
HRU-Net: A Transfer Learning Method for Carotid Artery Plaque Segmentation in Ultrasound Images
Abstract
:1. Introduction
- (A)
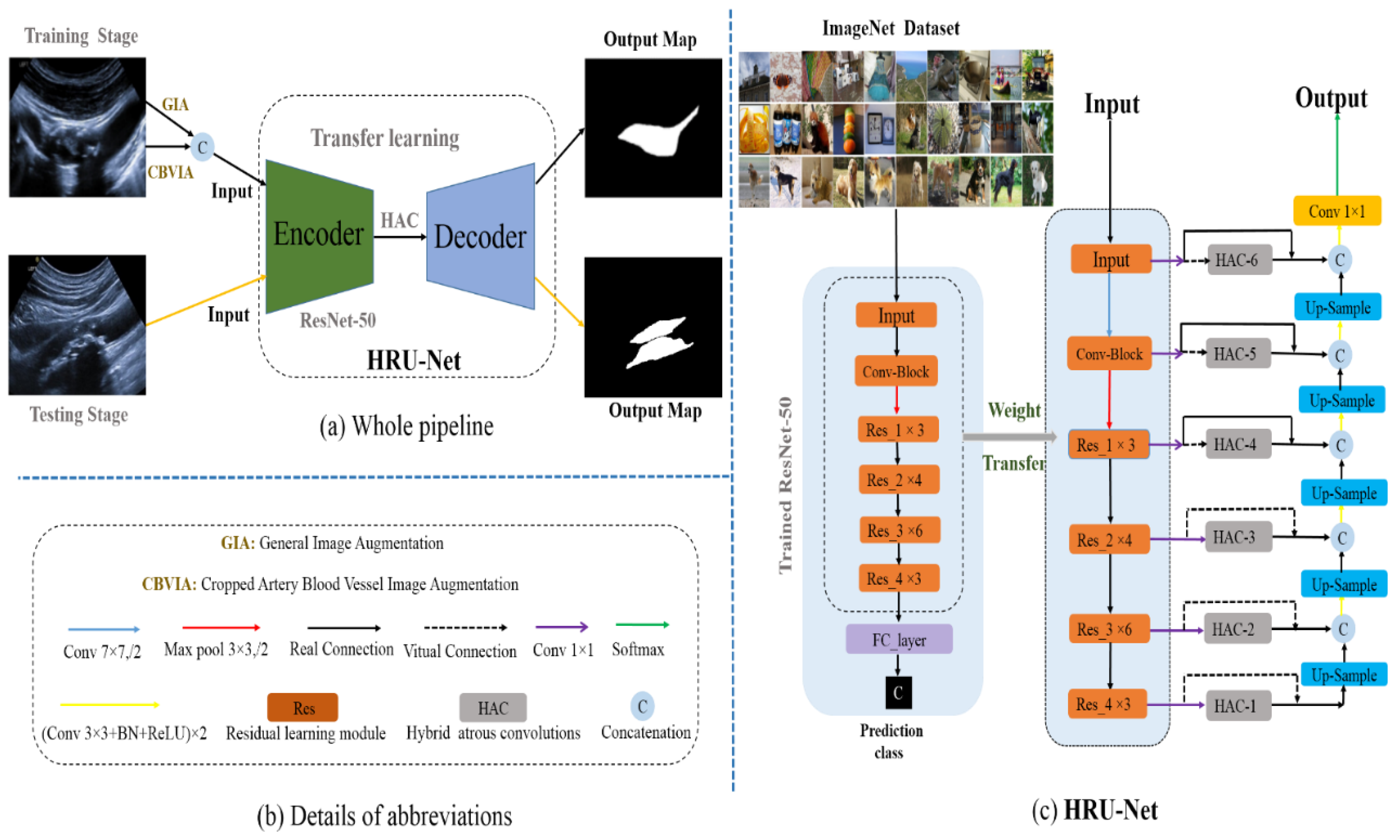
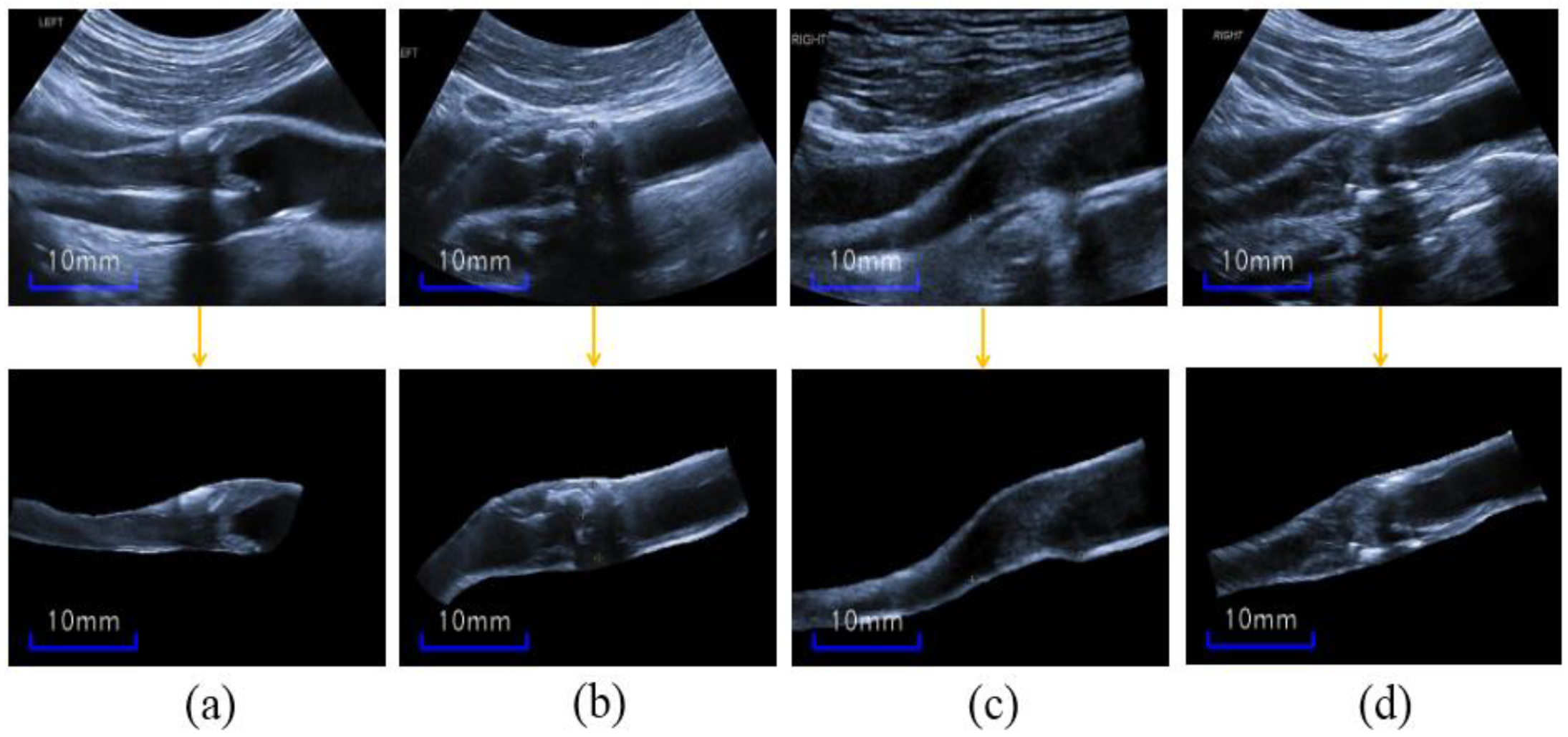
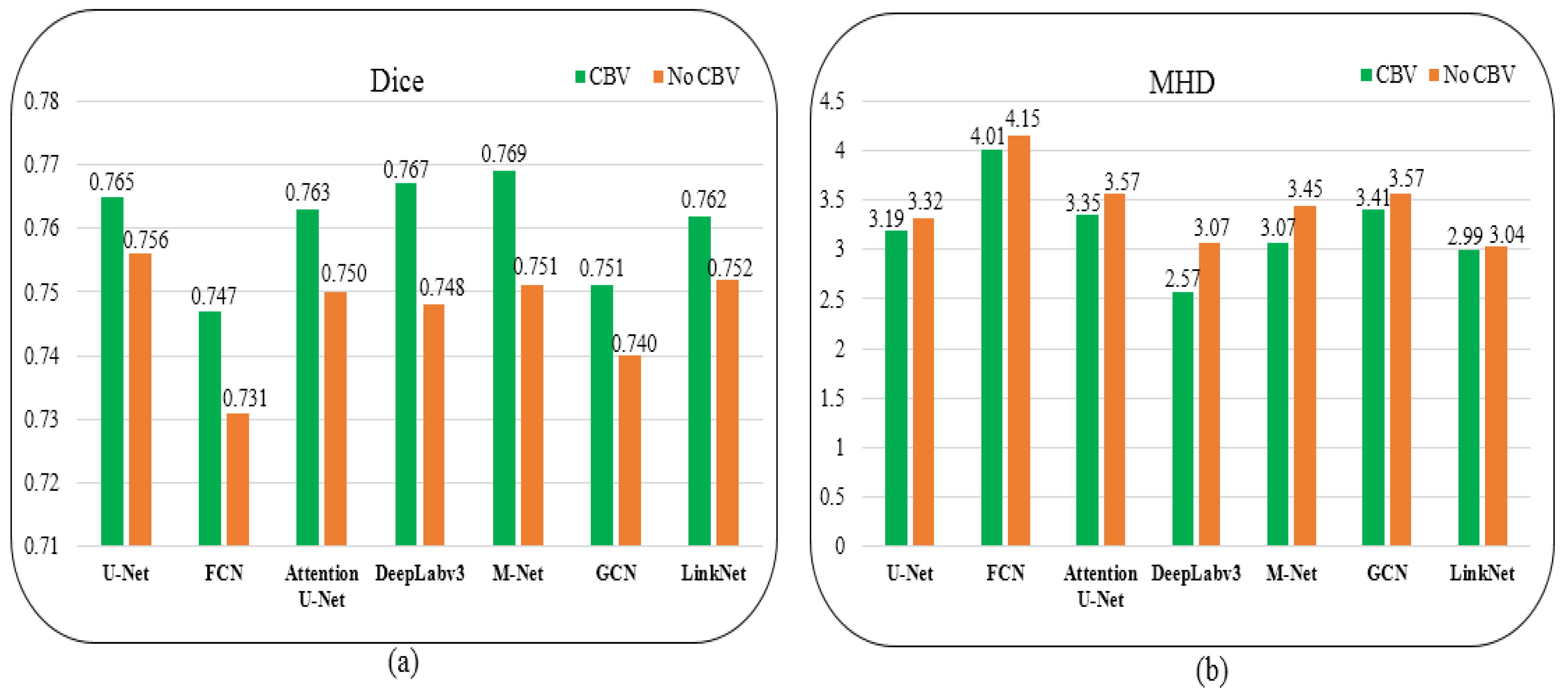
- We utilized cropped carotid blood vessel (CBV) images as a data augmentation mode, and CBV provided plaque position constraint during