

High Plasma Levels of Activated Factor VII-Antithrombin Complex Point to Increased Tissue Factor Expression in Patients with SARS-CoV-2 Pneumonia: A Potential Link with COVID-19 Prothrombotic Diathesis
 ,
,  , , , , , , ,
, , , , , , ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
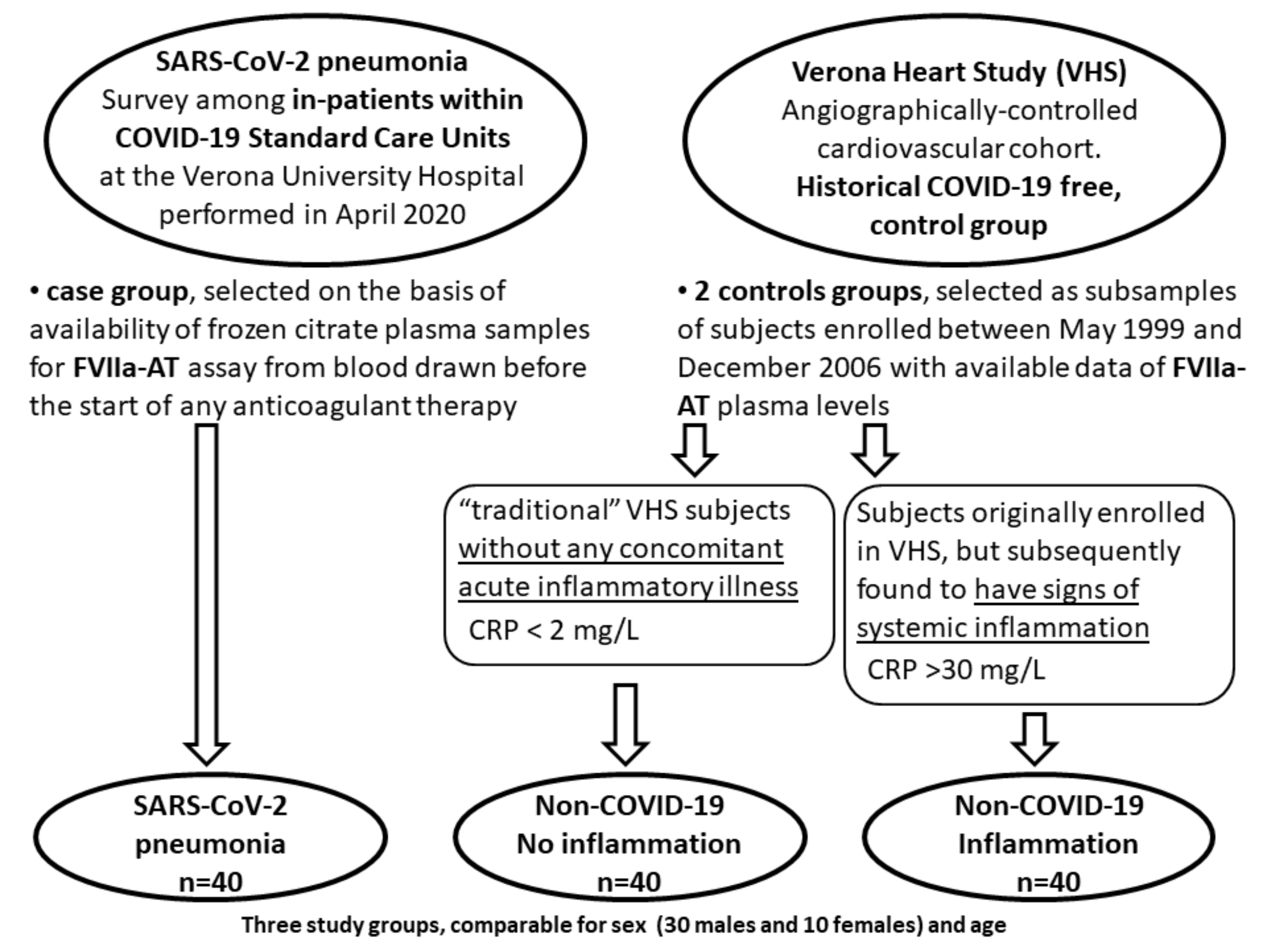
2.1. Study Populations
2.2. Biochemical Analysis, FVIIa-AT and Coagulation Assays
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center, COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 30 August 2022).
