
From Death Triad to Death Tetrad—The Addition of a Hypotension Component to the Death Triad Improves Mortality Risk Stratification in Trauma Patients: A Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
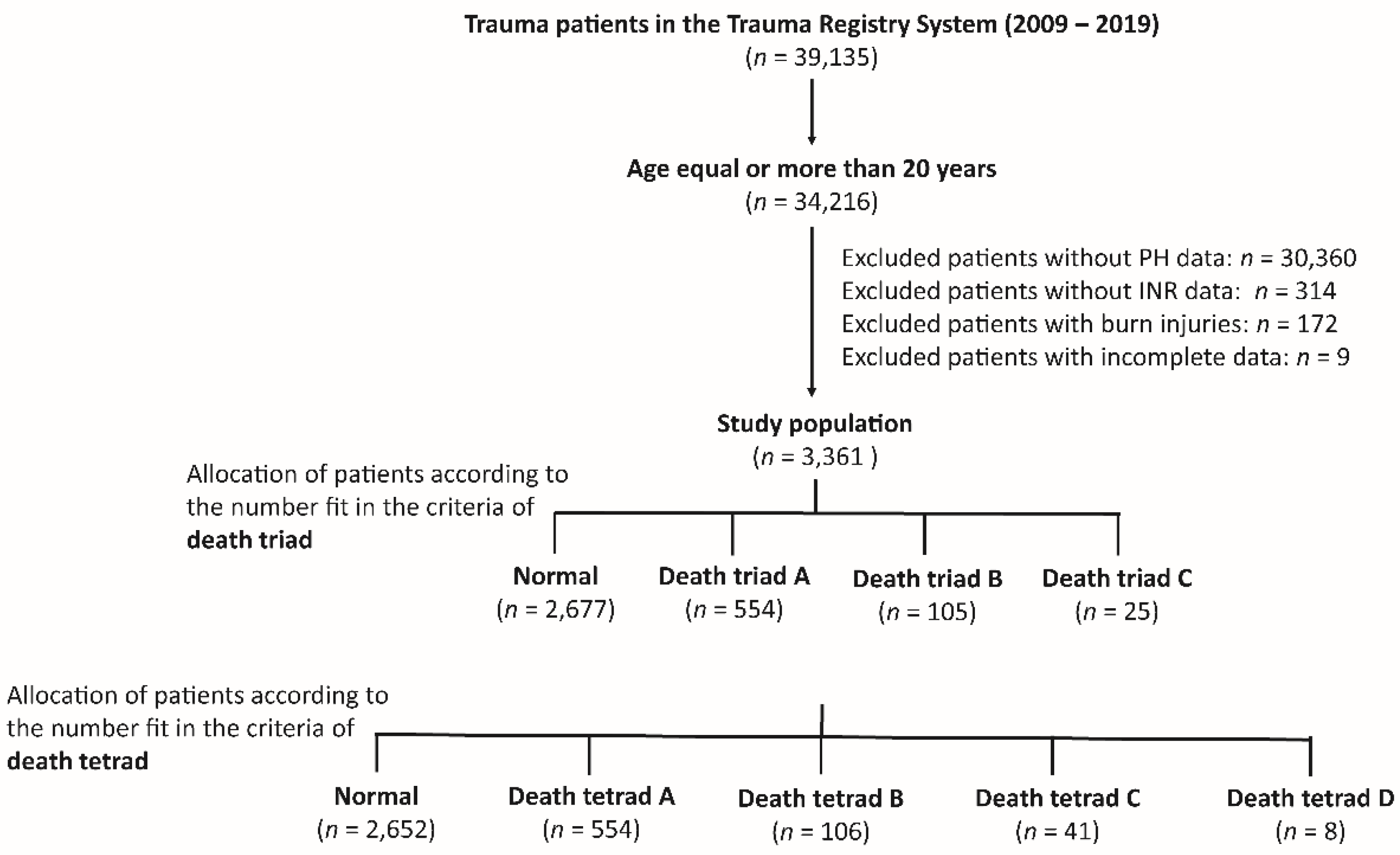
2.1. Study Population and Grouping
2.2. Study Parameter
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Outcomes of Trauma Accident Divided According to Death Triad
3.2. Outcomes of Trauma Patients with or without Hypotension and Those with One to Three Components of the Death Triad
3.3. Clinical Characteristics and Outcomes of Trauma Accidents with Different Death Tetrad Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitra, B.; Tullio, F.; Cameron, P.A.; Fitzgerald, M. Trauma patients with the ‘triad of death’. Emerg. Med. J. 2012, 29, 622–625. [Google Scholar] [CrossRef]
- Keane, M. Triad of death: The importance of temperature monitoring in trauma patients. Emerg. Nurse 2016, 24, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Mikhail, J. The trauma triad of death: Hypothermia, acidosis, and coagulopathy. AACN Clin. Issues 1999, 10, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Muthukumar, V.; Karki, D.; Jatin, B. Concept of Lethal Triad in Critical Care of Severe Burn Injury. Indian J. Crit. Care Med. 2019, 23, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Hendrix, V.; Shapiro, M.; Duchesne, J.; Taghavi, S.; Schroll, R.; Tatum, D.; Guidry, C. Is the “Death Triad” a Casualty of Modern Damage Control Resuscitation. J. Surg. Res. 2021, 259, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Bozorgi, F.; Khatir, I.G.; Ghanbari, H.; Jahanian, F.; Arabi, M.; Ahidashti, H.A.; Hosseininejad, S.M.; Ramezani, M.S.; Montazer, S.H. Investigation of Frequency of the Lethal Triad and Its 24 Hours Prognostic Value among Patients with Multiple Traumas. Open Access Maced. J. Med. Sci. 2019, 7, 962–966. [Google Scholar] [CrossRef] [Green Version]
- Feliciano, D.V. Abdominal vascular injuries. Surg. Clin. N. Am. 1988, 68, 741–755. [Google Scholar] [CrossRef]
- Samuels, J.M.; Moore, H.B.; Moore, E.E. Damage Control Resuscitation. Chirurgia 2017, 112, 514–523. [Google Scholar] [CrossRef]
- Corwin, G.S.; Sexton, K.W.; Beck, W.C.; Taylor, J.R.; Bhavaraju, A.; Davis, B.; Kimbrough, M.K.; Jensen, J.C.; Privratsky, A.; Robertson, R.D. Characterization of Acidosis in Trauma Patient. J. Emerg. Trauma Shock 2020, 13, 213–218. [Google Scholar] [CrossRef]
- Brohi, K.; Singh, J.; Heron, M.; Coats, T. Acute traumatic coagulopathy. J. Trauma 2003, 54, 1127–1130. [Google Scholar] [CrossRef]
