
Imaging and Clinical Parameters for Distinction between Infected and Non-Infected Fluid Collections in CT: Prospective Study Using Extended Microbiological Approach

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Informed Consent and Institutional Review Board Approval
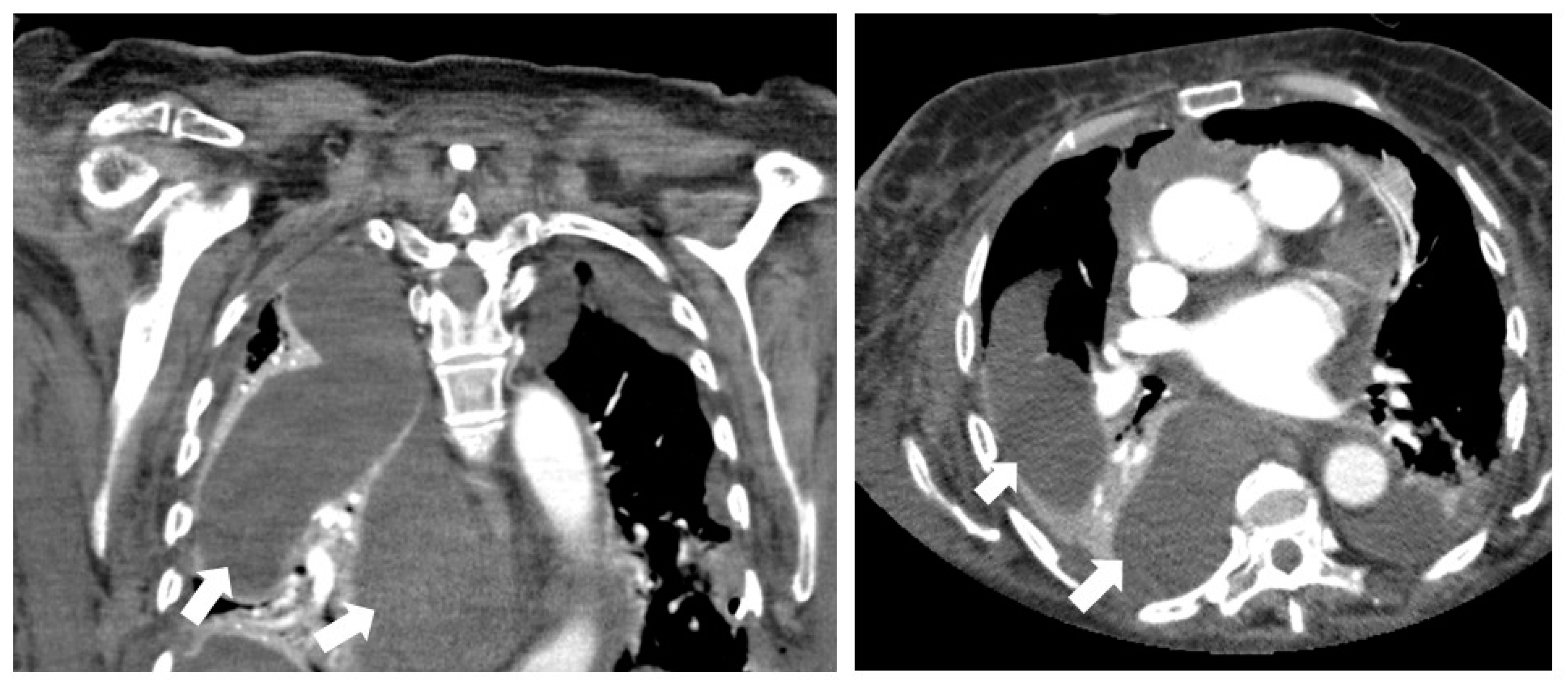
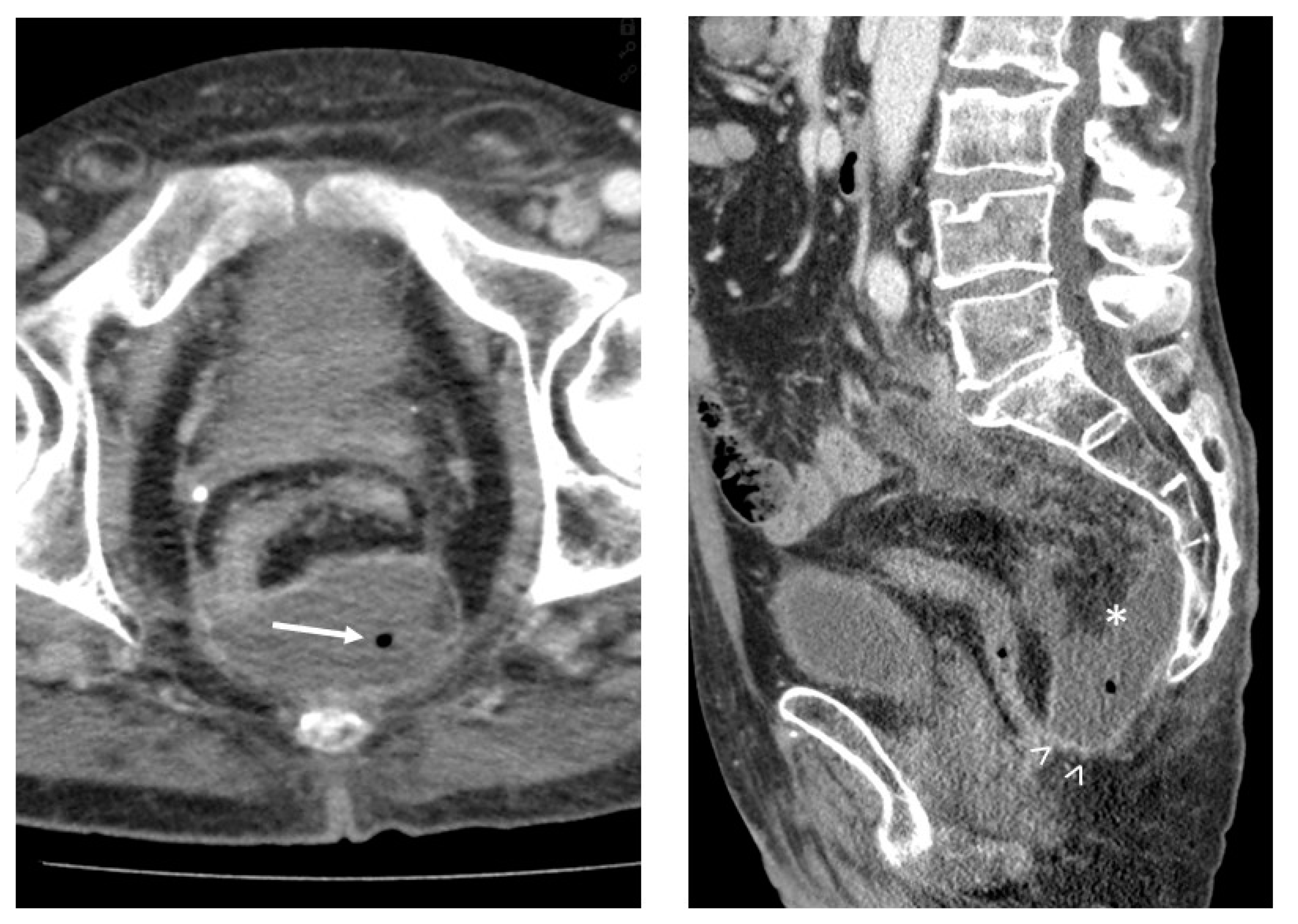
2.2. CT Imaging Prior to Drainage
- CT attenuation of the suspected fluid collection (in Hounsfield units (HU));
- Gas entrapment: the presence of superficial bubbles or air–fluid levels;
- Wall enhancement: contrast enhancement of the wall due to hypervascularization;
- Wall thickness: in case of encapsuled fluid collection, wall thickness was measured in millimeters;
- Fat stranding: increase in the attenuation of the surrounding adipose tissue.