- Osuchowski, M.F.; Winkler, M.S.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, F.M.; et al. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. COVID-19: Unravelling the clinical progression of nature’s virtually perfect biological weapon. Ann. Transl. Med. 2020, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Muller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef]
- Hippensteel, J.A.; Burnham, E.L.; Jolley, S.E. Prevalence of venous thromboembolism in critically ill patients with COVID-19. Br. J. Haematol. 2020, 190, e134–e137. [Google Scholar] [CrossRef]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Pizzolo, F.; Rigoni, A.M.; De Marchi, S.; Friso, S.; Tinazzi, E.; Sartori, G.; Stefanoni, F.; Nalin, F.; Montagnana, M.; Pilotto, S.; et al. Deep vein thrombosis in SARS-CoV-2 pneumonia-affected patients within standard care units: Exploring a submerged portion of the iceberg. Thromb. Res. 2020, 194, 216–219. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Wang, F.; Hou, H.; Luo, Y.; Tang, G.; Wu, S.; Huang, M.; Liu, W.; Zhu, Y.; Lin, Q.; Mao, L.; et al. The laboratory tests and host immunity of COVID-19 patients with different severity of illness. JCI Insight 2020, 5, e137799. [Google Scholar] [CrossRef] [Green Version]
- Seth, R.; McKinnon, T.A.J.; Zhang, X.F. Contribution of the von Willebrand factor/ADAMTS13 imbalance to COVID-19 coagulopathy. Am. J. Physiol. Heart Circ. Physiol. 2022, 322, H87–H93. [Google Scholar] [CrossRef]
- Spiezia, L.; Boscolo, A.; Poletto, F.; Cerruti, L.; Tiberio, I.; Campello, E.; Navalesi, P.; Simioni, P. COVID-19-Related Severe Hypercoagulability in Patients Admitted to Intensive Care Unit for Acute Respiratory Failure. Thromb. Haemost 2020, 120, 998–1000. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Martinelli, N.; Montagnana, M.; Pizzolo, F.; Friso, S.; Salvagno, G.L.; Forni, G.L.; Gianesin, B.; Morandi, M.; Lunardi, C.; Lippi, G.; et al. A relative ADAMTS13 deficiency supports the presence of a secondary microangiopathy in COVID-19. Thromb. Res. 2020, 193, 170–172. [Google Scholar] [CrossRef]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef]
- Tiwari, N.R.; Phatak, S.; Sharma, V.R.; Agarwal, S.K. COVID-19 and thrombotic microangiopathies. Thromb. Res. 2021, 202, 191–198. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchie, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Rovas, A.; Osiaevi, I.; Buscher, K.; Sackarnd, J.; Tepasse, P.R.; Fobker, M.; Kuhn, J.; Braune, S.; Gobel, U.; Tholking, G.; et al. Microvascular dysfunction in COVID-19: The MYSTIC study. Angiogenesis 2021, 24, 145–157. [Google Scholar] [CrossRef]
