumours: Interpretation and clinical value. J. Clin. Pathol. 1998, 51, 716–724. [Google Scholar] [CrossRef] [Green Version]
- Wach, J.; Brandecker, S.; Güresir, A.; Schuss, P.; Vatter, H.; Güresir, E. The impact of the MIB-1 index on facial nerve outcomes in vestibular schwannoma surgery. Acta Neurochir. 2020, 162, 1205–1213. [Google Scholar] [CrossRef] [Green Version]
- Gerdes, J.; Schwab, U.; Lemke, H.; Stein, H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int. J. Cancer 1983, 31, 13–20. [Google Scholar] [CrossRef]
- Scholzen, T.; Gerdes, J. The Ki-67 protein: From the known and the unknown. J. Cell Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Oya, S.; Kawai, K.; Nakatomi, H.; Saito, N. Significance of Simpson grading system in modern meningioma surgery: Integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO Grade I meningiomas. J. Neurosurg. 2012, 117, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.S.; Kim, K.H.; Lee, E.H.; Lee, Y.M.; Lee, S.H.; Kim, H.D.; Kim, Y.Z. Results of immunohistochemical staining for cell cycle regulators predict the recurrence of atypical meningiomas. J. Neurosurg. 2014, 121, 1189–1200. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Song, S.Y.; Jiang, J.B.; Wang, T.J.; Yan, C.X. The prognostic role of Ki-67/MIB-1 in meningioma: A systematic review with meta-analysis. Medicine 2020, 99, e18644. [Google Scholar] [CrossRef]
- Polley, M.Y.; Leung, S.C.; McShane, L.M.; Gao, D.; Hugh, J.C.; Mastropasqua, M.G.; Viale, G.; Zabaglo, L.A.; Penault-Llorca, F.; Bartlett, J.M.; et al. International Ki67 in Breast Cancer Working Group of the Breast International Group and North American Breast Cancer Group. An international Ki67 reproducibility study. J. Natl. Cancer Inst. 2013, 105, 1897–1906. [Google Scholar] [CrossRef]
- Mirian, C.; Skyrman, S.; Bartek, J., Jr.; Jensen, L.R.; Kihlström, L.; Förander, P.; Orrego, A.; Mathiesen, T. The Ki-67 Proliferation Index as a Marker of Time to Recurrence in Intracranial Meningioma. Neurosurgery 2020, 87, 1289–1298. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Kanungo, I.; Sudhir, S.; Chen, J.S.; Raleigh, D.R.; Magill, S.T.; McDermott, M.W.; Aghi, M.K. WHO grade I Meningioma Recurrence: Identifying High Risk Patients Using Histopathological Features and the MIB-1 Index. Front. Oncol. 2020, 10, 1522. [Google Scholar] [CrossRef]
- Nishimura, R.; Osako, T.; Nishiyama, Y.; Tashima, R.; Nakano, M.; Fujisue, M.; Toyozumi, Y.; Arima, N. Prognostic significance of Ki-67 index value at the primary breast tumor in recurrent breast cancer. Mol. Clin. Oncol. 2014, 2, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Schröder, R.; Feisel, K.D.; Ernestus, R.I. Ki-67 labeling is correlated with the time to recurrence in primary glioblastomas. J. Neurooncol. 2002, 56, 127–132. [Google Scholar] [CrossRef]
