
Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading, and Characterization of Prostate Cancer: A Systematic Review


Abstract
:1. Introduction
1.1. Prostate Cancer
1.2. Prostate Imaging Reporting and Data System
1.3. Sequences for Prostate MRI
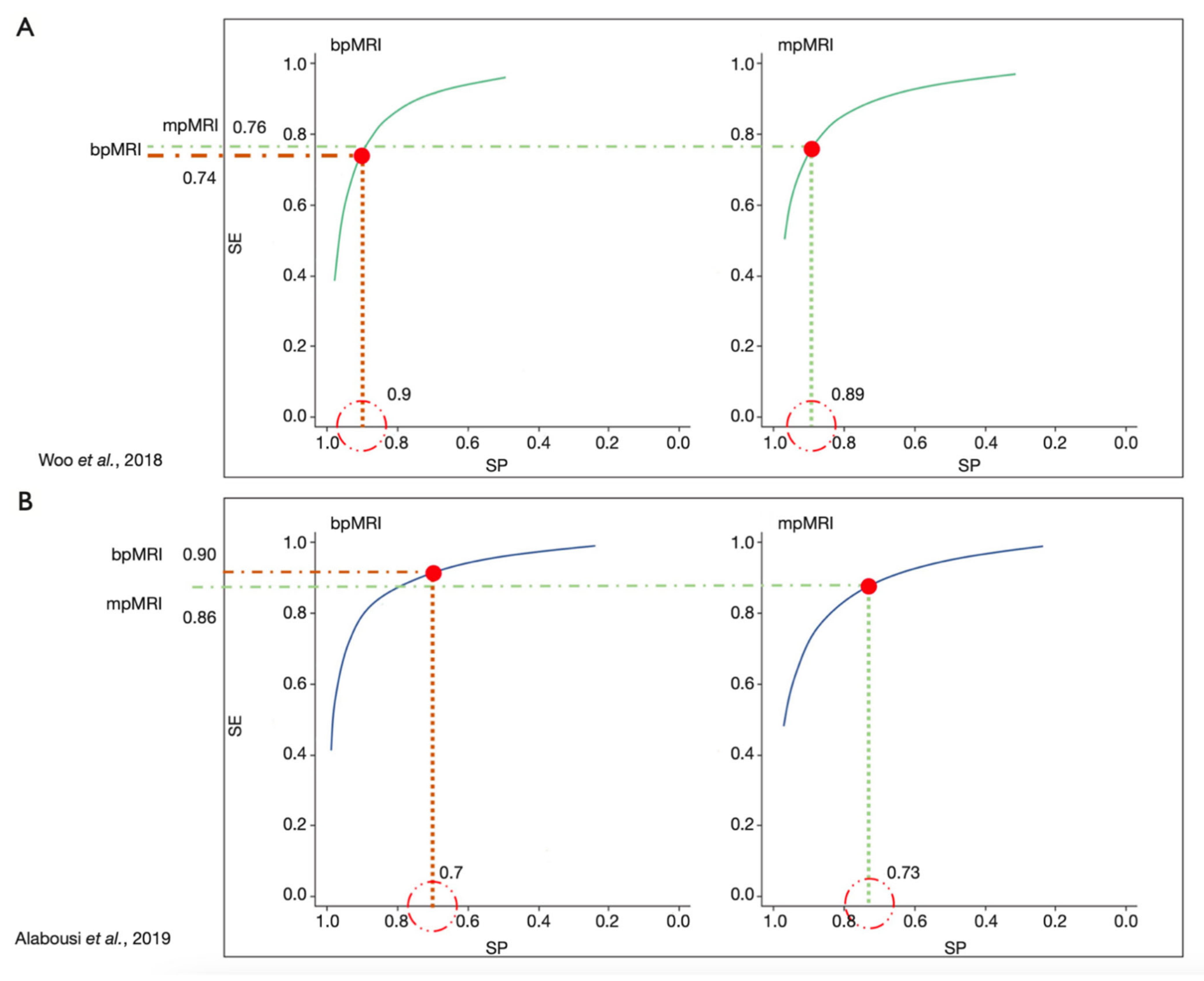
1.4. Multiparametric and Biparametric MRI of the Prostate
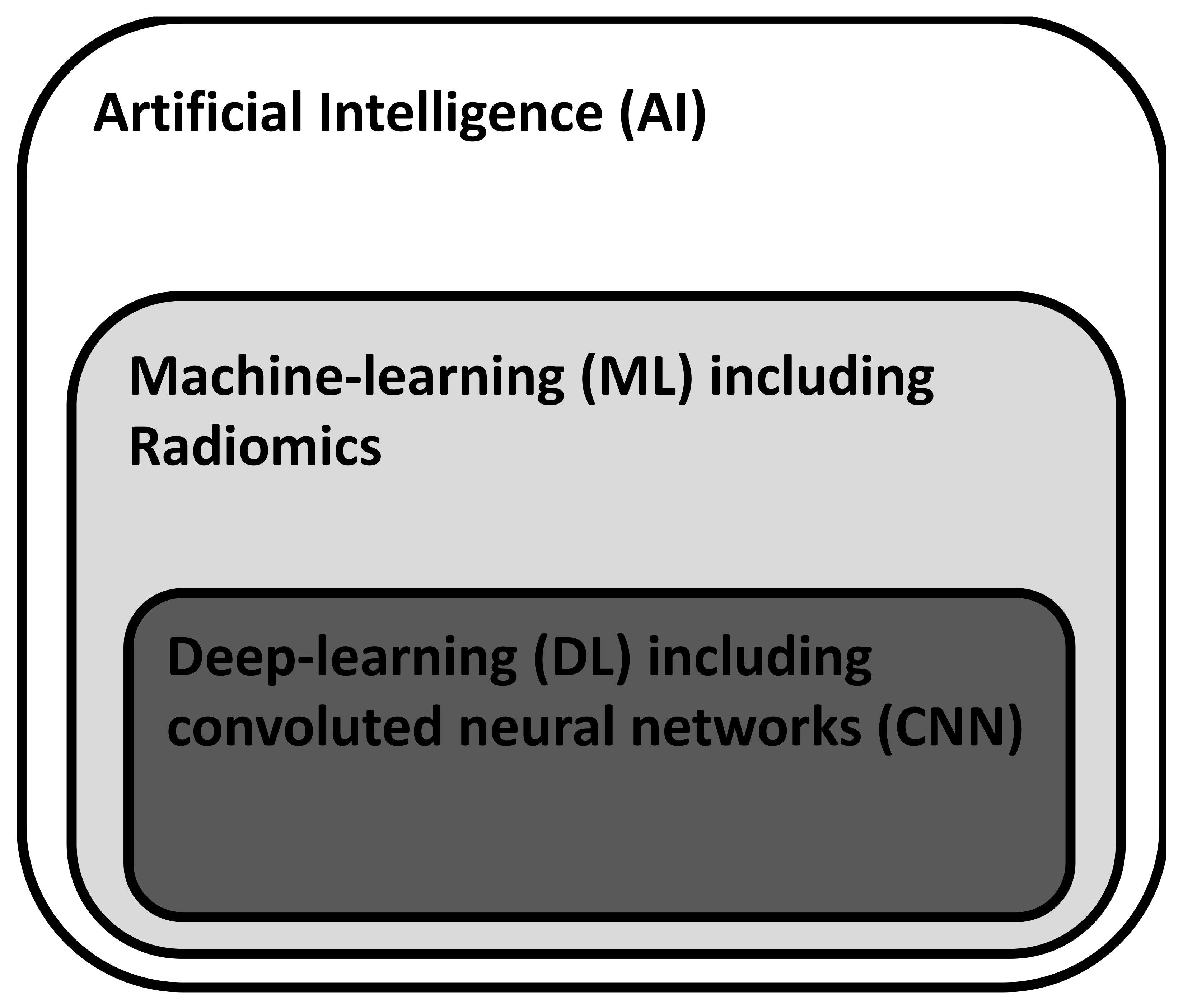
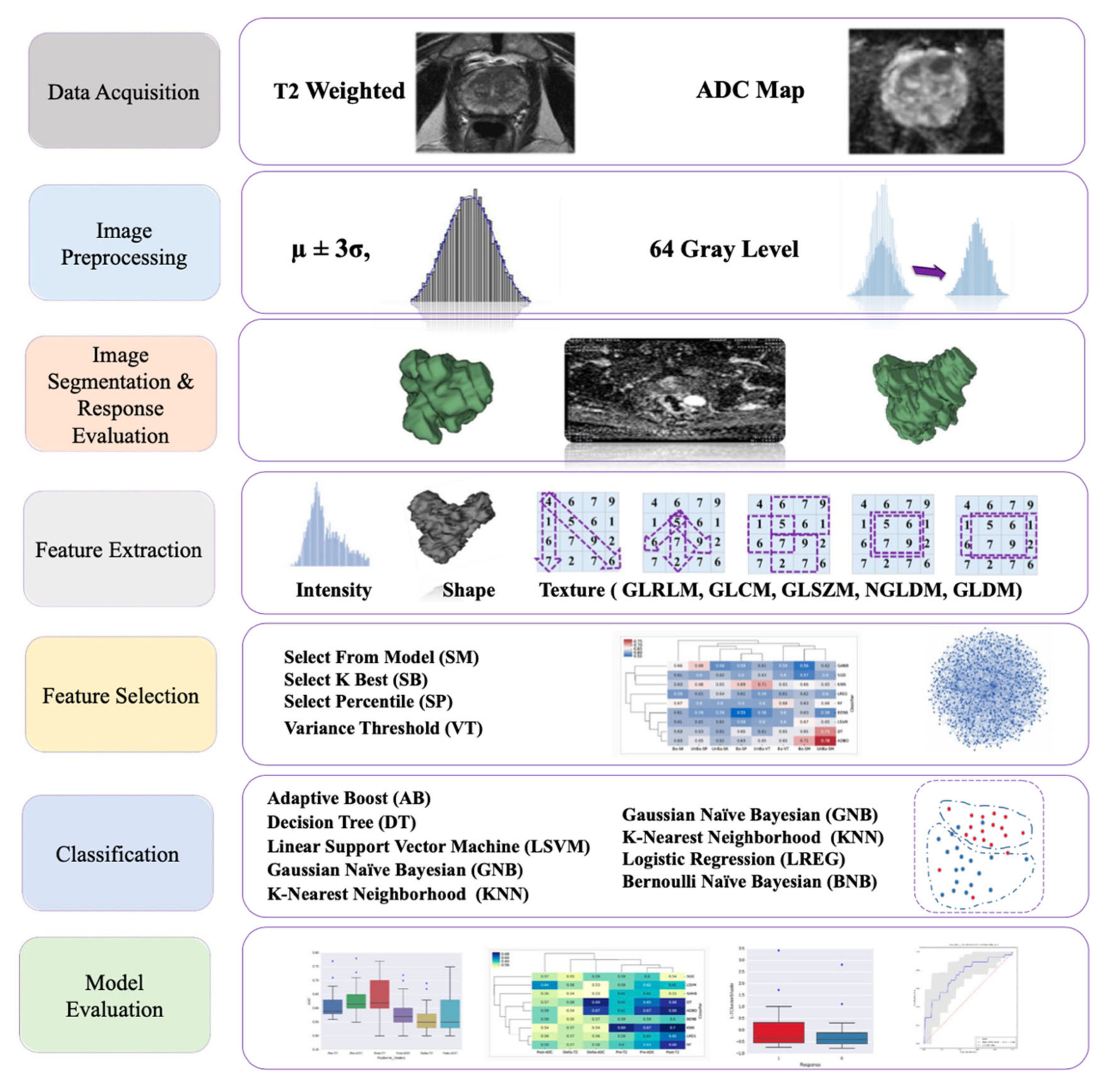
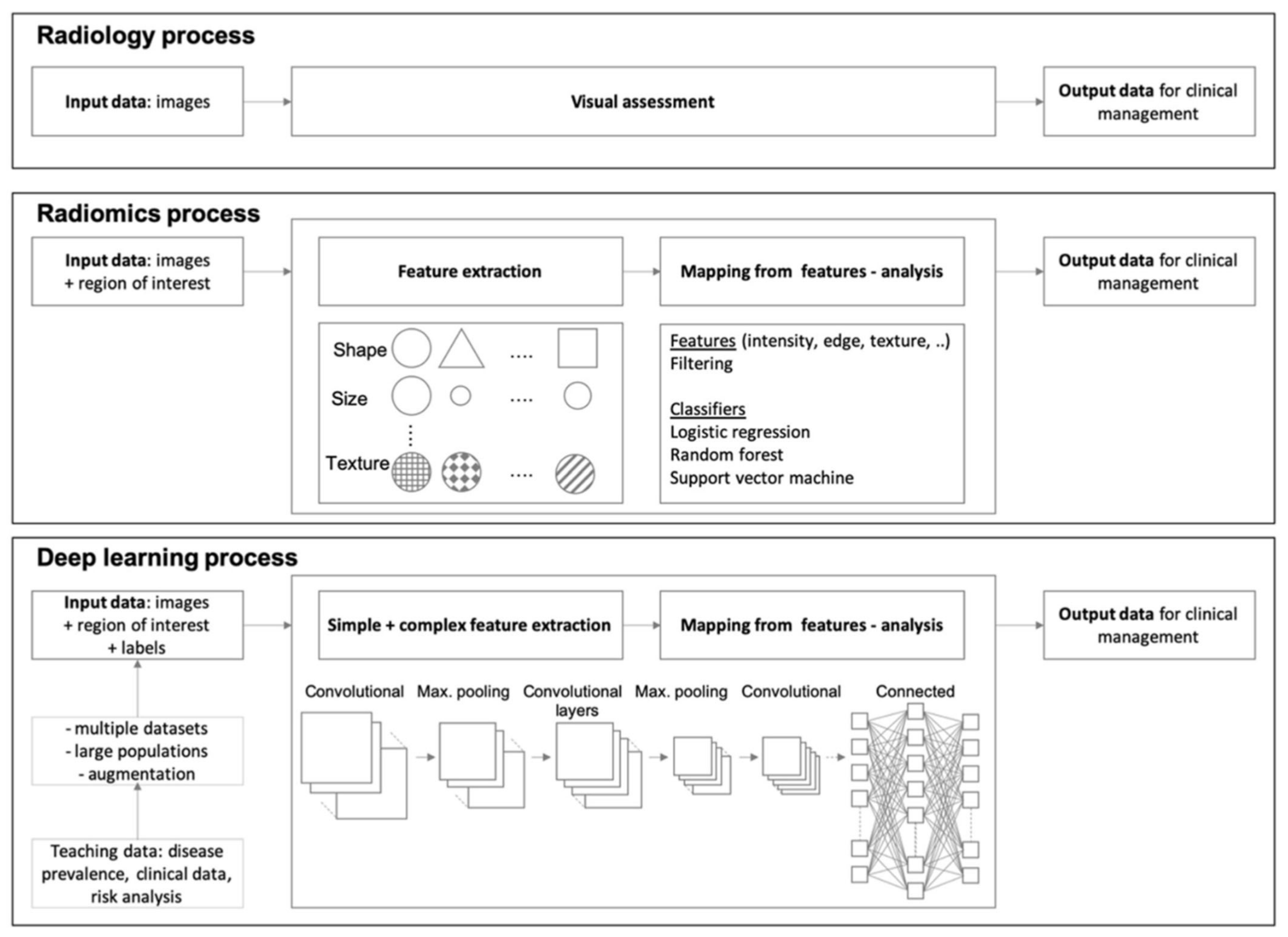
1.5. Artificial Intelligence (AI) for Image Postprocessing
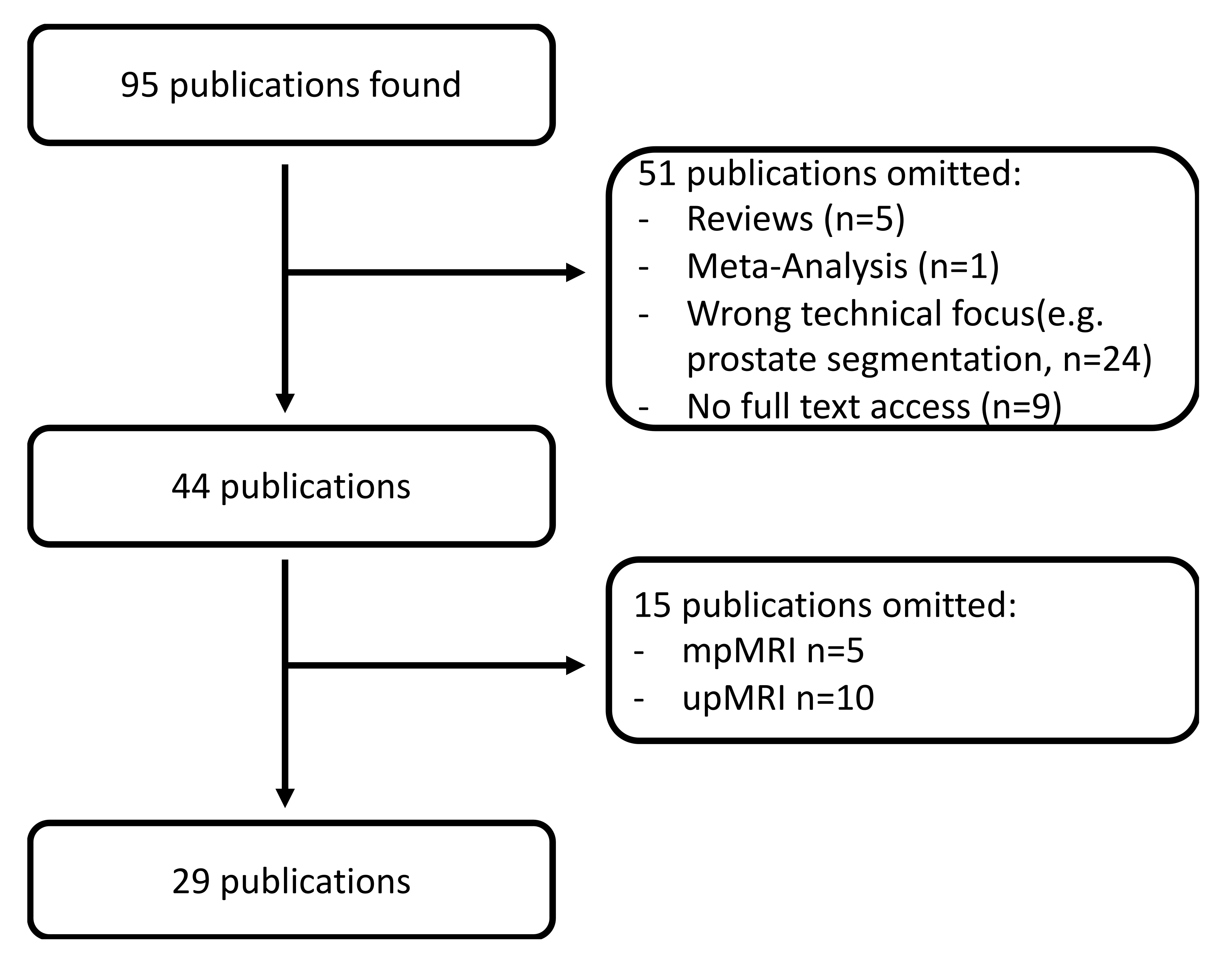
2. Materials and Methods
3. Results
3.1. Tumor Detection and Grading
3.2. PIRADS 3 Lesions
3.3. Extracapsular Extension and Biochemical Recurrence
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACR | American College of Radiology |
| ADC | Apparent Diffusion Coefficient |
| AFMS | Anterior Fibromuscular Stroma (of the Prostate) |
| AI | Artificial Intelligence |
| AS | Anterior stroma (of the Prostate) |
| AUC | Area under the Curve |
| BCR | Biochemical Recurrence |
| bp | bi-parametric |
| BPH | Benign Prostate Hyperplasia |
| ciPCA | Clinically Insignificant Prostate Cancer |
| CNN | Convoluted Neural Network |
| csPCA | Clinically Significant Prostate Cancer |
| CZ | Central Zone (of the Prostate) |
| DCE | Dynamic Contrast-Enhanced Imaging |
| DL | Deep-Learning |
| DRE | Digital Rectal Examination |
| DWI | Diffusion-Weighted Imaging |
| ECE | Extracapsular Extension |
| ESUR | European Society of Urologic Radiology |
| GS | Gleason Score |
| HBV | High b-Value (of DWI) |
| IMRT | Intensity-Modulated Radiation Therapy |
| ML | Machine-Learning |
| mp | multi-parametric |
| MR | Magnetic Resonance |
| MRI | Magnetic Resonance Imaging |
| nsPCA | Non-Significant Prostate Cancer |
| PZ | Peripheral Zone (of the Prostate) |
| PCA | Prostate Cancer |
| PIRADS | Prostate Imaging Reporting and Data System |
| PSM | Positive Surgical Margins |
| RP | Radical Prostatectomy |
| T2w | T2-weighted Imaging |
| TSE | TurboSpinEcho |
| TZ | Transitional Zone (of the Prostate) |
| up | uni-parametric |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRISMA Item | Description |
|---|---|
| Title | Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading and Characterization of Prostate Cancer: a systematic review. |
| Main objective | Assessing the current value of deep-learning and machine-learning applied to biparametric MRI of the prostate |
| Inclusion and exclusion criteria | Inclusion criteria:
|
| Information source and access time | PubMed query in August 2021 |
| Methods to assess risk of bias in included studies | No structured program was used to assess bias in study selection. Internal review by the authors and critical appraisal of the data was performed. |
| Methods to present and synthesize results | Descriptive statistics, listing in tabular form |
| Number of studies and participants included | 29 publications included 7466 participants included |