- Jurkovich, G.J.; Greiser, W.B.; Luterman, A.; Curreri, P.W. Hypothermia in trauma victims: An ominous predictor of survival. J. Trauma 1987, 27, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Valeri, C.R.; Feingold, H.; Cassidy, G.; Ragno, G.; Khuri, S.; Altschule, M.D. Hypothermia-induced reversible platelet dysfunction. Ann. Surg. 1987, 205, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Martini, W.Z. Coagulopathy by hypothermia and acidosis: Mechanisms of thrombin generation and fibrinogen availability. J. Trauma 2009, 67, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, W.H.; Rau, C.S.; Hsu, S.Y.; Wu, S.C.; Kuo, P.J.; Hsieh, H.Y.; Chen, Y.C.; Hsieh, C.H. Using the Reverse Shock Index at the Injury Scene and in the Emergency Department to Identify High-Risk Patients: A Cross-Sectional Retrospective Study. Int. J. Environ. Res. Public Health 2016, 13, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, S.C.; Kuo, P.J.; Hsu, S.Y.; Rau, C.S.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. The use of the reverse shock index to identify high-risk trauma patients in addition to the criteria for trauma team activation: A cross-sectional study based on a trauma registry system. BMJ Open 2016, 6, e011072. [Google Scholar] [CrossRef] [Green Version]
- Chuang, J.F.; Rau, C.S.; Wu, S.C.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C.; Hsieh, C.H. Use of the reverse shock index for identifying high-risk patients in a five-level triage system. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, W.H.; Wu, S.C.; Rau, C.S.; Kuo, P.J.; Hsu, S.Y.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. Systolic Blood Pressure Lower than Heart Rate upon Arrival at and Departure from the Emergency Department Indicates a Poor Outcome for Adult Trauma Patients. Int. J. Environ. Res. Public Health 2016, 13, 528. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.C.; Rau, C.S.; Kuo, S.C.H.; Chien, P.C.; Hsieh, H.Y.; Hsieh, C.H. The Reverse Shock Index Multiplied by Glasgow Coma Scale Score (rSIG) and Prediction of Mortality Outcome in Adult Trauma Patients: A Cross-Sectional Analysis Based on Registered Trauma Data. Int. J. Environ. Res. Public Health 2018, 15, 2346. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Chien, P.C. Defining polytrauma by abbreviated injury scale ≥ 3 for a least two body regions is insufficient in terms of short-term outcome: A cross-sectional study at a level I trauma center. Biomed. J. 2018, 41, 321–327. [Google Scholar] [CrossRef]