- Proctor, D.T.; Huang, J.; Lama, S.; Albakr, A.; Van Marle, G.; Sutherland, G.R. Tumor-associated macrophage infiltration in meningioma. Neurooncol. Adv. 2019, 1, vdz018. [Google Scholar] [CrossRef]
- Domingues, P.H.; Teodósio, C.; Ortiz, J.; Sousa, P.; Otero, A.; Maillo, A.; Bárcena, P.; García-Macias, M.C.; Lopes, M.C.; de Oliveira, C.; et al. Immunophenotypic identification and characterization of tumor cells and infiltrating cell populations in meningiomas. Am. J. Pathol. 2012, 181, 1749–1761. [Google Scholar] [CrossRef]
- Asai, J.; Suzuki, R.; Fujimoto, T.; Suzuki, T.; Nakagawa, N.; Nagashima, G.; Miyo, T.; Hokaku, H.; Takei, A. Fluorescence automatic cell sorter and immunohistochemical investigation of CD68-positive cells in meningioma. Clin. Neurol. Neurosurg. 1999, 101, 229–234. [Google Scholar] [CrossRef]
- Jung, K.Y.; Cho, S.W.; Kim, Y.A.; Kim, D.; Oh, B.C.; Park, D.J.; Park, Y.J. Cancers with Higher Density of Tumor-Associated Macrophages Were Associated with Poor Survival Rates. J. Pathol. Transl. Med. 2015, 49, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Antinheimo, J.; Haapasalo, H.; Haltia, M.; Tatagiba, M.; Thomas, S.; Brandis, A.; Sainio, M.; Carpen, O.; Samii, M.; Jääskeläinen, J. Proliferation potential and histological features in neurofibromatosis 2-associated and sporadic meningiomas. J. Neurosurg. 1997, 87, 610–614. [Google Scholar] [CrossRef]
- Roser, F.; Nakamura, M.; Bellinzona, M.; Ritz, R.; Ostertag, H.; Tatagiba, M.S. Proliferation potential of spinal meningiomas. Eur. Spine J. 2006, 15, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Coons, S.W.; Johnson, P.C. Regional heterogeneity in the proliferative activity of human gliomas as measured by the Ki-67 labeling index. J. Neuropathol. Exp. Neurol. 1993, 52, 609–618. [Google Scholar] [CrossRef]
- Wach, J.; Lampmann, T.; Güresir, Á.; Vatter, H.; Herrlinger, U.; Becker, A.; Cases-Cunillera, S.; Hölzel, M.; Toma, M.; Güresir, E. Proliferative Potential, and Inflammatory Tumor Microenvironment in Meningioma Correlate with Neurological Function at Presentation and Anatomical Location—From Convexity to Skull Base and Spine. Cancers 2022, 14, 1033. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.W.; Kim, M.S.; Kim, S.W.; Chang, C.H.; Kim, O.L. Peritumoral brain edema in meningiomas: Correlation of radiologic and pathologic features. J. Korean Neurosurg. Soc. 2011, 49, 26–30. [Google Scholar] [CrossRef]