data training; moreover, the transfer learning from trained ResNet-50 was made use of for ultrasound plaque segmentation.
- (B)
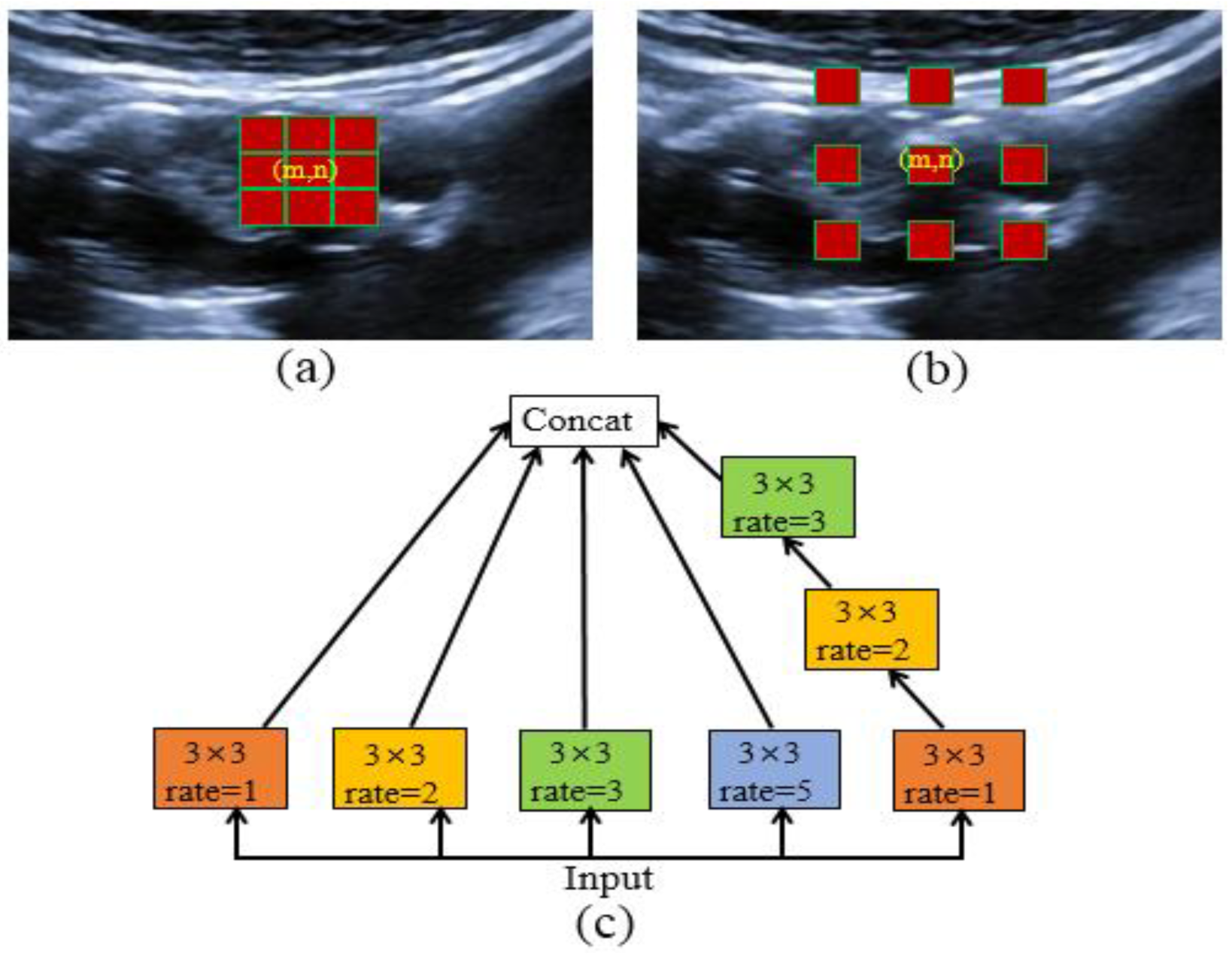
- Hybrid atrous convolutions (HACs) were used on the last three high-level layers of the ResNet-50, and the HACs could obtain more receptive fields to discriminate similar textures between plaques and speckle noise.
