
Correlation between CT Value on Lung Subtraction CT and Radioactive Count on Perfusion Lung Single Photon Emission CT in Chronic Thromboembolic Pulmonary Hypertension

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
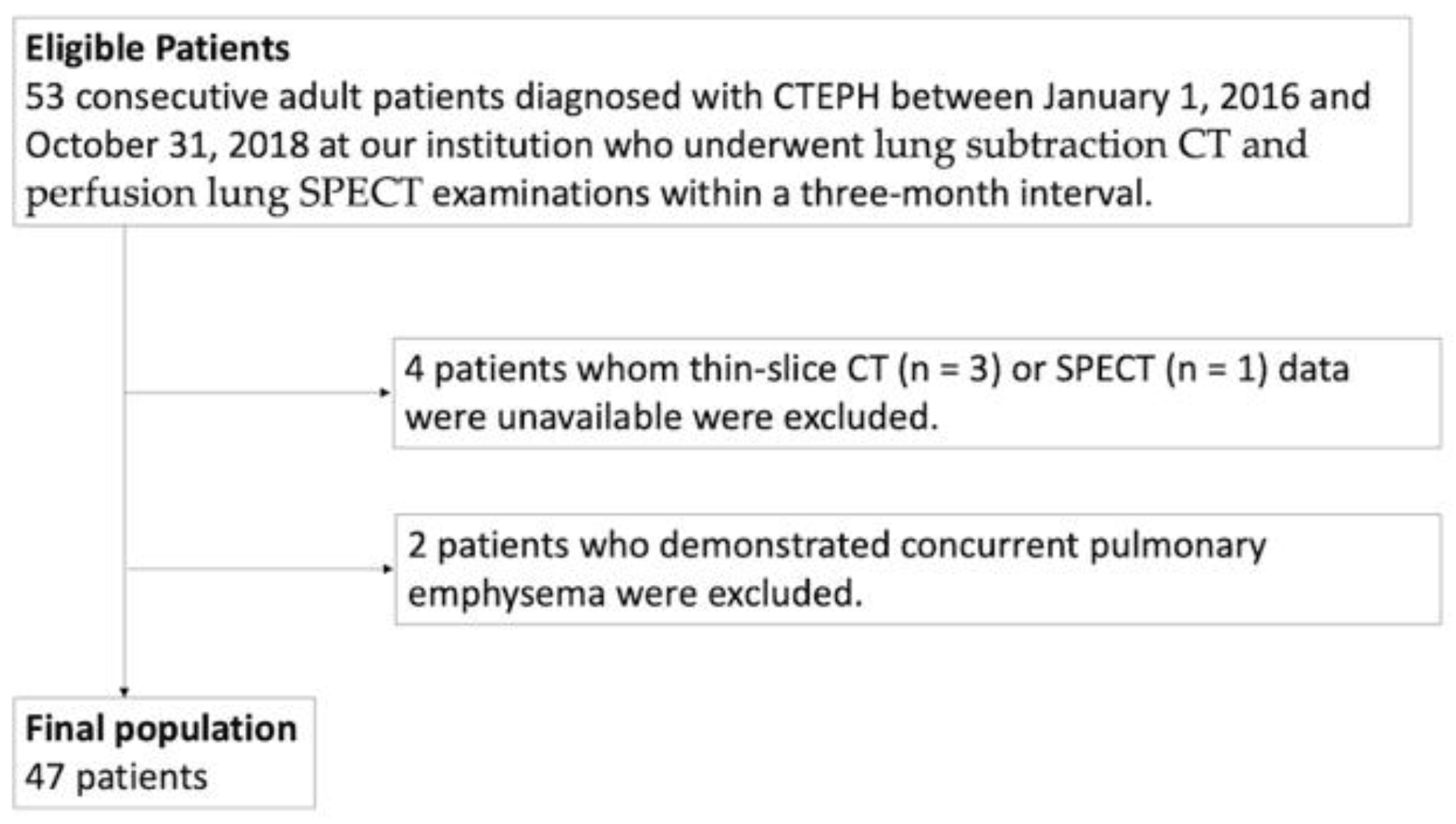
2.1. Subjects
2.2. Image Acquisition Protocol
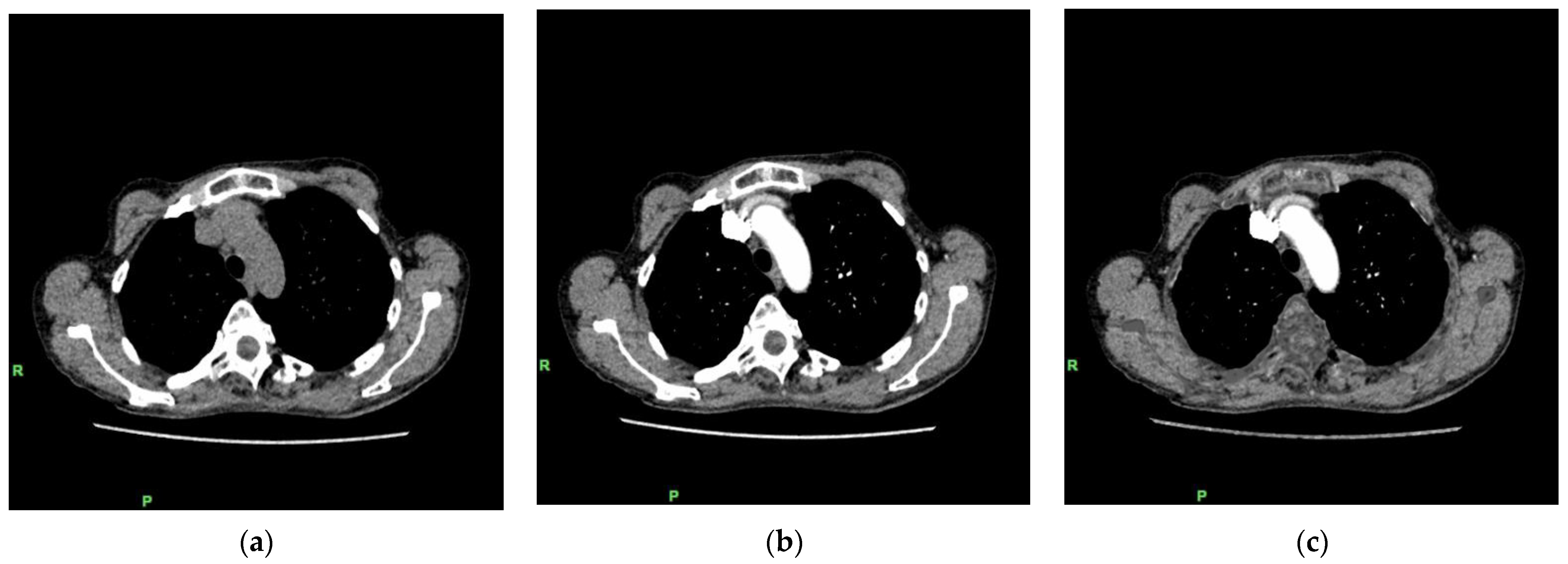
2.2.1. Lung Subtraction CT
2.2.2. Perfusion Lung SPECT
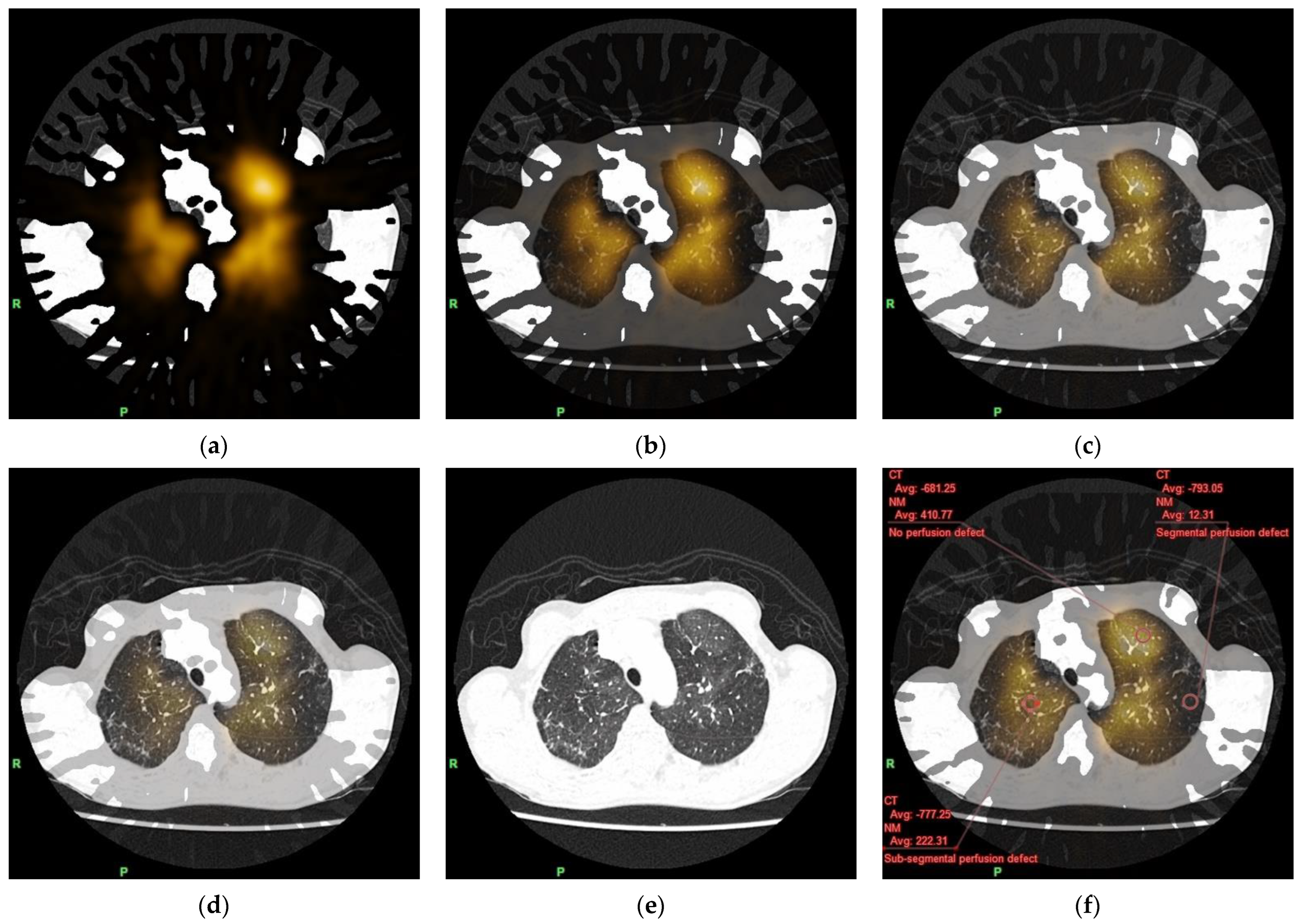
2.3. Fusion of Lung Subtraction CT and Perfusion Lung SPECT Images
2.4. Image Evaluation
2.5. Statistical Analysis
3. Results
3.1. Radiation Exposure
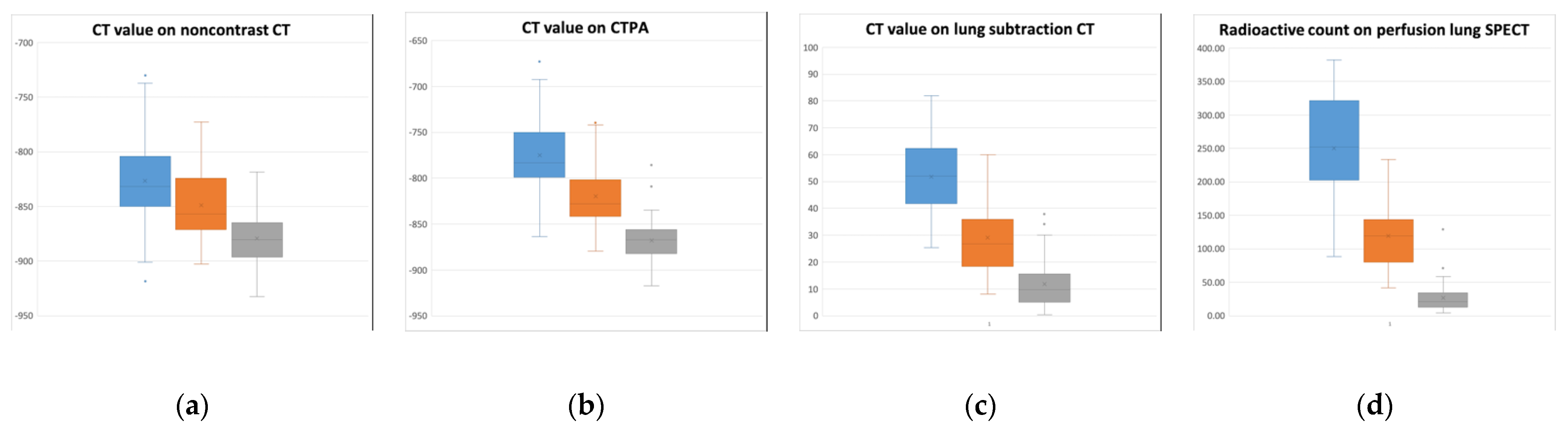
3.2. Comparison of CT Value and Radioactive Count among the Three Different Classes of Lung Perfusion
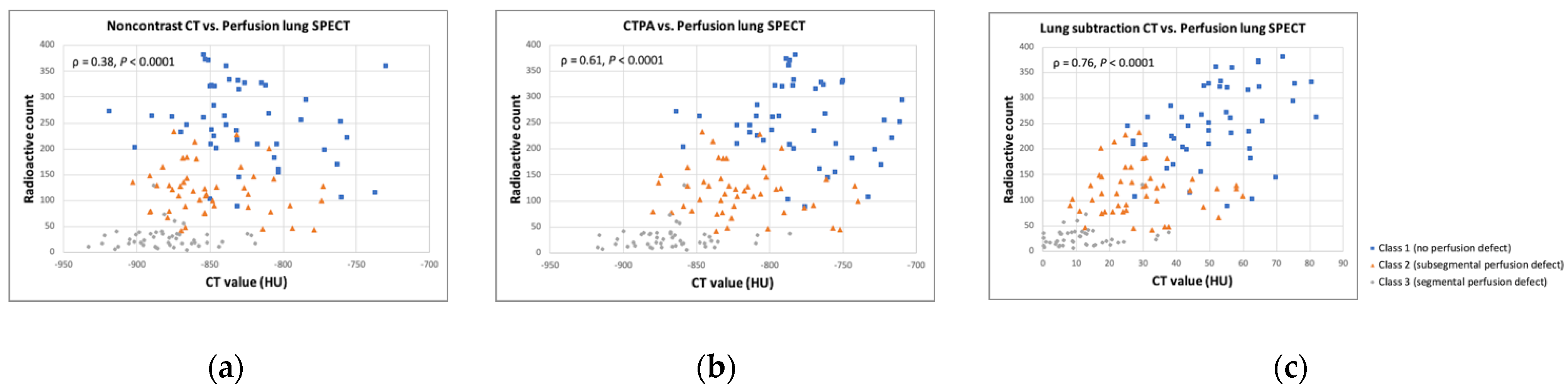
3.3. Correlations between CT Value and Radioactive Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fedullo, P.F.; Auger, W.R.; Kerr, K.M.; Rubin, L.J. Chronic thromboembolic pulmonary hypertension. N. Engl. J. Med. 2001, 345, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Goldhaber, S.Z. Chronic thromboembolic pulmonary hypertension. N. Engl. J. Med. 2011, 364, 351–360. [Google Scholar] [CrossRef] [Green Version]
- Vrigkou, E.; Tsantes, A.; Konstantonis, D.; Rapti, E.; Maratou, E.; Pappas, A.; Halvatsiotis, P.; Tsangaris, I. Platelet, Fibrinolytic and Other Coagulation Abnormalities in Newly-Diagnosed Patients with Chronic Thromboembolic Pulmonary Hypertension. Diagnostics 2022, 12, 1238. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Baratella, E.; Caforio, G.; Confalonieri, P.; Wade, B.; Marrocchio, C.; Geri, P.; Pozzan, R.; Andrisano, A.G.; Cova, M.A.; et al. Chronic Thromboembolic Pulmonary Hypertension: An Update. Diagnostics 2022, 12, 235. [Google Scholar] [CrossRef] [PubMed]
- Nazzareno, G.; Marc, H.; Jean, L.V.; Simon, G.; Irene, L.; Adam, T. ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur. Heart J. 2016, 37, 67–119. [Google Scholar]