- Wach, J.; Apallas, S.; Schneider, M.; Güresir, A.; Schuss, P.; Herrlinger, U.; Vatter, H.; Güresir, E. Baseline Serum C-Reactive Protein and Plasma Fibrinogen-Based Score in the Prediction of Survival in Glioblastoma. Front. Oncol. 2021, 11, 653614. [Google Scholar] [CrossRef]
- Majores, M.; Schick, V.; Engels, G.; Fassunke, J.; Elger, C.E.; Schramm, J.; Blumcke, I.; Becker, A.J. Mutational and immunohistochemical analysis of ezrin-, radixin-, moesin (ERM) molecules in epilepsy-associated glioneuronal lesions. Acta Neuropathol. 2005, 110, 537–546. [Google Scholar] [CrossRef]
- Majores, M.; von Lehe, M.; Fassunke, J.; Schramm, J.; Becker, A.J.; Simon, M. Tumor recurrence and malignant progression of gangliogliomas. Cancer 2008, 113, 3355–3363. [Google Scholar] [CrossRef]
- Schneider, M.; Borger, V.; Güresir, A.; Becker, A.; Vatter, H.; Schuss, P.; Güresir, E. High Mib-1-score correlates with new cranial nerve deficits after surgery for frontal skull base meningioma. Neurosurg. Rev. 2021, 44, 381–387. [Google Scholar] [CrossRef]
- Nassiri, F.; Price, B.; Shehab, A.; Au, K.; Cusimano, M.D.; Jenkinson, M.D.; Jungk, C.; Mansouri, A.; Santarius, T.; Suppiah, S.; et al. International Consortium on Meningiomas. Life after surgical resection of a meningioma: A prospective cross-sectional study evaluating health-related quality of life. Neuro Oncol. 2019, 21 (Suppl. 1), i32–i43. [Google Scholar] [CrossRef] [Green Version]
- Haller, B.; Ulm, K.; Hapfelmeier, A. A Stimulation Study Comparing Different Statistical Approaches for the Identification of Predictive Biomarkers. Comput. Math Methods Med. 2019, 2019, 7037230. [Google Scholar] [CrossRef] [Green Version]
- Faraji, A.H.; Tonetti, D.A.; Flickinger, J.C.; Engh, J.A. Alteration of the Ki-67 Proliferative Index following Surgical Resection with or without Radiation Therapy of Intracranial Meningiomas. Cureus 2017, 9, e1873. [Google Scholar] [CrossRef] [Green Version]
- Cornelius, J.F.; Slotty, P.J.; Steiger, H.J.; Hänggi, D.; Polivka, M.; George, B. Malignant potential of skull base versus non-skull base meningiomas: Clinical series of 1663 cases. Acta Neurochir. 2013, 155, 407–413. [Google Scholar] [CrossRef]
- Bečulić, H.; Skomorac, R.; Jusić, A.; Alić, F.; Mašović, A.; Burazerović, E.; Omerhodžić, I.; Dorić, M.; Imamović, M.; Mekić-Abazović, A.; et al. Correlation of peritumoral brain edema with morphological characteristics and Ki67 proliferative index in resected intracranial meningiomas. Acta Clin. Croat. 2019, 58, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Song, D.P.; Wang, T. Meningiomas with different histological grade in the same patient: Case report. Medicine 2017, 96, e9086. [Google Scholar] [CrossRef]
