
From NTM (Nontuberculous mycobacterium) to Gordonia bronchialis—A Diagnostic Challenge in the COPD Patient

 , , ,
, , ,
Abstract
:1. Introduction
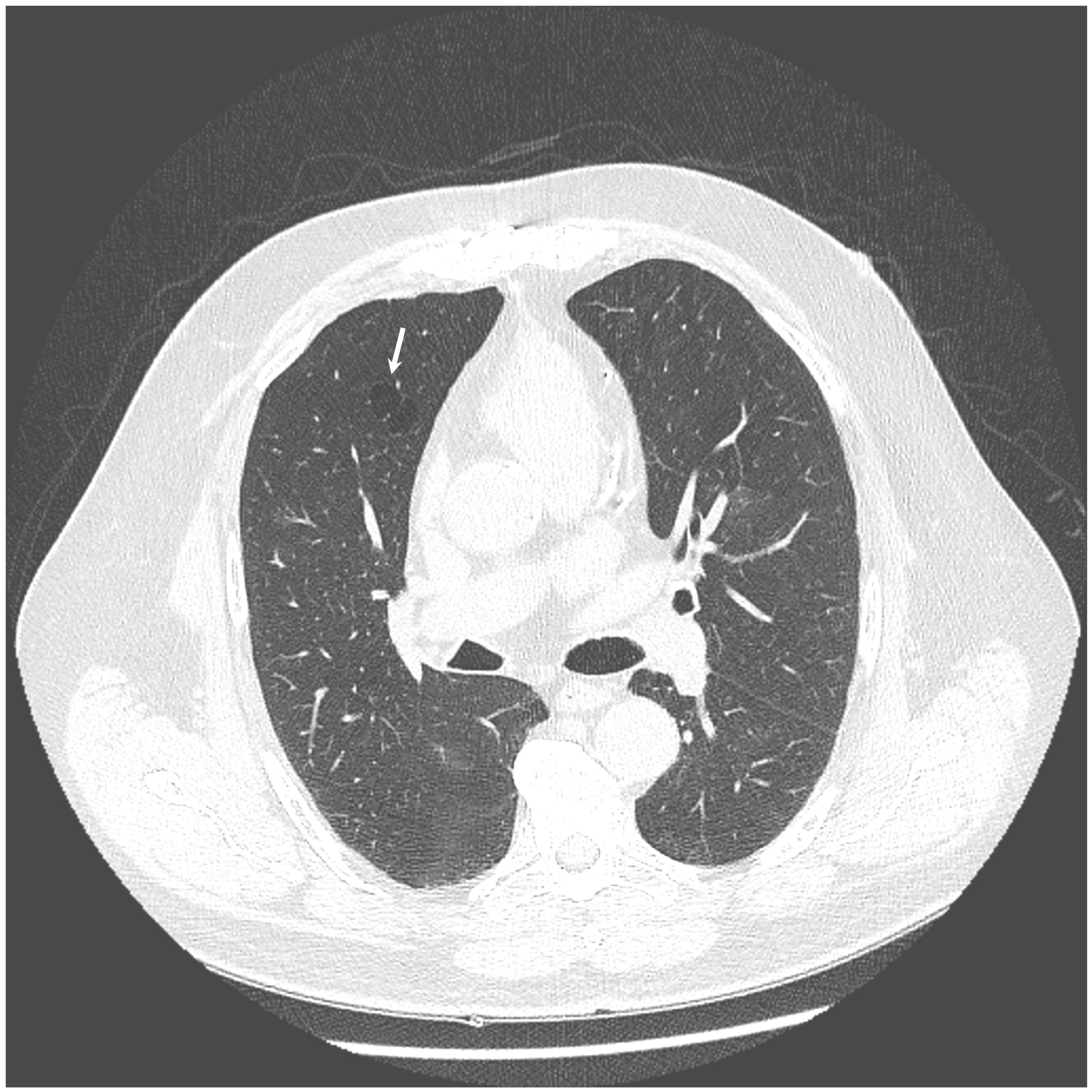
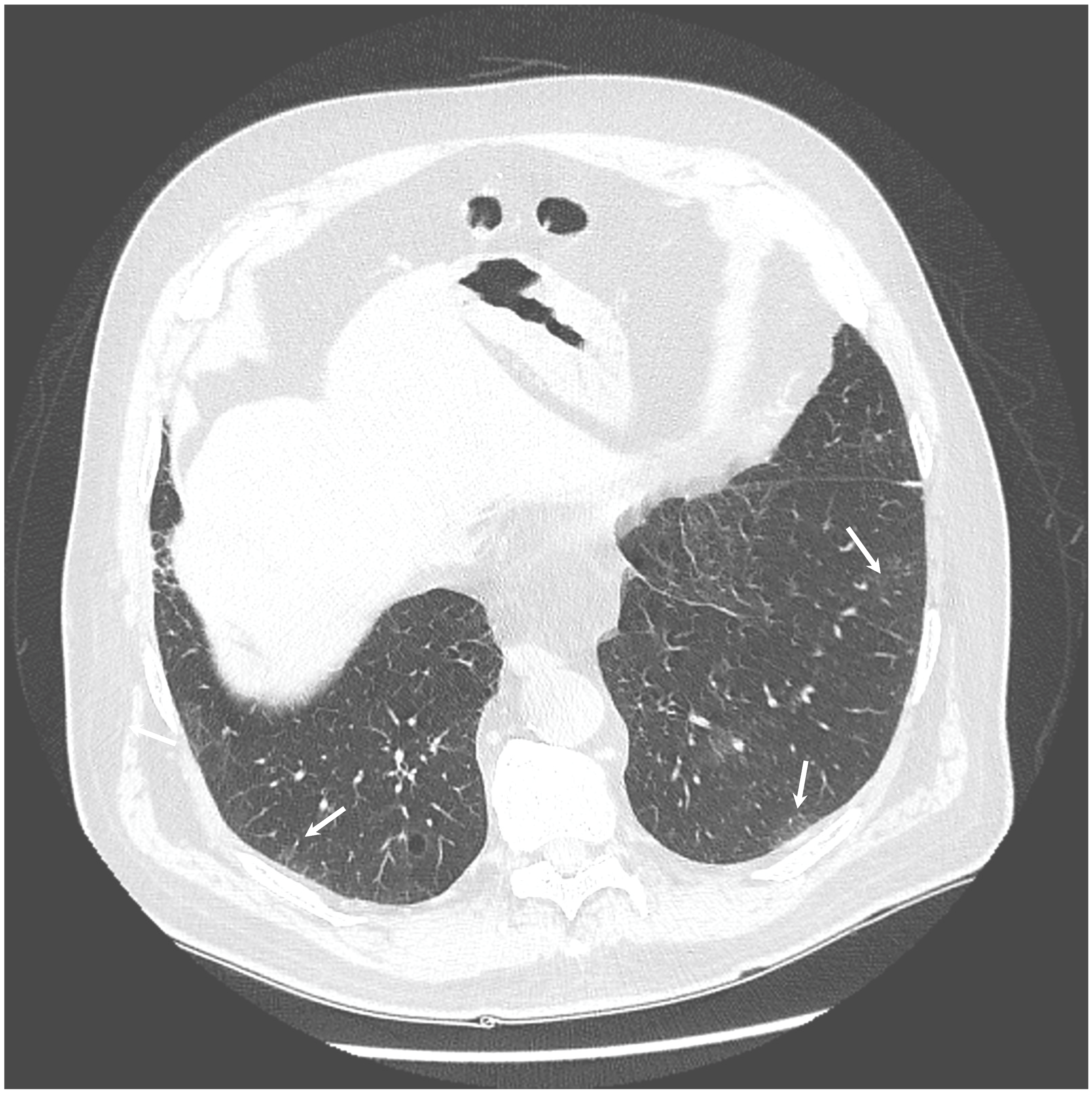
2. Case Presentation
3. Gene Sequencing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsukamura, M. Proposal of a new genus, Gordona, for slightly acid-fast organisms occurring in sputa of patients with pulmonary disease and in soil. J. Gen. Microbiol. 1971, 68, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.A.; Onderdonk, A.B.; Cosimi, L.A.; Yawetz, S.; Lasker, B.A.; Bolcen, S.J.; Brown, J.M.; Marty, F.M. CASE REPORTS Gordonia bronchialis Bacteremia and Pleural Infection: Case Report and Review of the Literature. J. Clin. Microbiol. 2011, 49, 1662–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, N.; Toumeh, A.; Georgescu, C. Tibial osteomyelitis caused by Gordonia bronchialis in an immunocompetent patient. J. Clin. Microbiol. 2012, 50, 3119–3121. [Google Scholar] [CrossRef] [Green Version]
- Bartolomé-Álvarez, J.; Sáez-Nieto, J.A.; Escudero-Jiménez, A.; Barba-Rodríguez, N.; Galán-Ros, J.; Carrasco, G.; Muñoz-Izquierdo, M.P. Cutaneous abscess due to Gordonia bronchialis: Case report and literature review. Rev. Esp. Quim. 2016, 29, 170–173. [Google Scholar]
- Choi, M.E.; Jung, C.J.; Won, C.H.; Chang, S.E.; Lee, M.W.; Choi, J.H.; Lee, W.J. Case report of cutaneous nodule caused by Gordonia bronchialis in an immunocompetent patient after receiving acupuncture. J. Dermatol. 2019, 46, 343–346. [Google Scholar] [CrossRef]
- Werno, A.M.; Anderson, T.P.; Chambers, S.T.; Laird, H.M.; Murdoch, D.R. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J. Clin. Microbiol. 2005, 43, 3009–3010. [Google Scholar] [CrossRef] [Green Version]
- Vidal, C.; Padilla, E.; Alcacer, P.; Campos, E.; Prieto, F.; Santos, C. Breast abscess caused by Gordonia bronchialis and the use of 16s rRNA gene sequence analysis for its definitive identification. JMM Case Rep. 2014, 1, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Griesinger, L.; Wojewoda, C. Microbiology Case Study: A 42 Year Old Woman with a Lump in Her Left Breast. 2016. Available online: http://labmedicineblog.com/2016 (accessed on 5 July 2019).
