
An In Vivo Observational Histological Study of Peripheral Arterial Damage in Patients with Acute Limb Ischemia in SARS-CoV-2 Infection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
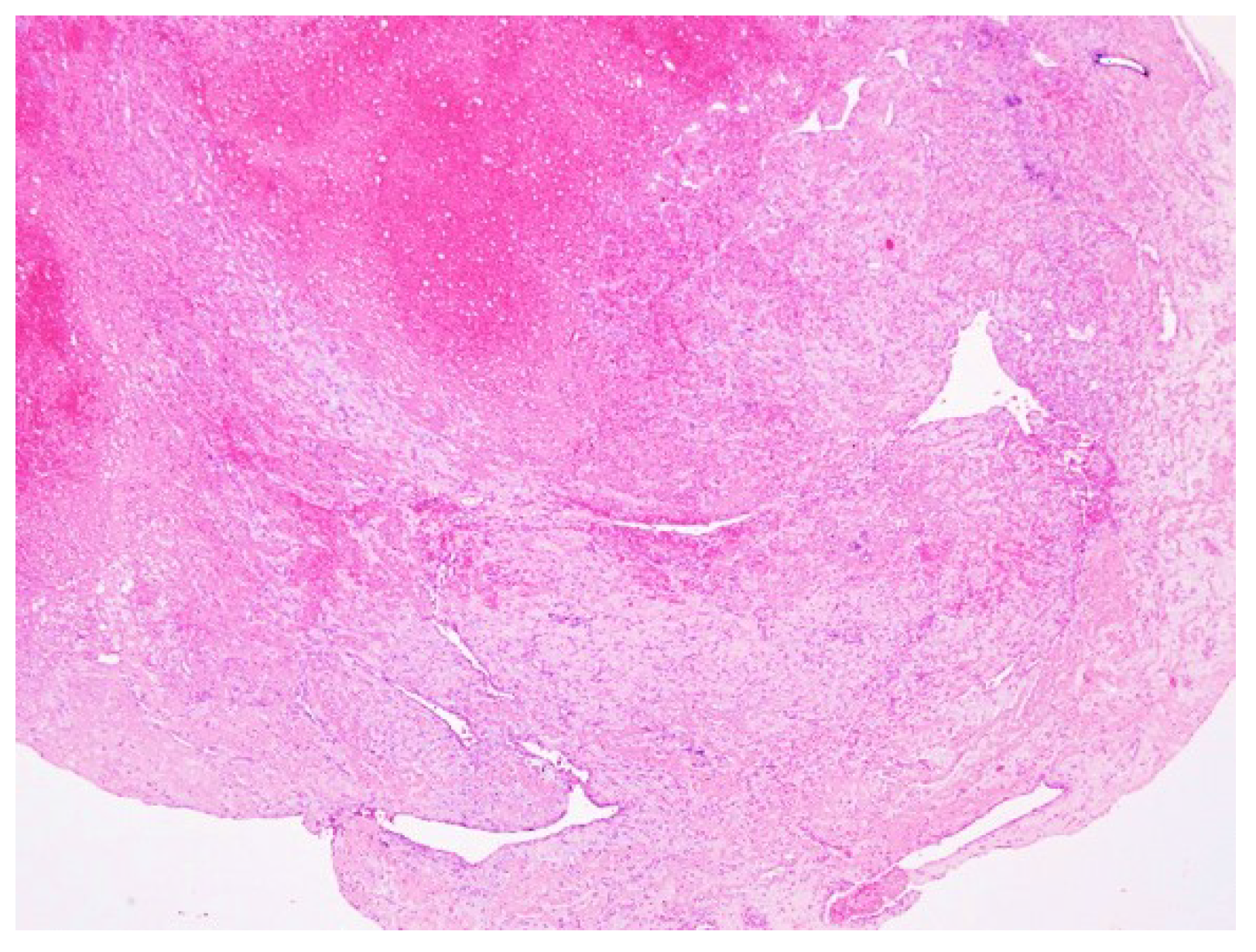
2.2. Histological Methods
2.3. Ethics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 10 January 2022).
- Nicolau, C.; Henter, R.; Roman, N.; Neculau, A.; Miclau, R. Tele-education under the COVID-19 Crisis: Asymmetries in Romanian education. Symmetry 2020, 12, 1502. [Google Scholar] [CrossRef]
- Vermesan, D.; Todor, A.; Andrei, D.; Niculescu, M.; Tudorache, E.; Haragus, H. Effect of COVID-19 Pandemic on orthopedic surgery in three centers from Romania. Int. J. Environ. Res. Public Health 2021, 18, 2196. [Google Scholar] [CrossRef]
- Roman, N.; Cojocaru, D.; Coman, C.; Repanovici, A.; Bou, S.F.; Miclaus, R. Materials for Respiratory Masks in the context of COVID-19 pandemic. Mater. Plast. 2020, 57, 236–247. [Google Scholar] [CrossRef]
- Deshmukh, V.; Motwani, R.; Kumar, A.; Kumari, C.; Raza, K. Hisopathological observations in COVID-19 systematic review. J. Clin. Pathol. 2021, 74, 78–83. [Google Scholar] [CrossRef]
- Tang, N. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential effects of coronaviruses on the cardiovascular system: A review. JAMA Cardiol. 2020, 5, 831. [Google Scholar] [CrossRef] [Green Version]
- Levi, M. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, e438–e440. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef]
- Cheruiyot, I.; Kipkorir, V.; Ngure, B.; Misiani, M.; Munguti, J.; Ogeng’o, J. Arterial Thrombosis in Coronavirus Disease 2019 Patients: A rapid systematic review. Ann. Vasc. Surg. 2021, 70, 273–281. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M. Editor’s choice e 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases; in collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 305e68. [Google Scholar] [CrossRef] [Green Version]
- Björck, M.; Earnshaw, J.J.; Acosta, S.; Gonçalves, F.B.; Cochennec, F.; Debus, E.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.; Menyhei, G.; et al. European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [Google Scholar] [CrossRef] [Green Version]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Zou, Y.; Guo, H.; Zhang, Y.; Zhang, Z.; Liu, Y.; Wang, J.; Lu, H.; Qian, Z. Analysis of coagulation parameters in patients with COVID-19 in Shanghai, China. Biosci. Trends 2020, 14, 285–289. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. Coronavirus disease 2019 (COVID-19): The portrait of a perfect storm. Ann. Transl. Med. 2020, 8, 497. [Google Scholar] [CrossRef]