- Ohba, S.; Kobayashi, M.; Horiguchi, T.; Onozuka, S.; Yoshida, K.; Ohira, T.; Kawase, T. Long-term surgical outcome and biological prognostic factors in patients with skull base meningiomas. J. Neurosurg. 2011, 114, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Soyuer, S.; Chang, E.L.; Selek, U.; Shi, W.; Maor, M.H.; DeMonte, F. Radiotherapy after surgery for benign cerebral meningioma. Radiother. Oncol. 2004, 71, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Cha, Y.J.; Suh, S.H.; Lee, I.J.; Lee, K.S.; Hong, C.K.; Kim, J.W. Risk group-adapted adjuvant radiotherapy for WHO grade I and II skull base meningioma. J. Cancer Res. Clin. Oncol. 2019, 145, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Oya, S.; Ikawa, F.; Ichihara, N.; Wanibuchi, M.; Akiyama, Y.; Nakatomi, H.; Mikuni, N.; Narita, Y. Effect of adjuvant radiotherapy after subtotal resection for WHO grade I meningioma: A propensity score matching analysis of the Brain Tumor Registry of Japan. J. Neurooncol. 2021, 153, 351–360. [Google Scholar] [CrossRef]
- Rogers, L.; Barani, I.; Chamberlain, M.; Kaley, T.J.; McDermott, M.; Raizer, J.; Schiff, D.; Weber, D.C.; Wen, P.Y.; Vogelbaum, M.A. Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review. J. Neurosurg. 2015, 122, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.L.; Cruz Sanchez, F.; Hughes, J.T.; Esiri, M.M.; Coakham, H.B. Immunocytochemical study of the cellular immune response in meningiomas. J. Clin. Pathol. 1988, 41, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Grund, S.; Schittenhelm, J.; Roser, F.; Tatagiba, M.; Mawrin, C.; Kim, Y.J.; Bornemann, A. The microglial/macrophagic response at the -brain border of invasive meningiomas. Neuropathol. Appl. Neurobiol. 2009, 35, 82–88. [Google Scholar] [CrossRef]
- Murray, P.J.; Allen, J.E.; Biswas, S.K.; Fisher, E.A.; Gilroy, D.W.; Goerdt, S.; Gordon, S.; Hamilton, J.A.; Ivashkiv, L.B.; Lawrence, T.; et al. Macrophage activation and polarization: Nomenclature and experimental guidelines. Immunity 2014, 41, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Adams, C.L.; Ercolano, E.; Ferluga, S.; Sofela, A.; Dave, F.; Negroni, C.; Kurian, K.M.; Hilton, D.A.; Hanemann, C.O. A Rapid Robust Method for Subgrouping Non-NF2 Meningiomas According to Genotype and Detection of Lower Levels of M2 Macrophages in AKT1 E17K Mutated Tumours. Int. J. Mol. Sci. 2020, 21, 1273. [Google Scholar] [CrossRef] [Green Version]