- Tunariu, N.; Gibbs, S.J.; Win, Z.; Gin-Sing, W.; Graham, A.; Gishen, P.; Al-Nahhas, A. Ventilation-Perfusion Scintigraphy Is More Sensitive than Multidetector CTPA in Detecting Chronic Thromboembolic Pulmonary Disease as a Treatable Cause of Pulmonary Hypertension. J. Nucl. Med. 2007, 48, 680–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutte, H.; Mortensen, J.; Jensen, C.V.; von der Recke, P.; Petersen, C.L.; Kristoffersen, U.S.; Kjaer, A. Comparison of V/Q SPECT and planar V/Q lung scintigraphy in diagnosing acute pulmonary embolism. Nucl. Med. Commun. 2010, 31, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, M.; Chan, K.; McMeekin, H.; Navalkissoor, S.; Wagner, T. Incidence of a single subsegmental mismatched perfusion defect in single-photon emission computed tomography and planar ventilation/perfusion scans. Nucl. Med. Commun. 2017, 38, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, M.; Yang, T.; Wu, D.; Xiong, C.; Fang, W. A prospective, comparative study of planar and single-photon emission computed tomography ventilation/perfusion imaging for chronic thromboembolic pulmonary hypertension. J. Nucl. Med. 2020, 61, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Sherrick, A.D.; Swensen, S.J.; Hartman, T.E. Mosaic pattern of lung attenuation on CT scans: Frequency among patients with pulmonary artery hypertension of different causes. Am. J. Roentgenol. 1997, 169, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasai, H.; Tanabe, N.; Fujimoto, K.; Hoshi, H.; Naito, J.; Suzuki, R.; Matsumura, A.; Sugiura, T.; Sakao, S.; Tatsumi, K. Mosaic attenuation pattern in non-contrast computed tomography for the assessment of pulmonary perfusion in chronic thromboembolic pulmonary hypertension. Respir. Investig. 2017, 55, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Hoey, E.T.D.; Agrawal, S.K.B.; Ganesh, V.; Gopalan, D.; Screaton, N.J. Dual energy CT pulmonary angiography: Findings in a patient with chronic thromboembolic pulmonary hypertension. Thorax 2009, 64, 1012. [Google Scholar] [CrossRef] [Green Version]
