
The Impact of Coronavirus Disease 2019 on Maternal and Fetal Wellbeing in New Mexico


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. COVID Data Tracker. Available online: https://COVID.cdc.gov/COVID-data-tracker (accessed on 15 June 2022).
- Diriba, K.; Awulachew, E.; Getu, E. The Effect of Coronavirus Infection (SARS-CoV-2, MERS-CoV, and SARS-CoV) during Pregnancy and the Possibility of Vertical Maternal-Fetal Transmission: A Systematic Review and Meta-Analysis. Eur. J. Med. Res. 2020, 25, 39. [Google Scholar] [CrossRef] [PubMed]
- Bahadur, G.; Homburg, R.; Yoong, W.; Singh, C.; Bhat, M.; Kotabagi, P.; Acharya, S.; Huirne, J.; Doreski, P.A.; Łukaszuk, M.; et al. Adverse Outcomes in SAR-CoV-2 (COVID-19) and SARS Virus Related Pregnancies with Probable Vertical Transmission. JBRA Assist. Reprod. 2020, 24, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, M.B.; Cavalcante, C.T.d.M.B.; Sarno, M.; Barini, R.; Kwak-Kim, J. Maternal Immune Responses and Obstetrical Outcomes of Pregnant Women with COVID-19 and Possible Health Risks of Offspring. J. Reprod. Immunol. 2021, 143, 103250. [Google Scholar] [CrossRef] [PubMed]
- Dang, D.; Wang, L.; Zhang, C.; Li, Z.; Wu, H. Potential Effects of SARS-CoV-2 Infection during Pregnancy on Fetuses and Newborns Are Worthy of Attention. J. Obstet. Gynaecol. Res. 2020, 46, 1951–1957. [Google Scholar] [CrossRef]
- Di Mascio, D.; Khalil, A.; Saccone, G.; Rizzo, G.; Buca, D.; Liberati, M.; Vecchiet, J.; Nappi, L.; Scambia, G.; Berghella, V.; et al. Outcome of Coronavirus Spectrum Infections (SARS, MERS, COVID-19) during Pregnancy: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100107. [Google Scholar] [CrossRef]
- Mahyuddin, A.P.; Kanneganti, A.; Wong, J.J.L.; Dimri, P.S.; Su, L.L.; Biswas, A.; Illanes, S.E.; Mattar, C.N.Z.; Huang, R.Y.-J.; Choolani, M. Mechanisms and Evidence of Vertical Transmission of Infections in Pregnancy Including SARS-CoV-2s. Prenat. Diagn. 2020, 40, 1655–1670. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic Characterisation and Epidemiology of 2019 Novel Coronavirus: Implications for Virus Origins and Receptor Binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Yang, Z.; Liu, Y. Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2: A Systematic Review. Am. J. Perinatol. 2020, 37, 1055–1060. [Google Scholar] [CrossRef]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Sinaci, S.; Ocal, D.F.; Seven, B.; Anuk, A.T.; Besimoglu, B.; Keven, M.C.; Goncu Ayhan, S.; Akin, M.S.; Tayman, C.; Keskin, H.L.; et al. Vertical Transmission of SARS-CoV-2: A Prospective Cross-Sectional Study from a Tertiary Center. J. Med. Virol. 2021, 93, 5864–5872. [Google Scholar] [CrossRef] [PubMed]
- Patanè, L.; Morotti, D.; Giunta, M.R.; Sigismondi, C.; Piccoli, M.G.; Frigerio, L.; Mangili, G.; Arosio, M.; Cornolti, G. Vertical Transmission of Coronavirus Disease 2019: Severe Acute Respiratory Syndrome Coronavirus 2 RNA on the Fetal Side of the Placenta in Pregnancies with Coronavirus Disease 2019-Positive Mothers and Neonates at Birth. Am. J. Obstet. Gynecol. MFM 2020, 2, 100145. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 Vertical Transmission during Pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical Transmission of Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Research Committee; Society for Maternal-Fetal Medicine (SMFM); Boelig, R.C.; Aagaard, K.M.; Debbink, M.P.; Shamshirsaz, A.A.; SMFM Research Committee. Society for Maternal-Fetal Medicine Special Statement: COVID-19 Research in Pregnancy: Progress and Potential. Am. J. Obstet. Gynecol. 2021, 225, B19–B31. [Google Scholar] [CrossRef]