2.3. CT-Guided Drainage
2.4. Sample Transport and Processing
2.5. Microbiological Analyses
2.6. Laboratory and Clinical Parameters
2.7. Statistical Assessment
3. Results
3.1. Patient Characteristics
3.2. Univariate Comparison between Infected and Sterile Fluid Collections
3.3. Multivariate Logistic Regression Analysis
3.4. Performance of Published Scoring Systems in Our Patient Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Politano, A.D.; Hranjec, T.; Rosenberger, L.H.; Sawyer, R.G.; Tache Leon, C.A. Differences in morbidity and mortality with percutaneous versus open surgical drainage of postoperative intra-abdominal infections: A review of 686 cases. Am. Surg. 2011, 77, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Van Sonnenberg, E.; Wittich, G.R.; Goodacre, B.W.; Casola, G.; D’Agostino, H.B. Percutaneous abscess drainage: Update. World J. Surg. 2001, 25, 362–369; discussion 370–372. [Google Scholar] [CrossRef] [PubMed]
- Benoist, S.; Panis, Y.; Pannegeon, V.; Soyer, P.; Watrin, T.; Boudiaf, M.; Valleur, P. Can failure of percutaneous drainage of postoperative abdominal abscesses be predicted? Am. J. Surg. 2002, 184, 148–153. [Google Scholar] [CrossRef]
- Cinat, M.E.; Wilson, S.E.; Din, A.M. Determinants for successful percutaneous image-guided drainage of intra-abdominal abscess. Arch. Surg. 2002, 137, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Çullu, N.; Kalemci, S.; Karakaş, Ö.; Eser, İ.; Yalçın, F.; Boyacı, F.N.; Karakaş, E. Efficacy of CT in diagnosis of transudates and exudates in patients with pleural effusion. Diagn. Interv. Radiol. 2013, 20, 116–120. [Google Scholar] [CrossRef]
- Gnannt, R.; Fischer, M.A.; Baechler, T.; Clavien, P.-A.; Karlo, C.; Seifert, B.; Lesurtel, M.; Alkadhi, H. Distinguishing infected from noninfected abdominal fluid collections after surgery: An imaging, clinical, and laboratory-based scoring system. Investig. Radiol. 2015, 50, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Radosa, C.G.; Radosa, J.C.; Laniado, M.; Brandt, J.; Streitzig, J.; Seppelt, D.; Volk, A.; Plodeck, V.; Kühn, J.P.; Hoffmann, R.-T. Infected versus sterile abdominal fluid collections in postoperative CT: A scoring system based on clinical and imaging findings. Abdom. Radiol. 2020, 45, 2871–2878. [Google Scholar] [CrossRef]
- Allen, B.C.; Barnhart, H.; Bashir, M.; Nieman, C.; Breault, S.; Jaffe, T.A. Diagnostic accuracy of intra-abdominal fluid collection characterization in the era of multidetector computed tomography. Am. Surg. 2012, 78, 185–189. [Google Scholar] [CrossRef]