| Main outcomes | Very heterogenous data did not allow for a general interpretation of all studies. Tumor detection and grading with machine-learning and deep-learning techniques is feasible in trials and shows promising results. Reported values for AUC ranging from 0.71 to 0.999. In studies comparing human radiologists to deep-learning algorithms comparable, statistically not different results for tumor detection were found. |
| Limitations |
|
| General interpretation | Detection of clinically significant prostate cancer and differentiation of prostate cancer from non-cancerous tissue using machine-learning and deep learning is feasible with promising results. Some techniques of machine-learning and deep-learning currently seem to be equally good as human radiologists in terms of classification of single lesions according to the PIRADS score. |
| Primary source for funding | No general funding. Publication costs are covered by the Universtiy of Pisa, Pisa, Italy. |
| Register name and registration number | No registration |
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Center, M.M.; DeSantis, C.; Ward, E.M. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1893–1907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Autier, P.; Boniol, M.; Heanue, M.; Colombet, M.; Boyle, P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann. Oncol. 2007, 18, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Barone, B.; Caputo, V.F.; Fontana, M.; de Cobelli, O.; Ferro, M. BRCA Germline Mutations in Prostate Cancer: The Future Is Tailored. Diagnostics 2021, 11, 908. [Google Scholar] [CrossRef] [PubMed]
- Brookman-May, S.D.; Campi, R.; Henríquez, J.D.S.; Klatte, T.; Langenhuijsen, J.F.; Brausi, M.; Linares-Espinós, E.; Volpe, A.; Marszalek, M.; Akdogan, B.; et al. Latest Evidence on the Impact of Smoking, Sports, and Sexual Activity as Modifiable Lifestyle Risk Factors for Prostate Cancer Incidence, Recurrence, and Progression: A Systematic Review of the Literature by the European Association of Urology Section of Oncological Urology (ESOU). Eur. Urol. Focus. 2019, 5, 756–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drudi, F.M.; Cantisani, V.; Angelini, F.; Ciccariello, M.; Messineo, D.; Ettorre, E.; Liberatore, M.; Scialpi, M. Multiparametric MRI Versus Multiparametric US in the Detection of Prostate Cancer. Anticancer Res. 2019, 39, 3101–3110. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Friend, C.; Dreher, A.; Allgar, V.; Macleod, U. The diagnostic test accuracy of rectal examination for prostate cancer diagnosis in symptomatic patients: A systematic review. BMC Fam. Pract. 2018, 19, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naji, L.; Randhawa, H.; Sohani, Z.; Dennis, B.; Lautenbach, D.; Kavanagh, O.; Bawor, M.; Banfield, L.; Profetto, J. Digital Rectal Examination for Prostate Cancer Screening in Primary Care: A Systematic Review and Meta-Analysis. Ann. Fam. Med. 2018, 16, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Pokorny, M.R.; de Rooij, M.; Duncan, E.; Schröder, F.H.; Parkinson, R.; Barentsz, J.O.; Thompson, L.C. Prospective study of diagnostic accuracy comparing prostate cancer detection by transrectal ultrasound-guided biopsy versus magnetic resonance (MR) imaging with subsequent MR-guided biopsy in men without previous prostate biopsies. Eur. Urol. 2014, 66, 22–29. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Fütterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef] [Green Version]