- Nakazawa, T.; Watanabe, Y.; Hori, Y.; Kiso, K.; Higashi, M.; Itoh, T.; Naito, H. Lung perfused blood volume images with dual-energy computed tomography for chronic thromboembolic pulmonary hypertension: Correlation to scintigraphy with single-photon emission computed to-mography. J. Comput. Assist. Tomogr. 2011, 35, 590–595. [Google Scholar] [CrossRef]
- Hoey, E.T.D.; Mirsadraee, S.; Pepke-Zaba, J.; Jenkins, D.P.; Gopalan, D.; Screaton, N.J. Dual-Energy CT Angiography for Assessment of Regional Pulmonary Perfusion in Patients With Chronic Thromboembolic Pulmonary Hypertension: Initial Experience. Am. J. Roentgenol. 2011, 196, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Ameli-Renani, S.; Ramsay, L.; Bacon, J.L.; Rahman, F.; Nair, A.; Smith, V.; Baskerville, K.; Devaraj, A.; Madden, B.; Vlahos, I. Dual-energy Computed Tomography in the Assessment of Vascular and Parenchymal Enhancement in Suspected Pulmonary Hypertension. J. Thorac. Imaging 2014, 29, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Dournes, G.; Verdier, D.; Montaudon, M.; Bullier, E.; Rivière, A.; Dromer, C. Dual-energy CT perfusion and angiography in chronic thromboembolic pul-monary hypertension: Diagnostic accuracy and concordance with radionuclide scintigraphy. Eur. Radiol. 2014, 24, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Meinel, F.G.; Graef, A.; Thierfelder, K.M.; Armbruster, M.; Schild, C.; Neurohr, C.; Reiser, M.F.; Johnson, T.R.C. Automated Quantification of Pulmonary Perfused Blood Volume by Dual-Energy CTPA in Chronic Thromboembolic Pulmonary Hypertension. Rofo 2013, 186, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koike, H.; Sueyoshi, E.; Sakamoto, I.; Uetani, M.; Nakata, T.; Maemura, K. Quantification of lung perfusion blood volume (lung PBV) by dual-energy CT in patients with chronic thromboembolic pulmonary hypertension (CTEPH) before and after balloon pulmonary angioplasty (BPA): Preliminary results. Eur. J. Radiol. 2016, 85, 1607–1612. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Ota, H.; Sugimura, K.; Otani, K.; Tominaga, J.; Aoki, T.; Tatebe, S.; Miura, M.; Yamamoto, S.; Sato, H.; et al. Dual-energy CT to estimate clinical severity of chronic thromboembolic pulmonary hypertension: Comparison with invasive right heart catheterization. Eur. J. Radiol. 2016, 85, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Koike, H.; Sueyoshi, E.; Sakamoto, I.; Uetani, M.; Nakata, T.; Maemura, K. Comparative clinical and predictive value of lung perfusion blood volume CT, lung perfusion SPECT and catheter pulmonary angiography images in patients with chronic thromboembolic pulmonary hypertension before and after balloon pulmonary angioplasty. Eur. Radiol. 2018, 28, 5091–5099. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.; Moreau-Triby, C.; Tylski, P.; Tatard-Leitman, V.; Wdowik, Q.; Boccalini, S.; Dessouky, R.; Douek, P.; Boussel, L. Head-to-head comparison of lung perfusion with dual-energy CT and SPECT-CT. Diagn. Interv. Imaging 2020, 101, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, Y.; Iwano, S.; Okumura, N.; Adachi, S.; Abe, S.; Kondo, T.; Kato, K.; Naganawa, S. Assessment of Severity in Chronic Thromboembolic Pulmonary Hypertension by Quantitative Parameters of Dual-Energy Computed Tomography. J. Comput. Assist. Tomogr. 2020, 44, 578–585. [Google Scholar] [CrossRef]