- Jaques, P.; Mauro, M.; Safrit, H.; Yankaskas, B.; Piggott, B. CT features of intraabdominal abscesses: Prediction of successful percutaneous drainage. AJR Am. J. Roentgenol. 1986, 146, 1041–1045. [Google Scholar] [CrossRef]
- Sertic, M.; Parkes, L.; Mattiassi, S.; Pritzker, K.; Gardam, M.; Murphy, K. The Efficacy of Computed Tomography-Guided Percutaneous Spine Biopsies in Determining a Causative Organism in Cases of Suspected Infection: A Systematic Review. Can. Assoc. Radiol. J. 2019, 70, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Schwarz-Nemec, U.; Friedrich, K.M.; Stihsen, C.; Schwarz, F.K.; Trattnig, S.; Weber, M.; Grohs, J.G.; Nemec, S.F. Vertebral Bone Marrow and Endplate Assessment on MR Imaging for the Differentiation of Modic Type 1 Endplate Changes and Infectious Spondylodiscitis. J. Clin. Med. 2020, 9, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, A.; Germann, T.; Wünnemann, F.; Weber, M.-A.; Schiltenwolf, M.; Akbar, M.; Burkholder, I.; Kauczor, H.-U.; Rehnitz, C. Impact of MRI, CT, and Clinical Characteristics on Microbial Pathogen Detection Using CT-Guided Biopsy for Suspected Spondylodiscitis. J. Clin. Med. 2019, 9, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spira, D.; Germann, T.; Lehner, B.; Hemmer, S.; Akbar, M.; Jesser, J.; Weber, M.-A.; Rehnitz, C. CT-Guided Biopsy in Suspected Spondylodiscitis—The Association of Paravertebral Inflammation with Microbial Pathogen Detection. PLoS ONE 2016, 11, e0146399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borens, B.; Arvanitakis, M.; Absil, J.; El Bouchaibi, S.; Matos, C.; Eisendrath, P.; Toussaint, E.; Deviere, J.; Bali, M.A. Added value of diffusion-weighted magnetic resonance imaging for the detection of pancreatic fluid collection infection. Eur. Radiol. 2017, 27, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Schmid-Tannwald, C.; Schmid-Tannwald, C.M.; Morelli, J.N.; Neumann, R.; Reiser, M.F.; Nikolaou, K.; Rist, C. Role of diffusion-weighted MRI in differentiation of hepatic abscesses from non-infected fluid collections. Clin. Radiol. 2014, 69, 687–694. [Google Scholar] [CrossRef]
- Chen, T.-Y.; Wu, T.-C.; Tsui, Y.-K.; Chen, H.-H.; Lin, C.-J.; Lee, H.-J.; Wu, T.-C. Diffusion-weighted magnetic resonance imaging and apparent diffusion coefficient mapping for diagnosing infectious spondylodiscitis: A preliminary study. J. Neuroimaging 2015, 25, 482–487. [Google Scholar] [CrossRef]
