
Development, Analytical, and Clinical Evaluation of Rapid Immunochromatographic Antigen Test for SARS-CoV-2 Variants Detection

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Colloidal Gold Conjugation
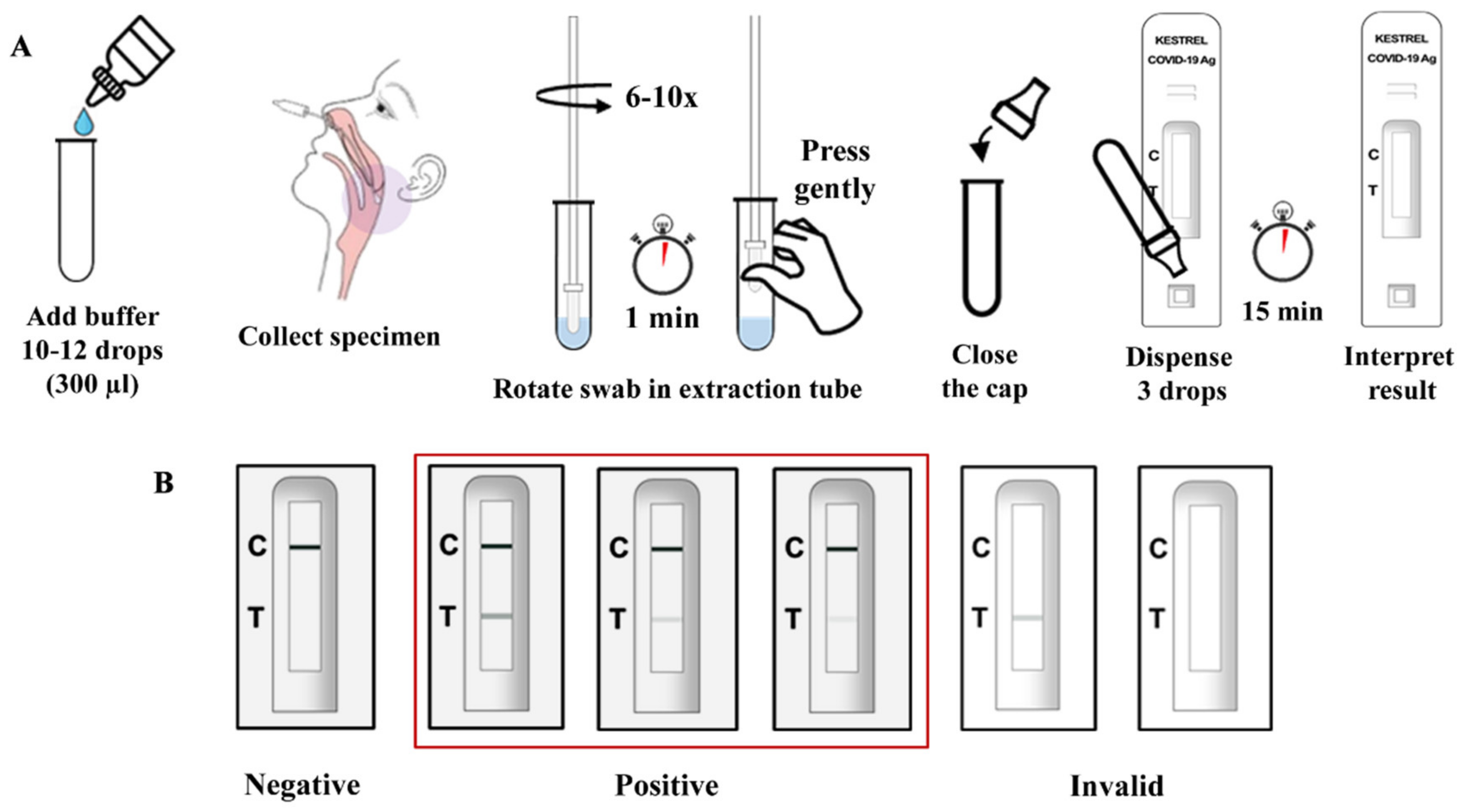
2.3. Assembly of Antigen Test Kit
2.4. Limit of Detection (LOD)
2.5. Cross-Reactivity and Interference Testing
2.6. Clinical Specimens
2.7. Viral RNA Extraction
2.8. Real-Time PCR Detection of SARS-CoV-2 RNA Detection
2.9. Clinical Evaluation Study of the Rapid Antigen Test
2.10. Statistical Analysis
3. Results
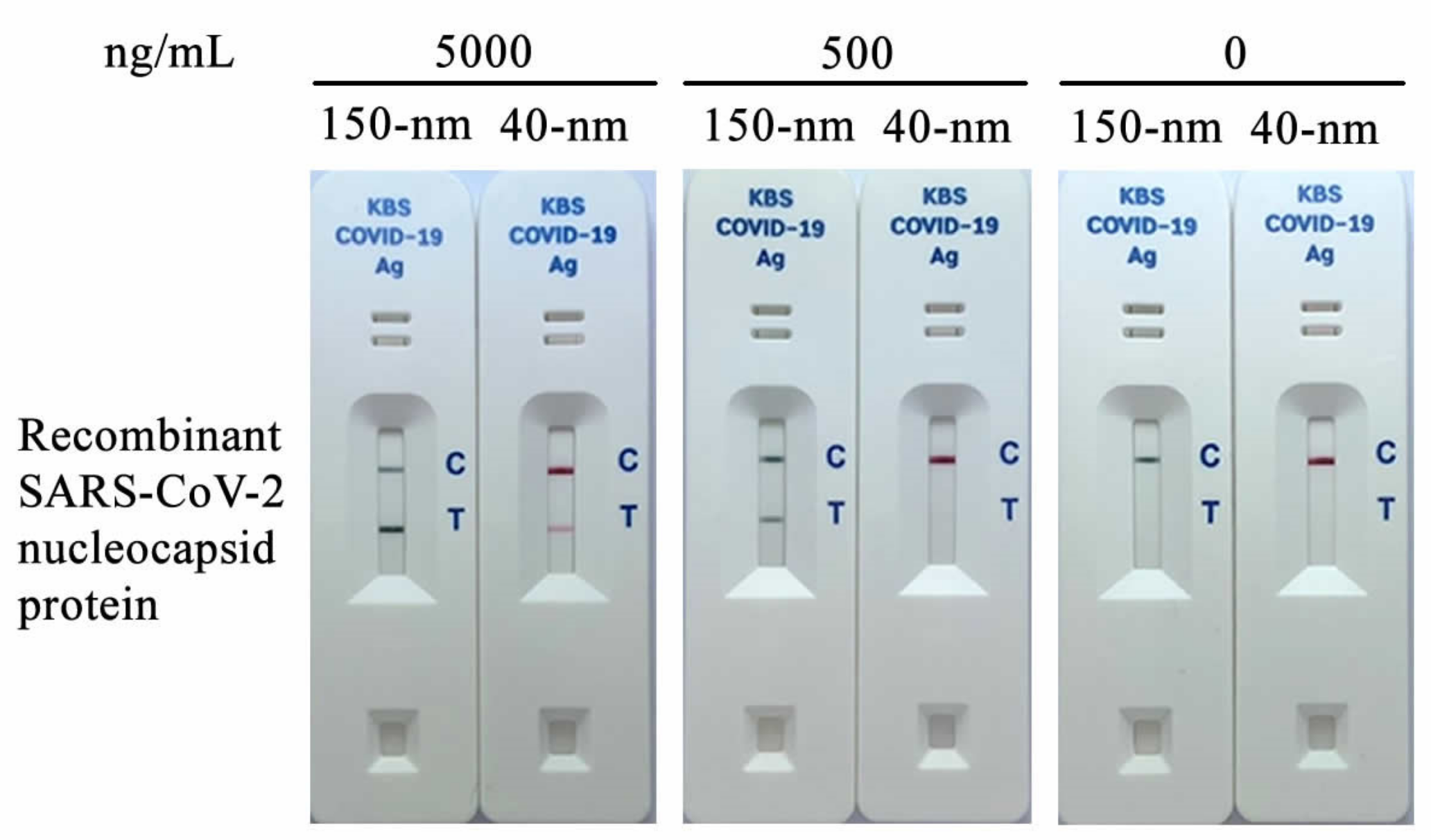
3.1. Selection of Gold Nanoparticles
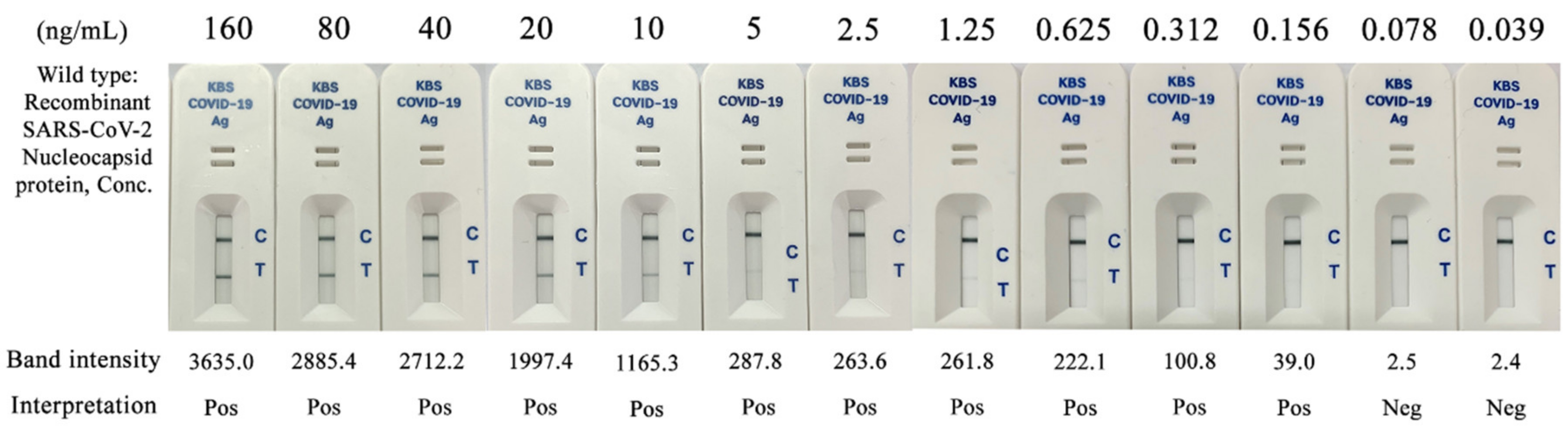
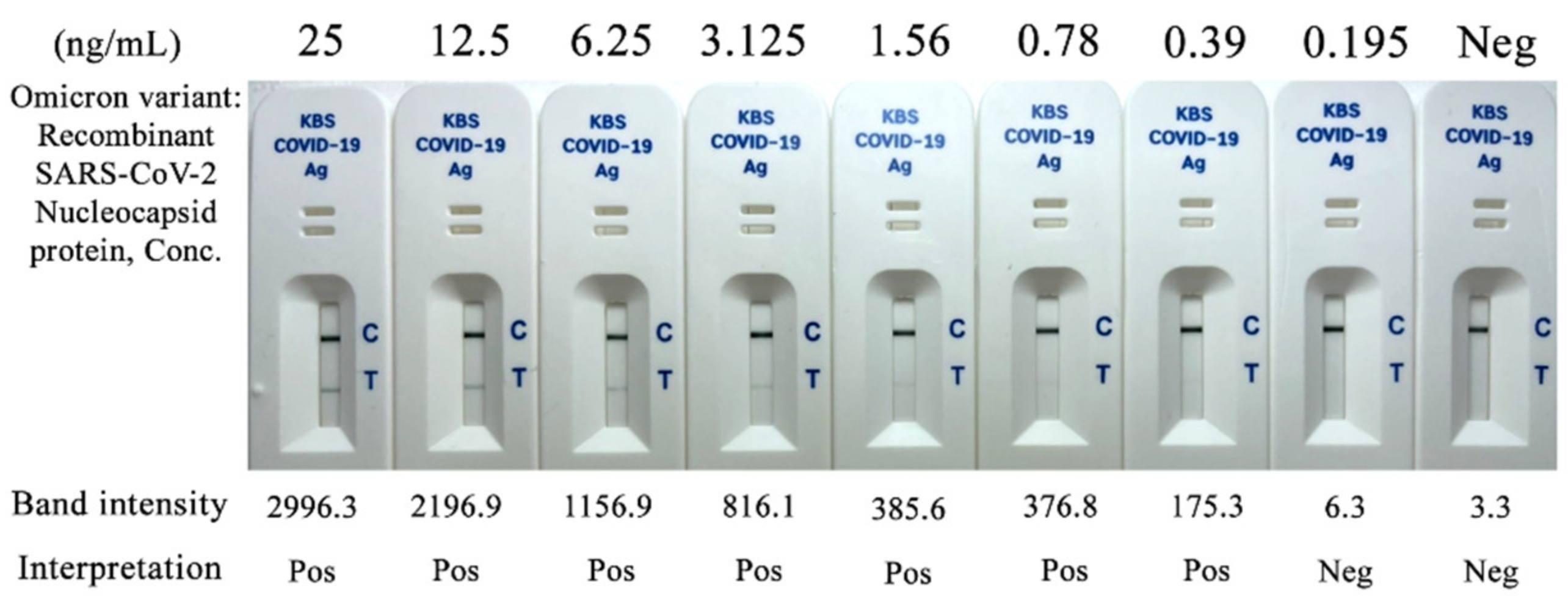
3.2. Limit of Detection (LOD) and Variant Detection of the KestrelTM COVID-19 Ag Rapid Test Kit
3.3. Cross-Reactivity and Interference
3.4. Clinical Evaluation of the KestrelTM COVID-19 Ag Rapid Test Kit
3.4.1. Real-Time RT-PCR
3.4.2. KestrelTM COVID-19 Antigen Test Kit
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feng, W.; Zong, W.; Wang, F.; Ju, S. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): A review. Mol. Cancer 2020, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Karim, S.S.A.; Sridhar, D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef]