- Spak, D.A.; Plaxco, J.S.; Santiago, L.; Dryden, M.J.; Dogan, B.E. BI-RADS® fifth edition: A summary of changes. Diagn. Interv. Imaging 2017, 98, 179–190. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging-Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Thompson, J.E.; van Leeuwen, P.J.; Moses, D.; Shnier, R.; Brenner, P.; Delprado, W.; Pulbrook, M.; Böhm, M.; Haynes, A.M.; Hayen, A.; et al. The Diagnostic Performance of Multiparametric Magnetic Resonance Imaging to Detect Significant Prostate Cancer. J. Urol. 2016, 195, 1428–1435. [Google Scholar] [CrossRef]
- Vargas, H.A.; Hötker, A.M.; Goldman, D.A.; Moskowitz, C.S.; Gondo, T.; Matsumoto, K.; Ehdaie, B.; Woo, S.; Fine, S.W.; Reuter, V.E.; et al. Updated prostate imaging reporting and data system (PIRADS v2) recommendations for the detection of clinically significant prostate cancer using multiparametric MRI: Critical evaluation using whole-mount pathology as standard of reference. Eur. Radiol. 2016, 26, 1606–1612. [Google Scholar] [CrossRef] [Green Version]
- Kasel-Seibert, M.; Lehmann, T.; Aschenbach, R.; Guettler, F.V.; Abubrig, M.; Grimm, M.O.; Teichgraeber, U.; Franiel, T. Assessment of PI-RADS v2 for the Detection of Prostate Cancer. Eur. J. Radiol. 2016, 85, 726–731. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, P.; Manetta, R.; Izzo, A.; Bruno, F.; Arrigoni, F.; de Filippo, M.; Splendiani, A.; di Cesare, E.; Masciocchi, C.; Barile, A. Biparametric (bp) and multiparametric (mp) magnetic resonance imaging (MRI) approach to prostate cancer disease: A narrative review of current debate on dynamic contrast enhancement. Gland. Surg. 2020, 9, 2235–2247. [Google Scholar] [CrossRef]
- Michaely, H.J.; Thomsen, H.S.; Reiser, M.F.; Schoenberg, S.O. Nephrogenic systemic fibrosis (NSF)—implications for radiology. Radiologe 2007, 47, 785–793. [Google Scholar] [CrossRef]
- Grobner, T. Gadolinium--a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol. Dial. Transplant. 2006, 21, 1104–1108. [Google Scholar] [CrossRef] [Green Version]
- Alkhunizi, S.M.; Fakhoury, M.; Abou-Kheir, W.; Lawand, N. Gadolinium Retention in the Central and Peripheral Nervous System: Implications for Pain, Cognition, and Neurogenesis. Radiology 2020, 297, 407–416. [Google Scholar] [CrossRef]
- Radbruch, A.; Weberling, L.D.; Kieslich, P.J.; Eidel, O.; Burth, S.; Kickingereder, P.; Heiland, S.; Wick, W.; Schlemmer, H.P.; Bendszus, M. Gadolinium retention in the dentate nucleus and globus pallidus is dependent on the class of contrast agent. Radiology 2015, 275, 783–791. [Google Scholar] [CrossRef]
- Strickler, S.E.; Clark, K.R. Gadolinium Deposition: A Study Review. Radiol. Technol. 2021, 92, 249–258. [Google Scholar]