- Ady, J.; Fong, Y. Imaging for Infection: From Visualization of Inflammation to Visualization of Microbes. Surg. Infect. (Larchmt) 2014, 15, 700–707. [Google Scholar] [CrossRef] [Green Version]
- Expertengremium Mikrobiologisch-Infektiologische Qualitätsstandards. Intraabdominelle Infektionen unter Besonderer Berücksichtigung der Peritonitis, 1st ed.; Elsevier Urban & Fischer: München, Germany, 2012; ISBN 9783437226199. [Google Scholar]
- Guarner, C.; Soriano, G. Spontaneous bacterial peritonitis. Semin. Liver Dis. 1997, 17, 203–217. [Google Scholar] [CrossRef]
- Sajjad, M.; Khan, Z.A.; Khan, M.S. Ascitic Fluid Culture in Cirrhotic Patients with Spontaneous Bacterial Peritonitis. J. Coll. Physicians Surg. Pak. 2016, 26, 658–661. [Google Scholar]
- Rimola, A.; García-Tsao, G.; Navasa, M.; Piddock, L.J.; Planas, R.; Bernard, B.; Inadomi, J.M. Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: A consensus document. J. Hepatol. 2000, 32, 142–153. [Google Scholar] [CrossRef]
- Sorlin, P.; Mansoor, I.; Dagyaran, C.; Struelens, M.J. Comparison of resin-containing BACTEC Plus Aerobic/F* medium with conventional methods for culture of normally sterile body fluids. J. Med. Microbiol. 2000, 49, 787–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetin, E.S.; Kaya, S.; Demirci, M.; Aridogan, B.C. Comparison of the BACTEC blood culture system versus conventional methods for culture of normally sterile body fluids. Adv. Ther. 2007, 24, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Akcam, F.Z.; Yayli, G.; Uskun, E.; Kaya, O.; Demir, C. Evaluation of the Bactec microbial detection system for culturing miscellaneous sterile body fluids. Res. Microbiol. 2006, 157, 433–436. [Google Scholar] [CrossRef]
- Gu, W.; Deng, X.; Lee, M.; Sucu, Y.D.; Arevalo, S.; Stryke, D.; Federman, S.; Gopez, A.; Reyes, K.; Zorn, K.; et al. Rapid pathogen detection by metagenomic next-generation sequencing of infected body fluids. Nat. Med. 2021, 27, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Lampejo, T.; Ciesielczuk, H.; Lambourne, J. Clinical utility of 16S rRNA PCR in pleural infection. J. Med. Microbiol. 2021, 70, 001366. [Google Scholar] [CrossRef] [PubMed]
- Bivand, J.M.; Nygaard, R.M.; Kommedal, Ø. Characterization of abscesses from liver, pancreas and kidney using deep sequencing of the 16S rRNA gene. Diagn. Microbiol. Infect. Dis. 2021, 99, 115277. [Google Scholar] [CrossRef]
- Nöldge, G.; Richter, G.M.; Grenacher, L.; Brado, M.; Kauffmann, G.W. CT-gesteuerte Punktionen. Radiologe 1996, 36, 683–691. [Google Scholar] [CrossRef]