- Dyson, L.; Hill, E.M.; Moore, S.; Curran-Sebastian, J.; Tildesley, M.J.; Lythgoe, K.A.; House, T.; Pellis, L.; Keeling, M.J. Possible future waves of SARS-CoV-2 infection generated by variants of concern with a range of characteristics. Nat. Commun. 2021, 12, 5730. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021, 8, CD013705. [Google Scholar] [CrossRef]
- Jungnick, S.; Hobmaier, B.; Mautner, L.; Hoyos, M.; Haase, M.; Baiker, A.; Lahne, H.; Eberle, U.; Wimmer, C.; Hepner, S.; et al. Detection of the new SARS-CoV-2 variants of concern B.1.1.7 and B.1.351 in five SARS-CoV-2 rapid antigen tests (RATs), Germany, March 2021. Eurosurveillance 2021, 26, 2100413. [Google Scholar] [CrossRef]
- Dinnes, J. COVID-19 Rapid antigen testing strategies require careful evaluation. EBioMedicine 2021, 70, 103491. [Google Scholar] [CrossRef]
- Frew, E.; Roberts, D.; Barry, S.; Holden, M.; Mand, A.R.; Mitsock, E.; Tan, E.; Yu, W.; Skog, J. A SARS-CoV-2 antigen rapid diagnostic test for resource limited settings. Sci. Rep. 2021, 11, 23009. [Google Scholar] [CrossRef]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection Using Rapid Immunoassays: Interim Guidance, 6 October 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Iglòi, Z.; Velzing, J.; van Beek, J.; van de Vijver, D.; Aron, G.; Ensing, R.; Benschop, K.; Han, W.; Boelsums, T.; Koopmans, M.; et al. Clinical evaluation of Roche Sd Biosensor rapid antigen test for SARS-CoV-2 in municipal health service testing site, the Netherlands. Emerg. Infect. Dis. 2021, 27, 1323–1329. [Google Scholar] [CrossRef]
- Nsoga, M.T.N.; Kronig, I.; Rodriguez, F.J.P.; Sattonnet-Roche, P.; da Silva, D.; Helbling, J.; Sacks, J.A.; de Vos, M.; Boehm, E.; Gayet-Ageron, A.; et al. Diagnostic accuracy of Panbio rapid antigen tests on oropharyngeal swabs for detection of SARS-CoV-2. PLoS ONE 2021, 16, e0253321. [Google Scholar] [CrossRef]
- Kim, D.; Lee, J.; Bal, J.; Seo, S.K.; Chong, C.K.; Lee, J.H.; Park, H. Development and clinical evaluation of an immunochromatography-based rapid antigen test (GenbodyTM Covag025) for COVID-19 diagnosis. Viruses 2021, 13, 796. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Nsoga, M.T.N.; Perez-Rodriguez, F.J.; Aad, Y.A.; Sattonnet-Roche, P.; Gayet-Ageron, A.; Jaksic, C.; Torriani, G.; Boehm, E.; Kronig, I.; et al. Diagnostic