- Golden, T.N.; Simmons, R.A. Maternal and Neonatal Response to COVID-19. Am. J. Physiol. Endocrinol. Metab. 2020, 319, E315–E319. [Google Scholar] [CrossRef]
- Tabary, M.; Khanmohammadi, S.; Araghi, F.; Dadkhahfar, S.; Tavangar, S.M. Pathologic Features of COVID-19: A Concise Review. Pathol. Res. Pract. 2020, 216, 153097. [Google Scholar] [CrossRef]
- Singh, N.; Buckley, T.; Shertz, W. Placental Pathology in COVID-19: Case Series in a Community Hospital Setting. Cureus 2021, 13, e12522. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Morotti, D. Placental Pathology of COVID-19 with and without Fetal and Neonatal Infection: Trophoblast Necrosis and Chronic Histiocytic Intervillositis as Risk Factors for Transplacental Transmission of SARS-CoV-2. Viruses 2020, 12, 1308. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Avvad-Portari, E.; Babál, P.; Baldewijns, M.; Blomberg, M.; Bouachba, A.; Camacho, J.; Collardeau-Frachon, S.; Colson, A.; Dehaene, I.; et al. Placental Tissue Destruction and Insufficiency From COVID-19 Causes Stillbirth and Neonatal Death From Hypoxic-Ischemic Injury. Arch. Pathol. Lab. Med. 2022, 146, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Watkins, J.C.; Torous, V.F.; Roberts, D.J. Defining Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Placentitis. Arch. Pathol. Lab. Med. 2021, 145, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Dumont, S.; Balduyck, J.; Reynders, M.; Vanwalleghem, L.; Lebbe, B. Acute SARS-CoV-2 Alpha Variant Infection Leading to Placental Insufficiency and Fetal Distress. J. Med. Virol. 2022, 94, 1196–1200. [Google Scholar] [CrossRef] [PubMed]
- Shook, L.L.; Sullivan, E.L.; Lo, J.O.; Perlis, R.H.; Edlow, A.G. COVID-19 in Pregnancy: Implications for Fetal Brain Development. Trends Mol. Med. 2022, 28, 319–330. [Google Scholar] [CrossRef]
- Marchand, G.; Patil, A.S.; Masoud, A.T.; Ware, K.; King, A.; Ruther, S.; Brazil, G.; Calteux, N.; Ulibarri, H.; Parise, J.; et al. Systematic Review and Meta-Analysis of COVID-19 Maternal and Neonatal Clinical Features and Pregnancy Outcomes up to June 3, 2021. AJOG Glob. Rep. 2022, 2, 100049. [Google Scholar] [CrossRef]
- Jering, K.S.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Vardeny, O.; Greene, M.F.; Solomon, S.D. Clinical Characteristics and Outcomes of Hospitalized Women Giving Birth With and Without COVID-19. JAMA Intern. Med. 2021, 181, 714–717. [Google Scholar] [CrossRef]
- Rosenbloom, J.I.; Raghuraman, N.; Carter, E.B.; Kelly, J.C. Coronavirus Disease 2019 Infection and Hypertensive Disorders of Pregnancy. Am. J. Obstet. Gynecol. 2021, 224, 623–624. [Google Scholar] [CrossRef]
- Norman, M.; Navér, L.; Söderling, J.; Ahlberg, M.; Hervius Askling, H.; Aronsson, B.; Byström, E.; Jonsson, J.; Sengpiel, V.; Ludvigsson, J.F.; et al. Association of Maternal SARS-CoV-2 Infection in Pregnancy With Neonatal Outcomes. JAMA 2021, 325, 2076–2086. [Google Scholar] [CrossRef]