- Wu, S.C.; Chou, S.E.; Liu, H.T.; Hsieh, T.M.; Su, W.T.; Chien, P.C.; Hsieh, C.H. Performance of Prognostic Scoring Systems in Trauma Patients in the Intensive Care Unit of a Trauma Center. Int. J. Environ. Res. Public Health 2020, 17, 7226. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.H.; Wu, S.C.; Chou, S.E.; Su, W.T.; Tsai, C.H.; Li, C.; Hsu, S.Y.; Hsieh, C.H. Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma. Int. J. Environ. Res. Public Health 2020, 17, 9233. [Google Scholar] [CrossRef] [PubMed]
- Wray, J.P.; Bridwell, R.E.; Schauer, S.G.; Shackelford, S.A.; Bebarta, V.S.; Wright, F.L.; Bynum, J.; Long, B. The diamond of death: Hypocalcemia in trauma and resuscitation. Am. J. Emerg. Med. 2021, 41, 104–109. [Google Scholar] [CrossRef]
- Ditzel, R.M., Jr.; Anderson, J.L.; Eisenhart, W.J.; Rankin, C.J.; DeFeo, D.R.; Oak, S.; Siegler, J. A review of transfusion- and trauma-induced hypocalcemia: Is it time to change the lethal triad to the lethal diamond? J. Trauma Acute Care Surg. 2020, 88, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Sewalt, C.A.; Venema, E.; Wiegers, E.J.A.; Lecky, F.E.; Schuit, S.C.E.; den Hartog, D.; Steyerberg, E.W.; Lingsma, H.F. Trauma models to identify major trauma and mortality in the prehospital setting. Br. J. Surg. 2020, 107, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Orhon, R.; Eren, S.H.; Karadayi, S.; Korkmaz, I.; Coskun, A.; Eren, M.; Katrancioglu, N. Comparison of trauma scores for predicting mortality and morbidity on trauma patients. Ulus. Travma Acil Cerrahi Derg. 2014, 20, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolstridge, J.; O’Neil, E.R.; Aden, J.K.; Muisyo, T.; Spinella, P.C.; Borgman, M.A. Use of the BIG score to predict mortality in pediatric trauma. Am. J. Emerg. Med. 2021, 45, 472–475. [Google Scholar] [CrossRef]
- Paladino, L.; Sinert, R.; Wallace, D.; Anderson, T.; Yadav, K.; Zehtabchi, S. The utility of base deficit and arterial lactate in differentiating major from minor injury in trauma patients with normal vital signs. Resuscitation 2008, 77, 363–368. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Grouping by Number of Components of Death Triad | ||||
|---|---|---|---|---|---|
| Death Triad A n = 554 | Death Triad B n = 105 | Death Triad C n = 25 | Normal n = 2677 | p | |
| Gender | <0.001 | ||||
| Male, n (%) | 385 (69.5) | 90 (85.7) | 20 (80.0) | 1698 (63.4) | |
| Female, n (%) | 169 (30.5) | 15 (14.3) | 5 (20.0) | 979 (36.6) | |
| Age, years (SD) | 53.8 ± 20.3 | 52.7 ± 18.8 | 47.2 ± 18.4 | 57.6 ± 19.9 | <0.001 |
| Comorbidities | |||||
| CVA, n (%) | 14 (2.5) | 1 (1.0) | 0 (0.0) | 156 (5.8) | 0.001 |
| HTN, n (%) | 159 (28.7) | 24 (22.9) | 5 (20.0) | 967 (36.1) | <0.001 |
| CAD, n (%) | 41 (7.4) | 4 (3.8) | 0 (0.0) | 173 (6.5) | 0.291 |