- Matsuno, A.; Fujimaki, T.; Sasaki, T.; Nagashima, T.; Ide, T.; Asai, A.; Matsuura, R.; Utsunomiya, H.; Kirino, T. Clinical and histopathological analysis of proliferative potentials of recurrent and non-recurrent meningiomas. Acta Neuropathol. 1996, 91, 504–510. [Google Scholar] [CrossRef]
- Kasuya, H.; Kubo, O.; Tanaka, M.; Amano, K.; Kato, K.; Hori, T. Clinical and radiological features related to the growth potential of meninigioma. Neurosurg. Rev. 2006, 29, 293–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, Z.Y.; Shao, C.; Huang, Y.L.; Hui, G.Z.; Zhou, Y.X.; Wang, Z. Reproductive and exogenous hormone factors in relation to risk of meningioma in women: A meta-analysis. PLoS ONE 2013, 8, e83261. [Google Scholar] [CrossRef] [PubMed]
- Pines, A. Hormone therapy and brain tumors. Climacteric 2011, 14, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Presta, I.; Guadagno, E.; Di Vito, A.; Malara, N.; Mignogna, C.; Maisano, D.; Donato, A.; Cardillo, G.; Del Basso De Caro, M.L.; Donato, G. Innate immunity may play a role in growth and relapse of chordoid meningioma. Int. J. Immunopathol. Pharmacol. 2017, 30, 429–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.J.; Reis, G.; Kohanbash, G.; Shrivastav, S.; Magill, S.T.; Molinaro, A.M.; McDermott, M.W.; Theodosopoulos, P.V.L.; Aghi, M.K.; Berger, M.S.; et al. Expression and prognostic impact of immune modulatory molecule PD-L1 in meningioma. J. Neurooncol. 2016, 130, 543–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arasanz, H.; Gato-Cañas, M.; Zuazo, M.; Ibañez-Vea, M.; Breckpot, K.; Kochan, G.; Escors, D. PD1 signal transduction pathways in T cells. Oncotarget 2017, 8, 51936–51945. [Google Scholar] [CrossRef] [Green Version]
- Garzon-Muvdi, T.; Bailey, D.D.; Pernik, M.N.; Pan, E. Basis for Immunotherapy for Treatment of Meningiomas. Front. Neurol. 2020, 11, 945. [Google Scholar] [CrossRef]
- Tian, W.; Liu, J.; Zhao, K.; Wang, J.; Jian, W.; Shu, K.; Lei, T. Analysis of Prognostic Factors of World Health Organization Grade III Meningiomas. Front. Oncol. 2020, 10, 593073. [Google Scholar] [CrossRef]
- Perry, A.; Stafford, S.L.; Scheithauer, B.W.; Suman, V.J.; Lohse, C.M. Meningioma grading: An analysis of histologic parameters. Am. J. Surg. Pathol. 1997, 21, 1455–1465. [Google Scholar] [CrossRef]
- Bruna, J.; Brell, M.; Ferrer, I.; Gimenez-Bonafe, P.; Tortosa, A. Ki-67 proliferative index predicts clinical outcome in patients with atypical or anaplastic meningioma. Neuropathology 2007, 27, 114–120. [Google Scholar] [CrossRef]
