
Common, Less Common, and Unexpected Complications after Bariatric Surgery: A Pictorial Essay
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Bariatric Surgical Techniques
2.1. Restrictive Procedures
2.2. Combined Restrictive and Malabsorptive Procedures
3. Complications
3.1. Imaging Techniques
- Upper gastrointestinal (UGI) barium studies;
- Fluoroscopic upper GI examinations with water-soluble contrast agents; and
- Enhanced-CT.
3.2. General Complications, Procedure Unrelated
3.3. Specific Complications
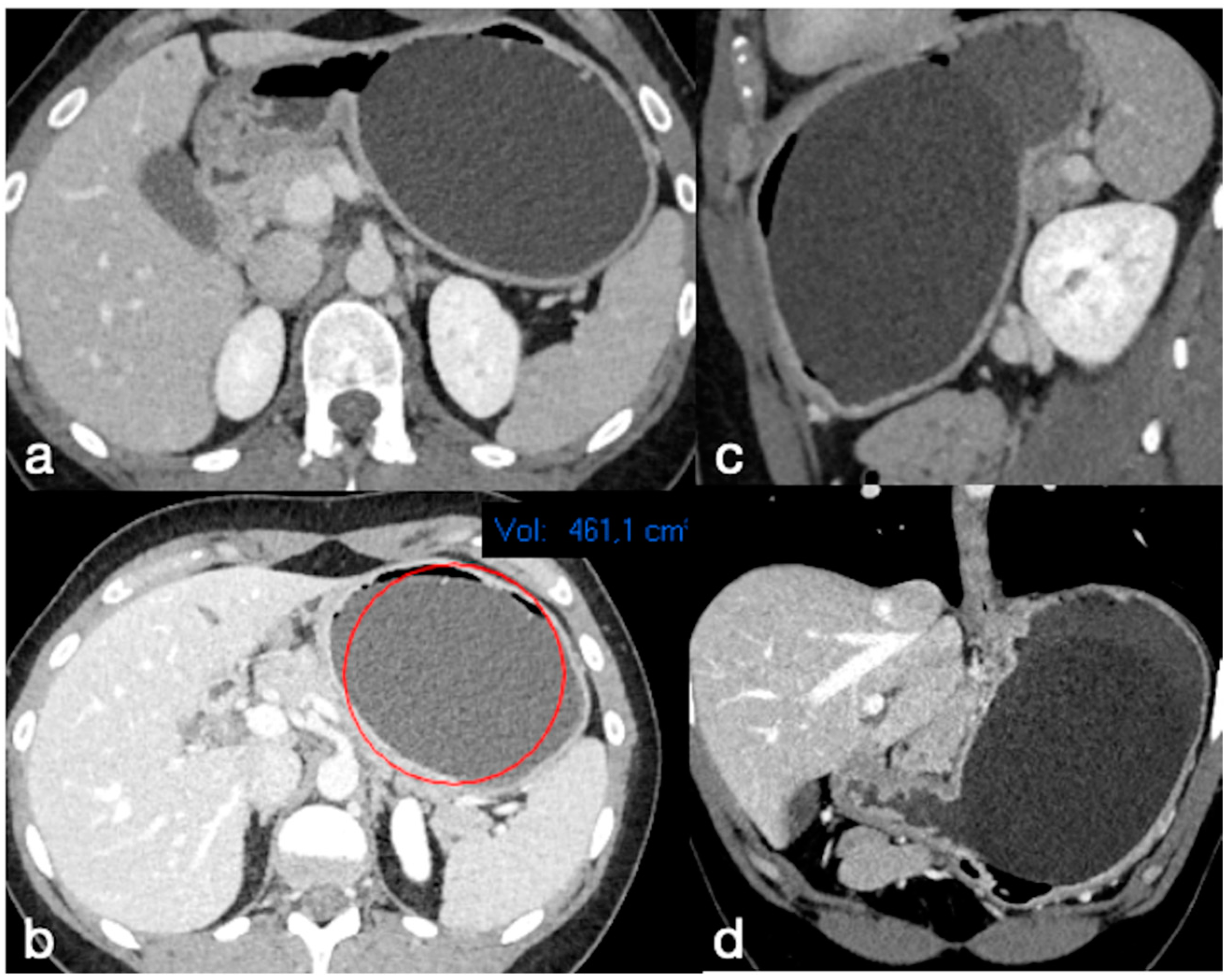
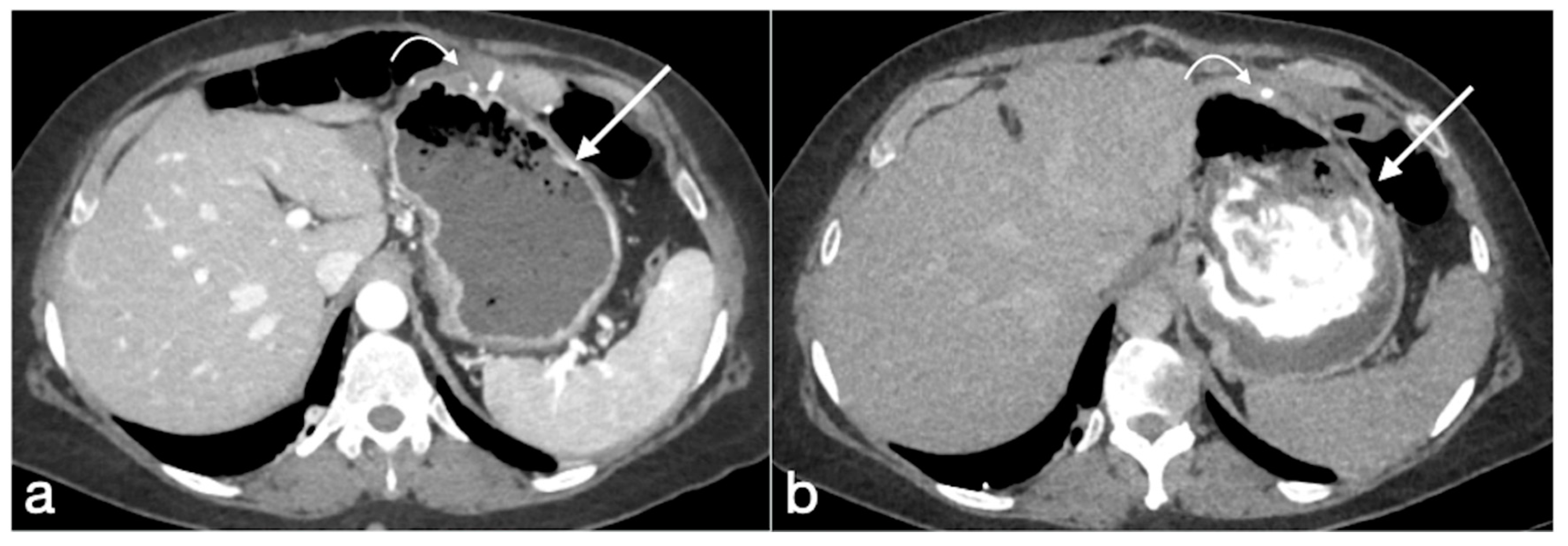
3.3.1. GB