- Vega-Fernández, A.G.; Zevallos-Vargas, B.M.; Flores-Figueroa, F.D.P.; Holguín-Plasencia, J.C.; Centeno-Fuentes, L.M.G.; Ayquipa-Gil, S.A.; Lescano-Alva, R.A.; Arrasco-Castro, K.P.; Alvarado-Herrera, H.A.; Zafra-Alegre, W.R.; et al. Clinical and epidemiological characteristics of mothers with COVID-19 and their neonates: Vertical transmission. Medwave 2021, 21, e8454. [Google Scholar] [CrossRef]
- Gee, S.; Chandiramani, M.; Seow, J.; Pollock, E.; Modestini, C.; Das, A.; Tree, T.; Doores, K.J.; Tribe, R.M.; Gibbons, D.L. The Legacy of Maternal SARS-CoV-2 Infection on the Immunology of the Neonate. Nat. Immunol. 2021, 22, 1490–1502. [Google Scholar] [CrossRef]
- Kyle, M.H.; Dumitriu, D. The Effect of Coronavirus Disease 2019 on Newborns. Curr. Opin. Pediatr. 2021, 33, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Rasmussen, S.A. An Update on COVID-19 and Pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef] [PubMed]
- de Medeiros, K.S.; Sarmento, A.C.A.; Costa, A.P.F.; Macêdo, L.T.d.A.; da Silva, L.A.S.; de Freitas, C.L.; Simões, A.C.Z.; Gonçalves, A.K. Consequences and Implications of the Coronavirus Disease (COVID-19) on Pregnancy and Newborns: A Comprehensive Systematic Review and Meta-Analysis. Int. J. Gynaecol. Obstet. 2022, 156, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Edlow, A.G.; Castro, V.M.; Shook, L.L.; Kaimal, A.J.; Perlis, R.H. Neurodevelopmental Outcomes at 1 Year in Infants of Mothers Who Tested Positive for SARS-CoV-2 During Pregnancy. JAMA Netw. Open. 2022, 5, e2215787. [Google Scholar] [CrossRef] [PubMed]
- Shuffrey, L.C.; Firestein, M.R.; Kyle, M.H.; Fields, A.; Alcántara, C.; Amso, D.; Austin, J.; Bain, J.M.; Barbosa, J.; Bence, M.; et al. Association of Birth During the COVID-19 Pandemic With Neurodevelopmental Status at 6 Months in Infants With and Without In Utero Exposure to Maternal SARS-CoV-2 Infection. JAMA Pediatr. 2022, 176, e215563. [Google Scholar] [CrossRef]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on Maternal and Neonatal Outcomes: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2021, 27, 36–46. [Google Scholar] [CrossRef]
- Omar, M.; Youssef, M.R.; Trinh, L.N.; Attia, A.S.; Elshazli, R.M.; Jardak, C.L.; Farhoud, A.S.; Hussein, M.H.; Shihabi, A.; Elnahla, A.; et al. Excess of Cesarean Births in Pregnant Women with COVID-19: A Meta-Analysis. Birth 2022, 49, 179–193. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. COVID-19 FAQs for Obstetricians-Gynecologists, Obstetrics. Available online: https://www.acog.org/clinical-information/physician-faqs/COVID-19-faqs-for-ob-gyns-obstetrics (accessed on 2 June 2022).
- Cai, J.; Tang, M.; Gao, Y.; Zhang, H.; Yang, Y.; Zhang, D.; Wang, H.; Liang, H.; Zhang, R.; Wu, B. Cesarean Section or Vaginal Delivery to Prevent Possible Vertical Transmission From a Pregnant Mother Confirmed With COVID-19 to a Neonate: A Systematic Review. Front. Med. 2021, 8, 634949. [Google Scholar] [CrossRef]
- Papapanou, M.; Papaioannou, M.; Petta, A.; Routsi, E.; Farmaki, M.; Vlahos, N.; Siristatidis, C. Maternal and Neonatal Characteristics and Outcomes of COVID-19 in Pregnancy: An Overview of Systematic Reviews. Int. J. Environ. Res. Public Health 2021, 18, 596. [Google Scholar] [CrossRef]