- Shan, B.; Zhang, J.; Song, Y.; Xu, J. Prognostic factors for patients with World Health Organization grade III meningioas treated at a single center. Medicine 2017, 96, e7385. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Xie, Q.; Zhou, Y.; Chen, H.; Mao, Y.; Zhong, P.; Zheng, K.; Wang, Y.; Wang, Y.; Xie, L.; et al. Analysis of prognostic factors and treatment of anaplastic meningioma in China. J. Clin. Neurosci. 2015, 22, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Ishida, M.; Fukami, T.; Nitta, N.; Iwai, M.; Yoshida, K.; Kagotani, A.; Nozaki, K.; Okabe, H. Xanthomatous meningioma: A case report with review of the literature. Int. J. Clin. Exp. Pathol. 2013, 6, 2242–2246. [Google Scholar] [PubMed]
- Wach, J.; Lampmann, T.; Güresir, Á.; Schuss, P.; Vatter, H.; Herrlinger, U.; Becker, A.; Hölzel, M.; Toma, M.; Güresir, E. Forge: A Novel Scoring System to Predict the MIB-1 Labeling Index in Intracranial Meningiomas. Cancers 2021, 13, 3643. [Google Scholar] [CrossRef] [PubMed]
- Todo, T.; Adams, E.F.; Rafferty, B.; Fahlbusch, R.; Dingermann, T.; Werner, H. Secretion of interleukin-6 by human meningioma cells: Possible autocrine inhibitory regulation of neoplastic cell growth. J. Neurosurg. 1994, 81, 394–401. [Google Scholar] [CrossRef]
- Wong, L.Y.F.; Leung, R.Y.H.; Ong, K.L.; Cheung, B.M.Y. Plasma levels of fibrinogen and C-reactive protein are related to interleukin-6 gene -572C>G polymorphism in subjects with and without hypertension. J. Hum. Hypertens. 2007, 21, 875–882. [Google Scholar] [CrossRef]
- Devaraj, S.; Jialal, I. C-reactive protein polarizes human macrophages to an M1 phenotype and inhibits transformation to the M2 phenotype. Arter. Thromb. Vasc. Biol. 2011, 31, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wang, G.; Zhang, J.; Zhang, G.; Lin, Y.; Lin, Z.; Gu, J.; Kang, D.; Ding, C. A Novel Scoring System Based on Preoperative Routine Blood Test in Predicting Prognosis of Atypical Meningioma. Front. Oncol. 2020, 10, 1705. [Google Scholar] [CrossRef]
- Ersoz, S.; Yilmaz, Z.S.; Eyuboglu, I.; Yazar, U. Xanthomatous Meningioma: A Case Report. Turk Neurosurg. 2019, 29, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Stone, J.; Hoffpauir, J.T.; Xiong, Z. Histiocytic meningioma: A distinctive subtype of meningioma? Intractable Rare Dis. Res. 2014, 3, 57–59. [Google Scholar] [CrossRef] [Green Version]
- Kirkegaard, L.J.; DeRose, P.B.; Yao, B.; Cohen, C. Image cytometric measurement of nuclear proliferation markers (MIB-1, PCNA) in astrocytomas. Prognostic significance. Am. J. Clin. Pathol. 1998, 109, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median Age (IQR) (in Year) | 53.5 (42.5–69.8) |
|---|---|
| Sex | |
| Female | 9 (56.3%) |
| Male | 7 (43.7%) |
| Median preoperative KPS (IQR) | 85 (80–90) |