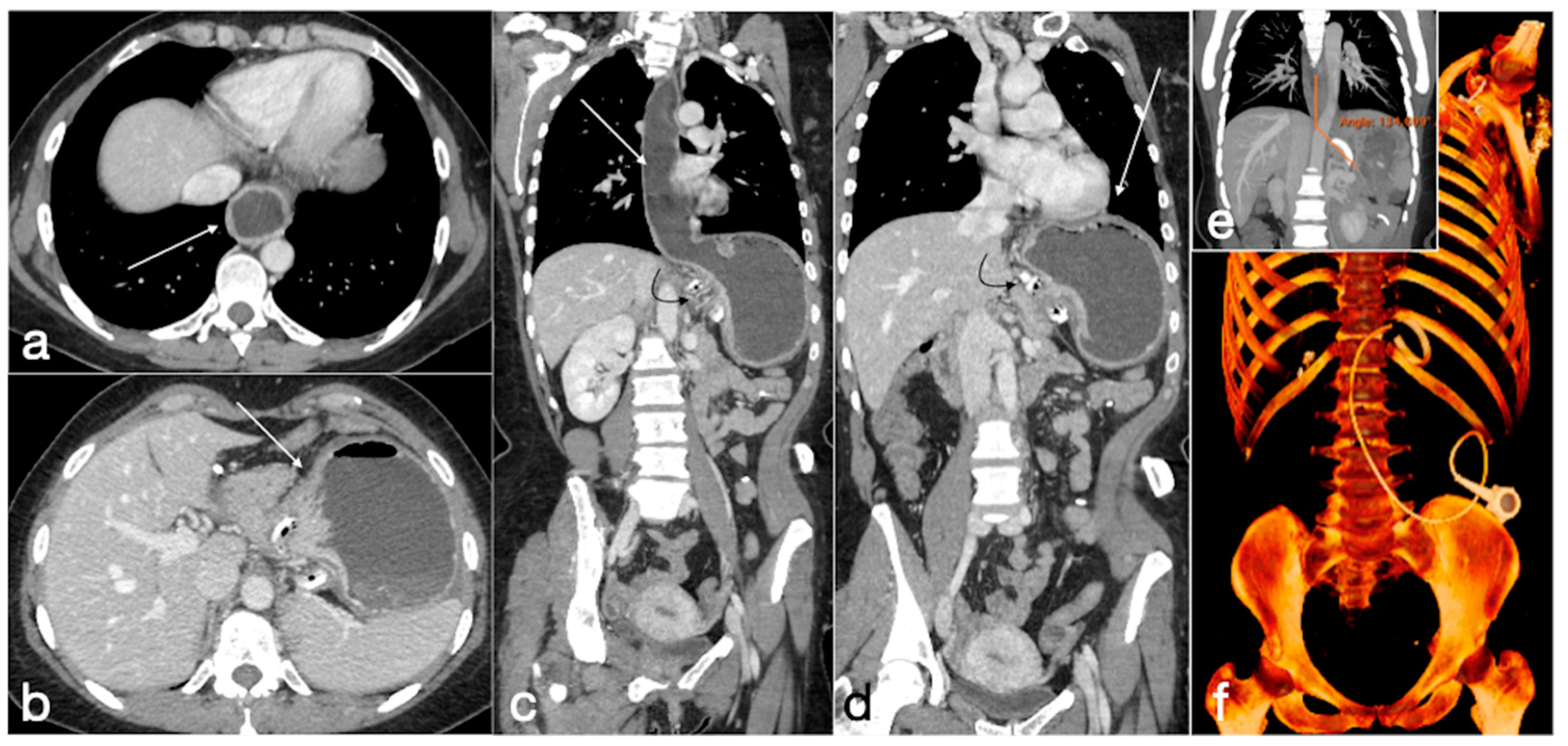
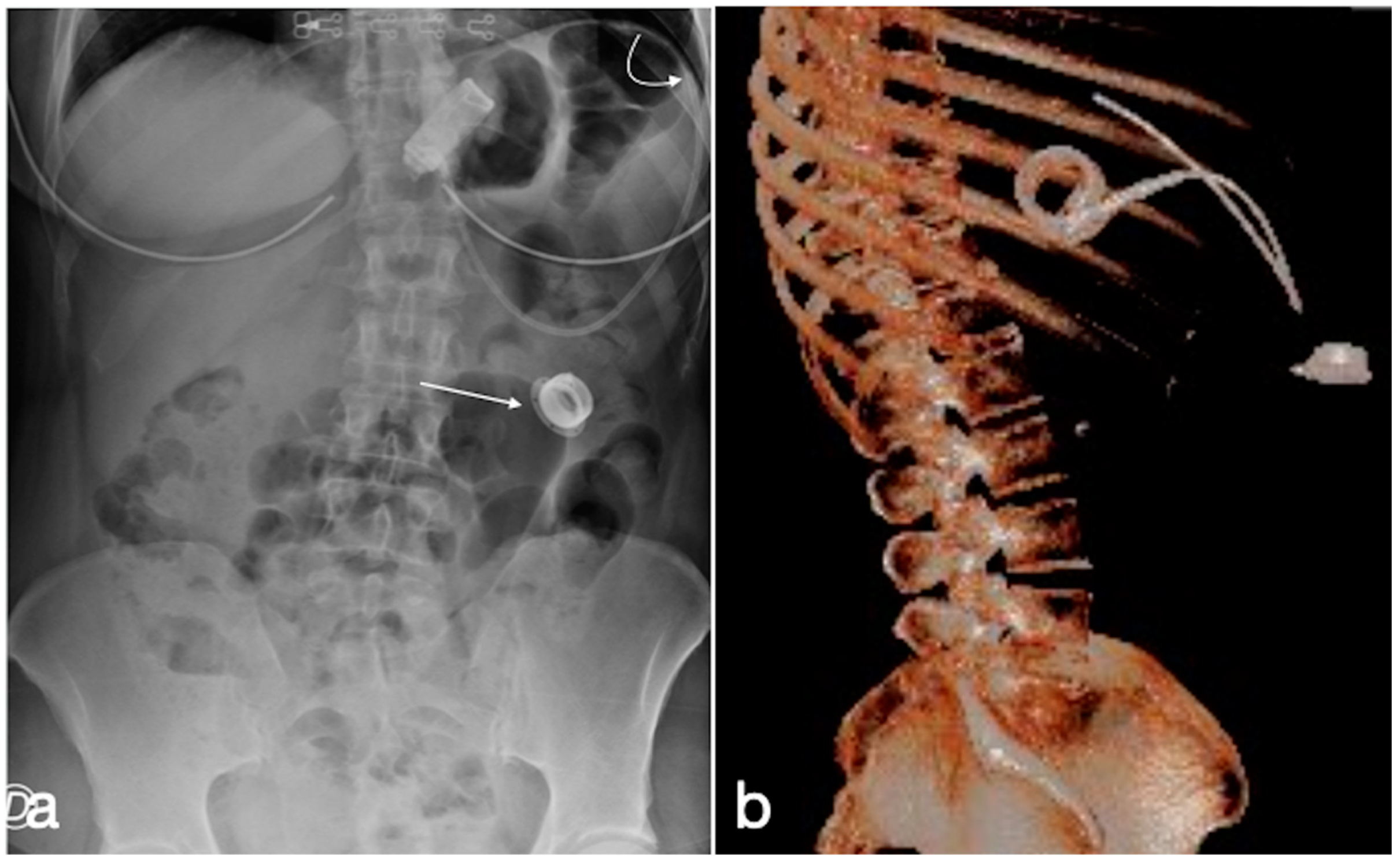
- Spontaneous deflation-rupture
- Ulceration
- Gastric outlet obstruction
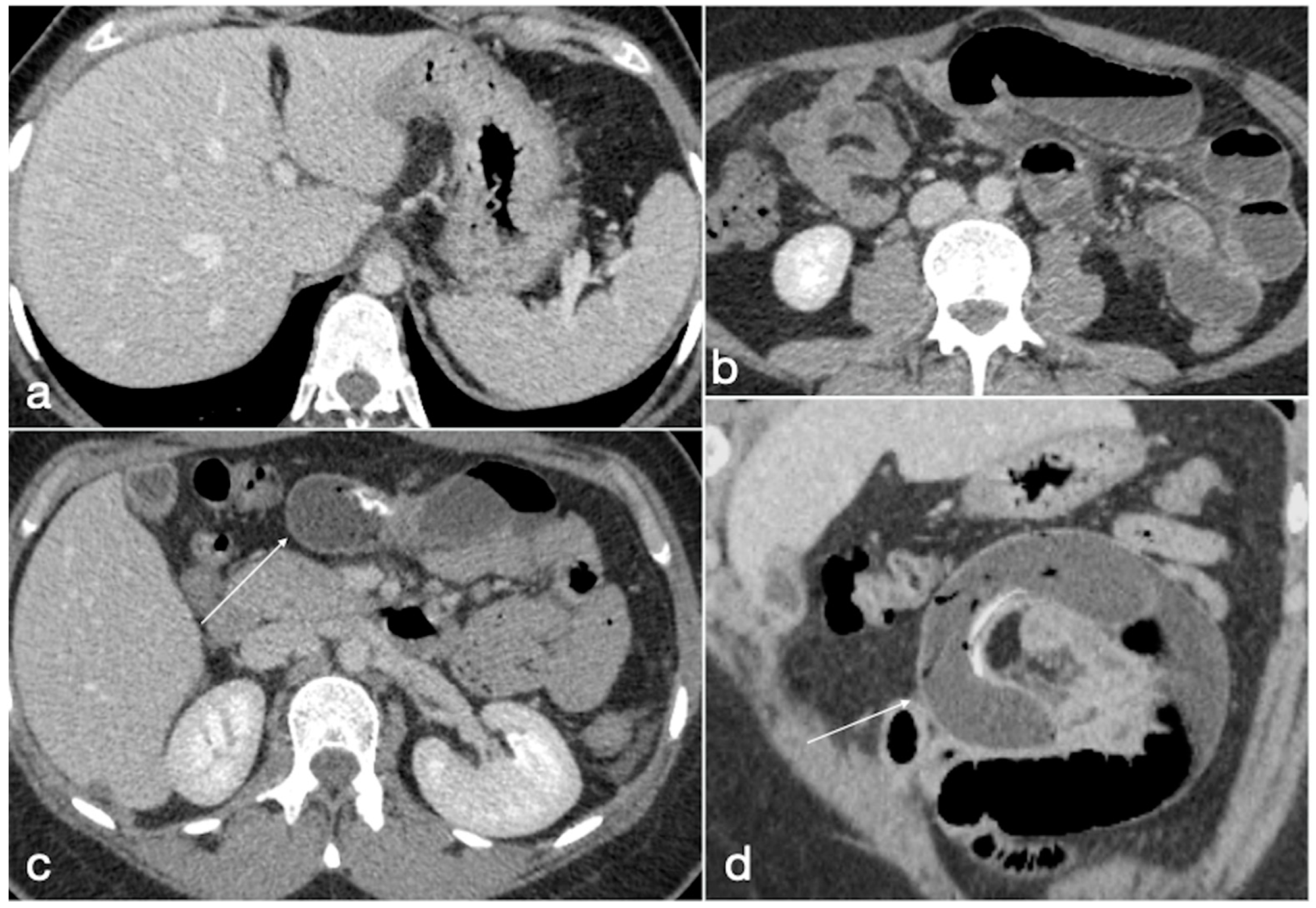
- Migration and bowel obstruction
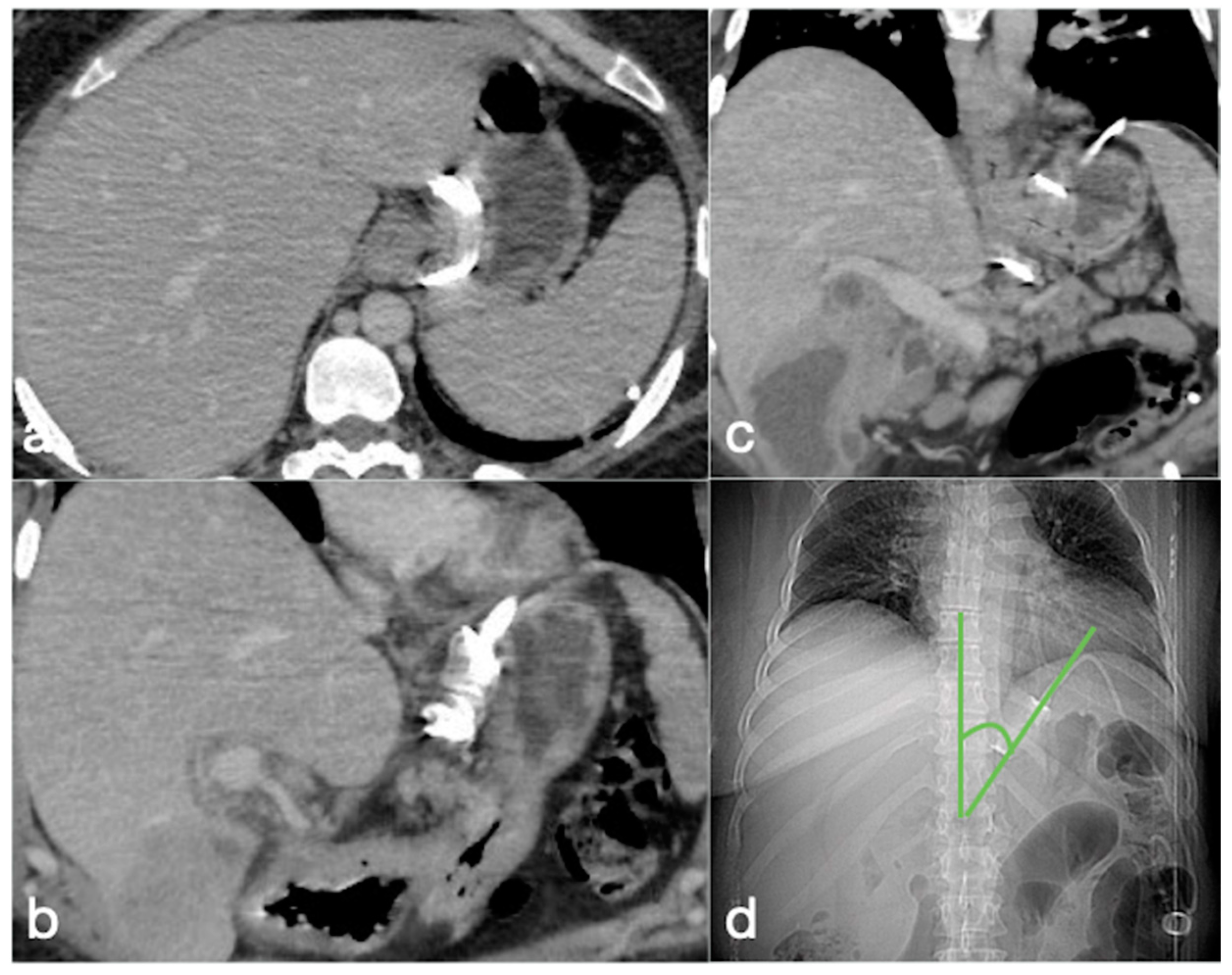
3.3.2. AGB
- Band slippage
