
Diagnostic Value of IP-10 Level in Plasma and Bronchoalveolar Lavage Fluid in Children with Tuberculosis and Other Lung Diseases


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Collection and Processing of BAL and Blood Samples
2.3. Determination of IP-10 Concentration
2.4. Statistics
3. Results
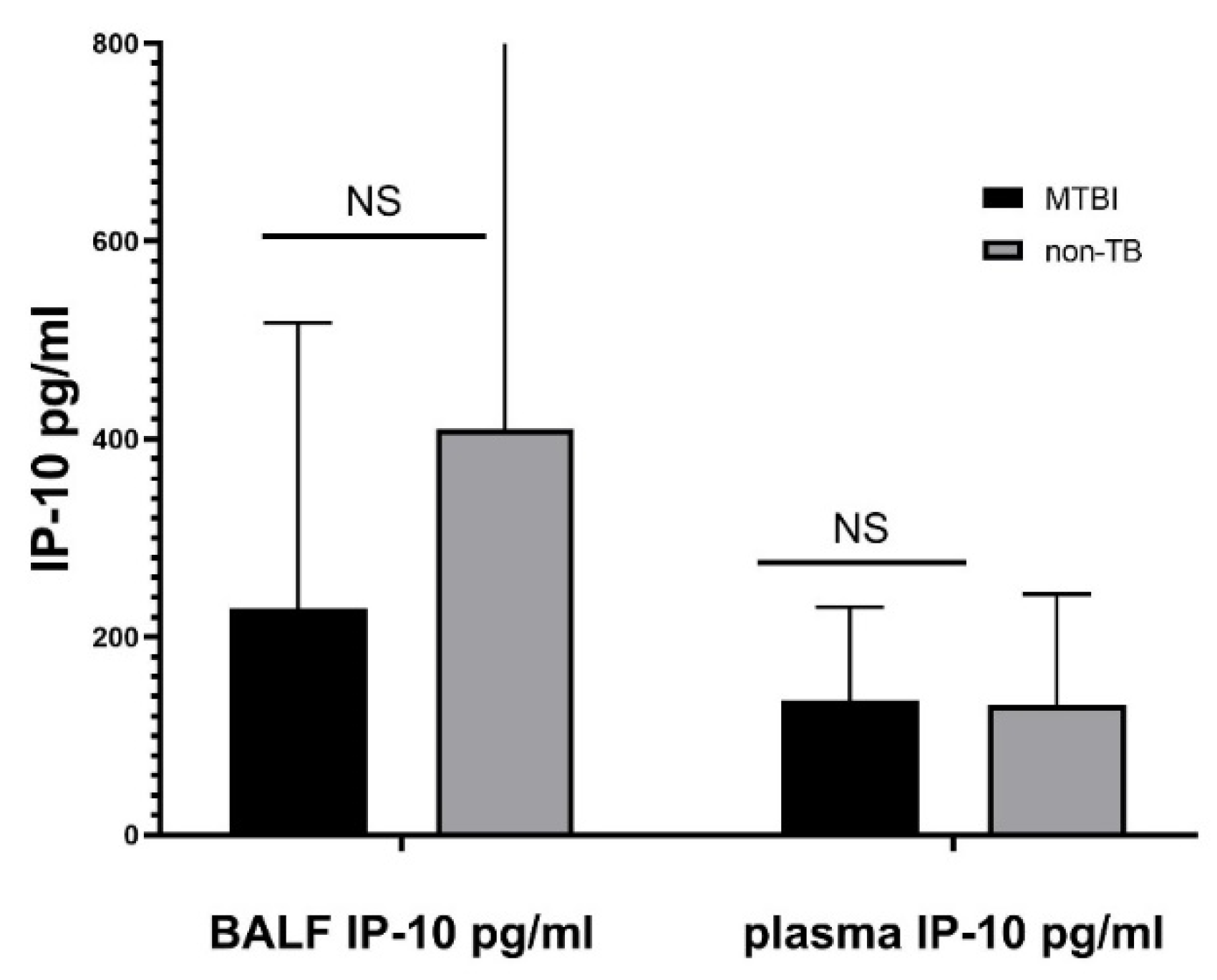
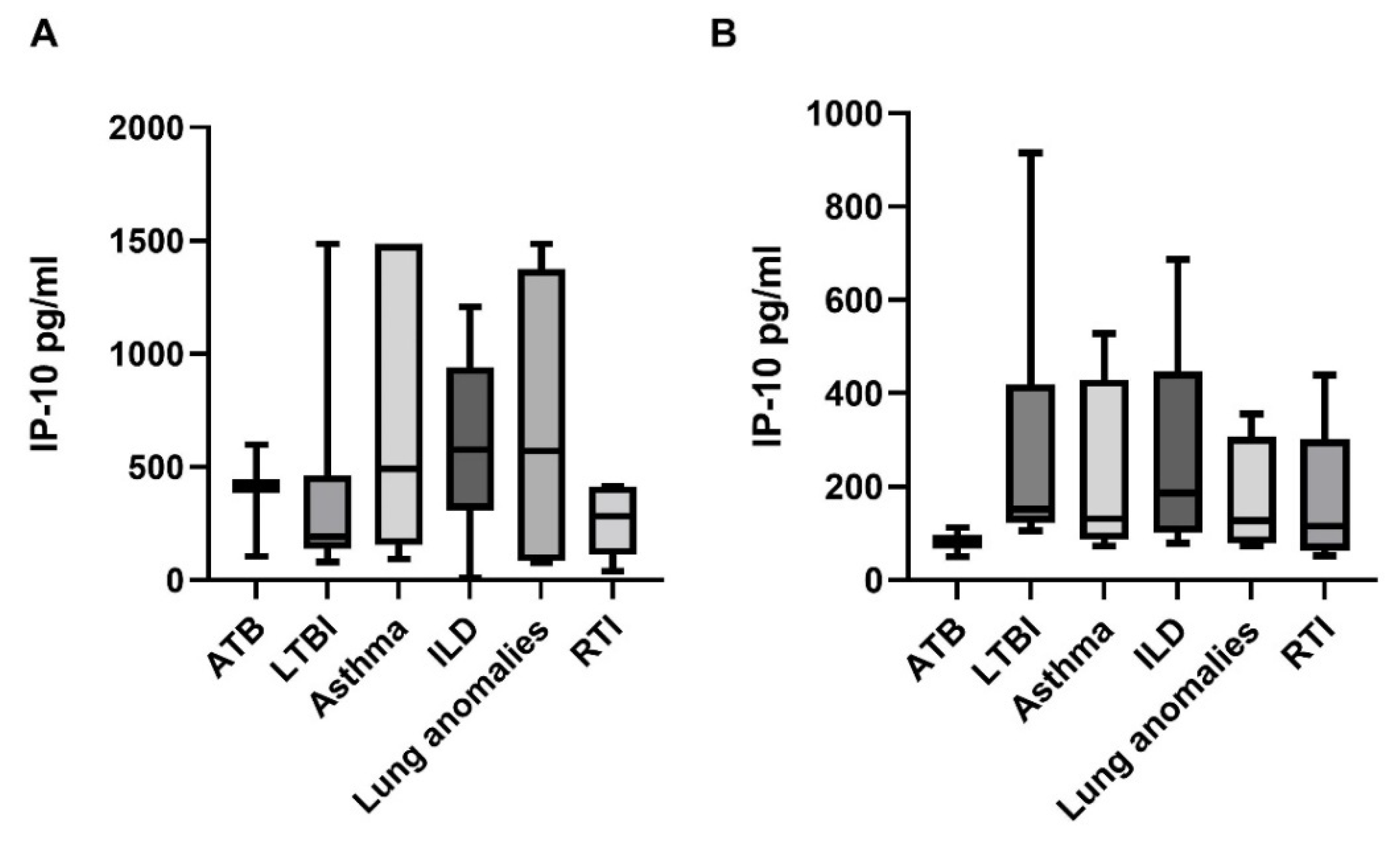
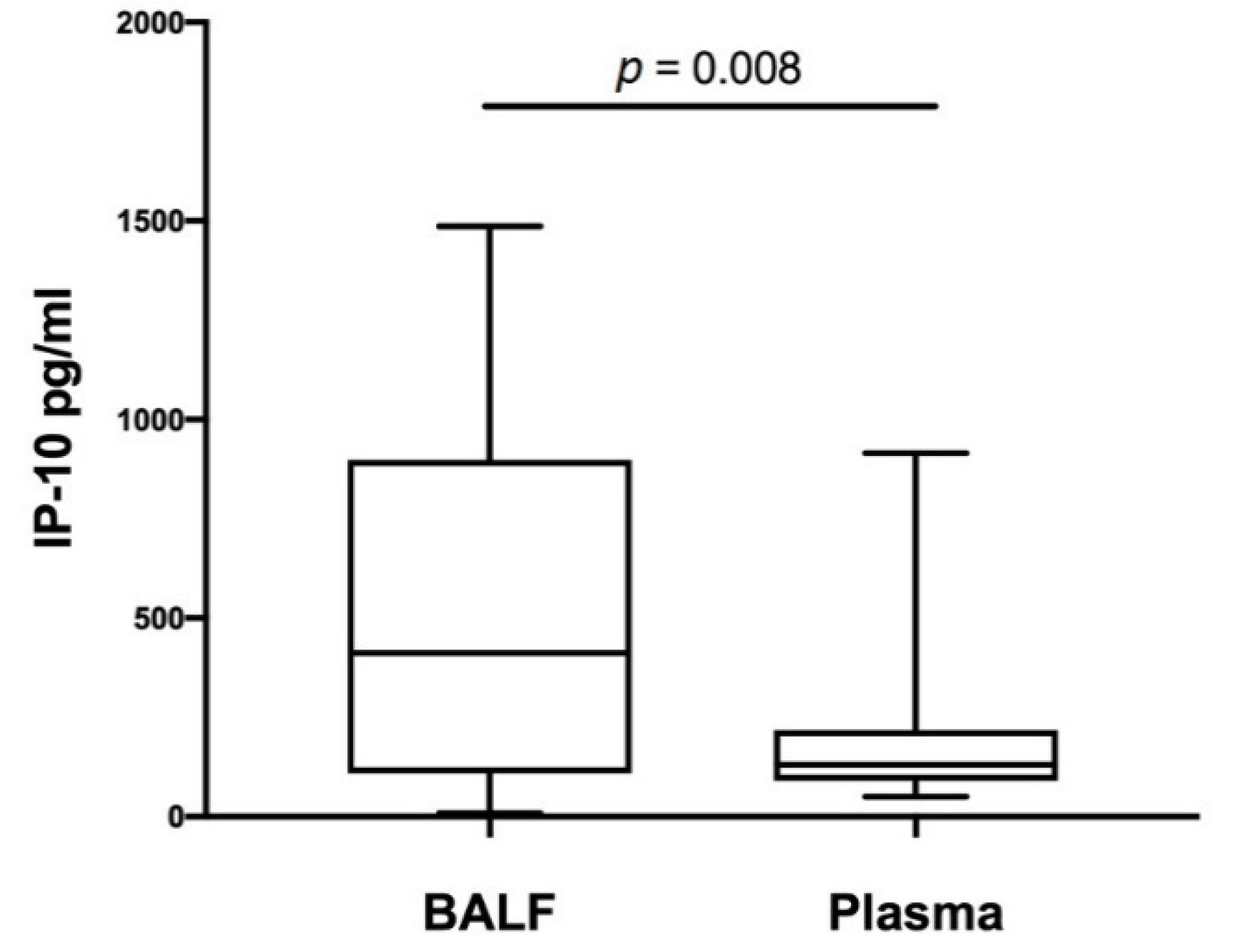
3.1. BALF and Plasma Concentrations of IP-10
3.2. Correlation of BALF and Plasma IP-10 Levels with Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; WHO: Geneva, Brussels, 2021. [Google Scholar]
- Jenkins, H.E.; Yuen, C.M.; Rodriguez, C.A.; Nathavitharana, R.R.; McLaughlin, M.M.; Donald, P.; Marais, B.J.; Becerra, M.C. Mortality in children diagnosed with tuberculosis: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Marais, B.J.; Hesseling, A.C.; Gie, R.P.; Schaaf, H.S.; Enarson, D.A.; Beyers, N. The bacteriologic yield in children with intrathoracic tuberculosis. Clin. Infect. Dis. 2006, 42, e69–e71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhat, M.; Greenaway, C.; Pai, M.; Menzies, D. False-positive tuberculin skin tests: What is the absolute effect of BCG and non-Tuberculous mycobacteria? Int. J. Tuberc. Lung Dis. 2006, 10, 1192–1204. [Google Scholar] [PubMed]
- Mancuso, J.D.; Mody, R.M.; Olsen, C.H.; Harrison, L.H.; Santosham, M.; Aronson, N.E. The Long-term Effect of Bacille Calmette-Guerin Vaccination on Tuberculin Skin Testing: A 55-Year Follow-Up Study. Chest 2017, 152, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Laurenti, P.; Raponi, M.; de Waure, C.; Marino, M.; Ricciardi, W.; Damiani, G. Performance of interferon-gamma release assays in the diagnosis of confirmed active tuberculosis in immunocompetent children: A new systematic review and meta-analysis. BMC Infect. Dis. 2016, 16, 131. [Google Scholar] [CrossRef] [Green Version]
- Mandalakas, A.M.; Detjen, A.K.; Hesseling, A.C.; Benedetti, A.; Menzies, D. Interferon-gamma release assays and childhood tuberculosis: Systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2011, 15, 1018–1032. [Google Scholar] [CrossRef]