- Commander, C.W.; Wilson, S.B.; Bilaj, F.; Isaacson, A.J.; Burke, C.T.; Yu, H. CT-Guided Percutaneous Drainage Catheter Placement in the Abdomen and Pelvis: Predictors of Outcome and Protocol for Follow-up. J. Vasc. Interv. Radiol. 2020, 31, 667–673. [Google Scholar] [CrossRef]
- Skusa, R.; Skusa, C.; Wohlfarth, M.; Hahn, A.; Frickmann, H.; Weber, M.-A.; Podbielski, A.; Warnke, P. How to Handle CT-Guided Abscess Drainages in Microbiological Analyses? Sterile Vials vs. Blood Culture Bottles for Transport and Processing. Microorganisms 2021, 9, 1510. [Google Scholar] [CrossRef]
- Yuruk, E.; Tuken, M.; Sulejman, S.; Colakerol, A.; Serefoglu, E.C.; Sarica, K.; Muslumanoglu, A.Y. Computerized tomography attenuation values can be used to differentiate hydronephrosis from pyonephrosis. World J. Urol. 2017, 35, 437–442. [Google Scholar] [CrossRef]
- Boeri, L.; Fulgheri, I.; Palmisano, F.; Lievore, E.; Lorusso, V.; Ripa, F.; D’Amico, M.; Spinelli, M.G.; Salonia, A.; Carrafiello, G.; et al. Hounsfield unit attenuation value can differentiate pyonephrosis from hydronephrosis and predict septic complications in patients with obstructive uropathy. Sci. Rep. 2020, 10, 18546. [Google Scholar] [CrossRef] [PubMed]
- Ming, P.C.; Yan, T.Y.Y.; Tat, L.H. Risk factors of postoperative infections in adults with complicated appendicitis. Surg. Laparosc. Endosc. Percutan. Tech. 2009, 19, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Trinh, J.V.; Chen, L.F.; Sexton, D.J.; Anderson, D.J. Risk factors for gram-negative bacterial surgical site infection: Do allergies to antibiotics increase risk? Infect. Control Hosp. Epidemiol. 2009, 30, 440–446. [Google Scholar] [CrossRef]
- Healy, B.; Freedman, A. Infections. BMJ 2006, 332, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Abet, E.; Drissi, F.; Couëtte, C.; Jean, M.-H.; Denimal, F.; Podevin, J.; Duchalais, E.; Meurette, G. Predictive value of inflammatory markers for postoperative recovery following colorectal surgery. Int. J. Colorectal Dis. 2020, 35, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- McSorley, S.T.; Ramanathan, M.L.; Horgan, P.G.; McMillan, D.C. Postoperative C-reactive protein measurement predicts the severity of complications following surgery for colorectal cancer. Int. J. Colorectal Dis. 2015, 30, 913–917. [Google Scholar] [CrossRef]