accuracy of two commercial SARS-CoV-2 antigen-detecting rapid tests at the point of care in community-based testing centers. PLoS ONE 2021, 16, e0248921. [Google Scholar] [CrossRef] [PubMed]
- Homza, M.; Zelena, H.; Janosek, J.; Tomaskova, H.; Jezo, E.; Kloudova, A.; Mrazek, J.; Svagera, Z.; Prymula, R. Five antigen tests for SARS-CoV-2: Virus viability matters. Viruses 2021, 13, 684. [Google Scholar] [CrossRef] [PubMed]
- Department of Medical Sciences, Ministry of Public Health. Department of Medical Sciences Announces Laboratory SARS-CoV2 Detection Network. Available online: https://service.dmsc.moph.go.th/labscovid19/indexen.php (accessed on 13 January 2022).
- Centers for Disease Control and Prevention. Interim Guidelines for Collecting and Handling of Clinical Specimens for COVID-19 Testing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 10 October 2021).
- Mertens, P.; de Vos, N.; Martiny, D.; Jassoy, C.; Mirazimi, A.; Cuypers, L.; van den Wijngaert, S.; Monteil, V.; Melin, P.; Stoffels, K.; et al. Development and potential usefulness of the COVID-19 Ag Respi-Strip diagnostic assay in a pandemic context. Front. Med. 2020, 7, 225. [Google Scholar] [CrossRef] [PubMed]