- Liu, F.; Han, K.; Blair, R.; Kenst, K.; Qin, Z.; Upcin, B.; Worsdorfer, P.; Midkiff, C.C.; Mudd, J.; Belyaeva, E.; et al. SARS-CoV-2 Infects Endothelial Cells In Vivo and In Vitro. Front. Cell Infect. Microbiol. 2021, 11, 701278. [Google Scholar] [CrossRef] [PubMed]
- Jose, R.J.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Resp. Med. 2020, 8, E46–E47. [Google Scholar] [CrossRef]
- Savla, S.R.; Prabhavalkar, K.S.; Bhatt, L.K. Cytokine storm associated coagulation complications in COVID-19 patients: Pathogenesis and Management. Expert Rev. Anti Infect. Ther. 2021, 19, 1397–1413. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, N.; Girelli, D.; Baroni, M.; Guarini, P.; Sandri, M.; Lunghi, B.; Tosi, F.; Branchini, A.; Sartori, F.; Woodhams, B.; et al. Activated factor VII-antithrombin complex predicts mortality in patients with stable coronary artery disease: A cohort study. J. Thromb. Haemost 2016, 14, 655–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, N.; Baroni, M.; Castagna, A.; Lunghi, B.; Stefanoni, F.; Tosi, F.; Croce, J.; Udali, S.; Woodhams, B.; Girelli, D.; et al. Apolipoprotein C-III Strongly Correlates with Activated Factor VII-Anti-Thrombin Complex: An Additional Link between Plasma Lipids and Coagulation. Thromb. Haemost 2019, 119, 192–202. [Google Scholar] [CrossRef]
- Olson, N.C.; Raffield, L.M.; Lange, L.A.; Lange, E.M.; Longstreth, W.T., Jr.; Chauhan, G.; Debette, S.; Seshadri, S.; Reiner, A.P.; Tracy, R.P. Associations of activated coagulation factor VII and factor VIIa-antithrombin levels with genome-wide polymorphisms and cardiovascular disease risk. J. Thromb. Haemost 2018, 16, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Yau, J.W.; Teoh, H.; Verma, S. Endothelial cell control of thrombosis. BMC Cardiovasc. Disord. 2015, 15, 130. [Google Scholar] [CrossRef] [Green Version]
- Olivieri, O.; Turcato, G.; Cappellari, M.; Stefanoni, F.; Osti, N.; Pizzolo, F.; Friso, S.; Bassi, A.; Castagna, A.; Martinelli, N. High Plasma Concentration of Apolipoprotein C-III Confers an Increased Risk of Cerebral Ischemic Events on Cardiovascular Patients Anticoagulated With Warfarin. Front. Cardiovasc. Med. 2021, 8, 781383. [Google Scholar] [CrossRef]
- Martinelli, N.; Girelli, D.; Lunghi, B.; Pinotti, M.; Marchetti, G.; Malerba, G.; Pignatti, P.F.; Corrocher, R.; Olivieri, O.; Bernardi, F. Polymorphisms at LDLR locus may be associated with coronary artery disease through modulation of coagulation factor VIII activity and independently from lipid profile. Blood 2010, 116, 5688–5697. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Naymagon, L.; Zubizarreta, N.; Feld, J.; van Gerwen, M.; Alsen, M.; Thibaud, S.; Kessler, A.; Venugopal, S.; Makki, I.; Qin, Q.; et al. Admission D-dimer levels, D-dimer trends, and outcomes in COVID-19. Thromb. Res. 2020, 196, 99–105. [Google Scholar] [CrossRef]