- Matar, R.; Alrahmani, L.; Monzer, N.; Debiane, L.G.; Berbari, E.; Fares, J.; Fitzpatrick, F.; Murad, M.H. Clinical Presentation and Outcomes of Pregnant Women With Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2021, 72, 521–533. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Overton, E.E.; Goffman, D.; Friedman, A.M. The Epidemiology of COVID-19 in Pregnancy. Clin. Obstet. Gynecol. 2022, 65, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Espinoza, J.; Gonçalves, L.F.; Kusanovic, J.P.; Friel, L.A.; Nien, J.K. Inflammation in Preterm and Term Labour and Delivery. Semin. Fetal Neonatal Med. 2006, 11, 317–326. [Google Scholar] [CrossRef]
- Wei, S.-Q.; Fraser, W.; Luo, Z.-C. Inflammatory Cytokines and Spontaneous Preterm Birth in Asymptomatic Women: A Systematic Review. Obstet. Gynecol. 2010, 116 Pt 1, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Perez, O.; Prats Rodriguez, P.; Muner Hernandez, M.; Encinas Pardilla, M.B.; Perez Perez, N.; Vila Hernandez, M.R.; Villalba Yarza, A.; Nieto Velasco, O.; Del Barrio Fernandez, P.G.; Forcen Acebal, L.; et al. The Association between SARS-CoV-2 Infection and Preterm Delivery: A Prospective Study with a Multivariable Analysis. BMC Pregnancy Childbirth 2021, 21, 273. [Google Scholar] [CrossRef]
- Bobei, T.-I.; Haj Hamoud, B.; Sima, R.-M.; Gorecki, G.-P.; Poenaru, M.-O.; Olaru, O.-G.; Ples, L. The Impact of SARS-CoV-2 Infection on Premature Birth-Our Experience as COVID Center. Medicina 2022, 58, 587. [Google Scholar] [CrossRef] [PubMed]
- Blitz, M.J.; Gerber, R.P.; Gulersen, M.; Shan, W.; Rausch, A.C.; Prasannan, L.; Meirowitz, N.; Rochelson, B. Preterm Birth among Women with and without Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Acta Obstet. Gynecol. Scand. 2021, 100, 2253–2259. [Google Scholar] [CrossRef]
- Gurol-Urganci, I.; Jardine, J.E.; Carroll, F.; Draycott, T.; Dunn, G.; Fremeaux, A.; Harris, T.; Hawdon, J.; Morris, E.; Muller, P.; et al. Maternal and Perinatal Outcomes of Pregnant Women with SARS-CoV-2 Infection at the Time of Birth in England: National Cohort Study. Am. J. Obstet. Gynecol. 2021, 225, 522.e1–522.e11. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Romero, R. SARS-CoV-2 Infection during Pregnancy and Risk of Preeclampsia: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2022, 226, 68–89.e3. [Google Scholar] [CrossRef]
- Papageorghiou, A.T.; Deruelle, P.; Gunier, R.B.; Rauch, S.; García-May, P.K.; Mhatre, M.; Usman, M.A.; Abd-Elsalam, S.; Etuk, S.; Simmons, L.E.; et al. Preeclampsia and COVID-19: Results from the INTERCOVID Prospective Longitudinal Study. Am. J. Obstet. Gynecol. 2021, 225, 289.e1–289.e17. [Google Scholar] [CrossRef]
- Metz, T.D.; Clifton, R.G.; Hughes, B.L.; Sandoval, G.; Saade, G.R.; Grobman, W.A.; Manuck, T.A.; Miodovnik, M.; Sowles, A.; Clark, K.; et al. Disease Severity and Perinatal Outcomes of Pregnant Patients With Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2021, 137, 571–580. [Google Scholar] [CrossRef]
- Vouga, M.; Favre, G.; Martinez-Perez, O.; Pomar, L.; Acebal, L.F.; Abascal-Saiz, A.; Hernandez, M.R.V.; Hcini, N.; Lambert, V.; Carles, G.; et al. Maternal Outcomes and Risk Factors for COVID-19 Severity among Pregnant Women. Sci. Rep. 2021, 11, 13898. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Samara, A.; Chowdhury, T.; O’Brien, P. Does COVID-19 Cause Pre-Eclampsia? Ultrasound Obstet. Gynecol. 2022, 59, 146–152. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Impact of Racism on Our Nation’s Health. Available online: https://www.cdc.gov/healthequity/racism-disparities/impact-of-racism.html (accessed on 23 June 2022).