- Choi, R.; Strnad, L.; Flaxel, C.J.; Lauer, A.K.; Suhler, E.B. Gordonia bronchialis–Associated Endophthalmitis. Emerg. Infect. Dis. 2019, 25, 1017–1019. [Google Scholar] [CrossRef] [Green Version]
- Brust, J.C.M.; Whittier, S.; Scully, B.E.; McGregor, C.C.; Yin, M.T. Five cases of bacteraemia due to Gordonia species. J. Med. Microbiol. 2009, 58, 1376–1378. [Google Scholar] [CrossRef]
- Ramanan, P.; Deziel, P.J.; Wengenack, N.L. Gordonia bacteremia. J. Clin. Microbiol. 2013, 51, 3443–3447. [Google Scholar] [CrossRef] [Green Version]
- Sng, L.H.; Koh, T.H.; Toney, S.R.; Floyd, M.; Butler, W.R.; Tan, B.H. Bacteremia caused by Gordonia bronchialis in a patient with sequestrated lung. J. Clin. Microbiol. 2004, 42, 2870–2871. [Google Scholar] [CrossRef] [Green Version]
- Lam, J.Y.W.; Wu, A.K.L.; Leung, W.-S.; Cheung, I.; Tsang, C.-C.; Chen, J.H.K.; Chan, J.F.W.; Tse, C.W.S.; Lee, R.A.; Lau, S.K.P.; et al. Gordonia Species as Emerging Causes of Continuous-Ambulatory-Peritoneal-Dialysis-Related Peritonitis Identified by 16S rRNA and secA1 Gene Sequencing and Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry (MALDI-TOF MS). J. Clin. Microbiol. 2015, 53, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukackiene, D.; Rimsevicius, L.; Kiveryte, S.; Marcinkeviciene, K.; Bratchikov, M.; Zokaityte, D.; Tyla, R.; Laucyte-Cibulskiene, A.; Miglinas, M. A case of successfully treated relapsing peritoneal dialysis-associated peritonitis caused by Gordonia bronchialis in a farmer. Nephrol. Ther. 2018, 14, 109–111. [Google Scholar] [CrossRef] [PubMed]
- King-Wing Ma, T.; Chow, K.M.; Ching-Ha Kwan, B.; Lee, K.P.; Leung, C.B.; Kam-Tao Li, P.; Szeto, C.C. Peritoneal-dialysis related peritonitis caused by Gordonia species: Report of four cases and literature review. Nephrology 2014, 19, 379–383. [Google Scholar]