- Chiappini, E.; Storelli, F.; Tersigni, C.; Venturini, E.; de Martino, M.; Galli, L. QuantiFERON-TB Gold In-Tube test performance in a large pediatric population investigated for suspected tuberculosis infection. Paediatr. Respir. Rev. 2019, 32, 36–47. [Google Scholar] [CrossRef]
- Hamzaoui, A.; Yaalaoui, S.; Cherif, F.T.; Saidi, L.S.; Berraies, A. Childhood tuberculosis: A concern of the modern world. Eur. Respir. Rev. 2014, 23, 278–291. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, E.; Biswas, P.; Vettoretto, K.; Ferrarini, M.; Uguccioni, M.; Piali, L.; Leone, B.E.; Moser, B.; Rugarli, C.; Pardi, R. Macrophages exposed to Mycobacterium tuberculosis release chemokines able to recruit selected leucocyte subpopulations: Focus on gammadelta cells. Immunology 2003, 108, 365–374. [Google Scholar] [CrossRef]
- Vanini, V.; Petruccioli, E.; Gioia, C.; Cuzzi, G.; Orchi, N.; Rianda, A.; Alba, L.; Giancola, M.L.; Conte, A.; Schinina, V.; et al. IP-10 is an additional marker for tuberculosis (TB) detection in HIV-infected persons in a low-TB endemic country. J. Infect. 2012, 65, 49–59. [Google Scholar] [CrossRef]
- Amanatidou, V.; Critselis, E.; Trochoutsou, A.; Soldatou, A.; Benetatou, K.; Spyridis, N.; Papadopoulos, N.G.; Tsolia, M.N. Interferon gamma inducible protein-10 in the diagnosis of paediatric tuberculosis infection in a low TB incidence country. Int. J. Tuberc. Lung Dis. 2015, 19, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Alsleben, N.; Ruhwald, M.; Russmann, H.; Marx, F.M.; Wahn, U.; Magdorf, K. Interferon-gamma inducible protein 10 as a biomarker for active tuberculosis and latent tuberculosis infection in children: A case-control study. Scand. J. Infect. Dis. 2012, 44, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Latorre, I.; Diaz, J.; Mialdea, I.; Serra-Vidal, M.; Altet, N.; Prat, C.; Diez, N.; Escribano, A.; Casas, I.; Rodrigo, C.; et al. IP-10 is an accurate biomarker for the diagnosis of tuberculosis in children. J. Infect. 