- Semelka, R.C.; Ramalho, J.; Vakharia, A.; AlObaidy, M.; Burke, L.M.; Jay, M.; Ramalho, M. Gadolinium deposition disease: Initial description of a disease that has been around for a while. Magn. Reson. Imaging 2016, 34, 1383–1390. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Alabousi, M.; Salameh, J.P.; Gusenbauer, K.; Samoilov, L.; Jafri, A.; Yu, H.; Alabousi, A. Biparametric vs multiparametric prostate magnetic resonance imaging for the detection of prostate cancer in treatment-naïve patients: A diagnostic test accuracy systematic review and meta-analysis. BJU Int. 2019, 124, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Bass, E.J.; Pantovic, A.; Connor, M.; Gabe, R.; Padhani, A.R.; Rockall, A.; Sokhi, H.; Tam, H.; Winkler, M.; Ahmed, H.U. A systematic review and meta-analysis of the diagnostic accuracy of biparametric prostate MRI for prostate cancer in men at risk. Prostate Cancer Prostatic Dis. 2020, 24, 596–611. [Google Scholar] [CrossRef] [PubMed]
- Boesen, L.; Nørgaard, N.; Løgager, V.; Balslev, I.; Bisbjerg, R.; Thestrup, K.C.; Winther, M.D.; Jakobsen, H.; Thomsen, H.S. Assessment of the Diagnostic Accuracy of Biparametric Magnetic Resonance Imaging for Prostate Cancer in Biopsy-Naive Men: The Biparametric MRI for Detection of Prostate Cancer (BIDOC) Study. JAMA Netw. Open 2018, 1, e180219. [Google Scholar] [CrossRef] [Green Version]
- Jambor, I.; Verho, J.; Ettala, O.; Knaapila, J.; Taimen, P.; Syvänen, K.T.; Kiviniemi, A.; Kähkönen, E.; Perez, I.M.; Seppänen, M.; et al. Validation of IMPROD biparametric MRI in men with clinically suspected prostate cancer: A prospective multi-institutional trial. PLoS Med. 2019, 16, e1002813. [Google Scholar] [CrossRef] [Green Version]
- Di Campli, E.; Delli Pizzi, A.; Seccia, B.; Cianci, R.; d’Annibale, M.; Colasante, A.; Cinalli, S.; Castellan, P.; Navarra, R.; Iantorno, R.; et al. Diagnostic accuracy of biparametric vs multiparametric MRI in clinically significant prostate cancer: Comparison between readers with different experience. Eur. J. Radiol. 2018, 101, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Faletti, R.; Calleris, G.; Giglio, J.; Berzovini, C.; Gentile, F.; Marra, G.; Misischi, F.; Molinaro, L.; Bergamasco, L.; et al. Prostate cancer detection with biparametric magnetic resonance imaging (bpMRI) by readers with different experience: Performance and comparison with multiparametric (mpMRI). Abdom. Radiol. 2019, 44, 1883–1893. [Google Scholar] [CrossRef]
- Cho, J.; Ahn, H.; Hwang, S.I.; Lee, H.J.; Choe, G.; Byun, S.S.; Hong, S.K. Biparametric versus multiparametric magnetic resonance imaging of the prostate: Detection of clinically significant cancer in a perfect match group. Prostate Int. 2020, 8, 146–151. [Google Scholar] [CrossRef]
