
Validation of PH and Varices Risk Scores for Prediction of High-Risk Esophageal Varix and Bleeding in Patients with B-Viral Cirrhosis

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Clinical Assessment and Calculation of PH and Varices Risk Scores
2.3. Patient Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics among the Training Cohort
3.2. Predictive Performances of Noninvasive Models to Detect the HEVs and Determine the Useful Cutoff Value in the Training Cohort
3.3. Predictive Performances of Noninvasive Models to Detect the HEVs in the Validation Cohort
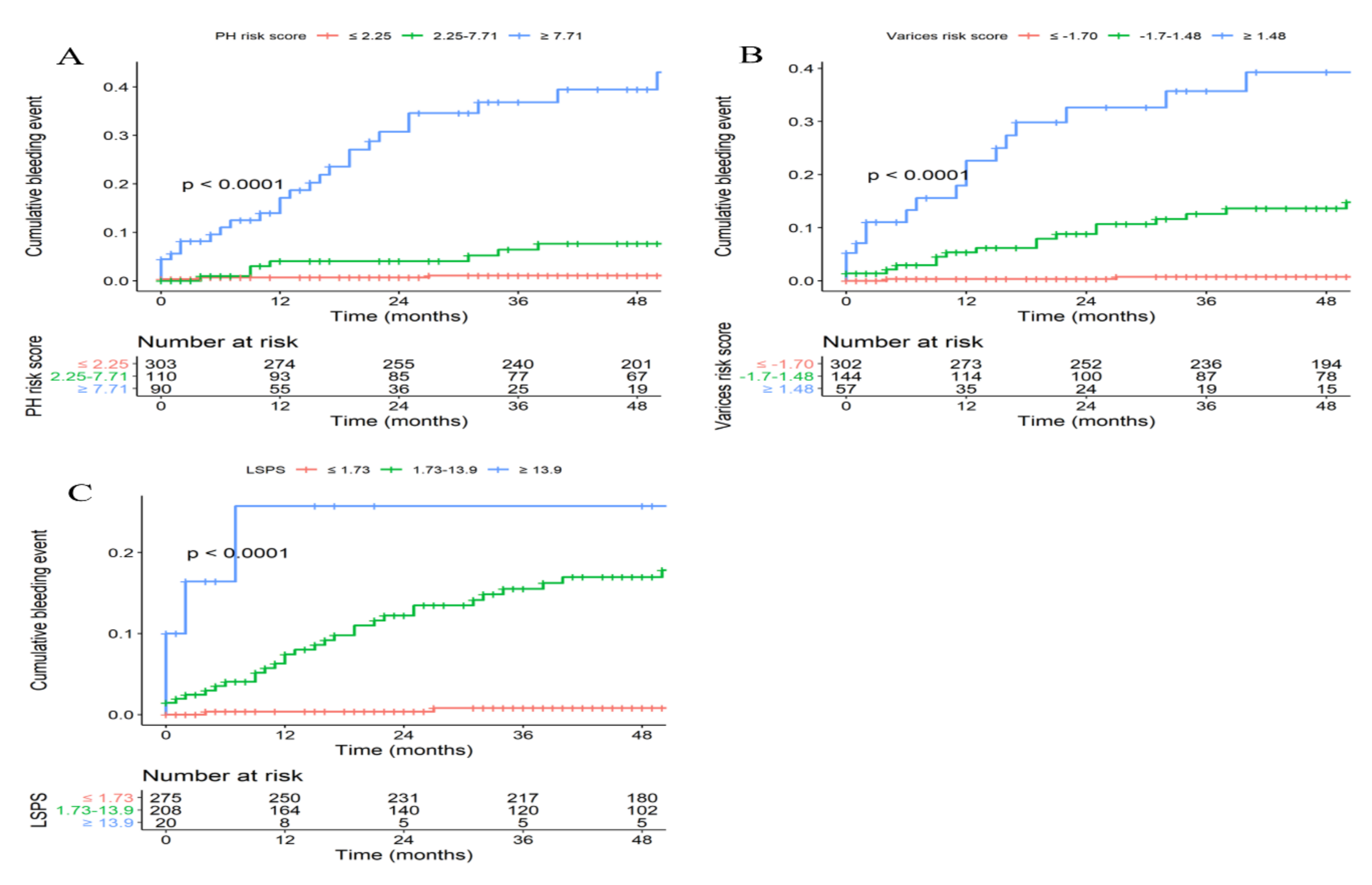
3.4. EVB Risk during Follow-Up in the Training Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garcia-Tsao, G.; Sanyal, A.J.; Grace, N.D.; Carey, W.D. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Am. J. Gastroenterol. 2007, 102, 2086–2102. [Google Scholar] [CrossRef] [PubMed]
- The Korean Association for the Study of the Liver (KASL). Kasl clinical practice guidelines for liver cirrhosis: Varices, hepatic encephalopathy, and related complications. Clin. Mol. Hepatol. 2020, 26, 83–127. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Yu, J.H.; Jin, Y.J.; Yim, H.J.; Jung, Y.K.; Yang, J.M.; Song, D.S.; Kim, Y.S.; Kim, S.G.; Kim, D.J.; et al. Acute-on-chronic liver failure as a major predictive factor for mortality in patients with variceal bleeding. Clin. Mol. Hepatol. 2020, 26, 540–553. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Jo, J.H.; Kim, S.E.; Bang, C.S.; Seo, S.I.; Park, C.H.; Park, S.W. Minimal and Maximal Extent of Band Ligation for Acute Variceal Bleeding during the First Endoscopic Session. Gut Liver 2022, 16, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef] [Green Version]
- de Franchis, R. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Lesmana, C.R.A.; Raharjo, M.; Gani, R.A. Managing liver cirrhotic complications: Overview of esophageal and gastric varices. Clin. Mol. Hepatol. 2020, 26, 444–460. [Google Scholar] [CrossRef]
- de Franchis, R.; Primignani, M. Natural history of portal hypertension in patients with cirrhosis. Clin. Liver Dis. 2001, 5, 645–663. [Google Scholar] [CrossRef]
- Giannini, E.; Botta, F.; Borro, P.; Risso, D.; Romagnoli, P.; Fasoli, A.; Mele, M.R.; Testa, E.; Mansi, C.; Savarino, V.; et al. Platelet count/spleen diameter ratio: Proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis. Gut 2003, 52, 1200–1205. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, F.; Kettaneh, A.; N’Kontchou, G.; Pinto, E.; Ganne-Carrie, N.; Trinchet, J.C.; Beaugrand, M. Liver stiffness measurement selects patients with cirrhosis at risk of bearing large oesophageal varices. J. Hepatol. 2006, 45, 230–235. [Google Scholar] [CrossRef]