2014, 69, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Ruhwald, M.; Aabye, M.G.; Ravn, P. IP-10 release assays in the diagnosis of tuberculosis infection: Current status and future directions. Expert Rev. Mol. Diagn. 2012, 12, 175–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, M.; Kawabe, T.; Iwasaki, Y.; Hara, T.; Hashimoto, N.; Imaizumi, K.; Hasegawa, Y.; Shimokata, K. Evaluation of interferon-gamma, interferon-gamma-inducing cytokines, and interferon-gamma-inducible chemokines in tuberculous pleural effusions. J. Lab. Clin. Med. 2005, 145, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Sauty, A.; Dziejman, M.; Taha, R.A.; Iarossi, A.S.; Neote, K.; Garcia-Zepeda, E.A.; Hamid, Q.; Luster, A.D. The T cell-specific CXC chemokines IP-10, Mig, and I-TAC are expressed by activated human bronchial epithelial cells. J. Immunol. 1999, 162, 3549–3558. [Google Scholar]
- Cannas, A.; Calvo, L.; Chiacchio, T.; Cuzzi, G.; Vanini, V.; Lauria, F.N.; Pucci, L.; Girardi, E.; Goletti, D. IP-10 detection in urine is associated with lung diseases. BMC Infect. Dis. 2010, 10, 333. [Google Scholar] [CrossRef] [Green Version]
- Walrath, J.; Zukowski, L.; Krywiak, A.; Silver, R.F. Resident Th1-like effector memory cells in pulmonary recall responses to Mycobacterium tuberculosis. Am. J. Respir. Cell Mol. Biol. 2005, 33, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Kibiki, G.S.; Myers, L.C.; Kalambo, C.F.; Hoang, S.B.; Stoler, M.H.; Stroup, S.E.; Houpt, E.R. Bronchoalveolar neutrophils, interferon gamma-inducible protein 10 and interleukin-7 in AIDS-associated tuberculosis. Clin. Exp. Immunol. 2007, 148, 254–259. [Google Scholar] [CrossRef] [Green Version]
- Raju, B.; Hoshino, Y.; Kuwabara, K.; Belitskaya, I.; Prabhakar, S.; Canova, A.; Gold, J.A.; Condos, R.; Pine, R.I.; Brown, S.; et al. Aerosolized gamma interferon (IFN-gamma) induces expression of the genes encoding the IFN-gamma-inducible 10-kilodalton protein but not inducible nitric oxide synthase in the lung during tuberculosis. Infect. Immun. 2004, 72, 1275–1283. [Google Scholar] [CrossRef] [Green Version]