- Lee, D.H.; Nam, J.K.; Lee, S.S.; Han, J.Y.; Lee, J.W.; Chung, M.K.; Park, S.W. Comparison of Multiparametric and Biparametric MRI in First Round Cognitive Targeted Prostate Biopsy in Patients with PSA Levels under 10 ng/mL. Yonsei Med. J. 2017, 58, 994–999. [Google Scholar] [CrossRef] [Green Version]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H.; Moon, M.H. Head-to-Head Comparison Between Biparametric and Multiparametric MRI for the Diagnosis of Prostate Cancer: A Systematic Review and Meta-Analysis. AJR Am. J. Roentgenol. 2018, 211, W226–W241. [Google Scholar] [CrossRef]
- Scialpi, M.; D’Andrea, A.; Martorana, E.; Malaspina, C.M.; Aisa, M.C.; Napoletano, M.; Orlandi, E.; Rondoni, V.; Scialpi, P.; Pacchiarini, D.; et al. Biparametric MRI of the prostate. Turk. J. Urol. 2017, 43, 401–409. [Google Scholar] [CrossRef] [Green Version]
- Scialpi, M.; Prosperi, E.; D’Andrea, A.; Martorana, E.; Malaspina, C.; Palumbo, B.; Orlandi, A.; Falcone, G.; Milizia, M.; Mearini, L.; et al. Biparametric versus Multiparametric MRI with Non-endorectal Coil at 3T in the Detection and Localization of Prostate Cancer. Anticancer Res. 2017, 37, 1263–1271. [Google Scholar] [CrossRef] [Green Version]
- Bernatz, S.; Ackermann, J.; Mandel, P.; Kaltenbach, B.; Zhdanovich, Y.; Harter, P.N.; Döring, C.; Hammerstingl, R.; Bodelle, B.; Smith, K.; et al. Comparison of machine learning algorithms to predict clinically significant prostate cancer of the peripheral zone with multiparametric MRI using clinical assessment categories and radiomic features. Eur. Radiol. 2020, 30, 6757–6769. [Google Scholar] [CrossRef]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Abdollahi, H.; Mofid, B.; Shiri, I.; Razzaghdoust, A.; Saadipoor, A.; Mahdavi, A.; Galandooz, H.M.; Mahdavi, S.R. Machine learning-based radiomic models to predict intensity-modulated radiation therapy response, Gleason score and stage in prostate cancer. Radiol. Med. 2019, 124, 555–567. [Google Scholar] [CrossRef]
- Wildeboer, R.R.; van Sloun, R.J.G.; Wijkstra, H.; Mischi, M. Artificial intelligence in multiparametric prostate cancer imaging with focus on deep-learning methods. Comput. Methods Programs Biomed. 2020, 189, 105316. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Ching, T.; Himmelstein, D.S.; Beaulieu-Jones, B.K.; Kalinin, A.A.; Do, B.T.; Way, G.P.; Ferrero, E.; Agapow, P.M.; Zietz, M.; Hoffman, M.M.; et al. Opportunities and obstacles for deep learning in biology and medicine. J. R. Soc. Interface 2018, 15, 20170387. [Google Scholar] [CrossRef] [Green Version]
- Penzkofer, T.; Padhani, A.R.; Turkbey, B.; Haider, M.A.; Huisman, H.; Walz, J.; Salomon, G.; Schoots, I.G.; Richenberg, J.; Villeirs, G.; et al. ESUR/ESUI position paper: Developing artificial intelligence for precision diagnosis of prostate cancer using magnetic resonance imaging. Eur. Radiol. 2021, 31, 9567–9578. [Google Scholar] [CrossRef]
- Chen, Q.; Hu, S.; Long, P.; Lu, F.; Shi, Y.; Li, Y. A Transfer Learning Approach for Malignant Prostate Lesion Detection on Multiparametric MRI. Technol. Cancer Res. Treat. 2019, 18, 1–9. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- American College of Radiology (ACR). PI-RADS. Available online: https://www.acr.org/-/media/ACR/Files/RADS/Pi-RADS/PIRADS-V2-1.pdf (accessed on 4 September 2021).