| Tumor location | |
| Falx | 8 (50.0%) |
| Convexity | 3 (18.8%) |
| Spheno-orbital | 2 (12.5%) |
| Sphenoid wing | 1 (6.25%) |
| Olfactory groove | 1 (6.25%) |
| Intraventricular | 1 (6.25%) |
| Multiple meningiomas | 4 (25.0%) |
| Median baseline tumor volume (cm3, 25th–75th percentile) | 46.0 (22.4–72.4) |
| Median tumor volume of recurrent meningiomas (cm3, 25th–75th percentile) | 6.13 (4.0–21.5) |
| Peritumoral edema | 11 (68.8%) |
| Sinus invasion | 3 (18.8%) |
| Brain invasion | 2 (12.5%) |
| Simpson grade | |
| Simpson grades I and II | 14 (87.5%) |
| Simpson grade ≥ III | 2 (12.5%) |
| WHO grade | |
| WHO grade 1 | 8 (50.0%) |
| WHO grade 2 | 8 (50.0%) |
| Median primary MIB-1 index (IQR) | 9 (6.5, 10.0) |
| Median MIB-1 index in recurrent tumor (IQR) | 10 (7.3, 10.0) |
| Median primary mitotic count (IQR) | 4 (2.3. 6.0) |
| Median mitotic count in recurrent tissue (IQR) | 3 (2.0, 6.0) |
| CD68+ macrophage infiltrates (Primary tumor) | |
| Focal | 11 (68.75) |
| Diffuse | 5 (31.25%) |
| CD68+ macrophage infiltrates (Recurrent tumor) [available in 14 patients] | |
| Focal | 6 (42.9%) |
| Diffuse | 8 (57.1%) |
| Primary Immunohistochemical Investigation | CD68− Cells | CD68+ Cells | p-Value |
|---|---|---|---|
| MIB-1 labeling index < 9% | 5 (83.3%) | 1 (16.7%) | 0.59 |
| MIB-1 labeling index ≥ 9% | 6 (60.0%) | 4 (40.0%) | |
| Immunohistochemical investigation in recurrent meningiomas [available in 14 patients] | |||
| MIB-1 labeling index < 10% | 3 (50.0%) | 3 (50.0%) | 0.99 |
| MIB-1 labeling index ≥ 10% | 3 (37.5%) | 5 (62.5%) | |
| “−” constituting no to focal positive staining; “+” constituting elevated positive staining | |||
| Variable | Mean (Months) | +/− SD (Months) | p-Value |
|---|---|---|---|
| Age | 0.98 | ||
| ≥54 | 39.3 | 17.1 | |
| <54 | 38.8 | 31.2 | |
| Sex | 0.07 | ||
| Male | 24.9 | 12.4 | |
| Female | 49.9 | 31.9 | |
| Tumor volume | 0.49 | ||
| <46 cm3 | 33.9 | 16.5 | |
| ≥46 cm3 | 44.0 | 36.3 | |
| Peritumoral edema | 0.36 | ||
| Present | 32.7 | 20.2 | |
| Not present | 43.2 | 34.8 | |
| Multiple meningiomas | 0.81 | ||
| Present | 38.0 | 18.6 | |
| Not present | 35.6 | 25.4 | |
| Tumor localization | 0.16 | ||
| Skull base | 57.5 | 44.1 | |
| Non-skull base | 32.8 | 15.9 | |
| Sinus invasion | 0.34 | ||
| Present | 28.4 | 12.8 | |
| Not present | 36.5 | 27.3 | |
| Brain invasion | 0.74 | ||
| Present | 41.8 | 25.6 | |
| Not present | 38.0 | 28.3 | |
| Simpson grade | 0.37 | ||
| Simpson grades I and II | 36.5 | 25.0 | |
| Simpson grade ≥ III | 56.0 | 52.3 | |
| WHO grade | 0.48 | ||
| 1 | 44.0 | 35.8 | |
| 2 | 33.9 | 17.6 | |