- Gentile, I.; Viola, C.; Graf, M.; Liuzzi, R.; Quarto, M.; Cerini, R.; Piazza, M.; Borgia, G. A simple noninvasive score predicts gastroesophageal varices in patients with chronic viral hepatitis. J. Clin. Gastroenterol. 2009, 43, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Vizzutti, F.; Arena, U.; Romanelli, R.G.; Rega, L.; Foschi, M.; Colagrande, S.; Petrarca, A.; Moscarella, S.; Belli, G.; Zignego, A.L.; et al. Liver stiffness measurement predicts severe portal hypertension in patients with HCV-related cirrhosis. Hepatology 2007, 45, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Gilabert, R.; Abraldes, J.G.; Nicolau, C.; Bru, C.; Bosch, J.; García-Pagan, J.C. Noninvasive prediction of clinically significant portal hypertension and esophageal varices in patients with compensated liver cirrhosis. Am. J. Gastroenterol. 2008, 103, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Giannini, E.G.; Zaman, A.; Kreil, A.; Floreani, A.; Dulbecco, P.; Testa, E.; Sohaey, R.; Verhey, P.; Peck-Radosavljevic, M.; Mansi, C.; et al. Platelet count/spleen diameter ratio for the noninvasive diagnosis of esophageal varices: Results of a multicenter, prospective, validation study. Am. J. Gastroenterol. 2006, 101, 2511–2519. [Google Scholar] [CrossRef]
- Alempijevic, T.; Kovacevic, N. Right liver lobe diameter:albumin ratio: A new non-invasive parameter for prediction of oesophageal varices in patients with liver cirrhosis (preliminary report). Gut 2007, 56, 1166–1167, authro reply 1167. [Google Scholar]
- Sohn, W.; Chang, Y.; Cho, Y.K.; Hong, Y.S.; Shin, H.; Ryu, S. Liver fibrosis scores and risk of liver-related mortality in young adults with chronic hepatitis B: A cohort study. J. Viral Hepat. 2022, 29, 69–77. [Google Scholar] [CrossRef]
- Wang, H.; Wen, B.; Chang, X.; Wu, Q.; Wen, W.; Zhou, F.; Guo, Y.; Ji, Y.; Gu, Y.; Lai, Q.; et al. Baveno VI criteria and spleen stiffness measurement rule out high-risk varices in virally suppressed HBV-related cirrhosis. J. Hepatol. 2021, 74, 584–592. [Google Scholar] [CrossRef]
- Augustin, S.; Pons, M.; Maurice, J.B.; Bureau, C.; Stefanescu, H.; Ney, M.; Blasco, H.; Procopet, B.; Tsochatzis, E.; Westbrook, R.H.; et al. Expanding the Baveno VI criteria for the screening of varices in patients with compensated advanced chronic liver disease. Hepatology 2017, 66, 1980–1988. [Google Scholar] [CrossRef]
- Kim, B.K.; Han, K.H.; Park, J.Y.; Ahn, S.H.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Chon, C.Y.; Kim, D.Y. A liver stiffness measurement-based, noninvasive prediction model for high-risk esophageal varices in B-viral liver cirrhosis. Am. J. Gastroenterol. 2010, 105, 1382–1390. [Google Scholar] [CrossRef]