- (C)
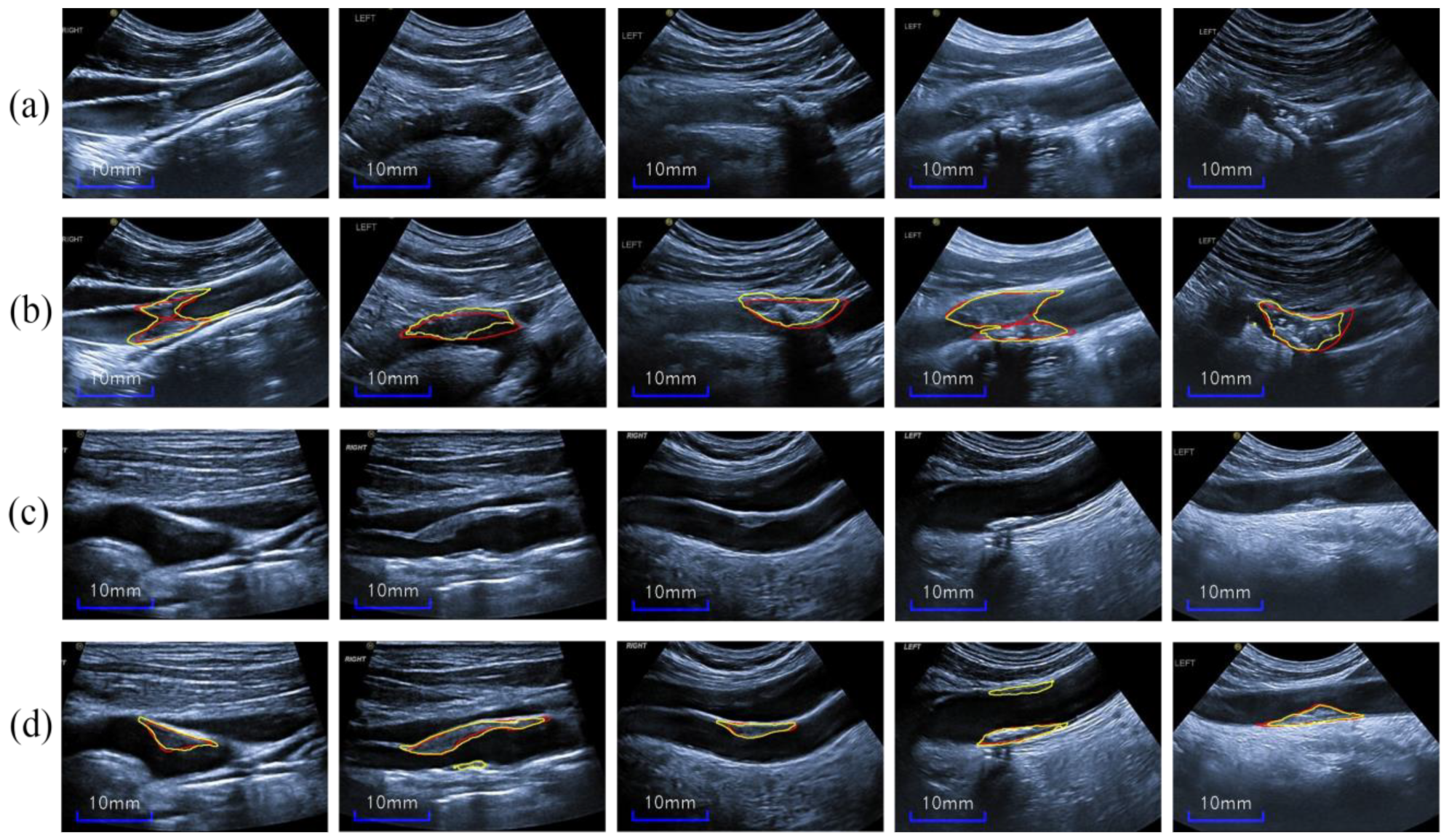
- We tested our model on noisy ultrasound images with varying degrees of carotid stenosis, showing a fine segmentation performance.
2. Related Work
CNN-Based Segmentation for Carotid Ultrasound Images
3. Methods
3.1. Image Augmentation
3.1.1. General Image Augmentation (GIA)
3.1.2. Cropped-Blood-Vessel Image Augmentation (CBVIA)
3.2. ResNet-50 Based U-Net (RU-Net) Transfer Learning
3.3. Hybrid Atrous Convolutions (HAC) Module
3.4. Dataset
3.5. Metric
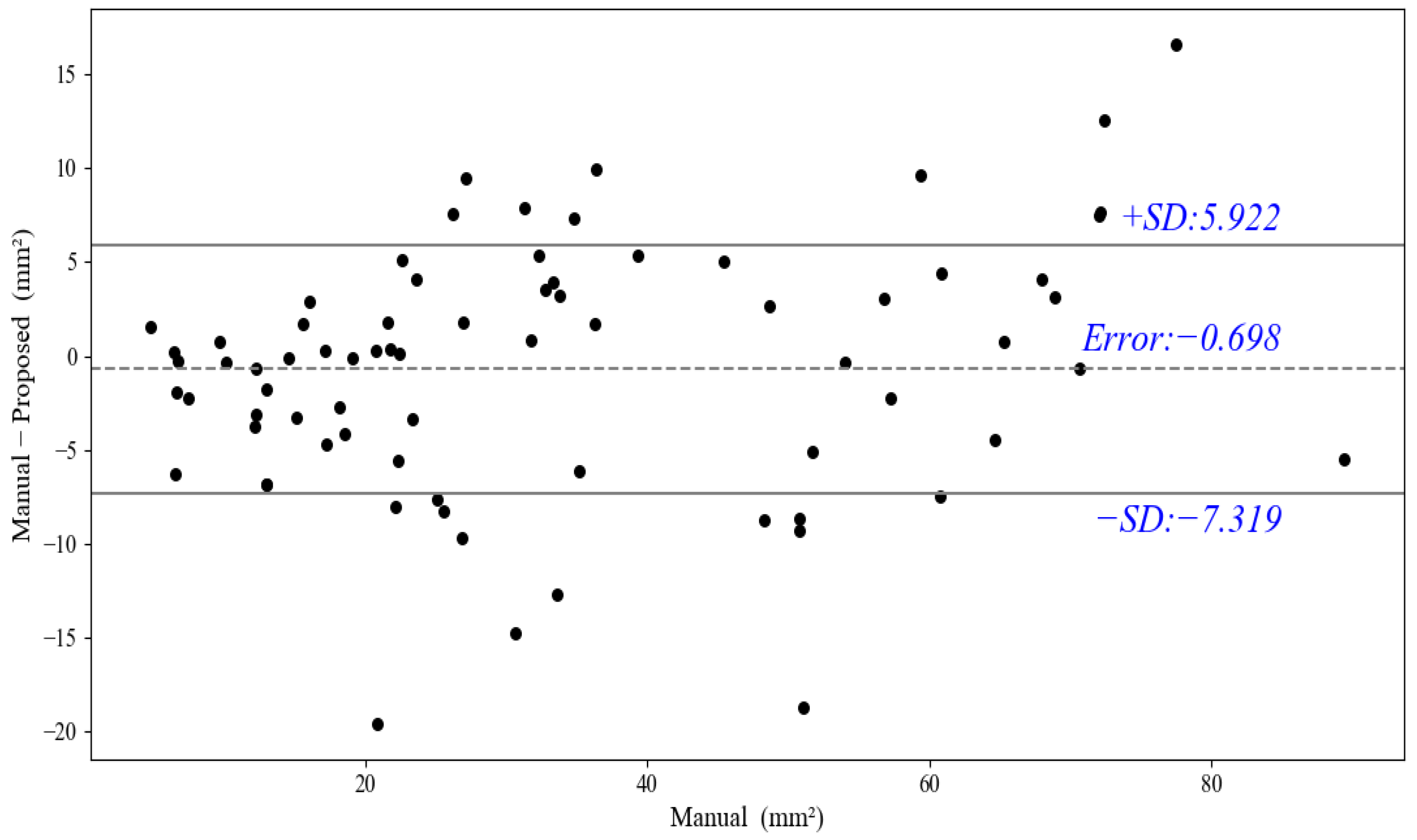
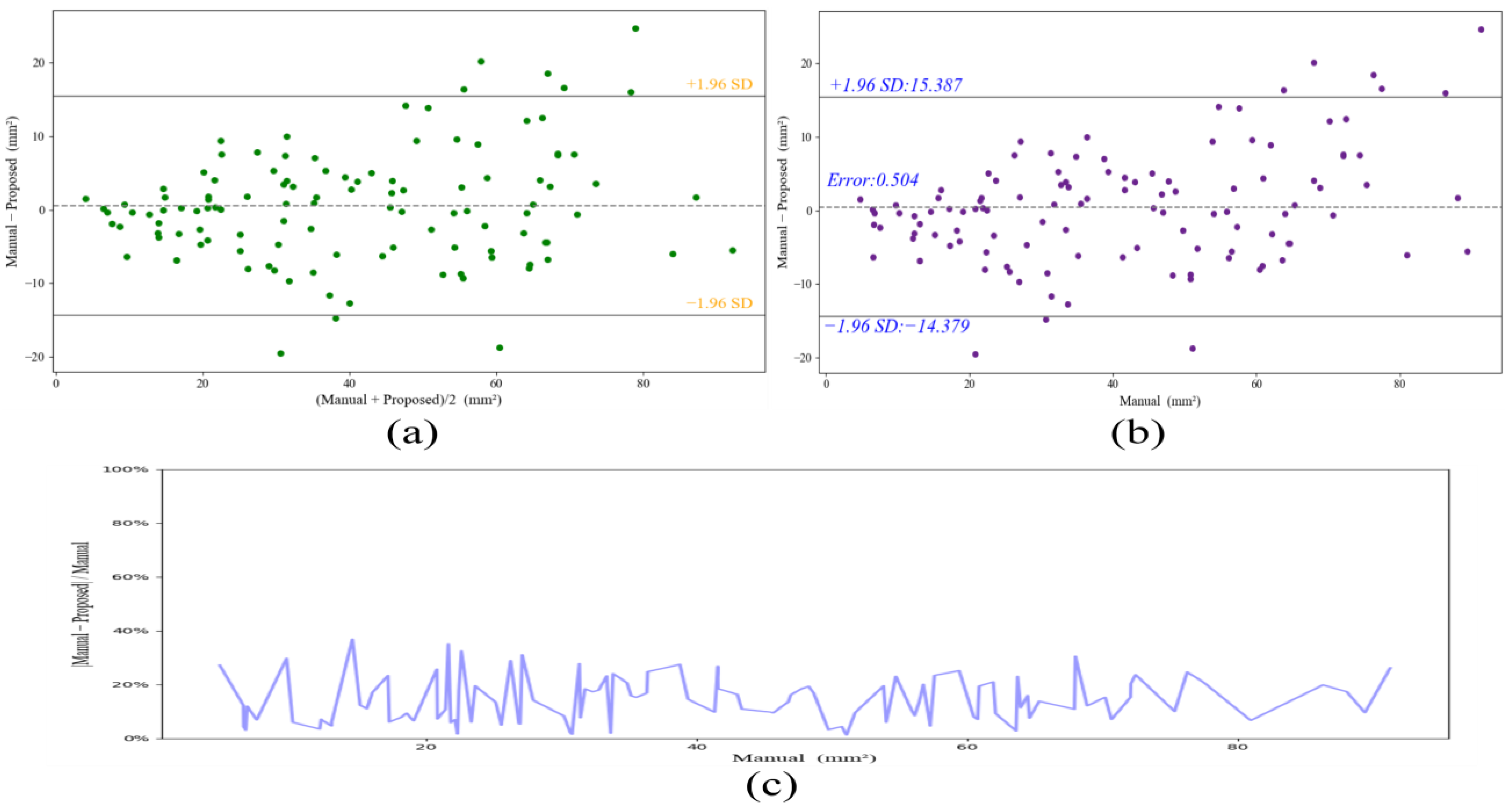
3.6. Statistical Analysis
3.7. Implementation Details
4. Results
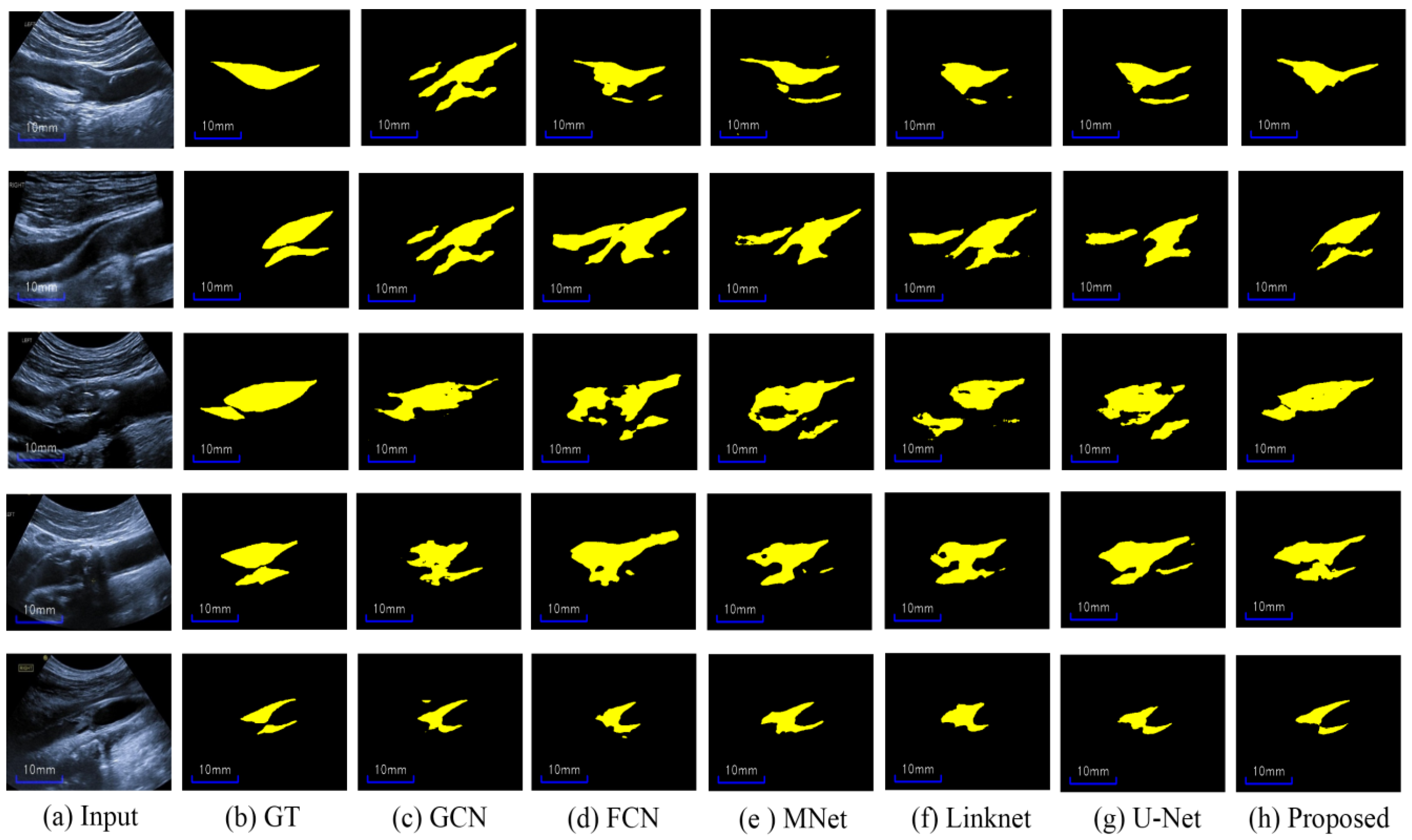
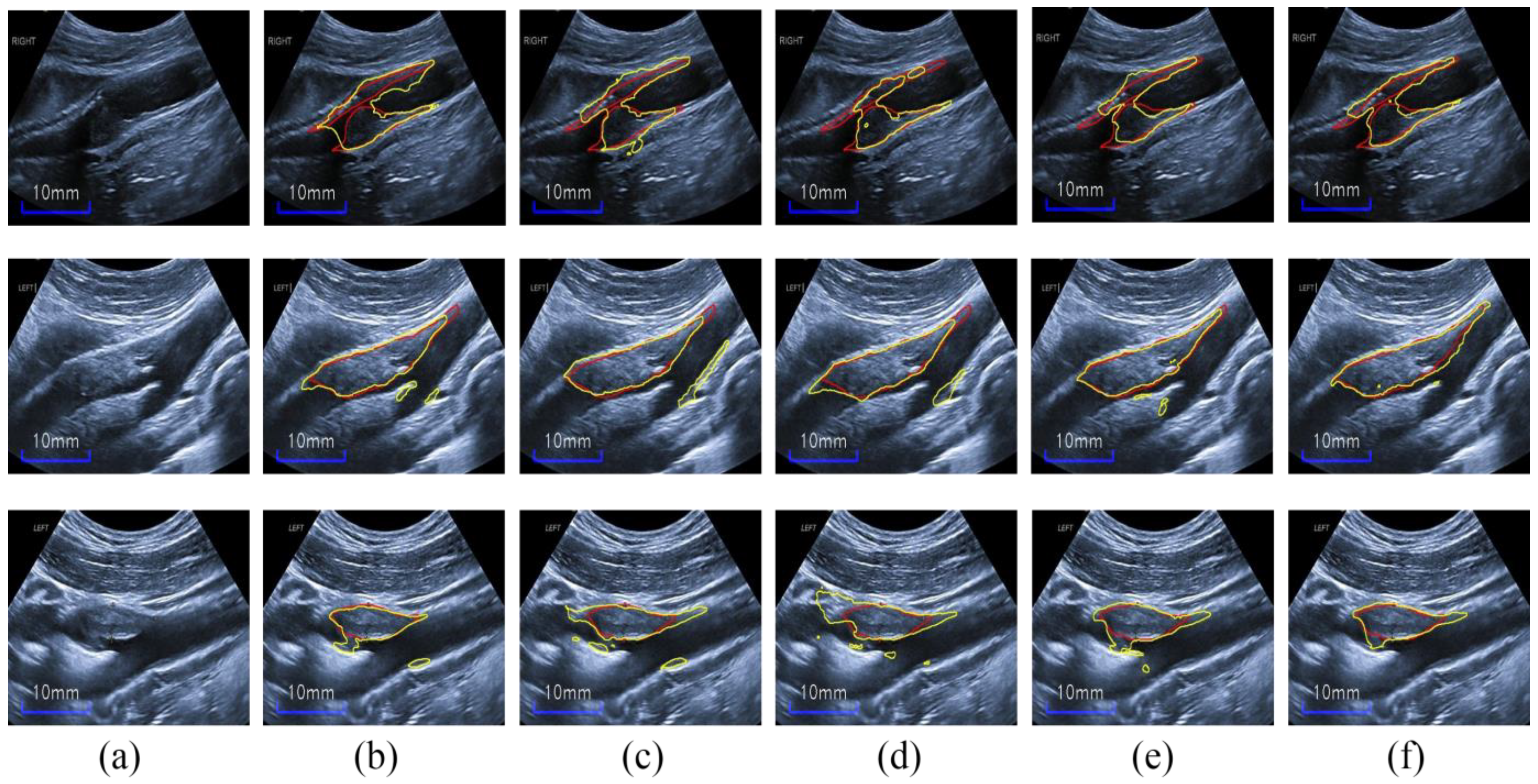
4.1. Compared with State-of-the-Art Methods
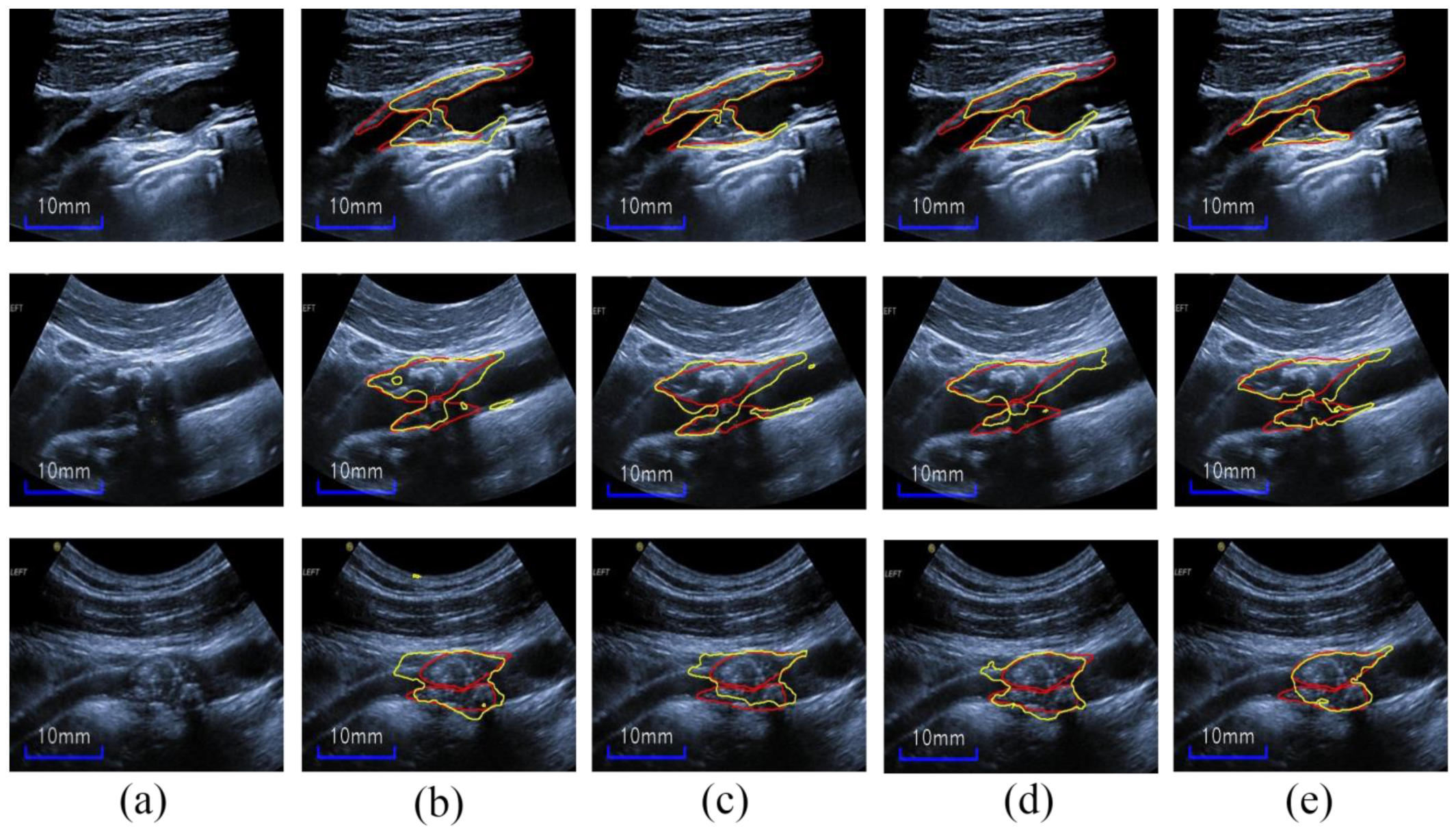
4.2. Ablation Study
4.2.1. Effect of Each Module
4.2.2. Effect of the Number of HAC Modules
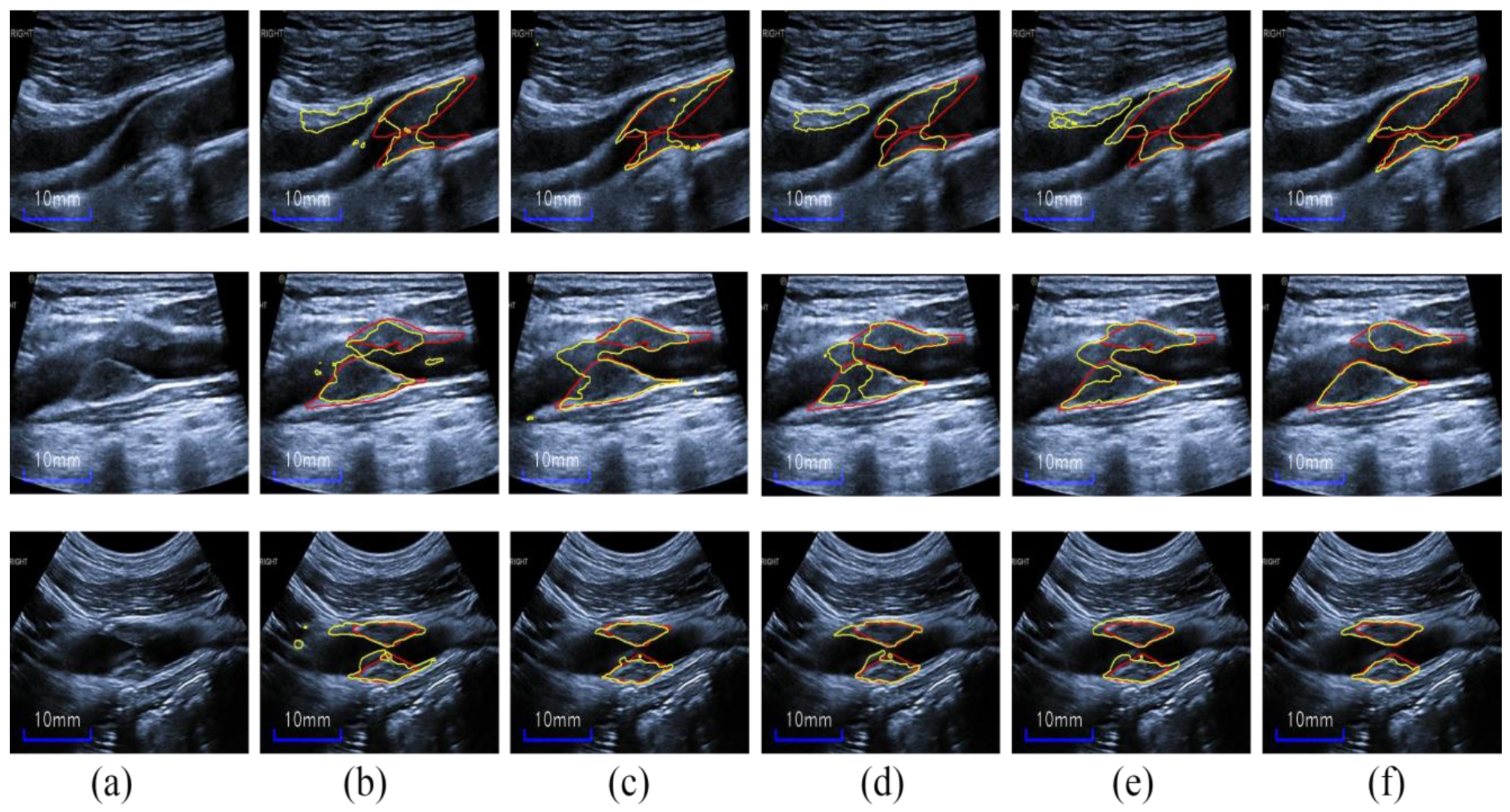
4.3. Test Results on New Images
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qian, C.; Yang, X. An Integrated Method for Atherosclerotic Carotid Plaque Segmentation In Ultrasound Image. Comput. Meth. Programs Biomed. 2017, 153, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Zarins, C.K.; Xu, C.; Glagov, S. Atherosclerotic enlargement of the human abdominal aorta. Atherosclerosis 2001, 155, 157–164. [Google Scholar] [CrossRef]
- Bogiatzi, C.; Hackam, D.G.; McLeod, A.I.; Spence, J.D. Secular trends in ischemic stroke subtypes and stroke risk factors. Stroke 2014, 45, 3208–3213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spence, J.D. Measurement of Carotid Plaque Burden. JAMA Neurol. 2015, 72, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Molinari, F.; Zeng, G.; Suri, J.S. A state of the art review on intima media thickness (IMT) measurement and wall segmentation techniques for carotid ultrasound. Comput. Meth. Programs Biomed. 2010, 100, 201–221. [Google Scholar] [CrossRef]
- Spence, J.D. Carotid ultrasound phenotypes are biologically distinct. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1910–1913. [Google Scholar] [CrossRef] [Green Version]
- Nicolaides, A.; Sabetai, M.; Kakkos, S.K.; Dhanjil, S.; Tegos, T.; Stevens, J.M. The asymptomatic carotid stenosis and risk of stroke study. Int. Angiol. 2003, 22, 263–272. [Google Scholar]
- Warlow, C. Endarterectomy for asymptomatic carotid stenosis? Lancet 1995, 345, 1254–1255. [Google Scholar] [CrossRef]
- Gao, P.; Chen, Z.-Q.; Bao, Y.-H.; Jia, L.-Q.; Lin, F. Correlation between carotid intraplaque hemorrhage and clinical symptoms: Systematic review of observational studies. Stroke 2007, 38, 2382–2390. [Google Scholar] [CrossRef] [Green Version]