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Gravlee, C.C. Systemic Racism, Chronic Health Inequities, and COVID-19: A Syndemic in the Making? Am. J. Hum. Biol. 2020, 32, e23482. [Google Scholar] [CrossRef] [PubMed]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural Racism and Health Inequities in the USA: Evidence and Interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Crear-Perry, J.; Correa-de-Araujo, R.; Lewis Johnson, T.; McLemore, M.R.; Neilson, E.; Wallace, M. Social and Structural Determinants of Health Inequities in Maternal Health. J. Women’s Health 2021, 30, 230–235. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ICD 10 Codes | |
|---|---|
| B34.2 | Coronavirus infection, unspecified |
| B97.2 | Coronavirus as the cause of diseases classified elsewhere |
| B97.29 | Other coronavirus as the cause of diseases classified elsewhere |
| J12.81 | Pneumonia due to SARS-associated coronavirus |
| Z20.822 | Contact with and (suspected) exposure to COVID-19 |
| Z11.52 | Encounter for screening for COVID-19 |
| Z86.16 | Personal history of COVID-19 |
| M35.81 | Multisystem inflammatory syndrome |
| J12.82 | Pneumonia due to coronavirus disease 2019 |
| Z33.1 | Pregnancy (single) (uterine) |
| 030.9 | Pregnancy (multiple) |
| Maternal COVID-19 Infection During Pregnancy | ||||
|---|---|---|---|---|