- Wu, M.; Krishna, S.; Thornhill, R.E.; Flood, T.A.; McInnes, M.D.F.; Schieda, N. Transition zone prostate cancer: Logistic regression and machine-learning models of quantitative ADC, shape and texture features are highly accurate for diagnosis. J. Magn. Reson. Imaging 2019, 50, 940–950. [Google Scholar] [CrossRef]
- Varghese, B.; Chen, F.; Hwang, D.; Palmer, S.L.; de Castro Abreu, A.L.; Ukimura, O.; Aron, M.; Aron, M.; Gill, I.; Duddalwar, V.; et al. Objective risk stratification of prostate cancer using machine learning and radiomics applied to multiparametric magnetic resonance images. Sci. Rep. 2019, 9, 1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, X.; Li, M.; Dong, D.; Feng, Z.; Zhang, P.; Ke, Z.; You, H.; Han, F.; Ma, H.; Tian, J.; et al. Multi-parametric MRI-based radiomics signature for discriminating between clinically significant and insignificant prostate cancer: Cross-validation of a machine learning method. Eur. J. Radiol. 2019, 115, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toivonen, J.; Montoya Perez, I.; Movahedi, P.; Merisaari, H.; Pesola, M.; Taimen, P.; Boström, P.J.; Pohjankukka, J.; Kiviniemi, A.; Pahikkala, T.; et al. Radiomics and machine learning of multisequence multiparametric prostate MRI: Towards improved non-invasive prostate cancer characterization. PLoS ONE 2019, 14, e0217702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Li, M.; Gu, Y.; Zhang, Y.; Yang, S.; Wei, C.; Wu, J.; Li, X.; Zhao, W.; Shen, J. Prostate Cancer Differentiation and Aggressiveness: Assessment With a Radiomic-Based Model vs. PI-RADS v2. J. Magn. Reson. Imaging 2019, 49, 875–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Fang, M.; Zou, J.; Yang, S.; Yu, D.; Zhong, L.; Hu, C.; Zang, Y.; Dong, D.; Tian, J.; et al. Using biparametric MRI radiomics signature to differentiate between benign and malignant prostate lesions. Eur. J. Radiol. 2019, 114, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Cao, R.; Shakeri, S.; Scalzo, F.; Lee, Y.; Enzmann, D.R.; Wu, H.H.; Raman, S.S.; Sung, K. Deep transfer learning-based prostate cancer classification using 3 Tesla multi-parametric MRI. Abdom. Radiol. 2019, 44, 2030–2039. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Qin, W.; Buyyounouski, M.; Ibragimov, B.; Hancock, S.; Han, B.; Xing, L. Prostate cancer classification with multiparametric MRI transfer learning model. Med. Phys. 2019, 46, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Baxter, J.S.H.; Akin, O.; Cantor-Rivera, D. Prostate cancer detection using residual networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1647–1650. [Google Scholar] [CrossRef]
- Schelb, P.; Kohl, S.; Radtke, J.P.; Wiesenfarth, M.; Kickingereder, P.; Bickelhaupt, S.; Kuder, T.A.; Stenzinger, A.; Hohenfellner, M.; Schlemmer, H.P.; et al. Classification of Cancer at Prostate MRI: Deep Learning versus Clinical PI-RADS Assessment. Radiology 2019, 293, 607–617. [Google Scholar] [CrossRef]
- Montoya Perez, I.; Jambor, I.; Pahikkala, T.; Airola, A.; Merisaari, H.; Saunavaara, J.; Alinezhad, S.; Väänänen, R.M.; Tallgrén, T.; Verho, J.; et al. Prostate Cancer Risk Stratification in Men With a Clinical Suspicion of Prostate Cancer Using a Unique Biparametric MRI and Expression of 11 Genes in Apparently Benign Tissue: Evaluation Using Machine-Learning Techniques. J. Magn. Reson. Imaging 2020, 51, 1540–1553. [Google Scholar] [CrossRef]
- Hou, Y.; Bao, M.L.; Wu, C.J.; Zhang, J.; Zhang, Y.D.; Shi, H.B. A radiomics machine learning-based redefining score robustly identifies clinically significant prostate cancer in equivocal PI-RADS score 3 lesions. Abdom. Radiol. 2020, 45, 4223–4234. [Google Scholar] [CrossRef]
- Mehralivand, S.; Harmon, S.A.; Shih, J.H.; Smith, C.P.; Lay, N.; Argun, B.; Bednarova, S.; Baroni, R.H.; Canda, A.E.; Ercan, K.; et al. Multicenter Multireader Evaluation of an Artificial Intelligence-Based Attention Mapping System for the Detection of Prostate Cancer With Multiparametric MRI. AJR Am. J. Roentgenol. 2020, 215, 903–912. [Google Scholar] [CrossRef]
- Gong, L.; Xu, M.; Fang, M.; Zou, J.; Yang, S.; Yu, X.; Xu, D.; Zhou, L.; Li, H.; He, B.; et al. Noninvasive Prediction of High-Grade Prostate Cancer via Biparametric MRI Radiomics. J. Magn. Reson. Imaging 2020, 52, 1102–1109. [Google Scholar] [CrossRef]
- Bleker, J.; Kwee, T.C.; Dierckx, R.; de Jong, I.J.; Huisman, H.; Yakar, D. Multiparametric MRI and auto-fixed volume of interest-based radiomics signature for clinically significant peripheral zone prostate cancer. Eur. Radiol. 2020, 30, 1313–1324. [Google Scholar] [CrossRef] [Green Version]
- Zong, W.; Lee, J.K.; Liu, C.; Carver, E.N.; Feldman, A.M.; Janic, B.; Elshaikh, M.A.; Pantelic, M.V.; Hearshen, D.; Chetty, I.J.; et al. A deep dive into understanding tumor foci classification using multiparametric MRI based on convolutional neural network. Med. Phys. 2020, 47, 4077–4086. [Google Scholar] [CrossRef]