- Lee, H.A.; Kim, S.U.; Seo, Y.S.; Lee, Y.S.; Kang, S.H.; Jung, Y.K.; Kim, M.Y.; Kim, J.H.; Kim, S.G.; Suk, K.T.; et al. Prediction of the varices needing treatment with non-invasive tests in patients with compensated advanced chronic liver disease. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39, 1071–1079. [Google Scholar] [CrossRef]
- Berzigotti, A.; Seijo, S.; Arena, U.; Abraldes, J.G.; Vizzutti, F.; García-Pagán, J.C.; Pinzani, M.; Bosch, J. Elastography, spleen size, and platelet count identify portal hypertension in patients with compensated cirrhosis. Gastroenterology 2013, 144, 102–111.e101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, J.; Berzigotti, A.; Garcia-Pagan, J.C.; Abraldes, J.G. The management of portal hypertension: Rational basis, available treatments and future options. J. Hepatol. 2008, 48 (Suppl. S1), S68–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Kim, S.S.; Chang, D.R.; Kim, H.; Kim, M.J. Comparison of LI-RADS 2018 and KLCA-NCC 2018 for noninvasive diagnosis of hepatocellular carcinoma using magnetic resonance imaging. Clin. Mol. Hepatol. 2020, 26, 340–351. [Google Scholar] [CrossRef]
- Yim, H.J.; Kim, J.H.; Park, J.Y.; Yoon, E.L.; Park, H.; Kwon, J.H.; Sinn, D.H.; Lee, S.H.; Lee, J.H.; Lee, H.W. Comparison of clinical practice guidelines for the management of chronic hepatitis B: When to start, when to change, and when to stop. Clin. Mol. Hepatol. 2020, 26, 411–429. [Google Scholar] [CrossRef]
- Na, J.E.; Sinn, D.H.; Lee, J.H.; Jang, H.J.; Baek, S.Y.; Kim, K.A.; Kang, W.S.; Gwak, G.Y.; Paik, Y.H.; Kim, Y.J.; et al. Efficacy of entecavir versus tenofovir in preventing hepatocellular carcinoma in patients with chronic hepatitis B with maintained virologic response. J. Viral Hepat. 2021, 28, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Cho, Y.Y.; Lee, H.; Lee, J.S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, B.K.; Park, S.Y. Impact of tenofovir alafenamide vs. entecavir on hepatocellular carcinoma risk in patients with chronic hepatitis B. Hepatol. Int. 2021, 15, 1083–1092. [Google Scholar] [CrossRef]
- Lee, H.W.; Cho, Y.Y.; Lee, H.; Lee, J.S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, B.K.; Park, S.Y. Effect of tenofovir alafenamide vs. tenofovir disoproxil fumarate on hepatocellular carcinoma risk in chronic hepatitis B. J. Viral Hepat. 2021, 28, 1570–1578. [Google Scholar] [CrossRef]
- Kim, B.K.; Kim, D.Y.; Han, K.H.; Park, J.Y.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Chon, C.Y.; Ahn, S.H. Risk assessment of esophageal variceal bleeding in B-viral liver cirrhosis by a liver stiffness measurement-based model. Am. J. Gastroenterol. 2011, 106, 1654–1662, 1730. [Google Scholar] [CrossRef]