- Sheth, A.; Modi, M.; Dawson, D.; Dominic, P. Prognostic value of cardiac biomarkers in COVID-19 infection. Sci. Rep. 2021, 11, 4930. [Google Scholar] [CrossRef]
- Zhan, H.T.; Chen, H.Z.; Liu, C.X.; Cheng, L.L.; Yan, S.X.; Li, H.L.; Li, Y.Z. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hem. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Francischetti, I.M.B.; Toomer, K.; Zhang, Y.; Jani, J.; Siddiqui, Z.; Brotman, D.J.; Hooper, J.E.; Kickler, T.S. Upregulation of pulmonary tissue factor, loss of thrombomodulin and immunothrombosis in SARS-CoV-2 infection. EClinicalMedicine 2021, 39, 101069. [Google Scholar] [CrossRef]
- Willems, L.H.; Nagy, M.; Ten Cate, H.; Spronk, H.M.H.; Groh, L.A.; Leentjens, J.; Janssen, N.A.F.; Netea, M.G.; Thijssen, D.H.J.; Hannink, G.; et al. Sustained inflammation, coagulation activation and elevated endothelin-1 levels without macrovascular dysfunction at 3 months after COVID-19. Thromb. Res. 2022, 209, 106–114. [Google Scholar] [CrossRef]
- Steffel, J.; Luscher, T.F.; Tanner, F.C. Tissue factor in cardiovascular diseases: Molecular mechanisms and clinical implications. Circulation 2006, 113, 722–731. [Google Scholar] [CrossRef] [Green Version]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Gupta, A.; Jimenez, D.; Burton, J.R.; Der Nigoghossian, C.; Chuich, T.; Nouri, S.N.; Dreyfus, I.; Driggin, E.; et al. Pharmacological Agents Targeting Thromboinflammation in COVID-19: Review and Implications for Future Research. Thromb. Haemost 2020, 120, 1004–1024. [Google Scholar] [CrossRef]
- Van Gorp, E.C.; Suharti, C.; ten Cate, H.; Dolmans, W.M.; van der Meer, J.W.; ten Cate, J.W.; Brandjes, D.P. Review: Infectious diseases and coagulation disorders. J. Infect. Dis. 1999, 180, 176–186. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef]
- Losche, W. Platelets and tissue factor. Platelets 2005, 16, 313–319. [Google Scholar] [CrossRef]
- Shibamiya, A.; Hersemeyer, K.; Schmidt Woll, T.; Sedding, D.; Daniel, J.M.; Bauer, S.; Koyama, T.; Preissner, K.T.; Kanse, S.M. A key role for Toll-like receptor-3 in disrupting the hemostasis balance on endothelial cells. Blood 2009, 113, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Canas, C.A.; Canas, F.; Bautista-Vargas, M.; Bonilla-Abadia, F. Role of Tissue Factor in the Pathogenesis of COVID-19 and the Possible Ways to Inhibit It. Clin. Appl. Thromb. Hemost 2021, 27, 10760296211003983. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Levi, M.; Hunt, B.J. Prevention and management of thrombosis in hospitalised patients with COVID-19 pneumonia. Lancet Respir. Med. 2022, 10, 214–220. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-COVID-19 No Inflammation (n = 40) | Non-COVID-19 Inflammation (n = 40) | SARS-CoV-2 Pneumonia (n = 40) | p * | |