- Crişan, S. Carotid ultrasound. Med. Ultrason. 2011, 13, 326–330. [Google Scholar]
- Menchón-Lara, R.-M.; Bastida-Jumilla, M.-C.; Morales-Sánchez, J.; Sancho-Gómez, J.-L. Automatic detection of the intima-media thickness in ultrasound images of the common carotid artery using neural networks. Med. Biol. Eng. Comput. 2014, 52, 169–181. [Google Scholar] [CrossRef]
- Scherl, H.; Hornegger, J.; Prummer, M.; Lell, M. Semi-automatic level-set based segmentation and stenosis quantification of the internal carotid artery in 3d cta data sets. Med. Image Anal. 2007, 11, 21–34. [Google Scholar] [CrossRef]
- Cardinal, M.-H.R.; Meunier, J.; Soulez, G.; Therasse, E.; Cloutier, G. Intravascular ultrasound image segmentation: A fast-marching method. In Proceedings of the 6th International Conference on Medical Image Computing and Computer-Assisted Intervention—MICCAI 2003, Montréal, QC, Canada, 15–18 November 2003; pp. 432–439. [Google Scholar]
- Smitha, B.; Joseph, K.P. A New Approach for Classification of Atherosclerosis of Common Carotid Artery from Ultrasound Images. J. Mech. Med. Biol. 2019, 19, 1940001–1940018. [Google Scholar] [CrossRef]
- Loizou, C.P.; Petroudi, S.; Pattichis, C.S.; Pantziaris, M.; Kasparis, T.; Nicolaides, A. Segmentation of atherosclerotic carotid plaque in ultrasound video. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 53–56. [Google Scholar] [CrossRef]
- Bonanno, L.; Sottile, F.; Ciurleo, R.; Lorenzo, G.D.; Bruschetta, D.; Bramanti, A.; Ascenti, G.; Bramanti, P.; Marino, S. Automatic Algorithm for Segmentation of Atherosclerotic Carotid Plaque. J. Stroke Cerebrovasc. Dis. 2017, 26, 411–416. [Google Scholar] [CrossRef]
- Shelhamer, E.; Long, J.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2015, 39, 640–651. [Google Scholar] [CrossRef]
- Xu, L.; Liu, M.; Shen, Z.; Wang, H.; Liu, X.; Wang, X.; Wang, S.; Li, T.; Yu, S.; Hou, M.; et al. DW-Net: A cascaded convolutional neural network for apical four-chamber view segmentation in fetal echocardiography. Comput. Med. Imaging Graph. 2020, 80, 101690. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Zhou, R.; Guo, F.; Azarpazhooh, M.R.; Hashemi, S.; Cheng, X.; Spence, J.D.; Ding, M.; Fenster, A. Deep Learning-Based Measurement of Total Plaque Area in B-Mode Ultrasound Images. IEEE J. Biomed. Health Inform. 2021, 25, 2967–2977. [Google Scholar] [CrossRef]
- Jain, P.K.; Sharma, N.; Giannopoulos, A.A.; Saba, L.; Nicolaides, A.; Suri, J.S. Hybrid deep learning segmentation models for atherosclerotic plaque in internal carotid artery B-mode ultrasound. Comput. Biol. Med. 2021, 136, 104721. [Google Scholar] [CrossRef]
- Vila, M.d.M.; Remeseiro, B.; Grau, M.; Elosua, R.; Betriu, À.; Fernandez-Giraldez, E.; Igual, L. Semantic Segmentation with DenseNets for Carotid Artery Ultrasound Plaque Segmentation and CIMT estimation. Artif. Intell. Med. 2020, 103, 101784. [Google Scholar] [CrossRef]