| Mitotic count (primary meningioma) | 0.82 | ||
| ≥4 | 40.6 | 27.3 | |
| <4 | 37.3 | 29.9 | |
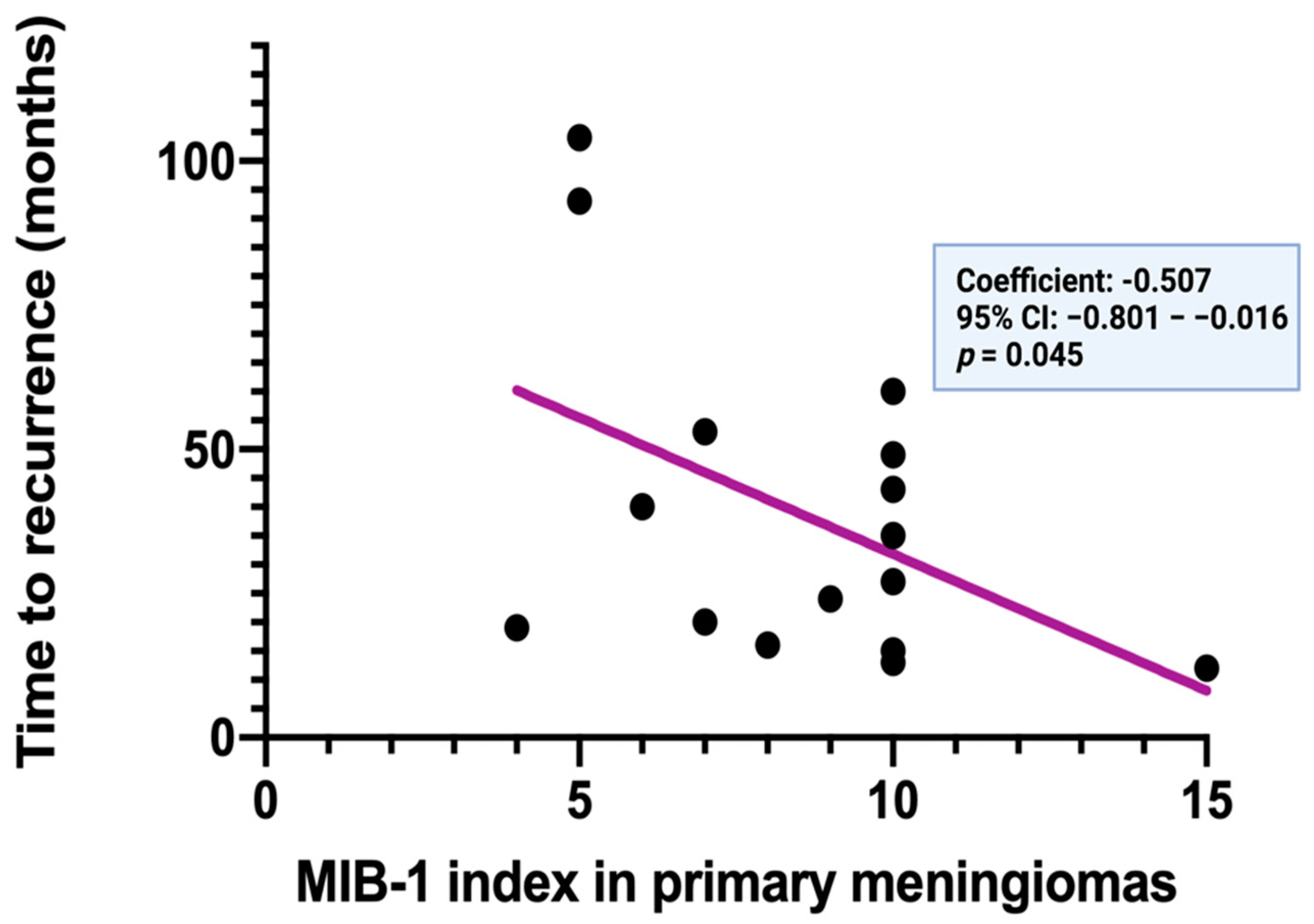
| MIB-I index (primary meningioma) | 0.04 | ||
| ≥9% | 27.6 | 16.0 | |
| <9% | 53.6 | 28.8 | |
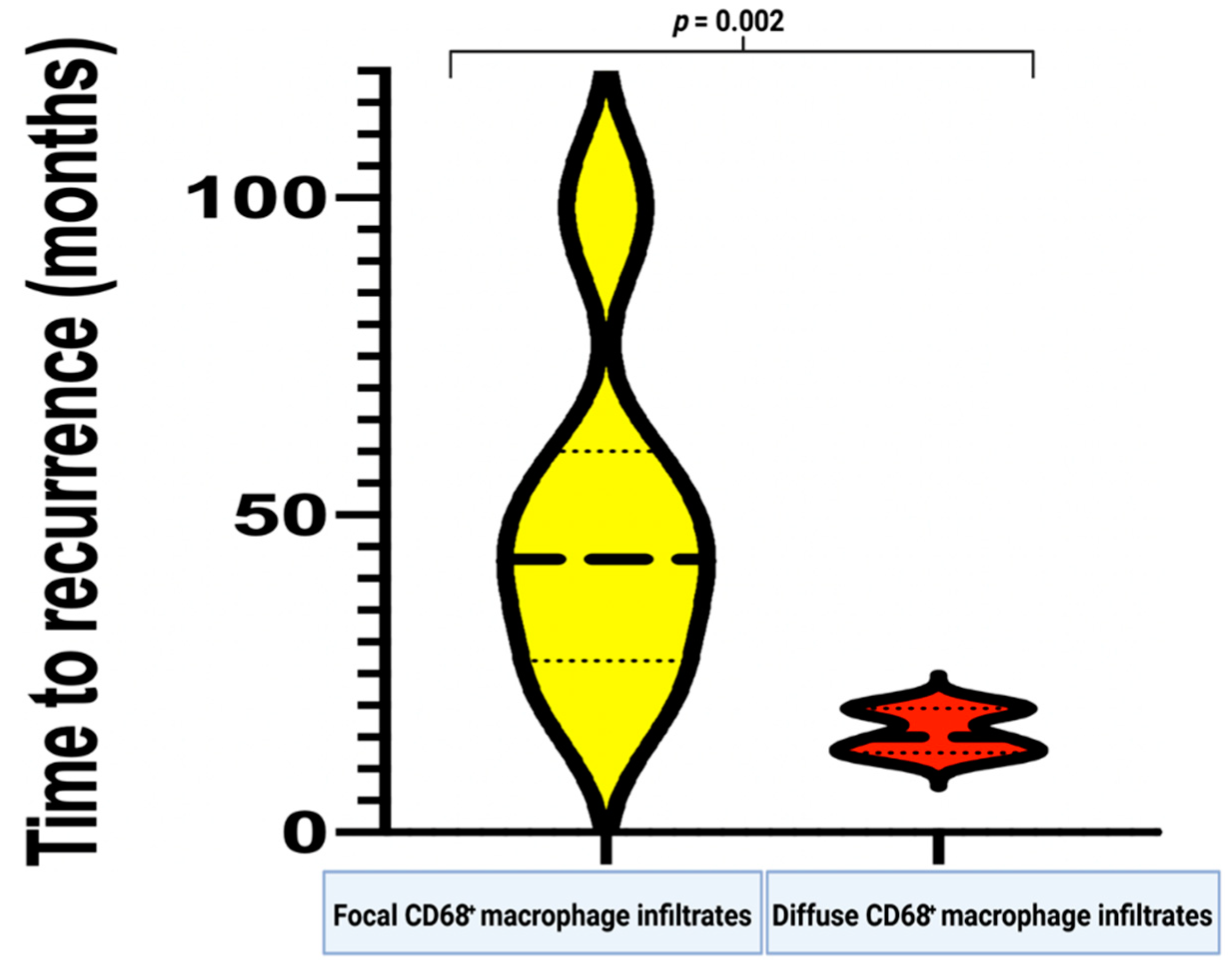
| CD68+ macrophage infiltrates (Primary meningioma) | 0.002 | ||
| Focal | 49.5 | 27.6 | |
| Diffuse | 15.8 | 3.6 |
| Variable | Smaller or Equal MIB-1 Index (n = 10) | Increased MIB-1 Index (n = 6) | p-Value |
|---|---|---|---|
| Age | 0.63 | ||
| ≥54 | 5 | 2 | |
| <54 | 5 | 4 | |
| Sex | 0.035 | ||
| Male | 2 | 5 | |
| Female | 8 | 1 | |
| Tumor volume | 0.99 | ||
| <46 cm3 | 5 | 3 | |
| ≥46 cm3 | 5 | 3 | |
| Peritumoral edema | 0.99 | ||
| Present | 8 | 3 | |
| Not present | 3 | 2 | |
| Multiple meningioma | 0.23 | ||
| Present | 4 | 0 | |
| Not present | 6 | 6 | |
| Tumor localization | 0.60 | ||
| Skull base | 2 | 2 | |
| Non-skull base | 8 | 4 | |
| Sinus invasion | 0.06 | ||
| Present | 0 | 3 | |
| Not present | 9 | 4 | |
| Brain invasion | 0.99 | ||
| Present | 0 | 2 | |
| Not present | 5 | 9 | |
| Primary MIB-1 index | 0.33 | ||
| ≥9% | 8 | 3 | |
| <9% | 3 | 4 | |
| Primary mitotic count | 0.99 | ||
| ≥4 | 5 | 3 | |
| <4 | 5 | 3 | |
| CD68+ macrophage infiltrates | 0.001 | ||
| Focal | 10 | 1 | |
| Diffuse | 0 | 5 | |
| Simpson grade | 0.63 | ||
| Simpson grades I and II | 9 | 5 | |
| Simpson grade ≥ III | 1 | 1 | |
| WHO grade | 0.61 | ||
| 1 | 6 | 2 | |
| 2 | 4 | 4 | |
| Mean serum C-reactive protein level (+/− SD) | 2.73 +/− 3.35 | 1.02 +/− 1.19 | 0.30 |
| Mean plasma fibrinogen level (+/− SD) | 3.67 +/− 0.73 | 2.23 +/− 0.38 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wach, J.; Lampmann, T.; Güresir, Á.; Vatter, H.; Herrlinger, U.; Becker, A.; Toma, M.; Hölzel, M.; Güresir, E. Inflammatory Tumor Microenvironment in Cranial Meningiomas: Clinical Implications and Intraindividual Reproducibility. Diagnostics 2022, 12, 853. https://doi.org/10.3390/diagnostics12040853
Wach J, Lampmann T, Güresir Á, Vatter H, Herrlinger U, Becker A, Toma M, Hölzel M, Güresir E. Inflammatory Tumor Microenvironment in Cranial Meningiomas: Clinical Implications and Intraindividual Reproducibility. Diagnostics. 2022; 12(4):853. https://doi.org/10.3390/diagnostics12040853
Chicago/Turabian StyleWach, Johannes, Tim Lampmann, Ági Güresir, Hartmut Vatter, Ulrich Herrlinger, Albert Becker, Marieta Toma, Michael Hölzel, and Erdem Güresir. 2022. "Inflammatory Tumor Microenvironment in Cranial Meningiomas: Clinical Implications and Intraindividual Reproducibility" Diagnostics 12, no. 4: 853. https://doi.org/10.3390/diagnostics12040853