- Dolhnikoff, M.; Duarte-Neto, A.N.; de Almeida Monteiro, R.A.; Da Silva, L.F.F.; De Oliveira, E.P.; Saldiva, P.H.N.; Mauad, T.; Negri, E.M. Pathological evidence of pulmonary thrombotic phenomena in severe COVID-19. J. Thromb. Haemost. 2020, 18, 1517–1519. [Google Scholar] [CrossRef] [Green Version]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Calabrese, F.; Pessuto, F.; Fortarezza, F.; Boscolo, A.; Lunardi, F.; Giraudo, C.; Catelan, A.; Del Vecchio, C.; Lorenzoni, G.; Vedovelli, L.; et al. Machine learning-based analysis of alveolar and vascular injury in SARS-CoV-2 acute respiratory failure. J. Pathol. 2021, 254, 173–184. [Google Scholar] [CrossRef]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 respiratory distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Roncati, L.; Manenti, A.; Manco, G.; Farinetti, A.; Mattioli, A. The COVID-19 Arterial Thromboembolic Complications: From Inflammation to Immunothrombosis Through Antiphospholipid Autoantibodies. Ann. Vasc. Surg. 2021, 72, 216–217. [Google Scholar] [CrossRef]
- Lucijanic, M.; Stojic, J.; Atic, A.; Cikara, T.; Osmani, B.; Barisic-Jaman, M.; Andrilovic, A.; Bistrovic, P.; Zrilic Vrkljan, A.; Lagancic, M.; et al. Clinical and prognostic significance of C-reactive protein to albumin ration in hospitalized coronavirus disease 2019 (COVID-19) patients: Data on 2309 patiients from a tertiary center and validation in an independent cohort. Wien. Klin. Wochenschr. 2022, 1–8. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.P.; Soric, E.; Sedinic, M.; Sablijic, A.; Derek, L.; Jacksic, O.; Kusek, R. Thrombocytosis in COVID-19 patients without myeloproliferative neoplasmns is associated with better prognosis but higher rate of venous thromboembolism. Blood Cancer J. 2021, 11, 189. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and thrombotic or thromboembolic disease: Implications for prevention, antithrombotic therapy, and follow-up. J. Am. Coll Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Gianotti, R.; Zerbi, P.; Dodiuk-Gad, R.P. Clinical and histopathological study of skin dermatoses in patients affected by COVID-19 infection in the Northern part of Italy. J. Dermatol. Sci. 2020, 98, 141–143. [Google Scholar] [CrossRef]
- Kolivras, A.; Dehavay, F.; Delplace, D.; Feoli, F.; Meiers, I.; Milone, L.; Olemans, C.; Sass, U.; Theunis, A.; Thompson, C.T.; et al. Coronavirus (COVID-19) infection- induced chilblains: A case report with histopathologic findings. JAAD Case Rep. 2020, 6, 489–492. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.-H.; He, Z.-C.; Li, T.-Y.; Zhang, H.-R.; Wang, Y.; Mou, H.; Guo, Q.; Yu, S.-C.; Ding, Y.; Liu, X.; et al. Pathological evidence for residual SARS- CoV-2 in pulmonary tissues of a ready-for-discharge patient. Cell Res. 2020, 30, 541–543. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable, n (%) * | Data |
|---|---|
| General Characteristics | |
| Age, years (mean ± SD) | 64.91 ± 9.57 |
| Sex, male | 15 (68.18) |
| BMI, kg/m2 (mean ± SD) | 31.63 ± 6.47 |