- Zhou, R.; Fenster, A.; Xia, Y.; Spence, J.D.; Ding, M. Deep Learning based Carotid Media-Adventitia and Lumen-intima Boundary Segmentation from Three-dimensional Ultrasound Images. Med. Phys. 2019, 46, 3180–3193. [Google Scholar] [CrossRef] [Green Version]
- Zhou, R.; Guo, F.; Azarpazhooh, M.R.; Spence, J.D.; Ukwatta, E.; Ding, M.; Fenster, A. A Voxel-based Fully Convolution Network and Continuous Max-flow for Carotid Vessel-wall-volume Segmentation from 3D Ultrasound Images. IEEE Trans. Med. Imaging 2020, 39, 2844–2855. [Google Scholar] [CrossRef] [PubMed]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional Neural Networks for Medical Image Analysis: Full Training or Fine Tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizpou, H.; Razavian, A.S.; Sullivan, J.; Maki, A.; Carlsson, S. From generic to specific deep representations for visual recognition. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Boston, MA, USA, 7–12 June 2015; pp. 36–45. [Google Scholar]
- Penatti, O.A.B.; Nogueira, K.; Santos, J.A.d. Do deep features generalize from everyday objects to remote sensing and aerial scenes domains? In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Boston, MA, USA, 7–12 June 2015; pp. 44–51. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; Volume 1, pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Chen, P.; Yuan, Y.; Liu, D.; Huang, Z.; Hou, X.; Cottrell, G. Understanding Convolution for Semantic Segmentation. In Proceedings of the 2018 IEEE Winter Conference on Applications of Computer Vision (WACV), Lake Tahoe, NV, USA, 12–15 March 2018; pp. 1451–1460. [Google Scholar]
- Yu, F.; Koltun, V. Multi-scale context aggregation by dilated convolutions. In Proceedings of the ICLR 2016, San Juan, Puerto Rico, 2–4 May 2016. [Google Scholar]
- Yu, F.; Koltun, V.; Funkhouser, T. Dilated Residual Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 636–644. [Google Scholar]
- Chen, L.-C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking Atrous Convolution for Semantic Image Segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, University of Maryland, College Park, MD, USA, 25–26 February 2017. [Google Scholar]
- Zhuang, Z.; Li, N.; Raj, A.N.J.; Mahesh, V.G.V.; Qiu, S. An RDAU-NET model for lesion segmentation in breast ultrasound images. PLoS ONE 2019, 14, e0221535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Faraji, M.; Basu, A. Robust segmentation of arterial walls in intravascular ultrasound images using Dual Path U-Net. Ultrasonics 2019, 96, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Li, C.; Xu, L.; Zhu, S.; Hua, Y.; Zhang, J. CSM-Net: Automatic joint segmentation of intima-media complex and lumen in carotid artery ultrasound images. Comput. Biol. Med. 2022, 150, 106119. [Google Scholar] [CrossRef]