- Pouch dilatation
- Device-related
- Erosion
- Acute perforation
- Gastric volvulus
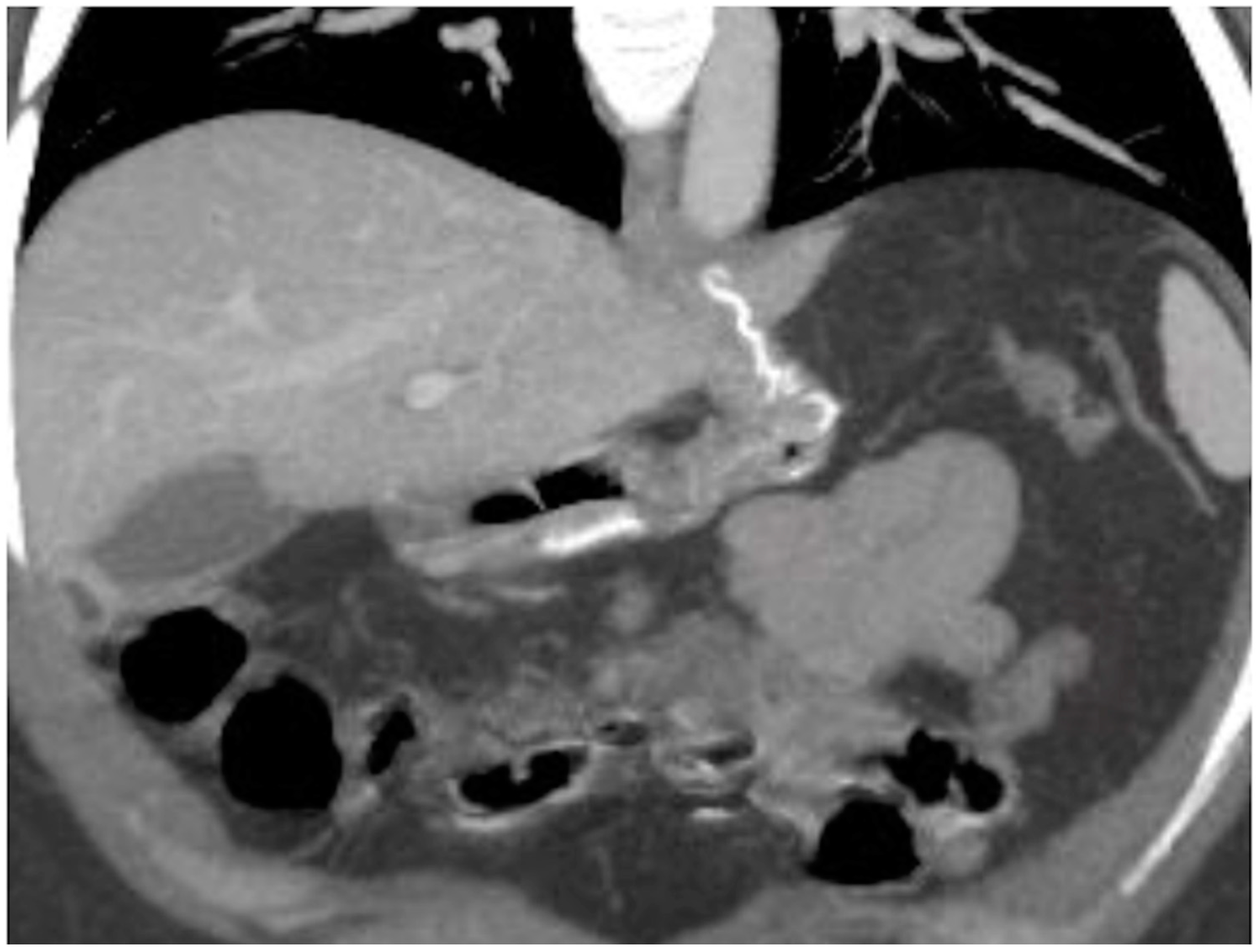
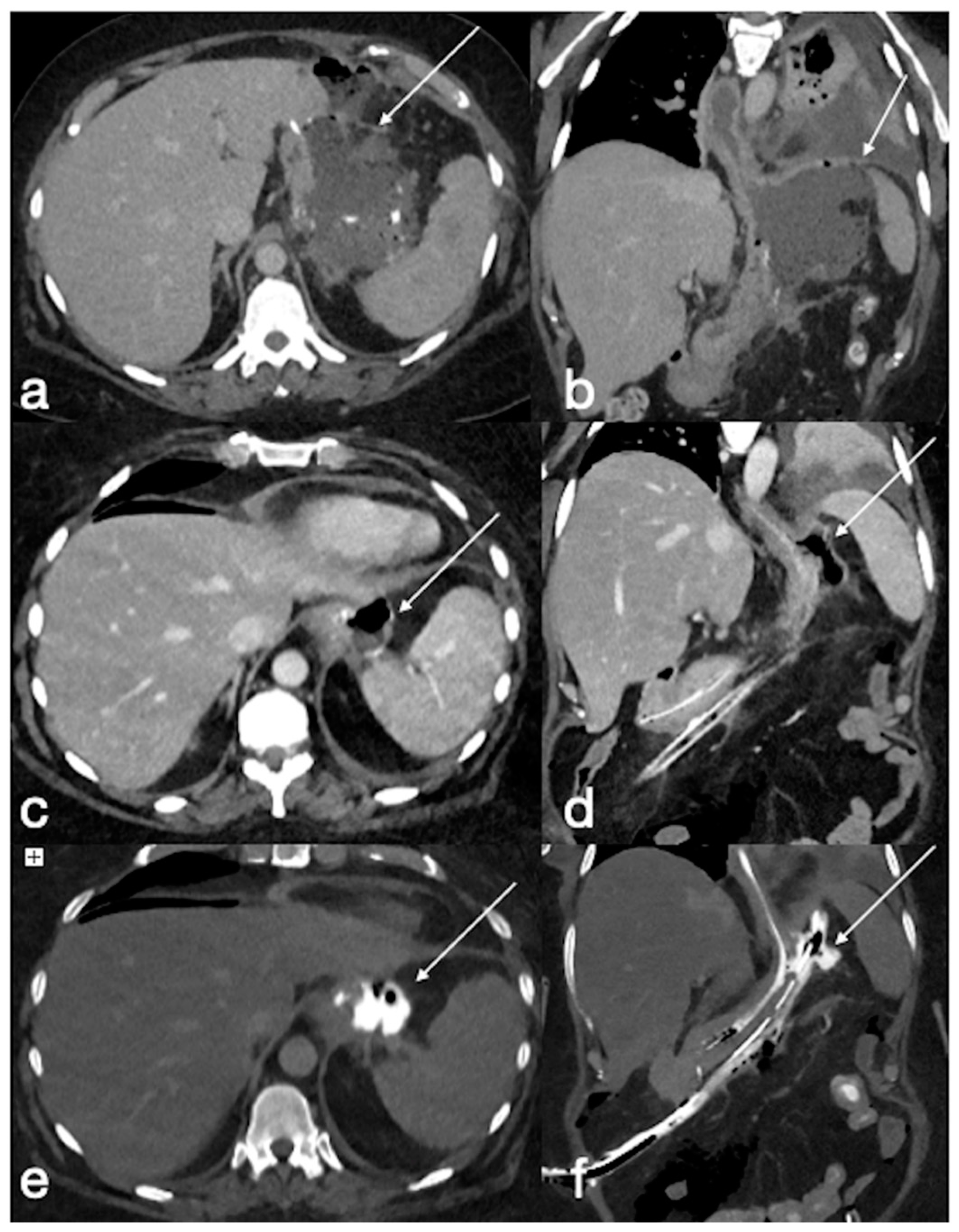
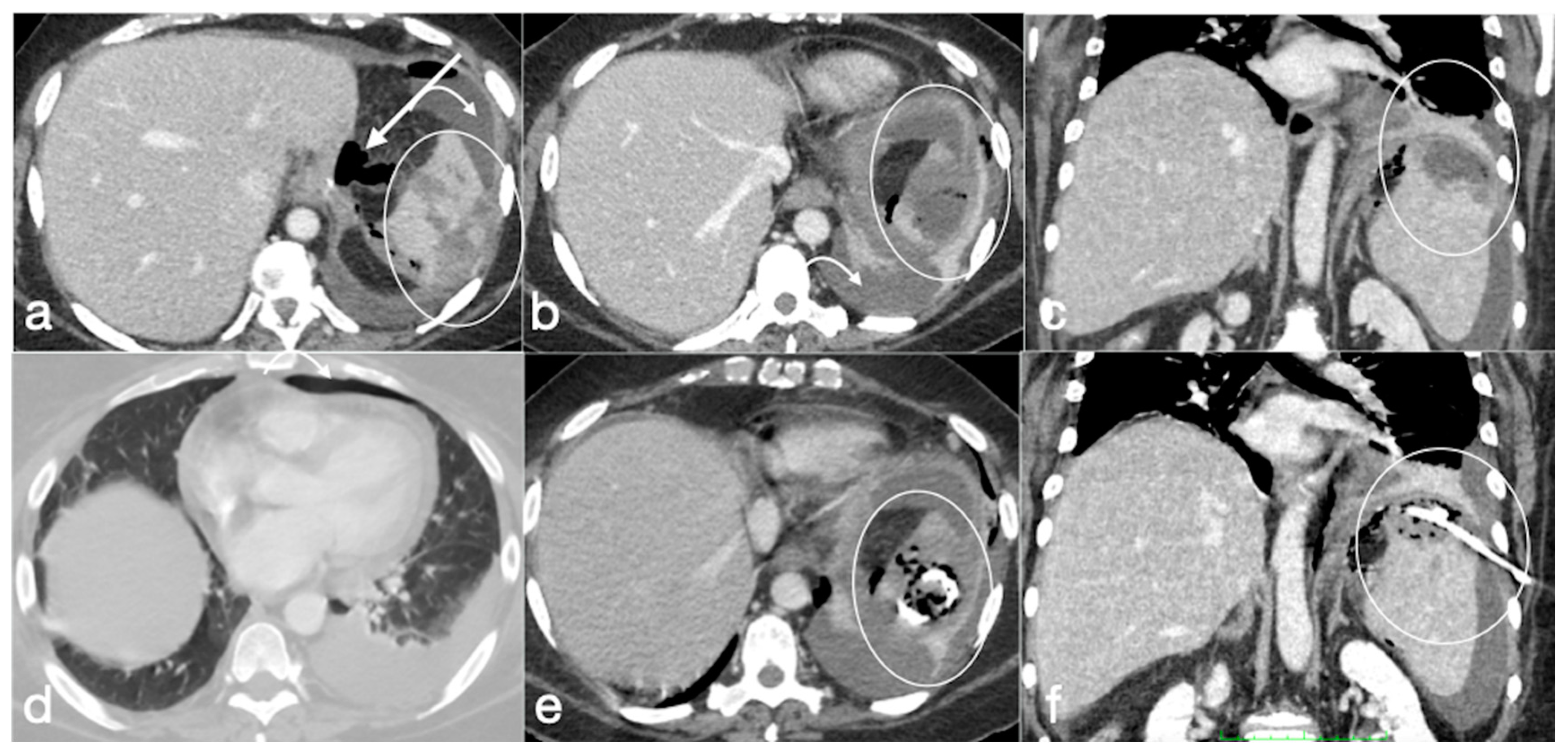
3.3.3. SG
- Leak
- After SG leakage classification
- Gastric dilatation
- Stenosis