- Tamura, M.; Yamada, Y.; Kawakami, T.; Kataoka, M.; Iwabuchi, Y.; Sugiura, H.; Hashimoto, M.; Nakahara, T.; Okuda, S.; Nakatsuka, S.; et al. Diagnostic accuracy of lung subtraction iodine mapping CT for the evaluation of pulmonary perfusion in patients with chronic thromboembolic pulmonary hypertension: Correlation with perfusion SPECT/CT. Int. J. Cardiol. 2017, 243, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Grob, D.; Smit, E.; Prince, J.; Kist, J.; Stöger, L.; Geurts, B.; Snoeren, M.M.; van Dijk, R.; Oostveen, L.J.; Prokop, M.; et al. Iodine Maps from Subtraction CT or Dual-Energy CT to Detect Pulmonary Emboli with CT Angiography: A Multiple-Observer Study. Radiology 2019, 292, 197–205. [Google Scholar] [CrossRef]
- Grob, D.; Smit, E.; Oostveen, L.J.; Snoeren, M.M.; Prokop, M.; Schaefer-Prokop, C.M.; Sechopoulos, I.; Brink, M. Image Quality of Iodine Maps for Pulmonary Embolism: A Comparison of Subtraction CT and Dual-Energy CT. Am. J. Roentgenol. 2019, 212, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.; Jenkins, D.; Lindner, J.; D’Armini, A.; Kloek, J.; Meyns, B.; Ilkjaer, L.B.; Klepetko, W.; Delcroix, M.; Lang, I.; et al. Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: Results from an international prospective registry. J. Thorac. Cardiovasc. Surg. 2011, 141, 702–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kataoka, M.; Inami, T.; Hayashida, K.; Shimura, N.; Ishiguro, H.; Abe, T.; Tamura, Y.; Ando, M.; Fukuda, K.; Yoshino, H.; et al. Percutaneous Transluminal Pulmonary Angioplasty for the Treatment of Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2012, 5, 756–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreassen, A.K.; Ragnarsson, A.; Gude, E.; Geiran, O.; Andersen, R. Balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension. Heart 2013, 99, 1415–1420. [Google Scholar] [CrossRef]