- Nolan, A.; Condos, R.; Huie, M.L.; Dawson, R.; Dheda, K.; Bateman, E.; Rom, W.N.; Weiden, M.D. Elevated IP-10 and IL-6 from bronchoalveolar lavage cells are biomarkers of non-cavitary tuberculosis. Int. J. Tuberc. Lung Dis. 2013, 17, 922–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrone, L.; Cannas, A.; Aloi, F.; Nsubuga, M.; Sserumkuma, J.; Nazziwa, R.A.; Jugheli, L.; Lukindo, T.; Girardi, E.; Reither, K.; et al. Blood or Urine IP-10 Cannot Discriminate between Active Tuberculosis and Respiratory Diseases Different from Tuberculosis in Children. BioMed Res. Int. 2015, 2015, 589471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Blic, J.; Midulla, F.; Barbato, A.; Clement, A.; Dab, I.; Eber, E.; Green, C.; Grigg, J.; Kotecha, S.; Kurland, G.; et al. Bronchoalveolar lavage in children. ERS Task Force on bronchoalveolar lavage in children. European Respiratory Society. Eur. Respir. J. 2000, 15, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Bush, A.; Cunningham, S.; de Blic, J.; Barbato, A.; Clement, A.; Epaud, R.; Hengst, M.; Kiper, N.; Nicholson, A.G.; Wetzke, M.; et al. European protocols for the diagnosis and initial treatment of interstitial lung disease in children. Thorax 2015, 70, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Chcialowski, A.; Chorostowska-Wynimko, J.; Fal, A.; Pawlowicz, R.; Domagala-Kulawik, J. Recommendation of the Polish Respiratory Society for bronchoalveolar lavage (BAL) sampling, processing and analysis methods. Pneumonol. Alergol. Pol. 2011, 79, 75–89. [Google Scholar]
- Ruhwald, M.; Bodmer, T.; Maier, C.; Jepsen, M.; Haaland, M.B.; Eugen-Olsen, J.; Ravn, P. Evaluating the potential of IP-10 and MCP-2 as biomarkers for the diagnosis of tuberculosis. Eur. Respir. J. 2008, 32, 1607–1615. [Google Scholar] [CrossRef] [Green Version]