- Ryu, S.R.; Yoo, J.J.; Kang, S.H.; Jeong, S.W.; Kim, M.Y.; Cho, Y.K.; Chang, Y.; Kim, S.G.; Jang, J.Y.; Kim, Y.S.; et al. The cut-off value of transient elastography to the value of hepatic venous pressure gradient in alcoholic cirrhosis. Clin. Mol. Hepatol. 2021, 27, 197–206. [Google Scholar] [CrossRef]
- Pons, M.; Augustin, S.; Scheiner, B.; Guillaume, M.; Rosselli, M.; Rodrigues, S.G.; Stefanescu, H.; Ma, M.M.; Mandorfer, M.; Mergeay-Fabre, M.; et al. Noninvasive Diagnosis of Portal Hypertension in Patients With Compensated Advanced Chronic Liver Disease. Am. J. Gastroenterol. 2021, 116, 723–732. [Google Scholar] [CrossRef]
- Berzigotti, A. Non-invasive evaluation of portal hypertension using ultrasound elastography. J. Hepatol. 2017, 67, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Ikejima, K.; Kon, K.; Yamashina, S. Nonalcoholic fatty liver disease and alcohol-related liver disease: From clinical aspects to pathophysiological insights. Clin. Mol. Hepatol. 2020, 26, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, B.; Valdes, J.D.; Sun, J.; Guo, H. Serum HBV RNA: A New Potential Biomarker for Chronic Hepatitis B Virus Infection. Hepatology 2019, 69, 1816–1827. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Tanaka, Y. Novel biomarkers for the management of chronic hepatitis B. Clin. Mol. Hepatol. 2020, 26, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.S.; Zhou, K.; Terrault, N.A. New and Old Biomarkers for Diagnosis and Management of Chronic Hepatitis B Virus Infection. Gastroenterology 2019, 156, 355–368.e353. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Park, Y.N.; Han, D.H.; Kim, K.S.; et al. Serum Wisteria floribunda agglutinin-positive human Mac-2 binding protein level predicts recurrence of hepatitis B virus-related hepatocellular carcinoma after curative resection. Clin. Mol. Hepatol. 2020, 26, 33–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, S.; Kurosaki, M.; Inada, K.; Kirino, S.; Hayakawa, Y.; Yamashita, K.; Osawa, L.; Sekiguchi, S.; Higuchi, M.; Takaura, K.; et al. Hepatitis B core-related antigen predicts disease progression and hepatocellular carcinoma in hepatitis B e antigen-negative chronic hepatitis B patients. J. Gastroenterol. Hepatol. 2021, 36, 2943–2951. [Google Scholar] [CrossRef]
- Zhang, M.; Li, G.; Shang, J.; Pan, C.; Zhang, M.; Yin, Z.; Xie, Q.; Peng, Y.; Mao, Q.; Xiao, X.; et al. Rapidly decreased HBV RNA predicts responses of pegylated interferons in HBeAg-positive patients: A longitudinal cohort study. Hepatol. Int. 2020, 14, 212–224. [Google Scholar] [CrossRef] [Green Version]