- Wilkens, H.; Konstantinides, S.; Lang, I.M.; Bunck, A.C.; Gerges, M.; Gerhardt, F. Chronic thromboembolic pulmonary hypertension (CTEPH): Updated recom-mendations from the Cologne Consensus Conference 2018. Int. J. Cardiol. 2018, 272S, 69–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inami, T.; Kataoka, M.; Shimura, N.; Ishiguro, H.; Yanagisawa, R.; Taguchi, H.; Fukuda, K.; Yoshino, H.; Satoh, T. Pulmonary Edema Predictive Scoring Index (PEPSI), a New Index to Predict Risk of Reperfusion Pulmonary Edema and Improvement of Hemodynamics in Percutaneous Transluminal Pulmonary Angioplasty. JACC Cardiovasc. Interv. 2013, 6, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, T.; Ogawa, A.; Miyaji, K.; Mizoguchi, H.; Shimokawahara, H.; Naito, T.; Oka, T.; Yunoki, K.; Munemasa, M.; Matsubara, H. Novel Angiographic Classification of Each Vascular Lesion in Chronic Thromboembolic Pulmonary Hypertension Based on Selective Angiogram and Results of Balloon Pulmonary Angioplasty. Circ. Cardiovasc. Interv. 2016, 9, e003318. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, J.B.; Werncke, T.; Kaireit, T.; Hoeper, M.; Olsson, K.; Kamp, J.-C.; Wacker, F.; Bengel, F.; von Falck, C.; Schatka, I.; et al. C-Arm Computed Tomography Adds Diagnostic Information in Patients with Chronic Thromboembolic Pulmonary Hypertension and a Positive V/Q SPECT. Rofo 2017, 189, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alis, J.; Latson Jr, L.A.; Haramati, L.B.; Shmukler, A. Navigating the pulmonary perfusion map: Dual-energy computed tomography in acute pulmonary embolism. J. Comput. Assist. Tomogr. 2018, 42, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Thieme, S.; Graute, V.; Nikolaou, K.; Maxien, D.; Reiser, M.; Hacker, M.; Johnson, T. Dual Energy CT lung perfusion imaging—Correlation with SPECT/CT. Eur. J. Radiol. 2012, 81, 360–365. [Google Scholar] [CrossRef]