- Titécat, M.; Loïez, C.; Courcol, R.J.; Wallet, F. Difficulty with Gordonia bronchialis identification by Microflex mass spectrometer in a pacemaker-induced endocarditis. JMM Case Rep. 2014, 1, e003681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mormeneo Bayo, S.; Palacián Ruíz, M.P.; Asin Samper, U.; Millán Lou, M.I.; Pascual Catalán, A.; Villuendas Usón, M.C. Pacemaker-induced endocarditis by Gordonia bronchialis. Enferm. Infecc. Microbiol. Clin. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Yamamoto, D.; Yokota, A.; Suzuki, A.; Nagasawa, H.; Sakuda, S. Gordonan, an Acidic Polysaccharide with Cell Aggregation-Inducing Activity in Insect BM-N4 Cells, Produced by Gordonia sp. Biosci. Biotechnol. Biochem. 2000, 64, 2388–2394. [Google Scholar] [CrossRef] [Green Version]
- Richet, H.M.; Craven, P.C.; Brown, J.M.; Lasker, B.A.; Cox, C.D.; McNeil, M.M.; Tice, A.D.; Jarvis, W.R.; Tablan, O.C. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N. Engl. J. Med. 1991, 324, 104–109. [Google Scholar] [CrossRef]
- Wright, S.N.; Gerry, J.S.; Busowski, M.T.; Klochko, A.Y. Gordonia bronchialis sternal wound infection in 3 patients following open heart surgery: Intraoperative transmission from a health worker. Infect. Control Hosp. Epidemiol. 2012, 33, 1238–1241. [Google Scholar] [CrossRef]
- Ambesh, P.; Kapoor, A.; Elsheshtawy, M.; Shetty, V.; Lin, Y.S.; Kamholz, S.; Kazmi, D.H.; Elsheshtawy, M.; Shetty, V.; Lin, Y.S.; et al. Sternal Osteomyelitis by Gordonia Bronchialis in an Immunocompetent Patient after Open Heart Surgery. Ann. Card. Anaesth. 2019, 22, 221–224. [Google Scholar] [CrossRef]
- Chang, J.H.; Misuk, J.; Hyo-Lim, H.; Sang-Ho, C.; Yang-Soo, K.; Cheol-Hyun, C.; Heungsup, S.; Mi-Na, K. Sternal osteomyelitis caused by Gordonia bronchialis after open-heart surgery. Infect. Chemother. 2014, 46, 110–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savini, V.; Fazii, P.; Favaro, M.; Astolfi, D.; Polilli, E.; Pompilio, A.; Vannucci, M.; D’Amario, C.; Di Bonaventura, G.; Fontana, C.; et al. Tuberculosis-like pneumonias by the aerobic actinomycetes Rhodococcus, Tsukamurella and Gordonia. Microbes. Infect. 