- Korenkov, M.; Poopalasingam, N.; Madler, M.; Vanshylla, K.; Eggeling, R.; Wirtz, M.; Fish, I.; Dewald, F.; Gieselmann, L.; Lehmann, C.; et al. Evaluation of a rapid antigen test to detect SARS-CoV-2 infection and identify potentially infectious individuals. J. Clin. Microbiol. 2021, 59, e0089621. [Google Scholar] [CrossRef]
- Crozier, A.; Rajan, S.; Buchan, I.; McKee, M. Put to the test: Use of rapid testing technologies for COVID-19. BMJ 2021, 372, n208. [Google Scholar] [CrossRef] [PubMed]
- Patriquin, G.; Davidson, R.J.; Hatchette, T.F.; Head, B.M.; Mejia, E.; Becker, M.G.; Meyers, A.; Sandstrom, P.; Hatchette, J.; Block, A.; et al. Generation of false-positive SARS-CoV-2 antigen results with testing conditions outside manufacturer recommendations: A scientific approach to pandemic misinformation. Microbiol. Spectr. 2021, 9, e0068321. [Google Scholar] [CrossRef]
- Jegerlehner, S.; Suter-Riniker, F.; Jent, P.; Bittel, P.; Nagler, M. Diagnostic accuracy of a SARS-CoV-2 rapid antigen test in real-life clinical settings. Int. J. Infect. Dis. 2021, 109, 118–122. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 variant of concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 7 December 2021).