- Riedel, M.; Stanek, V.; Widimsky, J.; Prerovsky, I. Longterm Follow-up of Patients with Pulmonary Thromboembolism. Chest 1982, 81, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, S.W.; Kapelanski, D.P.; Sakakibara, N.; Manecke, G.R.; Thistlethwaite, P.A.; Kerr, K.M.; Channick, R.N.; Fedullo, P.F.; Auger, W.R. Pulmonary endarterectomy: Experience and lessons learned in 1500 cases. Ann. Thorac. Surg. 2003, 76, 1457–1464. [Google Scholar] [CrossRef]
- Heinrich, M.; Uder, M.; Tscholl, D.; Grgic, A.; Kramann, B.; Schäfers, H.C.T. Scan findings in chronic thromboembolic pulmonary hypertension: Predictors of hemodynamic improvement after pulmonary thromboendarterectomy. Chest 2005, 127, 1606–1613. [Google Scholar] [CrossRef]
- Haramati, A.; Haramati, L.B. Imaging of Chronic Thromboembolic Disease. Lung 2020, 198, 245–255. [Google Scholar] [CrossRef]
- Derlin, T.; Kelting, C.; Hueper, K.; Weiberg, D.; Meyer, K.; Olsson, K.M. Quantitation of perfused lung volume using hybrid SPECT/CT allows refining the as-sessment of lung perfusion and estimating disease extent in chronic thromboembolic pulmonary hypertension. Clin. Nucl. Med. 2018, 43, e170–e177. [Google Scholar] [CrossRef] [PubMed]
- Faby, S.; Kuchenbecker, S.; Sawall, S.; Simons, D.; Schlemmer, H.P.; Lell, M.; Kachelrieß, M. Performance of today′s dual energy CT and future multi energy CT in virtual non-contrast imaging and in iodine quantification: A simulation study. Med. Phys. 2015, 42, 4349–4366. [Google Scholar] [CrossRef] [PubMed]
- Baerends, E.; Oostveen, L.J.; Smit, C.T.; Das, M.; Sechopoulos, I.; Brink, M. Comparing dual energy CT and subtraction CT on a phantom: Which one provides the best contrast in iodine maps for sub-centimetre details? Eur. Radiol. 2018, 28, 5051–5059. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 47 |
|---|---|
| Sex | Men, 9 (19.1%); women, 38 (80.9%) |
| Age (range) | 62 ± 14 years (38–83 years) |
| BMI (range) | 23.6 ± 3.9 kg/m2 (15.8–33.2 kg/m2) |