| CHF, n (%) | 8 (1.4) | 0 (0.0) | 1 (4.0) | 21 (0.8) | 0.115 |
| DM, n (%) | 84 (15.2) | 10 (9.5) | 1 (4.0) | 543 (20.3) | <0.001 |
| ESRD, n (%) | 18 (3.2) | 1 (1.0) | 1 (4.0) | 108 (4.0) | 0.364 |
| GCS, median (IQR) | 9 (4–15) | 4 (3–8) | 3 (3–7) | 15 (8–15) | <0.001 |
| Head AIS ≥ 3, n (%) | 345 (62.3) | 70 (66.7) | 16 (64.0) | 1497 (55.9) | 0.008 |
| Thorax AIS ≥ 3, n (%) | 153 (27.6) | 43 (41.0) | 12 (48.0) | 519 (19.4) | <0.001 |
| Abdomen AIS ≥ 3, n (%) | 75 (13.5) | 22 (21.0) | 8 (32.0) | 154 (5.8) | <0.001 |
| Extremities AIS ≥ 3, n (%) | 132 (23.8) | 28 (26.7) | 4 (16.0) | 652 (24.4) | 0.723 |
| External AIS ≥ 3, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.0) | 0.968 |
| Polytrauma, n (%) | 161 (29.1) | 51 (48.6) | 13 (52.0) | 418 (15.6) | <0.001 |
| ISS, median (IQR) | 22 (16–29) | 25 (21–34) | 25 (17–38) | 16 (9–24) | <0.001 |
| 1–15, n (%) | 131 (23.6) | 9 (8.6) | 5 (20.0) | 1066 (39.8) | <0.001 |
| 16–24, n (%) | 165 (29.8) | 28 (26.7) | 4 (16.0) | 956 (35.7) | 0.003 |
| ≥25, n (%) | 258 (46.6) | 68 (64.8) | 16 (64.0) | 655 (24.5) | <0.001 |
| Mortality, n (%) | 161 (29.1) | 60 (57.1) | 21 (84.0) | 283 (10.6) | <0.001 |
| Hospital LOS, days (SD) | 18.6 ± 16.9 | 17.7 ± 20.2 | 13.5 ± 18.8 | 16.7 ± 15.7 | 0.060 |
| Admitted into ICU, n (%) | 469 (84.7) | 99 (94.3) | 19 (76.0) | 1793 (67.0) | <0.001 |
| Variables | Death Triad A | |||
|---|---|---|---|---|
| SBP < 60 mmHg n = 25 | SBP ≥ 60 mmHg n = 529 | OR (95% CI) | p | |
| Gender | 0.243 | |||
| Male, n (%) | 20 (80.0) | 365 (69.0) | 1.80 (0.66–4.87) | |
| Female, n (%) | 5 (20.0) | 164 (31.0) | 0.56 (0.21–1.51) | |
| Age, years (SD) | 52.7 ± 17.8 | 53.8 ± 20.4 | - | 0.787 |
| Comorbidities | ||||
| CVA, n (%) | 1 (4.0) | 13 (2.5) | 1.65 (0.21–13.17) | 0.631 |
| HTN, n (%) | 7 (28.0) | 152 (28.7) | 0.97 (0.40–2.36) | 0.937 |
| CAD, n (%) | 1 (4.0) | 40 (7.6) | 0.51 (0.07–3.86) | 0.506 |
| CHF, n (%) | 0 (0.0) | 8 (1.5) | - | 0.536 |
| DM, n (%) | 3 (12.0) | 81 (15.3) | 0.75 (0.22–2.58) | 0.652 |
| ESRD, n (%) | 1 (4.0) | 17 (3.2) | 1.26 (0.16–9.83) | 0.828 |
| GCS, median (IQR) | 3 (3–6) | 9 (4–15) | - | <0.001 |
| ISS, median (IQR) | 25 (17–28) | 22 (16–29) | - | 0.245 |
| 1–15, n (%) | 4 (16.0) | 127 (24.0) | 0.60 (0.20–1.79) | 0.357 |
| 16–24, n (%) | 7 (28.0) | 158 (29.9) | 0.91 (0.37–2.23) | 0.842 |
| ≥25, n (%) | 14 (56.0) | 244 (46.1) | 1.49 (0.66–3.34) | 0.333 |
| Mortality, n (%) | 12 (48.0) | 149 (28.2) | 2.35 (1.05–5.28) | 0.033 |
| Hospital LOS, days (SD) | 18.0 ± 18.0 | 18.6 ± 16.8 | - | 0.873 |
| Admitted into ICU, n (%) | 20 (80.0) | 449 (84.9) | 0.71 (0.26–1.95) | 0.508 |