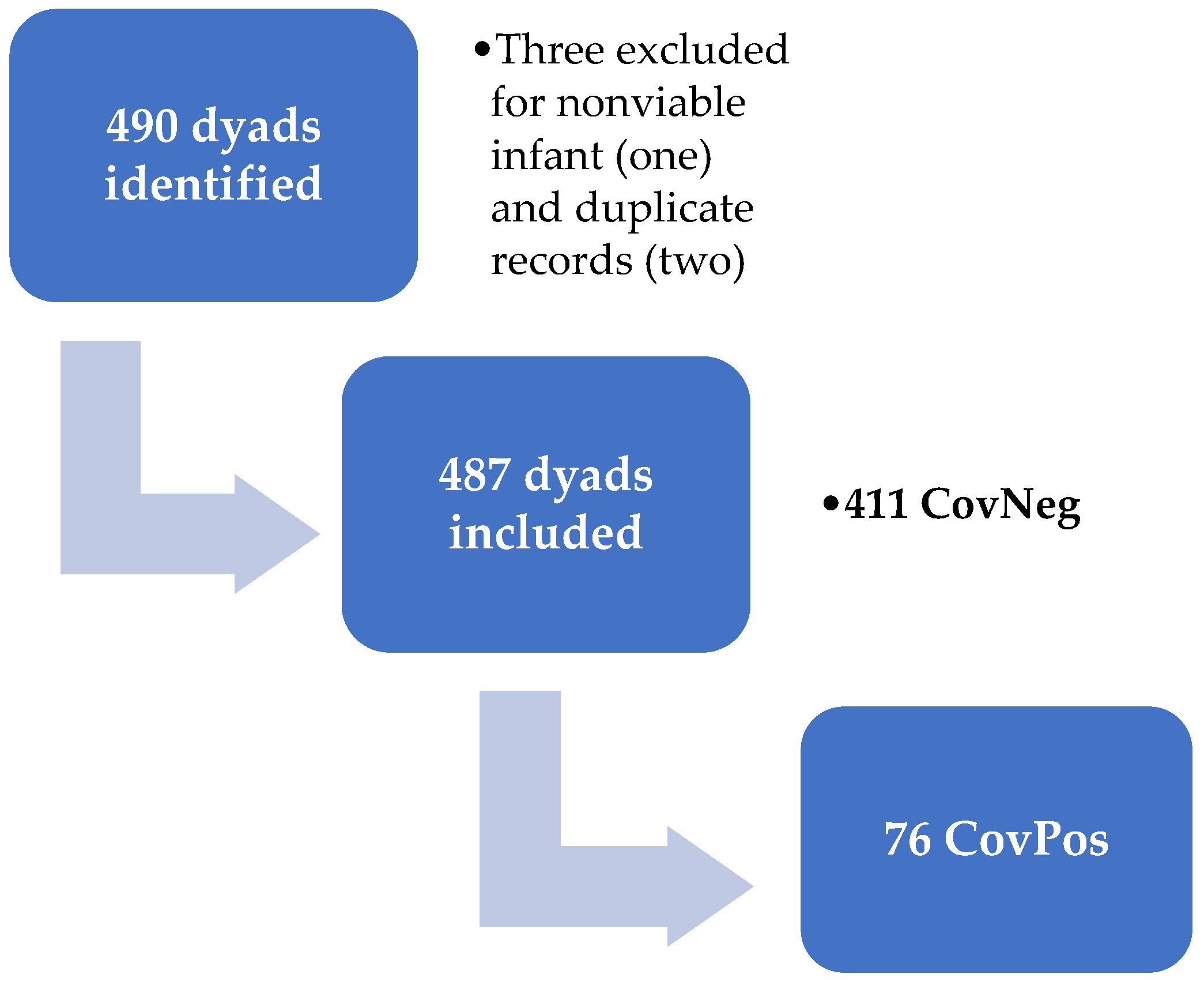
| Demographics | Overall (n = 487) | No (n = 411) | Yes (n = 76) | p-Value |
| n (%) | n (%) | n (%) | ||
| Trimester of Infection | ||||
| 1 | 5 (7) | |||
| 2 | 6 (21) | |||
| 3 | 55 (72) | |||
| Race/ethnicity | 0.02 | |||
| American Indian/Alaska Native | 66 (14) | 50 (12) | 16 (21) | |
| Hispanic | 263 (54) | 218 (53) | 45 (59) | |
| Non-Hispanic white | 82 (17) | 77 (19) | 5 (7) | |
| Asian | 14 (3) | 14 (3) | 0 (0) | |
| Black/AA * | 18 (4) | 16 (4) | 2 (3) | |
| Other/no answer | 44 (9) | 36 (9) | 8 (11) | |
| Sex of child | 0.77 | |||
| Female | 236 (48) | 198 (48) | 38 (50) | |
| Male | 251 (52) | 213 (52) | 38 (50) | |
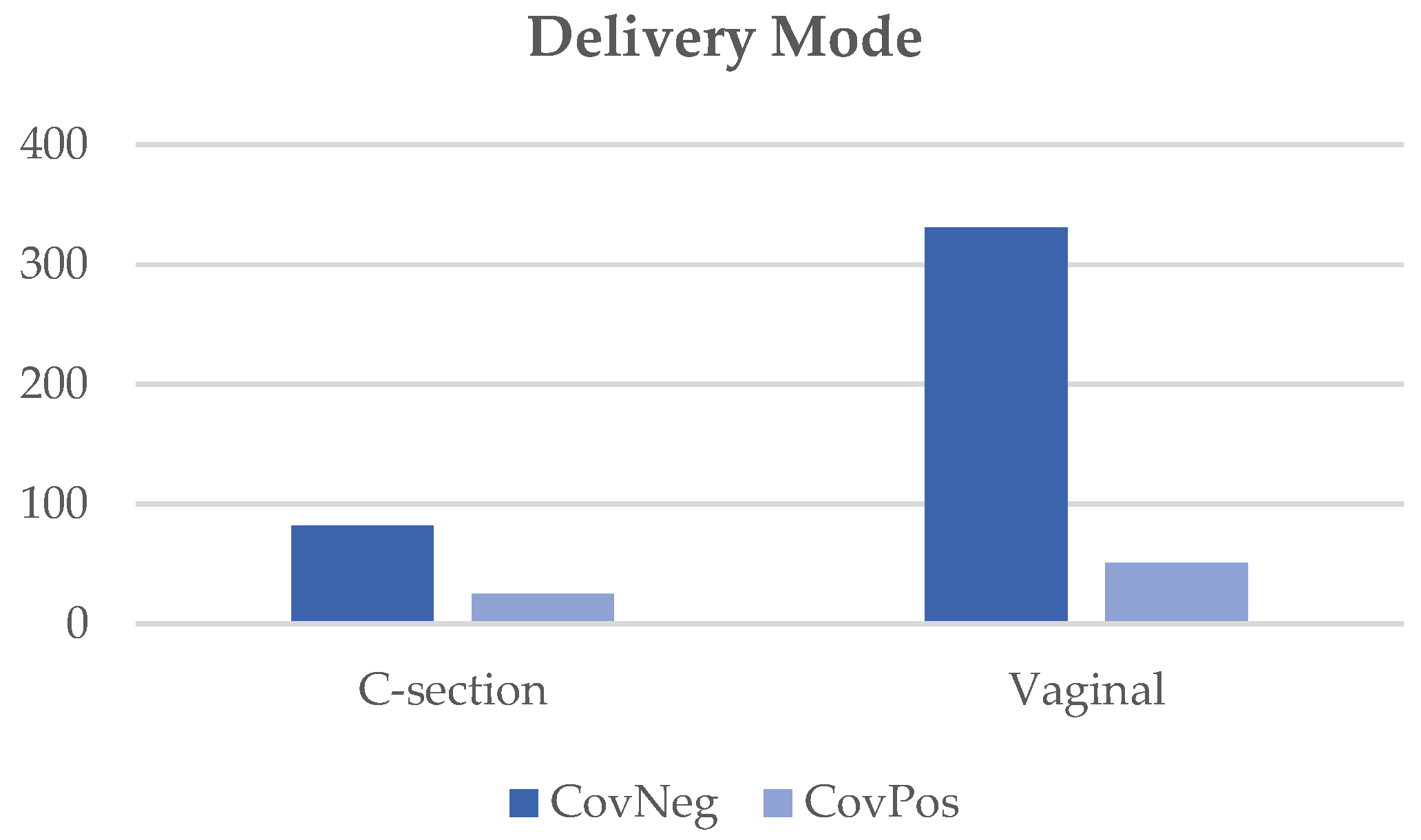
| Delivery mode | 0.01 | |||
| C-section | 107 (22) | 82 (20) | 25 (33) | |
| Vaginal | 380 (78) | 331 (80) | 51 (67) | |
| Hospitalization for COVID? | ||||
| n/a | 411 (100) | - | ||
| No | - | 59 (78) | ||
| Yes | - | 15 (20) | ||
| Unknown | - | 2 (2) | ||
| Pre-eclampsia | 0.97 | |||
| No | 430 (88) | 363 (88) | 67 (88) | |
| Yes | 57 (12) | 48 (12) | 9 (12) | |
| Chronic HTN + | 0.49 | |||
| No | 457 (94) | 387 (94) | 70 (92) | |
| Yes | 30 (6) | 24 (6) | 6 (8) | |
| Gestational HTN | 0.14 | |||
| No | 439 (90) | 367 (89) | 72 (95) | |
| Yes | 48 (10) | 44 (11) | 4 (5) | |
| Maternal COVID-19 Infection During Pregnancy | ||||