| Smoking | 10 (45.45%) |
| Ischemia time, hours (median, IQR) | 18.59 (5–34) |
| Preoperative antiplatelet treatment | 19 (86.36) |
| Comorbidities | |
| Heart Failure | 8 (36.36) |
| Obesity | 16 (72.72) |
| Diabetes mellitus | 14 (63.64) |
| Dyslipidemia | 18 (85.71) |
| Arterial hypertension | 22 (100) |
| Chronic obstructive pulmonary disease | 4 (18.18) |
| Cerebrovascular disease | 4 (18.18) |
| Malignancy | 2 (9.09) |
| Rutherford classification | |
| IIA | 15 (68.18) |
| IIB | 7 (31.81) |
| Characteristic | Patients’ Values | Range Values |
|---|---|---|
| Leukocyte count (no.×103/L), median [IQR] | 8.35 [5.34–14.28] | 4–9.5 |
| Neutrophils (%), mean ± SD | 62.28 ± 12.42 | 45–70% |
| Erythrocyte count (no.×103/L), median [IQR] | 3.64 [3.45–4.24] | 4–5.5 |
| Monocyte, median [IQR] | 7.34 [2.89–8.28] | 3.5–9% |
| Lymphocyte (no.×10), median [IQR] | 1.33 [1.09–1.77] | 0.8–3.8 |
| Haemoglobin level (g/dL), median [IQR] | 10.70 [10.31–11.40] | 11.5–15 |
| Haematocrit (%), mean ± SD | 34.08 ± 3.47 | 35–46 |
| Platelet count, mean ± SD | 275,545 ± 82,299 | 150–400 |
| LDH, median [IQR] | 278 [161.3–346.5] | 120–246 |
| Ferritin level (µg/L), mean ± SD | 728.9 ± 158.5 | 20–290 |
| CRP level (mg/L), mean ± SD | 68.08 ± 23.67 | 0–10 |
| aPTT (s), median [IQR] | 29.4 [24.4–35.41] | 25.1–36.5 |
| Quick time (s), median [IQR] | 14.67 [12.68–15.61] | 9.4–12.5 |
| INR, mean ± SD | 1.27 ± 0.18 | 0.8–1.07 |
| VSH (mm/1 h), mean ± SD | 82.41 ± 22.26 | 1–15 |
| AST (U/L), median [IQR] | 23.5 [18–28.25] | 14–36 |
| ALT (U/L), mean ± SD | 23.91 ± 10.45 | 0–35 |
| DDimers (ng/mL) mean ± SD | 957 ± 518.6 | 0–243 |
| Urea (mg/dL), median [IQR] | 30 [23–45] | 15–36 |
| Creatinine (mg/dL), median [IQR] | 0.89 [0.7–1.42] | 0.7–1.2 |
| Fibrinogen (mg/dL), mean ± SD | 668 ± 168.3 | 200–393 |
| CK (U/L), median [IQR] | 115 [43.75–508.8] | 30–170 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barac, S.; Onofrei, R.R.; Lazureanu, C.; Barna, R.; Tutelca, A.; Rata, A.L. An In Vivo Observational Histological Study of Peripheral Arterial Damage in Patients with Acute Limb Ischemia in SARS-CoV-2 Infection. Diagnostics 2022, 12, 488. https://doi.org/10.3390/diagnostics12020488
Barac S, Onofrei RR, Lazureanu C, Barna R, Tutelca A, Rata AL. An In Vivo Observational Histological Study of Peripheral Arterial Damage in Patients with Acute Limb Ischemia in SARS-CoV-2 Infection. Diagnostics. 2022; 12(2):488. https://doi.org/10.3390/diagnostics12020488
Chicago/Turabian StyleBarac, Sorin, Roxana Ramona Onofrei, Codruta Lazureanu, Robert Barna, Adrian Tutelca, and Andreea Luciana Rata. 2022. "An In Vivo Observational Histological Study of Peripheral Arterial Damage in Patients with Acute Limb Ischemia in SARS-CoV-2 Infection" Diagnostics 12, no. 2: 488. https://doi.org/10.3390/diagnostics12020488