| WHO-FC | I (n = 2), II (n = 41), III (n = 4), IV (n = 0) |
| Mean PA pressure (range) | 25.4 ± 16.8 mmHg (10–113 mmHg) |
| Prior therapy | Medication only (n = 6) Medication with PEA (n = 1) Medication with BPA (n = 40) |
| Noncontrast CT | CTPA | Lung Subtraction CT | Perfusion Lung SPECT | |
|---|---|---|---|---|
| Class 1 | −826.6 ± 40.6 | −774.8 ± 40.1 | 51.9 ± 14.5 | 250.1 ± 76.3 |
| Class 2 | −848.9 ± 33.1 | −819.8 ± 34.6 | 29.1 ± 13.1 | 119.1 ± 47.9 |
| Class 3 | −879.3 ± 25.8 | −867.6 ± 27.3 | 11.7 ± 9.3 | 26.5 ± 20.9 |
| ρ Value | p Value | |
|---|---|---|
| Noncontrast CT vs. Perfusion lung SPECT | 0.38 | <0.0001 |
| CTPA vs. Perfusion lung SPECT | 0.61 | <0.0001 |
| Lung subtraction CT vs. Perfusion lung SPECT | 0.76 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kariyasu, T.; Machida, H.; Yamashiro, T.; Fukushima, K.; Koyanagi, M.; Yokoyama, K.; Nishikawa, M.; Satoh, T. Correlation between CT Value on Lung Subtraction CT and Radioactive Count on Perfusion Lung Single Photon Emission CT in Chronic Thromboembolic Pulmonary Hypertension. Diagnostics 2022, 12, 2895. https://doi.org/10.3390/diagnostics12112895
Kariyasu T, Machida H, Yamashiro T, Fukushima K, Koyanagi M, Yokoyama K, Nishikawa M, Satoh T. Correlation between CT Value on Lung Subtraction CT and Radioactive Count on Perfusion Lung Single Photon Emission CT in Chronic Thromboembolic Pulmonary Hypertension. Diagnostics. 2022; 12(11):2895. https://doi.org/10.3390/diagnostics12112895
Chicago/Turabian StyleKariyasu, Toshiya, Haruhiko Machida, Tsuneo Yamashiro, Keita Fukushima, Masamichi Koyanagi, Kenichi Yokoyama, Makiko Nishikawa, and Toru Satoh. 2022. "Correlation between CT Value on Lung Subtraction CT and Radioactive Count on Perfusion Lung Single Photon Emission CT in Chronic Thromboembolic Pulmonary Hypertension" Diagnostics 12, no. 11: 2895. https://doi.org/10.3390/diagnostics12112895