| Variables | Death Triad B | |||
|---|---|---|---|---|
| SBP < 60 mmHg n = 24 | SBP ≥ 60 mmHg n = 81 | OR (95% CI) | p | |
| Gender | 0.018 | |||
| Male, n (%) | 17 (70.8) | 73 (90.1) | 0.27 (0.09–0.84) | |
| Female, n (%) | 7 (29.2) | 8 (9.9) | 3.76 (1.20–11.79) | |
| Age, years (SD) | 54.8 ± 17.6 | 52.1 ± 19.2 | - | 0.541 |
| Comorbidities | ||||
| CVA, n (%) | 0 (0.0) | 1 (1.2) | - | 0.584 |
| HTN, n (%) | 8 (33.3) | 16 (19.8) | 2.03 (0.74–5.58) | 0.164 |
| CAD, n (%) | 0 (0.0) | 4 (4.9) | - | 0.267 |
| CHF, n (%) | 0 (0.0) | 0 (0.0) | - | - |
| DM, n (%) | 3 (12.5) | 7 (8.6) | 1.51 (0.36–6.35) | 0.572 |
| ESRD, n (%) | 0 (0.0) | 1 (1.2) | - | 0.584 |
| GCS, median (IQR) | 3 (3–6) | 5 (3–9) | - | 0.230 |
| ISS, median (IQR) | 25 (17–36) | 25 (22–34) | - | 0.296 |
| 1–15, n (%) | 4 (16.7) | 5 (6.2) | 3.04 (0.75–12.38) | 0.107 |
| 16–24, n (%) | 6 (25.0) | 22 (27.2) | 0.89 (0.31–2.54) | 0.833 |
| ≥25, n (%) | 14 (58.3) | 54 (66.7) | 0.70 (0.28–1.78) | 0.453 |
| Mortality, n (%) | 19 (79.2) | 41 (50.6) | 3.71 (1.26–10.89) | 0.013 |
| Hospital LOS, days (SD) | 14.8 ± 21.2 | 18.5 ± 20.0 | - | 0.426 |
| Admitted into ICU, n (%) | 24 (100) | 75 (92.6) | - | 0.170 |
| Variables | Death Triad C | |||
|---|---|---|---|---|
| SBP < 60 mmHg n = 8 | SBP ≥ 60 mmHg n = 17 | OR (95% CI) | p | |
| Gender | 0.668 | |||
| Male, n (%) | 6 (75.0) | 14 (82.4) | 0.64 (0.09–4.89) | |
| Female, n (%) | 2 (25.0) | 3 (17.6) | 1.56 (0.21–11.83) | |
| Age, years (SD) | 52.3 ± 16.4 | 44.8 ± 19.4 | - | 0.359 |
| Comorbidities | ||||
| CVA, n (%) | 0 (0.0) | 0 (0.0) | - | - |
| HTN, n (%) | 2 (25.0) | 3 (17.6) | 1.56 (0.21–11.83) | 0.668 |
| CAD, n (%) | 0 (0.0) | 0 (0.0) | - | - |
| CHF, n (%) | 1 (12.5) | 0 (0.0) | - | 0.137 |
| DM, n (%) | 0 (0.0) | 1 (5.9) | - | 0.484 |
| ESRD, n (%) | 1 (12.5) | 0 (0.0) | - | 0.137 |
| GCS, median (IQR) | 3 (3–3) | 3 (3–12) | - | 0.048 |
| ISS, median (IQR) | 25 (18–37) | 29 (15–38) | - | 0.725 |
| 1–15, n (%) | 1 (12.5) | 4 (23.5) | 0.46 (0.04–5.00) | 0.520 |
| 16–24, n (%) | 2 (25.0) | 2 (11.8) | 2.50 (0.28–22.04) | 0.400 |
| ≥25, n (%) | 5 (62.5) | 11 (64.7) | 0.91 (0.16–5.20) | 0.915 |
| Mortality, n (%) | 8 (100) | 13 (76.5) | - | 0.134 |
| Hospital LOS, days (SD) | 7.1 ± 10.1 | 16.5 ± 21.3 | - | 0.151 |
| Admitted into ICU, n (%) | 4 (50.0) | 15 (88.2) | 0.13 (0.02–1.01) | 0.037 |
| Variables | Trauma Death Tetrad | |||||
|---|---|---|---|---|---|---|
| Death Tetrad A n = 554 | Death Tetrad B n = 106 | Death Tetrad C n = 41 | Death Tetrad D n = 8 | Normal n = 2652 | p | |
| Gender | <0.001 | |||||
| Male, n (%) | 381 (68.8) | 93 (87.7) | 31 (75.6) | 6 (75.0) | 1682 (63.4) | |