- Zhou, R.; Azarpazhooh, M.R.; Spence, J.D.; Hashemi, S.; Ma, W.; Cheng, X.; Gan, H.; Ding, M.; Fenster, A. Deep Learning-Based Carotid Plaque Segmentation from B-Mode Ultrasound Images. Ultrasound Med. Biol. 2021, 47, 2723–2733. [Google Scholar] [CrossRef]
- Jain, P.K.; Sharma, N.; Saba, L.; Paraskevas, K.I.; Kalra, M.K.; Johri, A.; Laird, J.R.; Nicolaides, A.N.; Suri, J.S. Unseen Artificial Intelligence—Deep Learning Paradigm for Segmentation of Low Atherosclerotic Plaque in Carotid Ultrasound: A Multicenter Cardiovascular Study. Diagnostics 2021, 11, 2257. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Girshick, R.; Gupta, A.; He, K. Non-local Neural Networks. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 7794–7803. [Google Scholar]
- Chen, Y.; Song, G.; Jiao, L.; Wang, Y.; Ma, Y.; Ling, F. A study of carotid endarterectomy in a Chinese population: Initial experience at a single center. Clin. Neurol. Neurosurg. 2014, 126, 88–92. [Google Scholar] [CrossRef]
- Naghavi, M.; Libby, P.; Falk, E.; Casscells, S.W.; Litovsky, S. From vulnerable plaque to vulnerable patient: A call for new definitions and risk assessment strategies: Part I. Circulation 2003, 108, 1664–1672. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Dubuisson, M.-P.; Jain, A.K. A modified Hausdorff distance for object matching. In Proceedings of the 12th International Conference on Pattern Recognition, Jerusalem, Israel, 9–13 October 1994; pp. 566–568. [Google Scholar]
- Peng, C.; Zhang, X.; Yu, G.; Luo, G.; Sun, J. Large Kernel Matters—Improve Semantic Segmentation by Global Convolutional Network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1743–1751. [Google Scholar]
- Chaurasia, A.; Culurciello, E. LinkNet: Exploiting encoder representations for efficient semantic segmentation. In Proceedings of the 2017 IEEE Visual Communications and Image Processing (VCIP), St. Petersburg, FL, USA, 10–13 December 2017; pp. 1–4. [Google Scholar]
- Oktay, O.; Schlemper, J.; Folgoc, L.L.; Lee, M.; Heinrich, M.; Misawa, K.; Mori, K.; McDonagh, S.; Hammerla, N.Y.; Kainz, B.; et al. Attention U-Net: Learning Where to Look for the Pancreas. In Proceedings of the 1st Conference on Medical Imaging with Deep Learning, Amsterdam, The Netherlands, 4–6 July 2018. [Google Scholar]
- Fu, H.; Cheng, J.; Xu, Y.; Wong, D.W.K.; Liu, J.; Cao, X. Joint Optic Disc and Cup Segmentation Based on Multi-label Deep Network and Polar Transformation. IEEE Trans. Med. Imaging 2018, 37, 1597–1605. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Zhang, P.; Shao, J.; Cheng, Y.; Zhang, Y.; Bai, J. A snake-based method for segmentation of intravascular ultrasound images and its in vivo validation. Ultrasonics 2011, 51, 181–189. [Google Scholar] [CrossRef]