|---|---|---|---|---|
| Overall (n = 487) | No (n = 411) | Yes (n = 76) | p-Value | |
| n (%) | n (%) | n (%) | ||
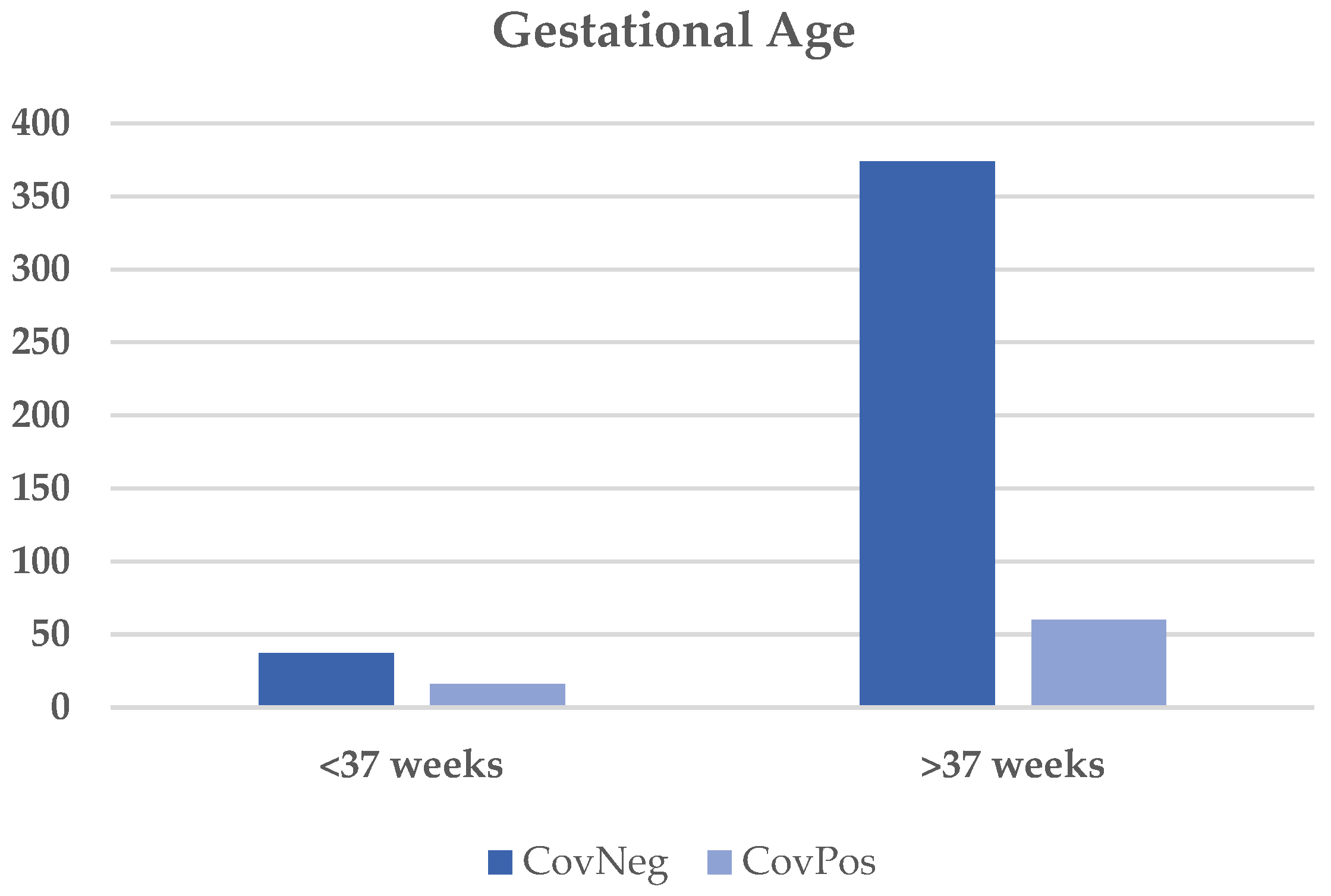
| Gestational Age | 0.002 | |||
| <37 weeks | 53 (11) | 37 (9) | 16 (21) | |
| ≥37 weeks | 434 (89) | 374 (91) | 60 (79) | |
| Birthweight Category ** | ||||
| AGA | 0.01 | |||
| LGA | 408 (84) | 348 (85) | 60 (79) | |
| SGA | 23 (5) | 14 (3) | 9 (12) | |
| sSGA | 30 (6) | 25 (6) | 5 (7) | |
| 26 (5) | 24 (6) | 2 (3) | ||
| Any SGA | ||||
| Yes | ||||
| No | 56 (11) | 49 (12) | 7 (9) | 0.50 |
| 431 (89) | 362 (88) | 69 (91) | ||
| Any LGA | ||||
| Yes | 23 (5) | 14 (3) | 9 (12) | 0.001 |
| No | 464 (95) | 397 (97) | 67 (88) | |
| Admit ++ | 0.07 | |||
| NBN | 385 (79) | 330 (80) | 55 (72) | |
| NICU | 85 (17) | 65 (16) | 20 (26) | |
| ICN | 16 (3) | 15 (4) | 1 (1) | |
| APGAR (1 min) | 0.37 | |||
| Abnormal (0–3) | 23 (5) | 17 (4) | 6 (8) | |
| Mod Abnormal (4–6) ^ | 45 (9) | 38 (9) | 7 (9) | |
| Normal (7–10) | 417 (85) | 354 (87) | 63 (83) | |
| APGAR (5 min) | 0.50 | |||
| Abnormal (0–3) | 7 (1) | 6 (1) | 1 (1) | |
| Mod Abnormal (4–6) ^ | 16 (3) | 12 (3) | 4 (5) | |
| Normal (7–10) | 462 (95) | 391 (96) | 71 (93) | |
| Maternal COVID-19 Infection | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | ||||||||
| n | Mean | SD | Median | n | Mean | SD | Median | ||