- Ruhwald, M.; Dominguez, J.; Latorre, I.; Losi, M.; Richeldi, L.; Pasticci, M.B.; Mazzolla, R.; Goletti, D.; Butera, O.; Bruchfeld, J.; et al. A multicentre evaluation of the accuracy and performance of IP-10 for the diagnosis of infection with M. tuberculosis. Tuberculosis 2011, 91, 260–267. [Google Scholar] [CrossRef]
- Holm, L.L.; Rose, M.V.; Kimaro, G.; Bygbjerg, I.C.; Mfinanga, S.G.; Ravn, P.; Ruhwald, M. A comparison of interferon-gamma and IP-10 for the diagnosis of tuberculosis. Pediatrics 2014, 134, e1568–e1575. [Google Scholar] [CrossRef] [Green Version]
- Whittaker, E.; Gordon, A.; Kampmann, B. Is IP-10 a better biomarker for active and latent tuberculosis in children than IFNgamma? PLoS ONE 2008, 3, e3901. [Google Scholar] [CrossRef] [Green Version]
- Lighter, J.; Rigaud, M.; Huie, M.; Peng, C.H.; Pollack, H. Chemokine IP-10: An adjunct marker for latent tuberculosis infection in children. Int. J. Tuberc. Lung Dis. 2009, 13, 731–736. [Google Scholar]
- Chegou, N.N.; Detjen, A.K.; Thiart, L.; Walters, E.; Mandalakas, A.M.; Hesseling, A.C.; Walzl, G. Utility of host markers detected in Quantiferon supernatants for the diagnosis of tuberculosis in children in a high-burden setting. PLoS ONE 2013, 8, e64226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzurri, A.; Sow, O.Y.; Amedei, A.; Bah, B.; Diallo, S.; Peri, G.; Benagiano, M.; D’Elios, M.M.; Mantovani, A.; Del Prete, G. IFN-gamma-inducible protein 10 and pentraxin 3 plasma levels are tools for monitoring inflammation and disease activity in Mycobacterium tuberculosis infection. Microbes Infect. 2005, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Petrone, L.; Chiacchio, T.; Vanini, V.; Petruccioli, E.; Cuzzi, G.; Di Giacomo, C.; Pucci, L.; Montalbano, M.; Lionetti, R.; Testa, A.; et al. High urine IP-10 levels associate with chronic HCV infection. J. Infect. 2014, 68, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Puapatanakul, P.; Chansritrakul, S.; Susantitaphong, P.; Ueaphongsukkit, T.; Eiam-Ong, S.; Praditpornsilpa, K.; Kittanamongkolchai, W.; Avihingsanon, Y. Interferon-Inducible Protein 10 and Disease Activity in Systemic Lupus Erythematosus and Lupus Nephritis: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 4954. [Google Scholar] [CrossRef] [Green Version]