| Female, n (%) | 173 (31.2) | 13 (12.3) | 10 (24.4) | 2 (25.0) | 970 (36.6) | |
| Age, years (SD) | 53.7 ± 20.3 | 52.2 ± 18.8 | 50.6 ± 18.8 | 52.3 ± 16.4 | 57.6 ± 19.9 | <0.001 |
| Comorbidities | ||||||
| CVA, n (%) | 13 (2.3) | 2 (1.9) | 0 (0.0) | 0 (0.0) | 156 (5.9) | 0.002 |
| HTN, n (%) | 157 (28.3) | 23 (21.7) | 11 (26.8) | 2 (25.0) | 962 (36.3) | <0.001 |
| CAD, n (%) | 42 (7.6) | 5 (4.7) | 0 (0.0) | 0 (0.0) | 171 (6.4) | 0.282 |
| CHF, n (%) | 8 (1.4) | 0 (0.0) | 0 (0.0) | 1 (12.5) | 21 (0.8) | 0.003 |
| DM, n (%) | 83 (15.0) | 10 (9.4) | 4 (9.8) | 0 (0.0) | 541 (20.4) | 0.001 |
| ESRD, n (%) | 18 (3.2) | 2 (1.9) | 0 (0.0) | 1 (12.5) | 107 (4.0) | 0.269 |
| GCS, median (IQR) | 9 (4–15) | 4 (3–8) | 3 (3–9) | 3 (3–3) | 15 (8–15) | <0.001 |
| ISS, median (IQR) | 22 (16–29) | 25 (21–33) | 25 (16–38) | 25 (18–37) | 16 (9–24) | <0.001 |
| 1–15, n (%) | 134 (24.2) | 9 (8.5) | 8 (19.5) | 1 (12.5) | 1059 (39.9) | <0.001 |
| 16–24, n (%) | 164 (29.6) | 29 (27.4) | 8 (19.5) | 2 (25.0) | 950 (35.8) | 0.005 |
| ≥25, n (%) | 256 (46.2) | 68 (64.2) | 25 (61.0) | 5 (62.5) | 643 (24.2) | <0.001 |
| Mortality(%) | 156 (28.2) | 53 (50.0) | 32 (78.0) | 8 (100) | 276 (10.4) | <0.001 |
| AOR of Mortality | 3.69 (2.93–4.65) | 10.10 (6.65–15.35) | 40.18 (18.73–86.22) | - | - | <0.001 |
| Hospital LOS, days (SD) | 18.4 ± 16.8 | 18.4 ± 19.5 | 15.5 ± 21.0 | 7.1 ± 10.1 | 16.7 ± 15.6 | 0.052 |
| Admitted into ICU, n (%) | 468 (84.5) | 95 (89.6) | 39 (95.1) | 4 (50.0) | 1774 (66.9) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzeng, W.-J.; Tseng, H.-Y.; Hou, T.-Y.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H. From Death Triad to Death Tetrad—The Addition of a Hypotension Component to the Death Triad Improves Mortality Risk Stratification in Trauma Patients: A Retrospective Cohort Study. Diagnostics 2022, 12, 2885. https://doi.org/10.3390/diagnostics12112885
Tzeng W-J, Tseng H-Y, Hou T-Y, Chou S-E, Su W-T, Hsu S-Y, Hsieh C-H. From Death Triad to Death Tetrad—The Addition of a Hypotension Component to the Death Triad Improves Mortality Risk Stratification in Trauma Patients: A Retrospective Cohort Study. Diagnostics. 2022; 12(11):2885. https://doi.org/10.3390/diagnostics12112885
Chicago/Turabian StyleTzeng, Wei-Juo, Hsiang-Yu Tseng, Teng-Yuan Hou, Sheng-En Chou, Wei-Ti Su, Shiun-Yuan Hsu, and Ching-Hua Hsieh. 2022. "From Death Triad to Death Tetrad—The Addition of a Hypotension Component to the Death Triad Improves Mortality Risk Stratification in Trauma Patients: A Retrospective Cohort Study" Diagnostics 12, no. 11: 2885. https://doi.org/10.3390/diagnostics12112885