2012, 14, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Lozano, J.; Pérez-Llantada, E.; Agüero, J.; Rodríguez-Fernández, A.; De Alegria, C.R.; Martinez-Martinez, L.L.; Calvo, J.; Perez-Llantada, E.; Aguero, J.; Rodriguez-Fernadez, A.; et al. Sternal wound infection caused by Gordonia bronchialis: Identification by MALDI-TOF MS. JMM Case Rep. 2016, 3, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaschke, A.J.; Bender, J.; Byington, C.L.; Korgenski, K.; Daly, J.; Petti, C.A.; Pavia, A.T.; Ampofo, K. Gordonia Species: Emerging Pathogens in Pediatric Patients That Are Identified by 16S Ribosomal RNA Gene Sequencing. Clin. Infect. Dis. 2007, 45, 483–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, P.; Brown, J.M.; Nunez, V.H.; Morey, R.E.; Steigerwalt, A.G.; Pellegrini, G.J.; Kessler, H.A. Native valve endocarditis due to Gordonia polyisoprenivorans: Case report and review of literature of bloodstream infections caused by Gordonia species. J. Clin. Microbiol. 2006, 44, 1905–1908. [Google Scholar] [CrossRef] [Green Version]
- Gil-Sande, E.; Brun-Otero, M.; Campo-Cerecedo, F.; Esteban, E.; Aguilar, L.; García-De-Lomas, J. Etiological misidentification by routine biochemical tests of bacteremia caused by Gordonia terrae infection in the course of an episode of acute cholecystitis. J. Clin. Microbiol. 2006, 44, 2645–2647. [Google Scholar] [CrossRef] [Green Version]
- Blanc, V.; Dalle, M.; Markarian, A.; Debunne, M.V.; Duplay, E.; Rodriguez-Nava, V.; Boiron, P. Gordonia terrae: A difficult-to-diagnose emerging pathogen? J. Clin. Microbiol. 2007, 45, 1076–1077. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample 2 | ||||||||
| L.P. | Description | Scientific Name | Max Score | Total Score | Query Cover | E Value | Per. Ident | Accession |
| 1 | Gordonia bronchialis DSM 43247 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 586 | 586 | 100% | 3.0 × 10−167 | 100.00% | NR_074529.1 |