- Miotto, D.; Christodoulopoulos, P.; Olivenstein, R.; Taha, R.; Cameron, L.; Tsicopoulos, A.; Tonnel, A.B.; Fahy, O.; Lafitte, J.J.; Luster, A.D.; et al. Expression of IFN-gamma-inducible protein; monocyte chemotactic proteins 1, 3, and 4; and eotaxin in TH1- and TH2-mediated lung diseases. J. Allergy Clin. Immunol. 2001, 107, 664–670. [Google Scholar] [CrossRef]
- Husain, S.; Resende, M.R.; Rajwans, N.; Zamel, R.; Pilewski, J.M.; Crespo, M.M.; Singer, L.G.; McCurry, K.R.; Kolls, J.K.; Keshavjee, S.; et al. Elevated CXCL10 (IP-10) in bronchoalveolar lavage fluid is associated with acute cellular rejection after human lung transplantation. Transplantation 2014, 97, 90–97. [Google Scholar] [CrossRef]
- Solomon, G.M.; Frederick, C.; Zhang, S.; Gaggar, A.; Harris, T.; Woodworth, B.A.; Steele, C.; Rowe, S.M. IP-10 is a potential biomarker of cystic fibrosis acute pulmonary exacerbations. PLoS ONE 2013, 8, e72398. [Google Scholar] [CrossRef] [Green Version]
- Augustynowicz-Kopeć, E.D.U.; Grzelewska-Rzymowska, I.; Korzeniewska-Koseła, M.; Langfort, R.; Michałowska-Mitczuk, D.; Rowińska-Zakrzewska, E.; Zielonka, T.M.; Ziołkowski, J.; Zwolska, Z. Zalecenia Polskiego Towarzystwa Chorób Płuc dotyczące rozpoznawania, leczenia i zapobiegania gruźlicy u dorosłych i dzieci. Pneumonol. Alergol. Pol. 2013, 81, 323–379. [Google Scholar]
- Erkens, C.G.; Kamphorst, M.; Abubakar, I.; Bothamley, G.H.; Chemtob, D.; Haas, W.; Migliori, G.B.; Rieder, H.L.; Zellweger, J.P.; Lange, C. Tuberculosis contact investigation in low prevalence countries: A European consensus. Eur. Respir. J. 2010, 36, 925–949. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Group | Control Group | |||||
|---|---|---|---|---|---|---|
| n = 13 (%) | Total n = 22 (%) | Asthma n = 5 (%) | ILD n = 6 (%) | Lung Anomalies n = 4 (%) | RTI n = 7 (%) | |
| Sex | ||||||
| Females | 10 (77) | 12 (55) | 2 (40) | 3 (50) | 2 (50) | 5 (71) |