- Sanford, T.; Harmon, S.A.; Turkbey, E.B.; Kesani, D.; Tuncer, S.; Madariaga, M.; Yang, C.; Sackett, J.; Mehralivand, S.; Yan, P.; et al. Deep-Learning-Based Artificial Intelligence for PI-RADS Classification to Assist Multiparametric Prostate MRI Interpretation: A Development Study. J. Magn. Reson. Imaging 2020, 52, 1499–1507. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Radiomics for Gleason Score Detection through Deep Learning. Sensors 2020, 20, 5411. [Google Scholar] [CrossRef]
- Chen, Y.; Xing, L.; Yu, L.; Bagshaw, H.P.; Buyyounouski, M.K.; Han, B. Automatic intraprostatic lesion segmentation in multiparametric magnetic resonance images with proposed multiple branch UNet. Med. Phys. 2020, 47, 6421–6429. [Google Scholar] [CrossRef]
- Winkel, D.J.; Wetterauer, C.; Matthias, M.O.; Lou, B.; Shi, B.; Kamen, A.; Comaniciu, D.; Seifert, H.H.; Rentsch, C.A.; Boll, D.T. Autonomous Detection and Classification of PI-RADS Lesions in an MRI Screening Population Incorporating Multicenter-Labeled Deep Learning and Biparametric Imaging: Proof of Concept. Diagnostics 2020, 10, 951. [Google Scholar] [CrossRef]
- Arif, M.; Schoots, I.G.; Castillo Tovar, J.; Bangma, C.H.; Krestin, G.P.; Roobol, M.J.; Niessen, W.; Veenland, J.F. Clinically significant prostate cancer detection and segmentation in low-risk patients using a convolutional neural network on multi-parametric MRI. Eur. Radiol. 2020, 30, 6582–6592. [Google Scholar] [CrossRef]
- He, D.; Wang, X.; Fu, C.; Wei, X.; Bao, J.; Ji, X.; Bai, H.; Xia, W.; Gao, X.; Huang, Y.; et al. MRI-based radiomics models to assess prostate cancer, extracapsular extension and positive surgical margins. Cancer Imaging 2021, 21, 46. [Google Scholar] [CrossRef]
- Vente, C.; Vos, P.; Hosseinzadeh, M.; Pluim, J.; Veta, M. Deep Learning Regression for Prostate Cancer Detection and Grading in Bi-Parametric MRI. IEEE Trans. Biomed. Eng. 2021, 68, 374–383. [Google Scholar] [CrossRef]
- Chen, J.; Wan, Z.; Zhang, J.; Li, W.; Chen, Y.; Li, Y.; Duan, Y. Medical image segmentation and reconstruction of prostate tumor based on 3D AlexNet. Comput Methods Programs Biomed. 2021, 200, 105878. [Google Scholar] [CrossRef]
- Cao, R.; Zhong, X.; Afshari, S.; Felker, E.; Suvannarerg, V.; Tubtawee, T.; Vangala, S.; Scalzo, F.; Raman, S.; Sung, K. Performance of Deep Learning and Genitourinary Radiologists in Detection of Prostate Cancer Using 3-T Multiparametric Magnetic Resonance Imaging. J. Magn. Reson. Imaging 2021, 54, 474–483. [Google Scholar] [CrossRef]
- Hou, Y.; Zhang, Y.H.; Bao, J.; Bao, M.L.; Yang, G.; Shi, H.B.; Song, Y.; Zhang, Y.D. Artificial intelligence is a promising prospect for the detection of prostate cancer extracapsular extension with mpMRI: A two-center comparative study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3805–3816. [Google Scholar] [CrossRef]
- Yan, Y.; Shao, L.; Liu, Z.; He, W.; Yang, G.; Liu, J.; Xia, H.; Zhang, Y.; Chen, H.; Liu, C.; et al. Deep Learning with Quantitative Features of Magnetic Resonance Images to Predict Biochemical Recurrence of Radical Prostatectomy: A Multi-Center Study. Cancers 2021, 13, 3098. [Google Scholar] [CrossRef]
- Schelb, P.; Wang, X.; Radtke, J.P.; Wiesenfarth, M.; Kickingereder, P.; Stenzinger, A.; Hohenfellner, M.; Schlemmer, H.P.; Maier-Hein, K.H.; Bonekamp, D. Simulated clinical deployment of fully automatic deep learning for clinical prostate MRI assessment. Eur. Radiol. 2021, 31, 302–313. [Google Scholar] [CrossRef]
- Antonelli, M.; Johnston, E.W.; Dikaios, N.; Cheung, K.K.; Sidhu, H.S.; Appayya, M.B.; Giganti, F.; Simmons, L.A.M.; Freeman, A.; Allen, C.; et al. Machine learning classifiers can predict Gleason pattern 4 prostate cancer with greater accuracy than experienced radiologists. Eur. Radiol. 2019, 29, 4754–4764. [Google Scholar] [CrossRef] [Green Version]
- Kan, Y.; Zhang, Q.; Hao, J.; Wang, W.; Zhuang, J.; Gao, J.; Huang, H.; Liang, J.; Marra, G.; Calleris, G.; et al. Clinico-radiological characteristic-based machine learning in reducing unnecessary prostate biopsies of PI-RADS 3 lesions with dual validation. Eur. Radiol. 2020, 30, 6274–6284. [Google Scholar] [CrossRef]
- Hiremath, A.; Shiradkar, R.; Merisaari, H.; Prasanna, P.; Ettala, O.; Taimen, P.; Aronen, H.J.; Boström, P.J.; Jambor, I.; Madabhushi, A. Test-retest repeatability of a deep learning architecture in detecting and segmenting clinically significant prostate cancer on apparent diffusion coefficient (ADC) maps. Eur. Radiol. 2021, 31, 379–391. [Google Scholar] [CrossRef]
- Dulhanty, C.; Wang, L.; Cheng, M.; Gunraj, H.; Khalvati, F.; Haider, M.A.; Wong, A. Radiomics Driven Diffusion Weighted Imaging Sensing Strategies for Zone-Level Prostate Cancer Sensing. Sensors 2020, 20, 1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Society for Optics and Photonics. Solve for X: Lessons Learned from PROSTATEx. Available online: https://spie.org/news/spie-professional-magazine-archive/2019-january/solve-for-x?SSO=1 (accessed on 10 October 2021).