|---|---|---|---|---|
| Female sex (%) | 25.0 | 25.0 | 25.0 | NS |
| Age (years) | 60.6 ± 11.5 | 60.9 ± 12.1 | 64.8 ± 12.3 | NS |
| BMI (kg/m2) | 26.5 ± 3.5 | 27.0 ± 3.9 | 26.8 ± 4.4 | NS |
| CRP (mg/L) | 0.9 (0.7–1.2) | 51.6 (44.0–60.4) | 71.5 (54.4–93.8) | <0.001 |
| eGFR (mL/min) # | 73.9 (67.9–80.4) | 71.8 (60.9–80.6) | 70.8 (63.6–78.8) | NS |
| PT | 0.98 (0.97–1.00) | 0.97 (0.95–1.00) | 1.10 (1.07–1.14) | <0.001 |
| aPTT | 0.97 (0.94–1.01) | 1.03 (0.98–1.08) | 1.01 (0.97–1.06) | NS |
| Fibrinogen (g/L) | 3.16 (2.95–3.37) | 5.33 (4.67–6.07) | 6.19 (5.48–7.00) | <0.001 |
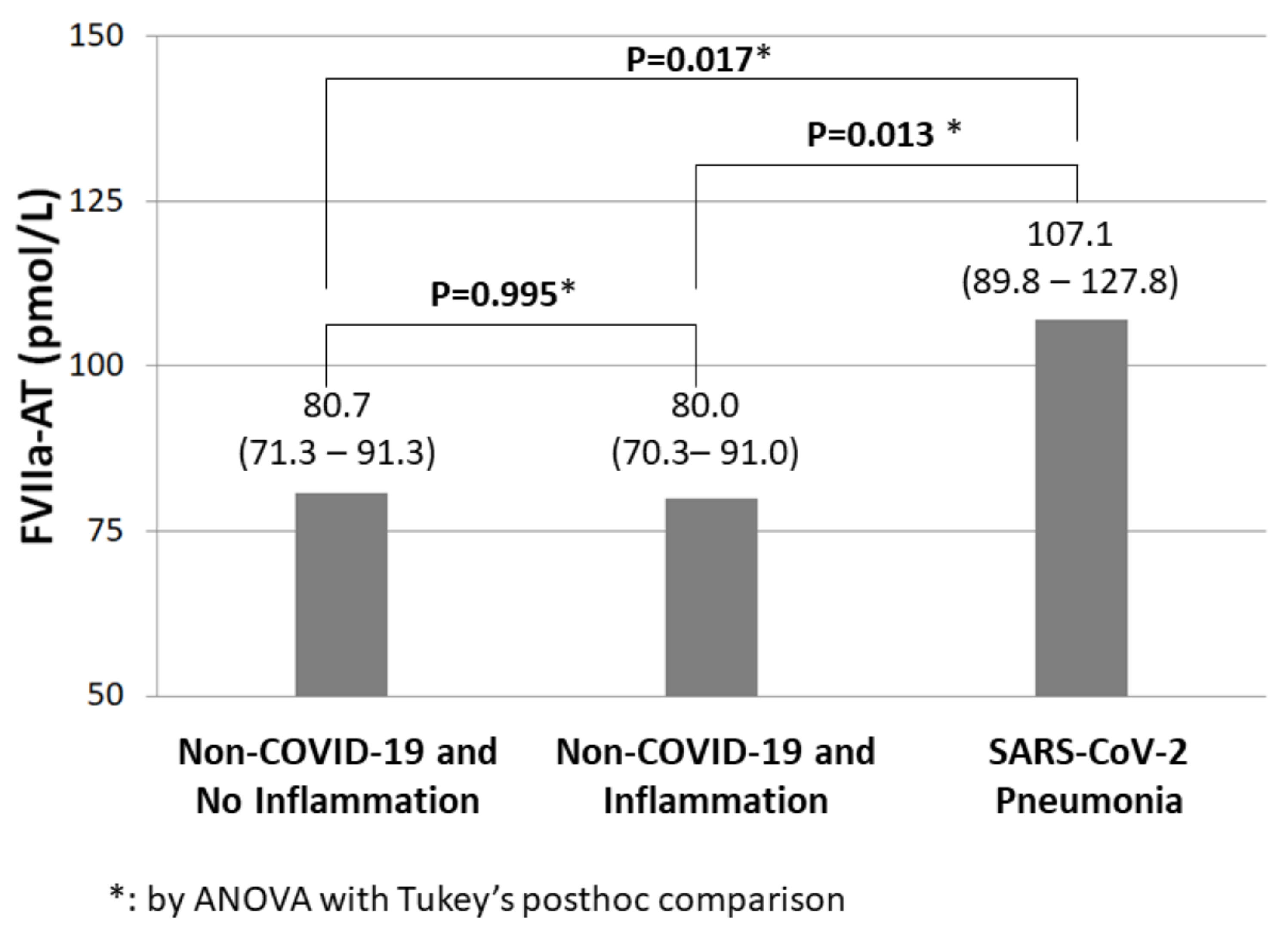
| FVIIa-AT (pmol/L) | 80.7 (71.3–91.3) | 80.0 (70.3–91.0) | 107.1 (89.8–127.8) | 0.006 |
| FII:c ^ | 120.0 ± 24.5 | 118.4 ± 24.2 | 82.9 ± 19.7 | <0.001 |
| FV:c ^ | 140.7 ± 52.2 | 142.2 ± 25.3 | 99.8 ± 23.3 | <0.001 |
| FVIII:c ^ | 148.9 ± 60.7 | 200.9 ± 66.6 | 65.2 ± 21.9 | <0.001 |
| SARS-CoV-2 Pneumonia as Determinant of FVIIa-AT Levels by Linear Regression Models | Beta Coefficient | 95% CI | p | |
|---|---|---|---|---|
| Unadjusted | 0.288 | 0.114–0.461 | 0.001 | |
| Adjusted | Model 1 | 0.276 | 0.100–0.452 | 0.002 |
| Model 2 | 0.265 | 0.056–0.474 | 0.014 | |
| Model 3 | 0.264 | 0.055–0.473 | 0.014 | |
| Model 4 | 0.322 | 0.055–0.589 | 0.019 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinelli, N.; Rigoni, A.M.; De Marchi, S.; Osti, N.; Donini, M.; Montagnana, M.; Castagna, A.; Pattini, P.; Udali, S.; De Franceschi, L.; et al. High Plasma Levels of Activated Factor VII-Antithrombin Complex Point to Increased Tissue Factor Expression in Patients with SARS-CoV-2 Pneumonia: A Potential Link with COVID-19 Prothrombotic Diathesis. Diagnostics 2022, 12, 2792. https://doi.org/10.3390/diagnostics12112792
Martinelli N, Rigoni AM, De Marchi S, Osti N, Donini M, Montagnana M, Castagna A, Pattini P, Udali S, De Franceschi L, et al. High Plasma Levels of Activated Factor VII-Antithrombin Complex Point to Increased Tissue Factor Expression in Patients with SARS-CoV-2 Pneumonia: A Potential Link with COVID-19 Prothrombotic Diathesis. Diagnostics. 2022; 12(11):2792. https://doi.org/10.3390/diagnostics12112792
Chicago/Turabian StyleMartinelli, Nicola, Anna Maria Rigoni, Sergio De Marchi, Nicola Osti, Martino Donini, Martina Montagnana, Annalisa Castagna, Patrizia Pattini, Silvia Udali, Lucia De Franceschi, and et al. 2022. "High Plasma Levels of Activated Factor VII-Antithrombin Complex Point to Increased Tissue Factor Expression in Patients with SARS-CoV-2 Pneumonia: A Potential Link with COVID-19 Prothrombotic Diathesis" Diagnostics 12, no. 11: 2792. https://doi.org/10.3390/diagnostics12112792