| Males | 3 (23) | 10 (45) | 3 (60) | 3 (50) | 2 (50) | 2 (29) |
| Age (yrs), median (IQR) | 5 (4–6) | 7 (4–12) | 12 (6–13) | 10 (3–12) | 6 (4–10.5) | 6 (2–9) |
| ≤5 yrs | 5 (38) | 6 (27) | 0 (0) | 2 (33) | 1 (25) | 3 (43) |
| 0–2 yrs | 0 (0) | 1 (5) | 0 (0) | 2 (33) | 0 (0) | 0 (0) |
| Origin | ||||||
| Poland | 13 (100) | 22 (100) | 5 (100) | 6 (100) | 4 (100) | 7 (100) |
| BMI | ||||||
| 3–97 percentile | 13 (100) | 22 (100) | 5 (100) | 6 (100) | 4 (100) | 7 (100) |
| BCG vaccinated | ||||||
| Yes | 13 (100) | 22 (100) | 5 (100) | 6 (100) | 4 (100) | 7 (100) |
| BCG scar | ||||||
| Present | 11 (85) | 19 (86) | 4 (80) | 5 (83) | 4 (100) | 6 (86) |
| Not recorded | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| TST | ||||||
| TST-positive | 12 (92) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| TST-negative | 1 (8) | 5 (23) | 1 (20) | 0 (0) | 1 (25) | 3 (43) |
| TST not performed | 0 (0) | 17 (77) | 4 (80) | 6 (100) | 3 (75) | 4 (57) |
| QFT | ||||||
| QFT-positive | 7 (54) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| QFT-negative | 1 (8) | 4 (18) | 1 (20) | 0 (0) | 0 (0) | 3 (43) |
| QFT-indeterminate | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| QFT Not performed | 5 (38) | 18 (82) | 4 (80) | 6 (100) | 4 (100) | 4 (57) |
| Known TB contact | ||||||
| Yes | 13 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| No | 0 (0) | 22 (100) | 5 (100) | 6 (100) | 4 (100) | 7 (100) |
| Index case | ||||||
| Smear–positive | 10 (77) | n/A | n/A | n/A | n/A | n/A |
| Smear–negative | 1 (8) | n/A | n/A | n/A | n/A | n/A |
| Not known | 2 (15) | n/A | n/A | n/A | n/A | n/A |
| TB diagnosis | ||||||
| Microbiological | 0 (0) | n/A | n/A | n/A | n/A | n/A |
| Clinical | 3 (100) | n/A | n/A | n/A | n/A | n/A |
| Clinical symptoms | 2 (66) | n/A | n/A | n/A | n/A | n/A |
| Chest X-ray abnormalities | 2 (66) | n/A | n/A | n/A | n/A | n/A |
| Abnormal bronchofiberoscopy | 3 (100) | n/A | n/A | n/A | n/A | n/A |
| IP-10 measured in BALF | 13 (100) | 22 (100) | 5 (100) | 6 (100) | 4 (100) | 7 (100) |