- Chen, L.-C.; Papandreou, G.; Kokkinos, I.; Murphy, K.; Yuille, A.L. DeepLab: Semantic Image Segmentation with Deep Convolutional Nets, Atrous Convolution, and Fully Connected CRFs. IEEE Trans. Pattern Anal. Mach. Intell. 2016, 40, 834–848. [Google Scholar] [CrossRef] [Green Version]
- Alsheikh-Ali, A.A.; Kitsios, G.D.; Balk, E.M.; Lau, J.; Ip, S. The vulnerable atherosclerotic plaque: Scope of the literature. Ann. Intern. Med. 2010, 153, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Acharya, R.U.; Faust, O.; Alvin, A.P.C.; Sree, S.V.; Molinari, F.; Saba, L.; Nicolaides, A.; Suri, J.S. Symptomatic vs. Asymptomatic Plaque Classification in Carotid Ultrasound. J. Med. Syst. 2011, 36, 1861–1871. [Google Scholar] [CrossRef]
- Acharya, U.R.; Sree, S.V.; Krishnan, M.M.R.; Molinari, F.; Saba, L.; Ho, S.Y.S.; Ahuja, A.T.; Ho, S.C.; Nicolaides, A.; Suri, J.S. Atherosclerotic Risk Stratification Strategy for Carotid Arteries Using Texture-Based Features. Ultrasound Med. Biol. 2012, 38, 899–915. [Google Scholar] [CrossRef]
- Roy-Cardinal, M.-H.; Destrempes, F.; Soulez, G.; Cloutier, G. Assessment of Carotid Artery Plaque Components with Machine Learning Classification Using Homodyned-K Parametric Maps and Elastograms. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 493–504. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Name | Block | Output Size | Original Output Channels | Reduced Output Channels |
|---|---|---|---|---|
| CONV-Block | 7 × 7, 64, stride 2 | H/2 × W/2 | 64 | 32 |
| Res1 | H/4 × W/4 | 256 | 64 | |
| Res2 | H/8 × W/8 | 512 | 96 | |
| Res3 | H/16 × W/16 | 1024 | 128 | |
| Res4 | H/32 × W/32 | 2048 | 128 |
| Methods | Dice | IoU | Acc | MHD |
|---|---|---|---|---|
| Proposed | 0.821 ± 0.053 | 0.701 ± 0.078 | 0.977 ± 0.008 | 1.69 ± 1.46 |
| U-Net [19] | 0.765 ± 0.069 | 0.625 ± 0.091 | 0.969 ± 0.013 | 3.19 ± 2.62 |
| FCN [17] | 0.747 ± 0.073 | 0.601 ± 0.089 | 0.965 ± 0.015 | 4.01 ± 3.59 |
| Attention U-Net [46] | 0.763 ± 0.083 | 0.624 ± 0.105 | 0.968 ± 0.016 | 3.35 ± 3.52 |
| DeepLabv3 [32] | 0.767 ± 0.075 | 0.629 ± 0.098 | 0.969 ± 0.014 | 2.57 ± 1.79 |
| M-Net [47] | 0.769 ± 0.084 | 0.633 ± 0.108 | 0.968 ± 0.013 | 3.07 ± 2.70 |
| GCN [44] | 0.751 ± 0.095 | 0.610 ± 0.112 | 0.965 ± 0.021 | 3.41 ± 3.91 |
| LinkNet [45] | 0.762 ± 0.082 | 0.622 ± 0.105 | 0.967 ± 0.014 | 2.99 ± 2.65 |
| Jain et al., 2021 [21] | 0.889 ± 0.01 | NA | NA | NA |
| Zhou et al., 2021 [20] | 0.833–0.857 | NA | NA | NA |
| Jain et al., 2021 [37] | 0.784/0.825 | NA | 0.986/0.987 | NA |