| 2 | Gordonia bronchialis DSM 43247 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 586 | 586 | 100% | 3.0 × 10−167 | 100.00% | NR_027594.1 |
| 3 | Gordonia effusa strain IFM 10200 16S ribosomal RNA, partial sequence | Gordonia effusa | 580 | 580 | 100% | 1.0 × 10−165 | 99.68% | NR_041008.1 |
| 4 | Gordonia bronchialis DSM 43247 strain NCTC 10667 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 575 | 575 | 100% | 6.0 × 10−164 | 99.37% | NR_119065.1 |
| 5 | Gordonia soli strain CC-AB07 16S ribosomal RNA, partial sequence | Gordonia soli | 575 | 575 | 100% | 6.0 × 10−164 | 99.37% | NR_043331.1 |
| 6 | Gordonia rubripertincta strain ATCC 14352 16S ribosomal RNA, partial sequence | Gordonia rubripertincta | 569 | 569 | 100% | 3.0 × 10−162 | 99.05% | NR_119117.1 |
| 7 | Gordonia westfalica strain Kb2 16S ribosomal RNA, partial sequence | Gordonia westfalica | 569 | 569 | 100% | 3.0 × 10−162 | 99.05% | NR_025468.1 |
| 8 | Gordonia rubripertincta strain N4 16S ribosomal RNA, partial sequence | Gordonia rubripertincta | 569 | 569 | 100% | 3.0 × 10−162 | 99.05% | NR_104572.1 |
| 9 | Gordonia namibiensis strain NAM-BN063A 16S ribosomal RNA, partial sequence | Gordonia namibiensis | 569 | 569 | 100% | 3.0 × 10−162 | 99.05% | NR_025165.1 |
| 10 | Gordonia hankookensis strain ON-33 16S ribosomal RNA, partial sequence | Gordonia hankookensis | 569 | 569 | 100% | 3.0 × 10−162 | 99.05% | NR_104507.1 |
| Sample 3 | ||||||||
| L.P. | Description | Scientific Name | Max Score | Total Score | Query Cover | E Value | Per. Ident | Accession |
| 1 | Gordonia bronchialis DSM 43247 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 575 | 575 | 100% | 5.0 × 10−164 | 100.00% | NR_074529.1 |
| 2 | Gordonia bronchialis DSM 43247 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 575 | 575 | 100% | 5.0 × 10−164 | 100.00% | NR_027594.1 |
| 3 | Gordonia effusa strain IFM 10200 16S ribosomal RNA, partial sequence | Gordonia effusa | 569 | 569 | 100% | 3.0 × 10−162 | 99.68% | NR_041008.1 |