- Grifoni, A.; Sidney, J.; Zhang, Y.; Scheuermann, R.H.; Peters, B.; Sette, A. A sequence homology and bioinformatic approach can predict candidate targets for immune responses to SARS-CoV-2. Cell Host Microbe 2020, 27, 671.e2–680.e2. [Google Scholar] [CrossRef]
- Che, X.-Y.; Hao, W.; Wang, Y.; Di, B.; Yin, K.; Xu, Y.-C.; Feng, C.-S.; Wan, Z.-Y.; Cheng, V.C.C.; Yuen, K.-Y. Nucleocapsid protein as early diagnostic marker for SARS. Emerg. Infect. Dis. 2004, 10, 1947–1949. [Google Scholar] [CrossRef]
- Chen, X.; Miao, X.; Ma, T.; Leng, Y.; Hao, L.; Duan, H.; Yuan, J.; Li, Y.; Huang, X.; Xiong, Y. Gold nanobeads with enhanced absorbance for improved sensitivity in competitive lateral flow immunoassays. Foods 2021, 10, 1488. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Simundic, A.-M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Richard-Greenblatt, M.; Ziegler, M.J.; Bromberg, V.; Huang, E.; Abdallah, H.; Tolomeo, P.; Lautenbach, E.; Glaser, L.; Kelly, B.J. Impact of nasopharyngeal specimen quality on SARS-CoV-2 test sensitivity. medRxiv 2020. [Google Scholar] [CrossRef]
- Higgins, T.S.; Wu, A.W.; Ting, J.Y. SARS-CoV-2 nasopharyngeal swab testing—false-negative results from a pervasive anatomical misconception. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 993–994. [Google Scholar] [CrossRef] [PubMed]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Haage, V.; de Oliveira-Filho, E.F.; Moreira-Soto, A.; Kühne, A.; Fischer, C.; Sacks, J.A.; Corman, V.M.; Müller, M.A.; Drosten, C.; Drexler, J.F. Impaired performance of SARS-CoV-2 antigen-detecting rapid diagnostic tests at elevated and low temperatures. J. Clin. Virol. 2021, 138, 104796. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Gourgoulianis, K.I. False-positive and false-negative COVID-19 cases: Respiratory prevention and management strategies, vaccination, and further perspectives. Expert Rev. Respir. Med. 2021, 15, 993–1002. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KestrelTM COVID-19 Antigen Test | RT-PCR (Sansure® Novel Coronavirus (2019-nCoV) Nucleic Acid Diagnostic Kit | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 57 | 0 | 57 |
| Negative | 2 | 100 | 102 |
| Total | 59 | 100 | 159 |
| KestrelTM COVID-19 Antigen Test | RT-PCR (Sansure® Novel Coronavirus (2019-nCoV) Nucleic Acid Diagnostic Kit | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 59 | 0 | 59 |
| Negative | 1 | 100 | 101 |
| Total | 60 | 100 | 160 |
| Clinical Evaluation | Hat Yai Hospital | Ramathibodi Hospital | Accepted Criteria by Thai FDA |
|---|---|---|---|
| %Sensitivity (95%CI) | 96.49% (87.89–99.57%) | 98.33% (91.06–99.96%) | ≥90% |
| Specificity (95%CI) | 100% (97.49–100%) | 100% (96.38–100%) | ≥98% |
| Accuracy (95%CI) | 99.01% (96.47–99.88%) | 99.44% (NR) * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szekely, J.; Mongkolprasert, J.; Jeayodae, N.; Senorit, C.; Chaimuti, P.; Swangphon, P.; Nanakorn, N.; Nualnoi, T.; Wongwitwichot, P.; Pengsakul, T. Development, Analytical, and Clinical Evaluation of Rapid Immunochromatographic Antigen Test for SARS-CoV-2 Variants Detection. Diagnostics 2022, 12, 381. https://doi.org/10.3390/diagnostics12020381
Szekely J, Mongkolprasert J, Jeayodae N, Senorit C, Chaimuti P, Swangphon P, Nanakorn N, Nualnoi T, Wongwitwichot P, Pengsakul T. Development, Analytical, and Clinical Evaluation of Rapid Immunochromatographic Antigen Test for SARS-CoV-2 Variants Detection. Diagnostics. 2022; 12(2):381. https://doi.org/10.3390/diagnostics12020381
Chicago/Turabian StyleSzekely, Jidapa, Jenureeyah Mongkolprasert, Nitikorn Jeayodae, Chadarat Senorit, Panuttha Chaimuti, Piyawut Swangphon, Natthaphon Nanakorn, Teerapat Nualnoi, Paweena Wongwitwichot, and Theerakamol Pengsakul. 2022. "Development, Analytical, and Clinical Evaluation of Rapid Immunochromatographic Antigen Test for SARS-CoV-2 Variants Detection" Diagnostics 12, no. 2: 381. https://doi.org/10.3390/diagnostics12020381