| IP-10 measured in plasma | 8 (62) | 18 (82) | 4 (80) | 5 (83) | 4 (100) | 5 (71) |
| BALF Recovery (%) | BALF Cell Count, 103/mL | Macrophages (%) | Lymphocytes (%) | Neutrophils (%) | Eosinophils (%) | |
|---|---|---|---|---|---|---|
| Mtb.-infected | 53 (49.4–63) | 155 (107–293) | 52 (49.4–64) | 44 (31.7–45) | 4 (3.0–4) | 0 (0.2–1) |
| ATB | 56 (50–61) | 129 (81–177) | 64 (36–65) | 32 (15–61) | 4 (3–20) | 0 (0–1) |
| LTBI | 50 (49–64) | 271 (133–410) | 51 (49–52) | 45 (44–45) | 4 (3–4) | 1 (0–2) |
| Non-TB | 62 (50–74) | 225 (107–355) | 72 (54–79) | 16 (13–26) | 5 (2–17) | 0 (0–1) |
| Asthma | 59 (54–65) | 187.5 (107–290) | 78 (61–82) | 15 (15–33) | 5 (3–7) | 0 (0–1) |
| ILD | 61 (60.0–74) | 341 (131.8–687.5) | 73 (66–87) | 18 (8–27) | 2 (0–5) | 0 (0–0) |
| Lung anomalies | 73 (60–78) | 313 (286.7–340) | 40 (24–56) | 12 (8–17) | 46 (26–66) | 2 (1–3) |
| RTI | 56.7 (42.2–68) | 78 (60–230.7) | 71 (52.7–76) | 21 (14.3–26) | 13 (5.9–16) | 0 (0.1–3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strzelak, A.; Komorowska-Piotrowska, A.; Krenke, K.; Zagórska, W.; Bartosiewicz, W.; Feleszko, W.; Kulus, M. Diagnostic Value of IP-10 Level in Plasma and Bronchoalveolar Lavage Fluid in Children with Tuberculosis and Other Lung Diseases. Diagnostics 2022, 12, 840. https://doi.org/10.3390/diagnostics12040840
Strzelak A, Komorowska-Piotrowska A, Krenke K, Zagórska W, Bartosiewicz W, Feleszko W, Kulus M. Diagnostic Value of IP-10 Level in Plasma and Bronchoalveolar Lavage Fluid in Children with Tuberculosis and Other Lung Diseases. Diagnostics. 2022; 12(4):840. https://doi.org/10.3390/diagnostics12040840
Chicago/Turabian StyleStrzelak, Agnieszka, Anna Komorowska-Piotrowska, Katarzyna Krenke, Wioletta Zagórska, Witold Bartosiewicz, Wojciech Feleszko, and Marek Kulus. 2022. "Diagnostic Value of IP-10 Level in Plasma and Bronchoalveolar Lavage Fluid in Children with Tuberculosis and Other Lung Diseases" Diagnostics 12, no. 4: 840. https://doi.org/10.3390/diagnostics12040840