| 4 | Gordonia bronchialis DSM 43247 strain NCTC 10667 16S ribosomal RNA, partial sequence | Gordonia bronchialis DSM 43247 | 564 | 564 | 100% | 1.0 × 10−160 | 99.36% | NR_119065.1 |
| 5 | Gordonia soli strain CC-AB07 16S ribosomal RNA, partial sequence | Gordonia soli | 564 | 564 | 100% | 1.0 × 10−160 | 99.36% | NR_043331.1 |
| 6 | Gordonia rubripertincta strain ATCC 14352 16S ribosomal RNA, partial sequence | Gordonia rubripertincta | 558 | 558 | 100% | 6.0 × 10−159 | 99.04% | NR_119117.1 |
| 7 | Gordonia westfalica strain Kb2 16S ribosomal RNA, partial sequence | Gordonia westfalica | 558 | 558 | 100% | 6.0 × 10−159 | 99.04% | NR_025468.1 |
| 8 | Gordonia rubripertincta strain N4 16S ribosomal RNA, partial sequence | Gordonia rubripertincta | 558 | 558 | 100% | 6.0 × 10−159 | 99.04% | NR_104572.1 |
| 9 | Gordonia namibiensis strain NAM-BN063A 16S ribosomal RNA, partial sequence | Gordonia namibiensis | 558 | 558 | 100% | 6.0 × 10−159 | 99.04% | NR_025165.1 |
| 10 | Gordonia hankookensis strain ON-33 16S ribosomal RNA, partial sequence | Gordonia hankookensis | 558 | 558 | 100% | 6.0 × 10−159 | 99.04% | NR_104507.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franczuk, M.; Klatt, M.; Filipczak, D.; Zabost, A.; Parniewski, P.; Kuthan, R.; Jakubowska, L.; Augustynowicz-Kopeć, E. From NTM (Nontuberculous mycobacterium) to Gordonia bronchialis—A Diagnostic Challenge in the COPD Patient. Diagnostics 2022, 12, 307. https://doi.org/10.3390/diagnostics12020307
Franczuk M, Klatt M, Filipczak D, Zabost A, Parniewski P, Kuthan R, Jakubowska L, Augustynowicz-Kopeć E. From NTM (Nontuberculous mycobacterium) to Gordonia bronchialis—A Diagnostic Challenge in the COPD Patient. Diagnostics. 2022; 12(2):307. https://doi.org/10.3390/diagnostics12020307
Chicago/Turabian StyleFranczuk, Monika, Magdalena Klatt, Dorota Filipczak, Anna Zabost, Paweł Parniewski, Robert Kuthan, Lilia Jakubowska, and Ewa Augustynowicz-Kopeć. 2022. "From NTM (Nontuberculous mycobacterium) to Gordonia bronchialis—A Diagnostic Challenge in the COPD Patient" Diagnostics 12, no. 2: 307. https://doi.org/10.3390/diagnostics12020307