- Warschkow, R.; Beutner, U.; Steffen, T.; Müller, S.A.; Schmied, B.M.; Güller, U.; Tarantino, I. Safe and early discharge after colorectal surgery due to C-reactive protein: A diagnostic meta-analysis of 1832 patients. Ann. Surg. 2012, 256, 245–250. [Google Scholar] [CrossRef]
- Carboni, G.L.; Fahrner, R.; Gazdhar, A.; Printzen, G.; Schmid, R.A.; Hoksch, B. Comparison of procalcitonin and CrP in the postoperative course after lung decortication. Eur. J. Cardiothorac. Surg. 2008, 33, 777–780. [Google Scholar] [CrossRef]
- Suberviola, B.; Rellan, L.; Riera, J.; Iranzo, R.; Garcia Campos, A.; Robles, J.C.; Vicente, R.; Miñambres, E.; Santibanez, M. Role of biomarkers in early infectious complications after lung transplantation. PLoS ONE 2017, 12, e0180202. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, S. The rapidly expanding role of procalcitonin as a diagnostic and prognostic assay besides in UTIs. Int. Urol. Nephrol. 2009, 41, 435–436. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| No. of CT-guided drainages performed (n1) | 100 |
| No. of patients (n2) | 87 |
| Age, years (±SD) | 63 (±16) |
| Sex, male/female (n2 = 78) | 59/28 |
| Localization of fluid collection (n1 = 100) | |
| Thorax | 21 |
| Abdomen | 69 |
| Musculoskeletal | 10 |
| Underlying primary disease (n1 = 100) | |
| Carcinoma | 38 |
| Infection or inflammation | 41 |
| Vascular | 13 |
| Other | 8 |
| Referring unit (n1 = 100) | |
| General and visceral surgery | 43 |
| Intensive care unit | 23 |
| Internal medicine | 20 |
| Urology | 5 |
| Other surgical departments | 8 |
| Other departments | 1 |
| Imaging Parameter | All Lesions (n = 100) | Infected Fluid Collection (n = 73) | Sterile Fluid Collection (n = 27) | p-Value |
|---|---|---|---|---|
| Attenuation, HU | Median (IQR) | 14 (13) | 5 (14) | 0.001 |
| Entrapped gas | Existent | 35 | 2 | <0.001 |
| None | 38 | 25 | ||
| Wall thickness, mm | Median (IQR) | 2.6 (1.55) | 0 (2.2) | <0.001 |
| Wall enhancement | Existent | 60 | 10 | <0.001 |
| Strong | 30 | 5 | ||
| Slight | 30 | 5 | ||
| None | 6 | 10 | ||
| Scan without contrast | 7 | 7 | ||
| Fat stranding (without thorax, n = 79) | Existent | 61 | 7 | <0.001 |
| None | 7 | 4 | ||
| Clinical and laboratory parameters | ||||
| CRP, mg/L (n = 94) | Median (IQR) | 161 (145) | 107 (187) | 0.096 |
| Leukocytes, 103/µL (n = 99) | Median (IQR) | 12.5 (7.7) | 11.7 (7.9) | 0.356 |
| Procalcitonin, ng/mL (n = 25) | Median (IQR) | 3.0 (28.0) | 0.4 (0.3) | 0.003 |
| Diabetes (n = 27) | 20 | 7 | 1 | |
| Immunosuppressive drugs (n = 15) | 13 | 2 | 0.23 | |