| Birthweight (g) | 409 | 3144 | 546 | 3190 | 76 | 3064 | 769 | 3168 | 0.37 |
| Head Circumference | 410 | 34 | 2 | 34 | 76 | 34 | 2 | 34 | 0.28 |
| Gestational Age (Weeks) | 411 | 38.7 | 2.3 | 38.9 | 76 | 37.9 | 2.5 | 38.9 | 0.005 |
| Factors from Table 2 | Associations | p-Value |
|---|---|---|
| Race/Ethnicity | Gestational HTN | 0.004 |
| Delivery Mode | Tobacco use | <0.001 |
| Pre-eclampsia | <0.001 | |
| GA * < 37 Weeks | Trimester of infection | 0.01 |
| Pre-eclampsia | <0.001 | |
| Chronic HTN | 0.02 | |
| Any LGA | Trimester of infection | 0.01 |
| Admit | APGAR (1 Min) | <0.001 |
| APGAR (5 Min) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emery, T.; Baillie, K.; Myers, O.; Ko, H.; Maxwell, J.R. The Impact of Coronavirus Disease 2019 on Maternal and Fetal Wellbeing in New Mexico. Diagnostics 2022, 12, 2856. https://doi.org/10.3390/diagnostics12112856
Emery T, Baillie K, Myers O, Ko H, Maxwell JR. The Impact of Coronavirus Disease 2019 on Maternal and Fetal Wellbeing in New Mexico. Diagnostics. 2022; 12(11):2856. https://doi.org/10.3390/diagnostics12112856
Chicago/Turabian StyleEmery, Tiffany, Kati Baillie, Orrin Myers, Hellen Ko, and Jessie R. Maxwell. 2022. "The Impact of Coronavirus Disease 2019 on Maternal and Fetal Wellbeing in New Mexico" Diagnostics 12, no. 11: 2856. https://doi.org/10.3390/diagnostics12112856