| U-Net | FCN | Attention U-Net | DeepLabv3 | M-Net | GCN | LinkNet | |
|---|---|---|---|---|---|---|---|
| Dice p-value | 2.36 × 10−6 | 8.97 × 10−7 | 0.000107 | 3.31× 10−5 | 0.000403 | 0.00027 | 7.93 × 10−5 |
| MHD p-value | 0.0099 | 0.00246 | 0.00246 | 0.03335 | 0.014517 | 0.04184 | 0.03561 |
| GIA 1 | CBV 2 | T 3 | HAC | Dice | IoU | Acc | MHD |
|---|---|---|---|---|---|---|---|
| ✓ | 0.742 ± 0.069 | 0.594 ± 0.085 | 0.965 ± 0.011 | 3.53 ± 2.81 | |||
| ✓ | ✓ | 0.751 ± 0.088 | 0.609 ± 0.111 | 0.967 ± 0.013 | 3.13 ± 2.65 | ||
| ✓ | ✓ | ✓ | 0.804 ± 0.061 | 0.676 ± 0.086 | 0.974 ± 0.011 | 2.13 ± 1.53 | |
| ✓ | ✓ | ✓ | 0.806 ± 0.056 | 0.679 ± 0.081 | 0.975 ± 0.010 | 2.06 ± 1.52 | |
| ✓ | ✓ | ✓ | ✓ | 0.821 ± 0.053 | 0.701 ± 0.078 | 0.977 ± 0.008 | 1.69 ± 1.46 |
| Methods | p-Value of Dice | p-Value of MHD |
|---|---|---|
| RU-CBV vs. RU-CBV-T | 0.002 | 0.047 |
| RU-CBV vs. proposed | 2.78 × 10−5 | 0.012 |
| RU-CBV-T vs. proposed | 0.042 | 0.374 |
| HRU-T vs. proposed | 0.035 | 0.12 |
| HACs | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Dice | 0.812 | 0.815 | 0.821 | 0.818 | 0.814 | 0.808 |
| Authors | Methods | Data | Metrics | Results |
|---|---|---|---|---|
| Jain et al., 2021 [21] | SDL/HDL models | 97 patients/970 images | Jaccard, Dice, FoM, ΔPA | 80.44 ± 1.59, 88.98 ± 1.04, 99.00 ± 1.10, best 3.49 mm2 using UNet with CE-loss |
| Zhou et al., 2021 [20] | UNet++ ensemble | 144 patients/510 plaques | Dice, ΔPA, ICC, CoV | 83.3–85.7, 0.73–6.75 mm2, 0.996, 6.98 |
| Jain et al., 2021 [37] | UNet | 165 Japanese patients/330 images 50 Hong Kong patients/300 images | mean accuracy, Dice, correlation-coefficient | Unseen AI pair one: 98.55, 0.784 and 0.80 Unseen AI pair two: 98.67, 0.825, and 0.87 Seen AI: 99.01, 0.869 and 0.92 |
| Zhou et al., 2021 [36] | Two UNet | 144 patients/510 plaques | ΔTPA, Pearson correlation | 0.05 ± 7.13 mm2, 0.8 ± 8.7 mm2 0.989, 0.987 |
| Proposed | HRU-NET | 90 patients/115 images | Dice, IOU, Acc, MHD, ΔTPA | 0.811, 0.689, 0.982, 2.06, 0.5 ± 7.59 mm2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, Y.; Li, C.; Zhang, K.; Hua, Y.; Zhang, J. HRU-Net: A Transfer Learning Method for Carotid Artery Plaque Segmentation in Ultrasound Images. Diagnostics 2022, 12, 2852. https://doi.org/10.3390/diagnostics12112852
Yuan Y, Li C, Zhang K, Hua Y, Zhang J. HRU-Net: A Transfer Learning Method for Carotid Artery Plaque Segmentation in Ultrasound Images. Diagnostics. 2022; 12(11):2852. https://doi.org/10.3390/diagnostics12112852
Chicago/Turabian StyleYuan, Yanchao, Cancheng Li, Ke Zhang, Yang Hua, and Jicong Zhang. 2022. "HRU-Net: A Transfer Learning Method for Carotid Artery Plaque Segmentation in Ultrasound Images" Diagnostics 12, no. 11: 2852. https://doi.org/10.3390/diagnostics12112852