| Chemotherapeutics (n = 14) | 10 | 4 | 1 | |
| Previous antibiotic therapy (n = 95) | 0.801 | |||
| yes | 50 | 18 | ||
| no | 19 | 8 | ||
| Previous operation (n = 95) | 49 | 18 | 1 |
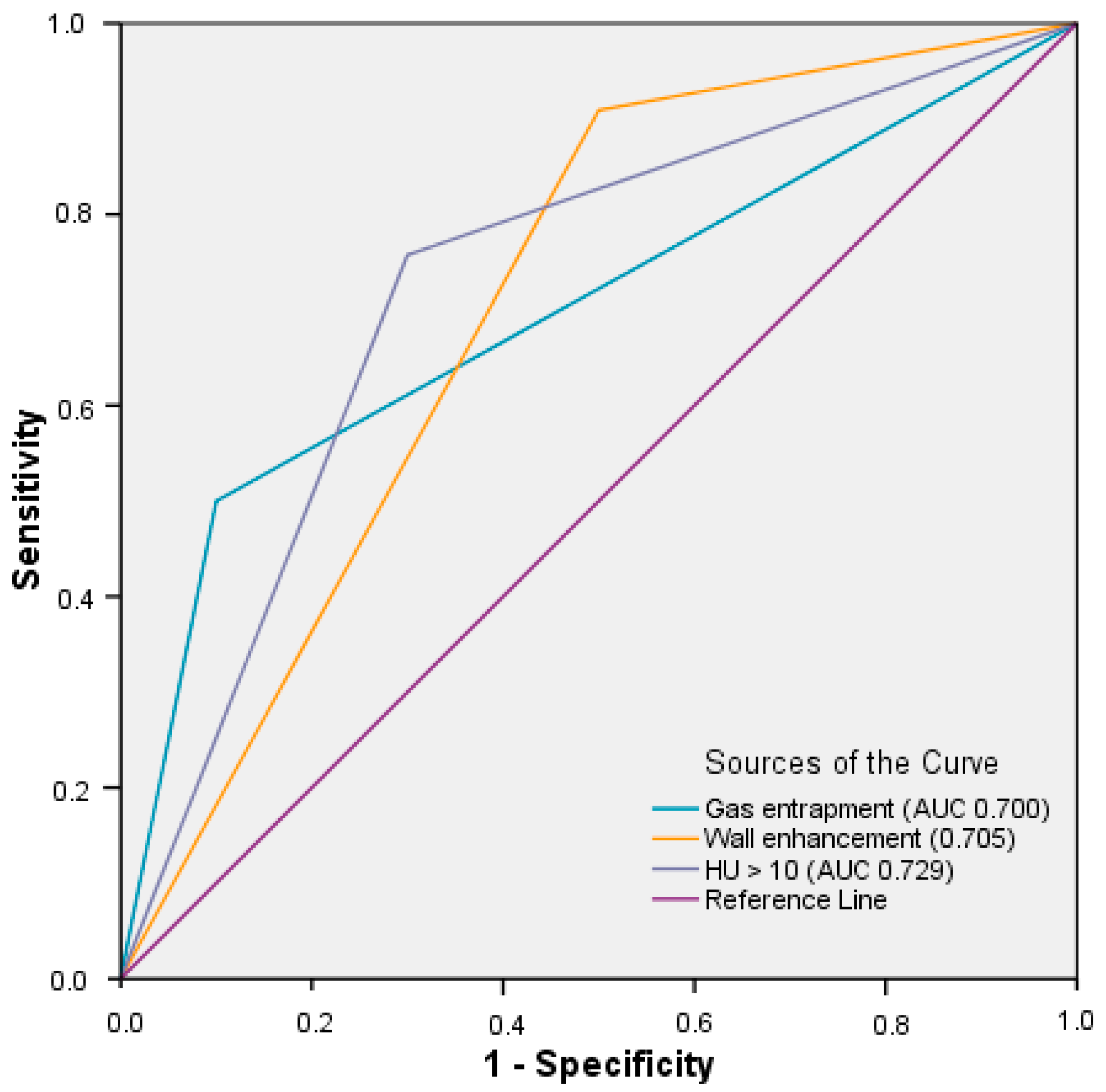
| Parameter | Sens | Spec | NPV | PPV | AUC |
|---|---|---|---|---|---|
| Fat stranding present (n = 100) | 0.90 | 0.36 | 0.36 | 0.90 | 0.630 |
| Gas entrapment present (n = 100) | 0.48 | 0.93 | 0.40 | 0.95 | 0.703 |
| Wall thickness > 1 mm (n = 100) | 0.92 | 0.56 | 0.71 | 0.85 | 0.737 |
| Wall enhancement present (n = 86) | 0.91 | 0.50 | 0.63 | 0.86 | 0.705 |
| CT attenuation > 10 HU (n = 100) | 0.74 | 0.70 | 0.50 | 0.87 | 0.722 |
| Parameter | β | p-Value | OR |
|---|---|---|---|
| Fat stranding Yes/no | 0.906 | ||
| Gas entrapment Yes/no | 1.830 | 0.027 | 6.234 |
| Wall enhancement Yes/no | 1.582 | 0.028 | 4.865 |
| CT attenuation HU > 10 HU ≤ 10 | 1.343 | 0.038 | 3.832 |
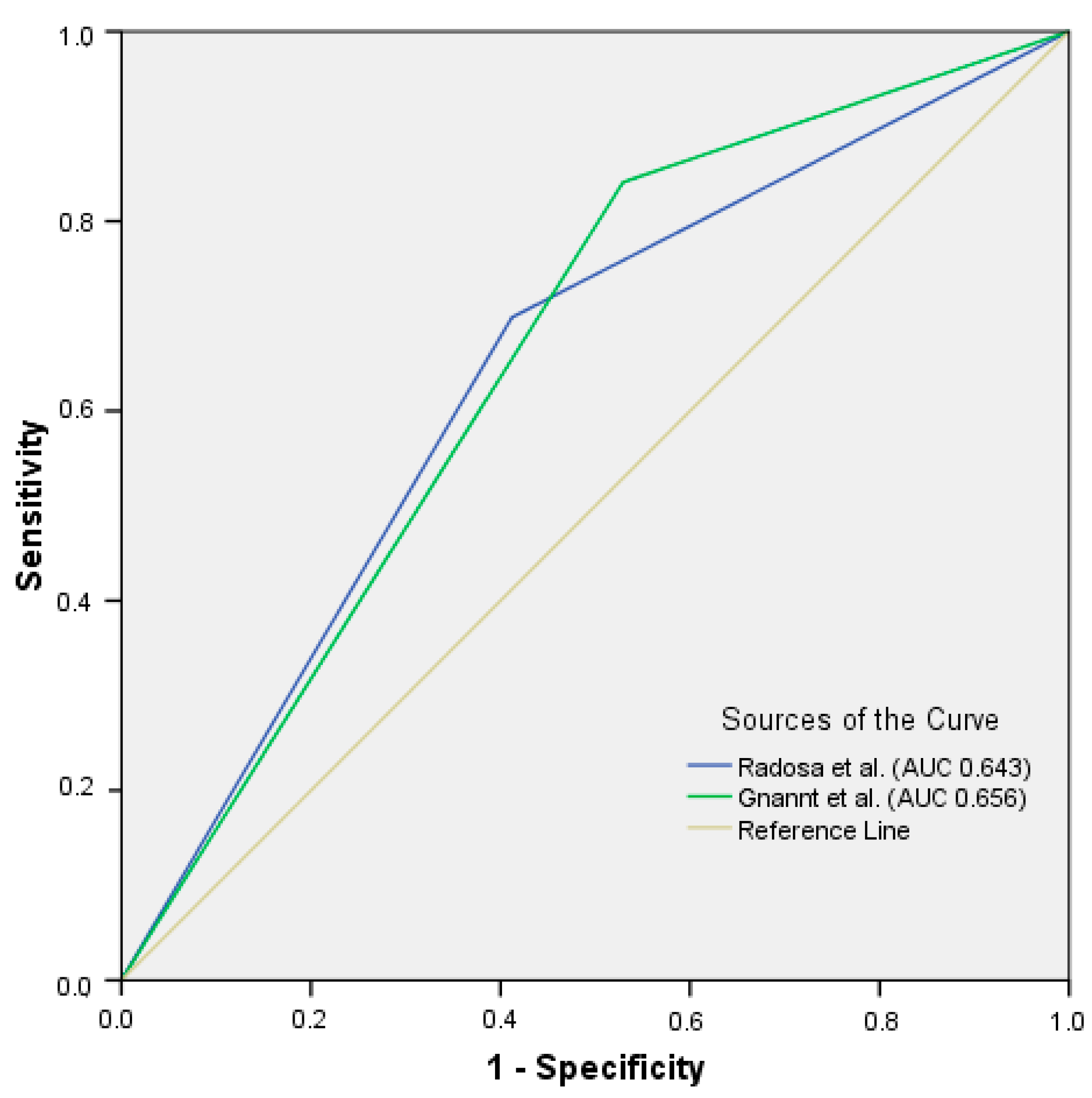
| Applied Score | Sens | Spec | NPV | PPV | AUC |
|---|---|---|---|---|---|
| Gnannt score | 0.84 [CI 0.77; 0.91] | 0.47 [CI 0.37; 0.57] | 0.44 [CI 0.34; 0.54] | 0.86 [CI 0.78; 0.93] | 0.656 |
| Radosa score | 0.70 [CI 0.60; 0.80] | 0.59 [CI 0.48; 0.70] | 0.35 [CI 0.24; 0.44] | 0.86 [CI 0.79; 0.94] | 0.643 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skusa, C.; Skusa, R.; Wohlfarth, M.; Warnke, P.; Podbielski, A.; Bath, K.; Groß, J.; Schafmayer, C.; Frickmann, H.; Weber, M.-A.; et al. Imaging and Clinical Parameters for Distinction between Infected and Non-Infected Fluid Collections in CT: Prospective Study Using Extended Microbiological Approach. Diagnostics 2022, 12, 493. https://doi.org/10.3390/diagnostics12020493
Skusa C, Skusa R, Wohlfarth M, Warnke P, Podbielski A, Bath K, Groß J, Schafmayer C, Frickmann H, Weber M-A, et al. Imaging and Clinical Parameters for Distinction between Infected and Non-Infected Fluid Collections in CT: Prospective Study Using Extended Microbiological Approach. Diagnostics. 2022; 12(2):493. https://doi.org/10.3390/diagnostics12020493
Chicago/Turabian StyleSkusa, Christopher, Romy Skusa, Moritz Wohlfarth, Philipp Warnke, Andreas Podbielski, Kristina Bath, Justus Groß, Clemens Schafmayer, Hagen Frickmann, Marc-André Weber, and et al. 2022. "Imaging and Clinical Parameters for Distinction between Infected and Non-Infected Fluid Collections in CT: Prospective Study Using Extended Microbiological Approach" Diagnostics 12, no. 2: 493. https://doi.org/10.3390/diagnostics12020493