- Mak, L.Y.; Huang, Q.; Wong, D.K.; Stamm, L.; Cheung, K.S.; Ko, K.L.; Yan, R.; Ouyang, L.; Fung, J.; Seto, W.K.; et al. Residual HBV DNA and pgRNA viraemia is associated with hepatocellular carcinoma in chronic hepatitis B patients on antiviral therapy. J. Gastroenterol. 2021, 56, 479–488. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Age, years | 53.0 ± 8.9 |
| Male | 347 (69.0) |
| Presence of HEV | 146 (29.0) |
| Child–Pugh class A/B | 484 (96.2)/19 (3.8) |
| Ascites | 82 (16.3) |
| AST, U/L | 47.1 ± 50.8 |
| ALT, U/L | 43.8 ± 57.4 |
| Albumin, g/dL | 4.2 ± 2.0 |
| Total bilirubin, mg/dL | 1.6 ± 3.7 |
| PT-INR | 1.1 ± 0.2 |
| Platelet count, ×109/L | 129.6 ± 63.3 |
| LS, kPa | 22.6 ± 18.8 |
| Spleen diameter, cm | 11.6 ± 2.6 |
| LSPS | 3.3 ± 4.2 |
| PH risk score | 2.7 ± 5.1 |
| Varices risk score | −2.9 ± 3.7 |
| Cutoff Values | NPV (95% CI) | PPV (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|
| PH score ≤ 2.25 | 95.0% (92.0–97.2) | 65.5% (58.5–72.1) | 89.7% (83.6–94.1) | 80.7% (76.2–84.6) |
| PH score ≥ 7.71 | 84.3% (80.4–87.6) | 90.0% (81.9–95.3) | 55.5% (47.0–63.7) | 97.5% (95.3–98.8) |
| Varices score ≤ −1.70 | 95.0% (91.9–97.2) | 65.2% (58.2–71.7) | 89.7% (83.6–94.1) | 80.4% (75.9–84.4) |
| Varices score ≥ 1.48 | 78.9% (74.8–82.6) | 91.2% (80.7–97.1) | 35.6% (27.9–44.0) | 98.6% (96.8–99.5) |
| LSPS ≤ 1.73 | 95.3% (92.1–97.5) | 58.3% (51.6–64.8) | 91.1% (85.3–95.2) | 73.4% (68.5–77.9) |
| LSPS ≥ 13.9 | 73.7% (69.5–77.6) | 95.0% (75.1–99.9) | 13.0% (8.0–19.6) | 99.7% (98.4–100) |
| Scoring Model | NPV ≥ 95% (Cutoff) | PPV ≥ 90% (Cutoff) |
|---|---|---|
| PH risk score | 88.2% (≤2.25) | 62.2% (≥7.71) |
| Varices risk score | 93.2% (≤−1.70) | 45.8% (≥1.48 |
| LSPS | 88.9% (≤1.73) | 83.3% (≥13.9) |
| Scoring Model | 24 Month | 48 Month |
|---|---|---|
| PH risk score | 91.7% | 91.0% |
| Varices risk score | 89.2% | 88.2% |
| LSPS | 91.0% | 90.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, B.K. Validation of PH and Varices Risk Scores for Prediction of High-Risk Esophageal Varix and Bleeding in Patients with B-Viral Cirrhosis. Diagnostics 2022, 12, 441. https://doi.org/10.3390/diagnostics12020441
Shin S, Kim SU, Park JY, Kim DY, Ahn SH, Kim BK. Validation of PH and Varices Risk Scores for Prediction of High-Risk Esophageal Varix and Bleeding in Patients with B-Viral Cirrhosis. Diagnostics. 2022; 12(2):441. https://doi.org/10.3390/diagnostics12020441
Chicago/Turabian StyleShin, Seunghwan, Seung Up Kim, Jun Yong Park, Do Young Kim, Sang Hoon Ahn, and Beom Kyung Kim. 2022. "Validation of PH and Varices Risk Scores for Prediction of High-Risk Esophageal Varix and Bleeding in Patients with B-Viral Cirrhosis" Diagnostics 12, no. 2: 441. https://doi.org/10.3390/diagnostics12020441