| Reference | Year | ML | DL | Field Strength | Target | Number of Patients | Age | SS/SP/Accuracy | AUC | Sequences Used |
|---|---|---|---|---|---|---|---|---|---|---|
| Abdollahi H. et al. [40] | 2019 | 1 | 0 | 1.5 T | Gleason score prediction | 33 | 73 (51–82) | 0.739 | T2, ADC | |
| Wu M. et al. [48] | 2019 | 1 | 0 | 3 T | TZ PCA detection | 44 | 68 ± 7 | 93.2%/98.4% | 0.989 (LR) | T2, ADC |
| Varghese B. et al. [49] | 2019 | 1 | 0 | 3 T | Grading prediction | 68 53 | 86%/72% | 0.71 | T2, ADC, | |
| Min X. et al. [50] | 2019 | 1 | 0 | 3 T | ci/csPCA discrimination TZ and PZ | 280 | 84.1%/72.7% | 0.823 | T2, ADC, b1500 | |
| Toivonen J. et al. [51] | 2019 | 1 | 0 | 3 T | Gleason prediction TZ and PZ | 62 | 65 (45–73) | 0.88 | T2, b0-b2000, T2mapping | |
| Chen T. et al. [52] | 2019 | 1 | 0 | 3 T | Tumor detection aggressiveness prediction TZ and PZ | 182 199 | 73 (55–90) | 98.6/99.2%/98.9% (noPCA vs. PCA) 100/98.25 8/99.1% (ci vs. csPCA) | 0.999 (noPCA vs. PCA) 0.933 (ciPCA vs. csPCA) | T2, ADC |
| Xu M. et al. [53] | 2019 | 1 | 0 | 3 T | Tumor detection | 331 | 71 (46–94) | 0.92 (Radiomics) 0.993 (R + clinical data) | T2, ADC, DWI | |
| Zhong X. et al. [54] | 2019 | 0 | 1 | 3 T | ci/cs PCA discrimination DL vs. PIRADS exp. radiologists | 140 | 63.6%/80.6%/72.3% 86.4%/48.0%/86.4% | 0.726 (DL) 0.711 (PIRADS v2) | ||
| Yuan Y. et al. [55] | 2019 | 0 | 1 | 3 T | ci/cs PCS discrimination (GS > 7) | 132 112 | –/–/86.9% | T2 ax and sag, ADC | ||
| Xu H. et al. [56] | 2019 | 0 | 1 | 3 T | Detection of PIRADS ≥ 3 lesions | 346 | –/–/93.0% | 0.950 | T2, ADC, high b-value | |
| Schelb P. et al. [57] | 2019 | 0 | 1 | 3 T | DL and radiologist for lesion (PIRADS ≥ 3 and 4) detection and segmentation | 250 62 | 64 (58–71) 64 (60–69) | 98/17% Rad, PIRADS ≥ 3 84/48% Rad, PRIADS ≥ 4 99/25%, DL, PIRADS ≥ 3 83/55%, DL, PIRADS ≥ 4 | T2, ADC, DWI | |
| Montoya Perez I. et al. [58] | 2020 | 1 | 0 | 3 T | Detection of csPCA with bpMRI, RNA and clinical data | 80 | 65 ± 7.1 | 0.92 | T2, DWI | |
| Hou Y. et al. [59]. | 2020 | 1 | 0 | 3 T | csPCA in PIRADS 3 identification in TZ and PZ | 263 | 66.8 ± 11.4 | 0.89 | T2, ADC, b1500 | |
| Mehralivand S. et al. [60] | 2020 | 1 | 0 | 3 T | Detection csPCA in TZ and PZ | 236 | 50.8%/–/– (TZ, MRI) 61.8%/–/– (TZ, DL) | 0.749 (MRI) 0.775 (DL) | T2, b1500 | |
| Gong L et al. [61] | 2020 | 1 | 0 | 3 T | ci/cs PCA discrimination | 326 163 | 73.8%/65.8%/69.9% | 0.788 | T2, ADC, b800 | |
| Bleker J. et al. [62] | 2020 | 1 | 0 | 3 T | ci/cs PCA discrimination in PZ | 206 | 66 (48–83) | 0.870 (mpMRI) 0.816 (bpMRI) | T2, ADC, DWI, (DCE) | |
| Zong W. et al. [63] | 2020 | 0 | 1 | 3 T | CNN optimization | 367 | 100/92% | 0.840 | T2, ADC, b0 | |
| Sanford T. et al. [64] | 2020 | 0 | 1 | 3 T | Automated PIRADS classification compared to radiologist | 687 | 67 (46–89) | T2, ADC, high b-value | ||
| Brunese L. et al. [65] | 2020 | 1 | 1 | 1.5 T | Gleason score prediction | 52 | –/–/98% | T2, DCE | ||
| Chen Y. et al. [66] | 2020 | 0 | 1 | 3 T | Prostate and cancer segmentation | 136 | 68 (49–62) | 75.1/99.9% | T2, ADC, b1200 | |
| Winkel D.J. et al. [67] | 2020 | 0 | 1 | 3 T | bpMRI PCA Screening | 49 | 58 (45–75) | 87/50% | T2, ADC, b2000 | |
| Arif M. et al. [68] | 2020 | 0 | 1 | 3 T | Detection of csPCA in AS | 292 | 68 (62–72) | 92/76% | 0.89 | T2, ADC, b800 |
| He D. et al. [69] | 2021 | 1 | 0 | 3 T | Tumor detection Prediction ECE Prediction PSM | 459 | 65 (30–89) | 0.863 0.905 (integrated model) | T2, ADC | |
| Vente C. et al. [70] | 2021 | 0 | 1 | 3 T | csPCA detection and grading | 99 63 | T2, ADC | |||
| Chen J. et al. [71] | 2021 | 0 | 1 | 3 T | csPCA detection and grading | 25 | 89.6/90.2%/92.1% | 0.964 | T2, T1 | |
| Cao R. et al. [72] | 2021 | 0 | 1 | 3 T | PCA detection and grading | 126 427 | 62.4 ± 6.4 61.1 ± 7.1 | 98/17% PIRADS, ≥3 85/58% PIRADS, ≥4 100/17% Unet ≥ 3 83/58% Unet ≥ 4 | T2, ADC | |
| Hou Y. et al. [73] | 2021 | 0 | 1 | 3 T | ECE prediction | 590 150 103 | 69.2 (42–86) 69.2 (48–83) 70.2 (52–87) | 0.857 0.728 | T2, ADC, b1500 | |
| Yan Y. et al. [74] | 2021 | 1 | 1 | 3 T | BCR prediction | 485 | 69.8 | 0.802 (C-index) | T2 | |
| Schelb P. et al. [75] | 2021 | 0 | 1 | 3 T | csPCA detection and grading | 284 | 64 (IQR 61–72) | 98/17% PIRADS, ≥3 85/55% PIRADS, ≥4 99/24% Unet ≥ 3 83/55% Unet ≥ 4 | T2, ADC, b1500 |
| Reference | Year | ML | DL | Metric | Human Radiologist | AI-Approach |
|---|---|---|---|---|---|---|
| Chen T. et al. [52] | 2019 | 1 | 0 | AUC | 0.867 | 0.999 |
| Schelb P. et al. [57] | 2019 | 0 | 1 | Sensitivity/Specificity | 98/17% PIRADS ≥ 3 84/48% PRIADS ≥ 4 | 99/25% PIRADS ≥ 3 83/55% PIRADS ≥ 4 |
| Mehralivand S. et al. [60] | 2020 | 1 | 0 | AUC Sensitivity | 0.816 89.6% | 0.780 87.9% |
| Sanford T. et al. [64] | 2020 | 0 | 1 | Cancer detection rates | 53% PIRADS 3 61% PRIADS 4 92% PIRADS 5 | 57%, PIRADS 3 60%, PIRADS 4 89% PIRADS 5 |
| Cao R. et al. [72] | 2021 | 0 | 1 | Sensitivity/Specificity | 98/17% PIRADS, ≥3 85/58% PIRADS, ≥4 | 100/17% PIRADS, ≥3 83/58% PIRADS, ≥4 |
| Schelb P. et al. [75] | 2021 | 0 | 1 | Sensitivity/Specificity | 98/17% PIRADS, ≥3 85/55% PIRADS, ≥4 | 99/24% PIRADS, ≥3 83/55% PIRADS, ≥4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaely, H.J.; Aringhieri, G.; Cioni, D.; Neri, E. Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading, and Characterization of Prostate Cancer: A Systematic Review. Diagnostics 2022, 12, 799. https://doi.org/10.3390/diagnostics12040799
Michaely HJ, Aringhieri G, Cioni D, Neri E. Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading, and Characterization of Prostate Cancer: A Systematic Review. Diagnostics. 2022; 12(4):799. https://doi.org/10.3390/diagnostics12040799
Chicago/Turabian StyleMichaely, Henrik J., Giacomo Aringhieri, Dania Cioni, and Emanuele Neri. 2022. "Current Value of Biparametric Prostate MRI with Machine-Learning or Deep-Learning in the Detection, Grading, and Characterization of Prostate Cancer: A Systematic Review" Diagnostics 12, no. 4: 799. https://doi.org/10.3390/diagnostics12040799