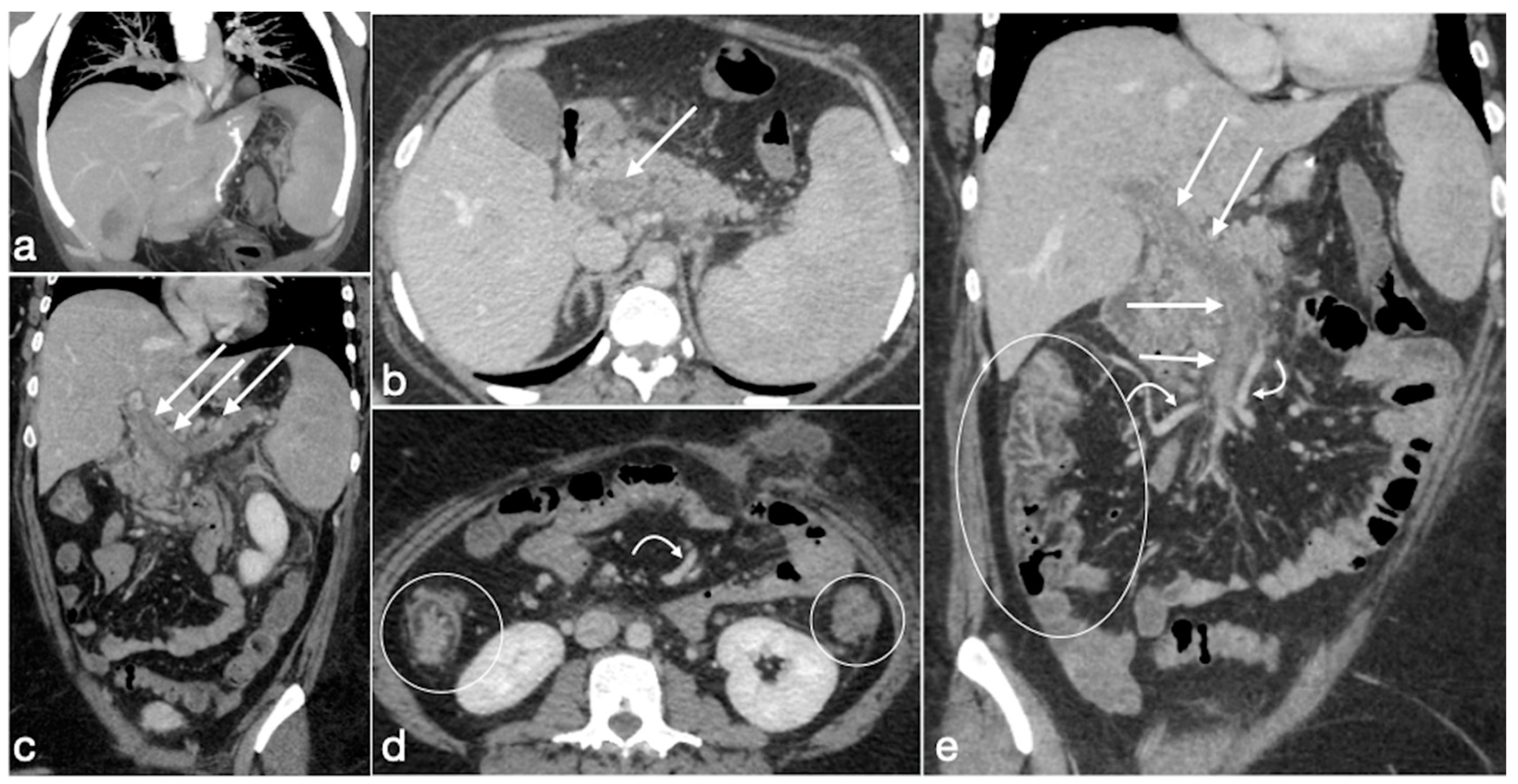
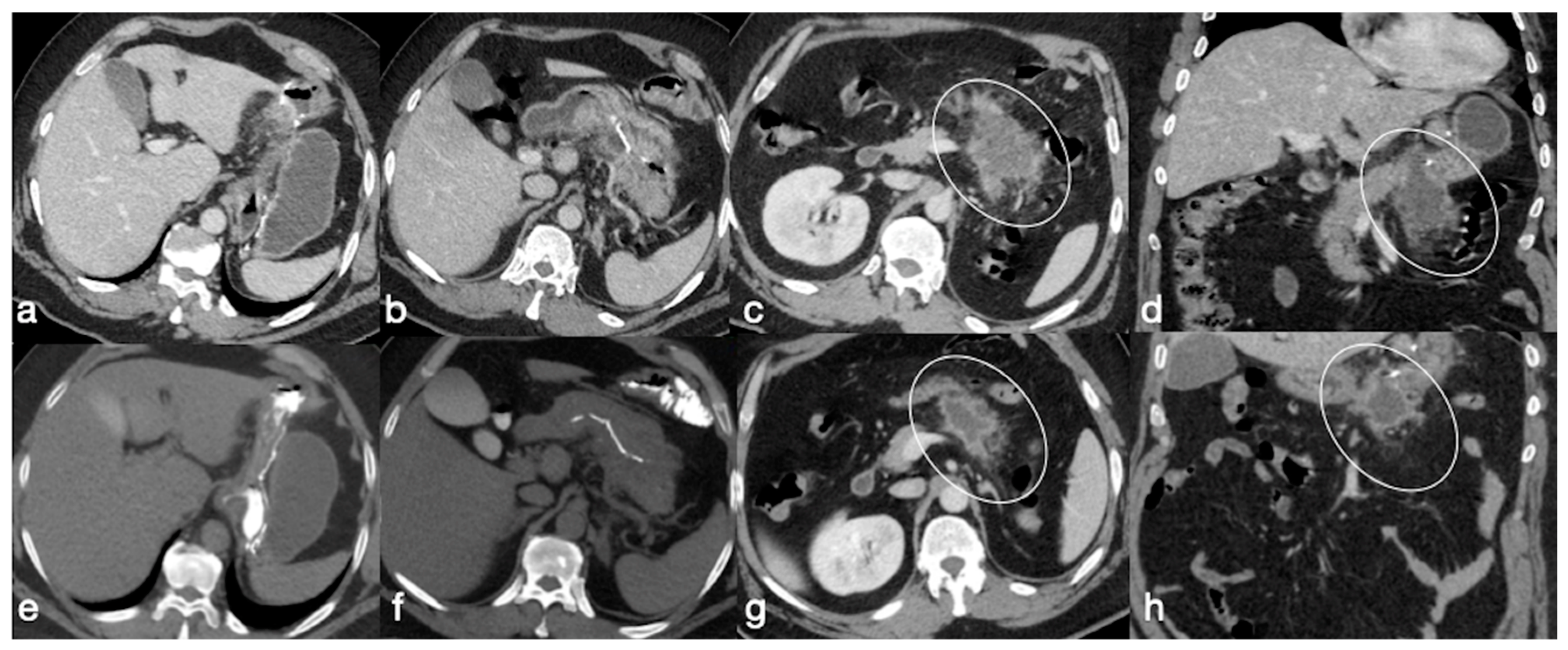
- Spleno-porto-mesenteric vein thrombosis (PVT)
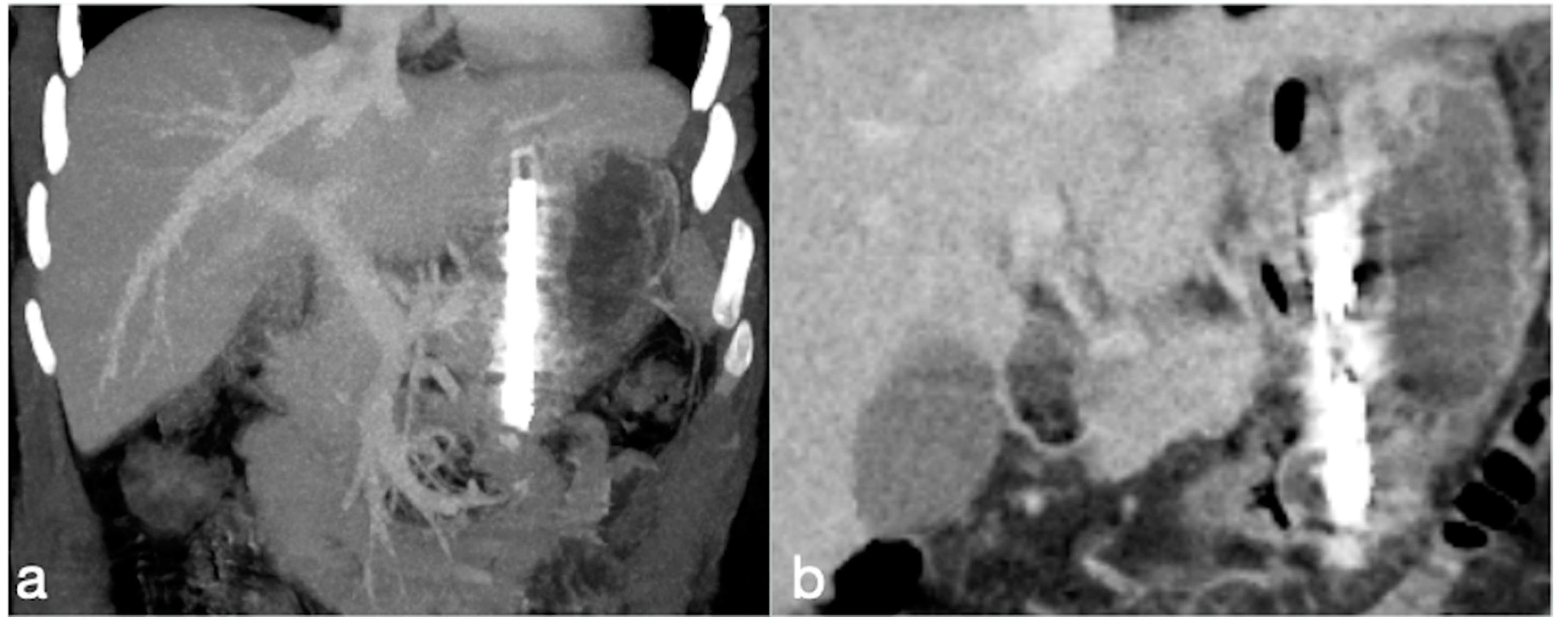
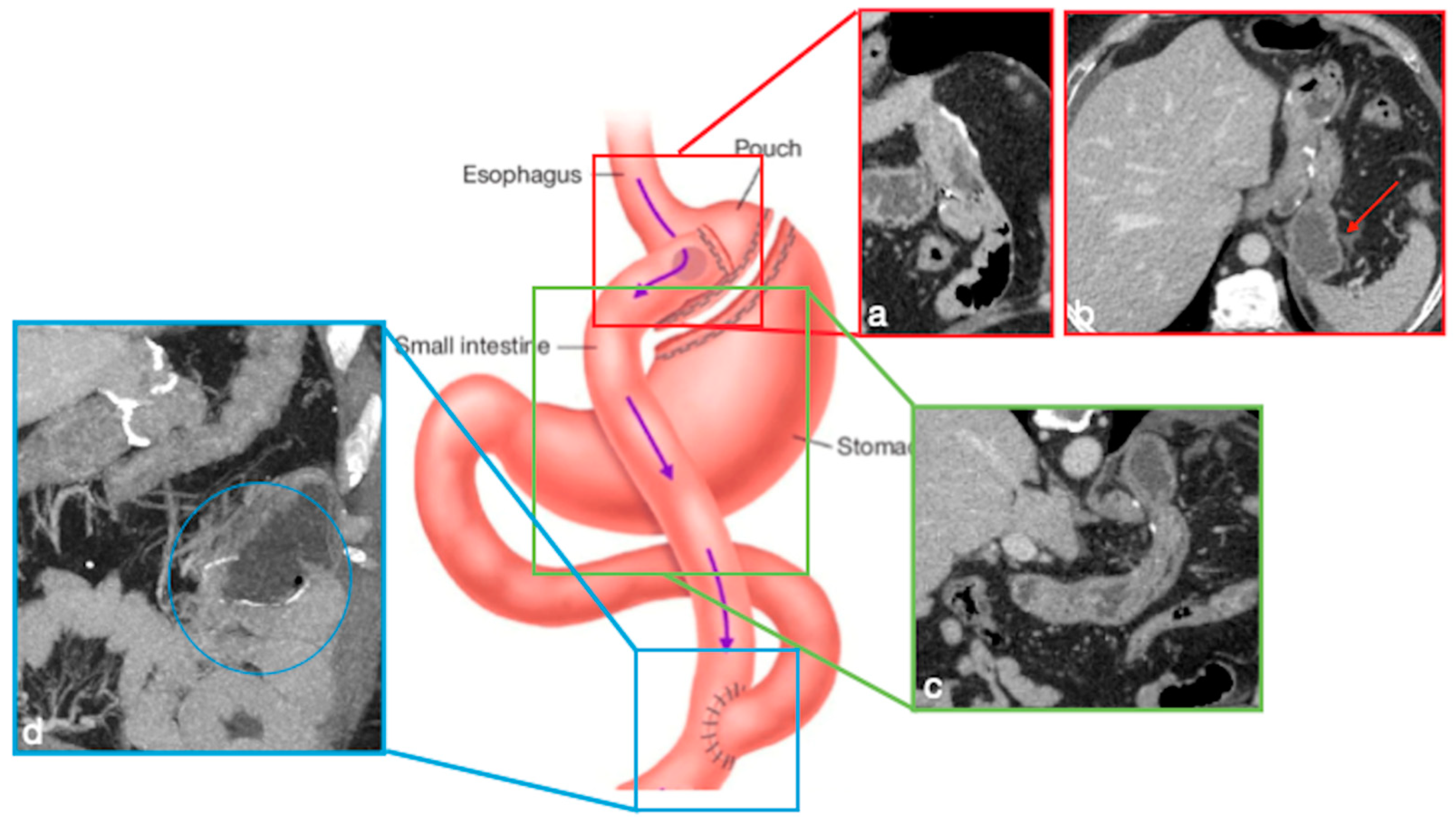
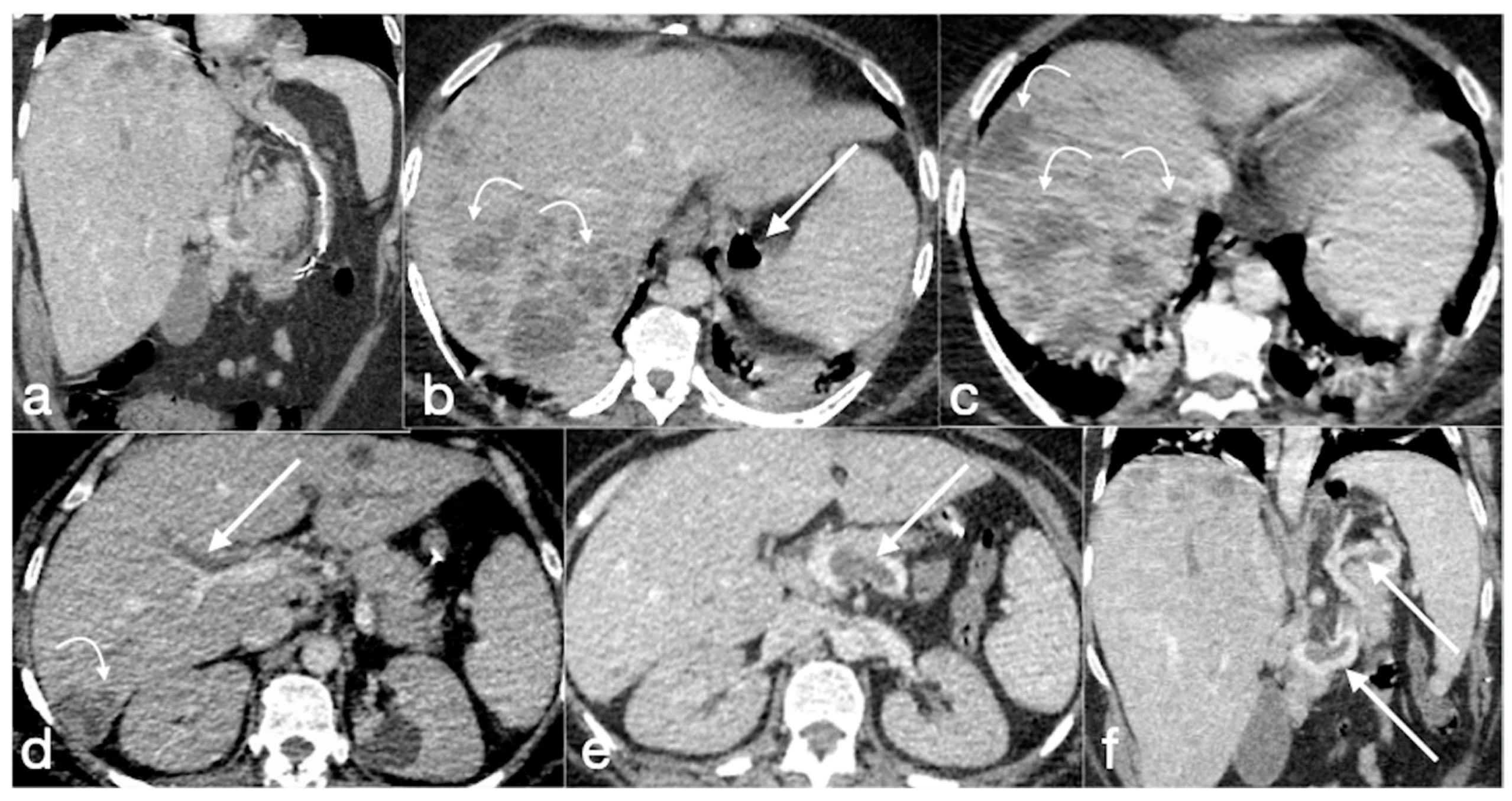
3.3.4. RYGB
- Stenosis
- Leak
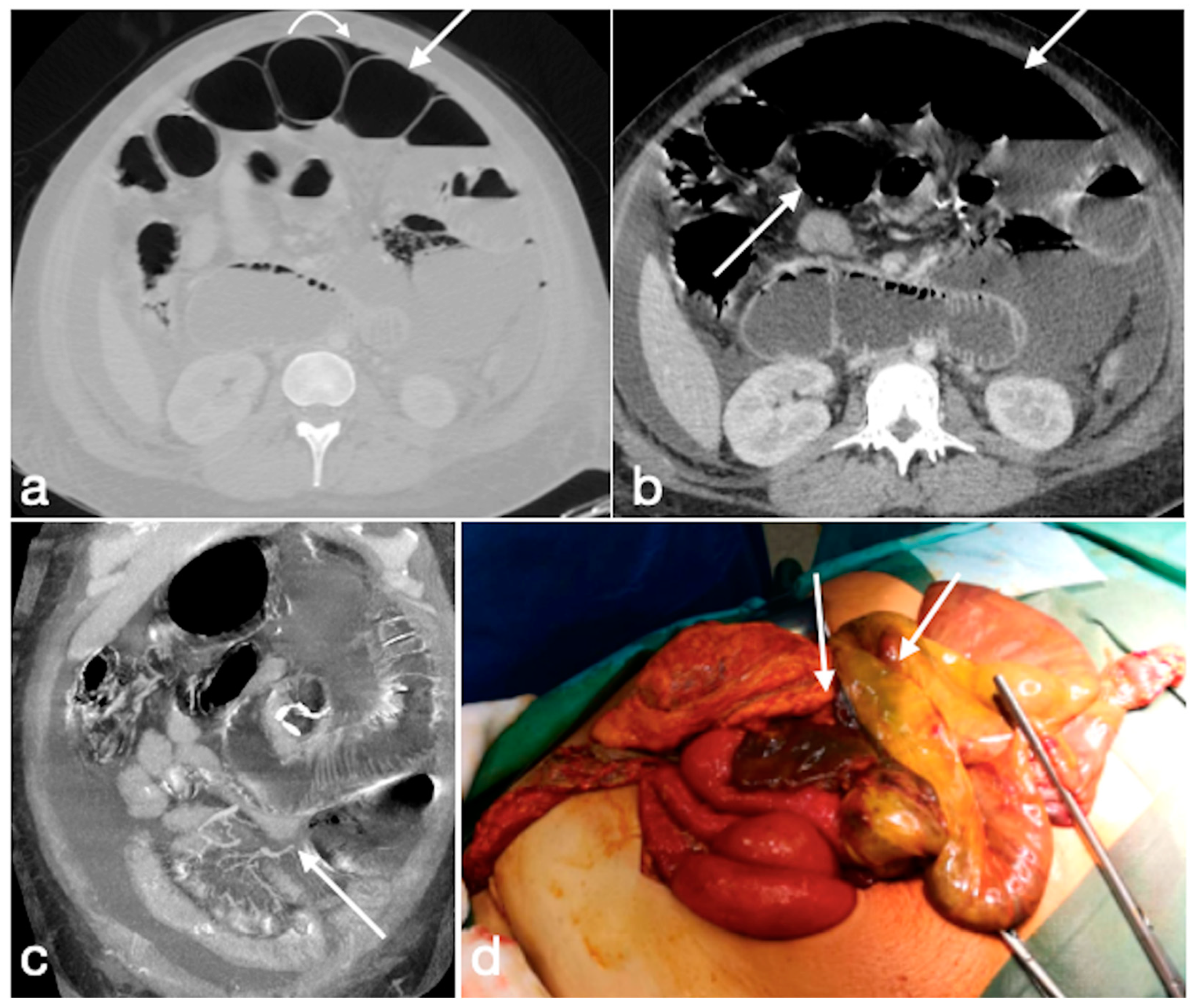
- Small bowel obstruction
- (a)
- The obstruction involves the alimentary limb, that appears dilated, while both biliopancreatic limb and distal common channel are hypotonic.
- (b)
- The obstruction involves the biliopancreatic limb, which appears dilated, whereas the alimentary limb and distal common channel are decompressed. This closed-loop obstruction could determine perforation of excluded gastric cavity. On UGI, there is a dilated and fluid-filled limb (biliopancreatic) excluded by an oral contrast passage that could determine a mass-effect on the other bowel loops. Upon CT, detection is easy, and it should be suspected not only for the biliopancreatic limb appearance associated to decompression of alimentary and common channel, but also for the recognition of dilatation of excluded gastric room.
- (c)
- The obstruction involves the common channel; any bowel loops upstream appear dilated [4].
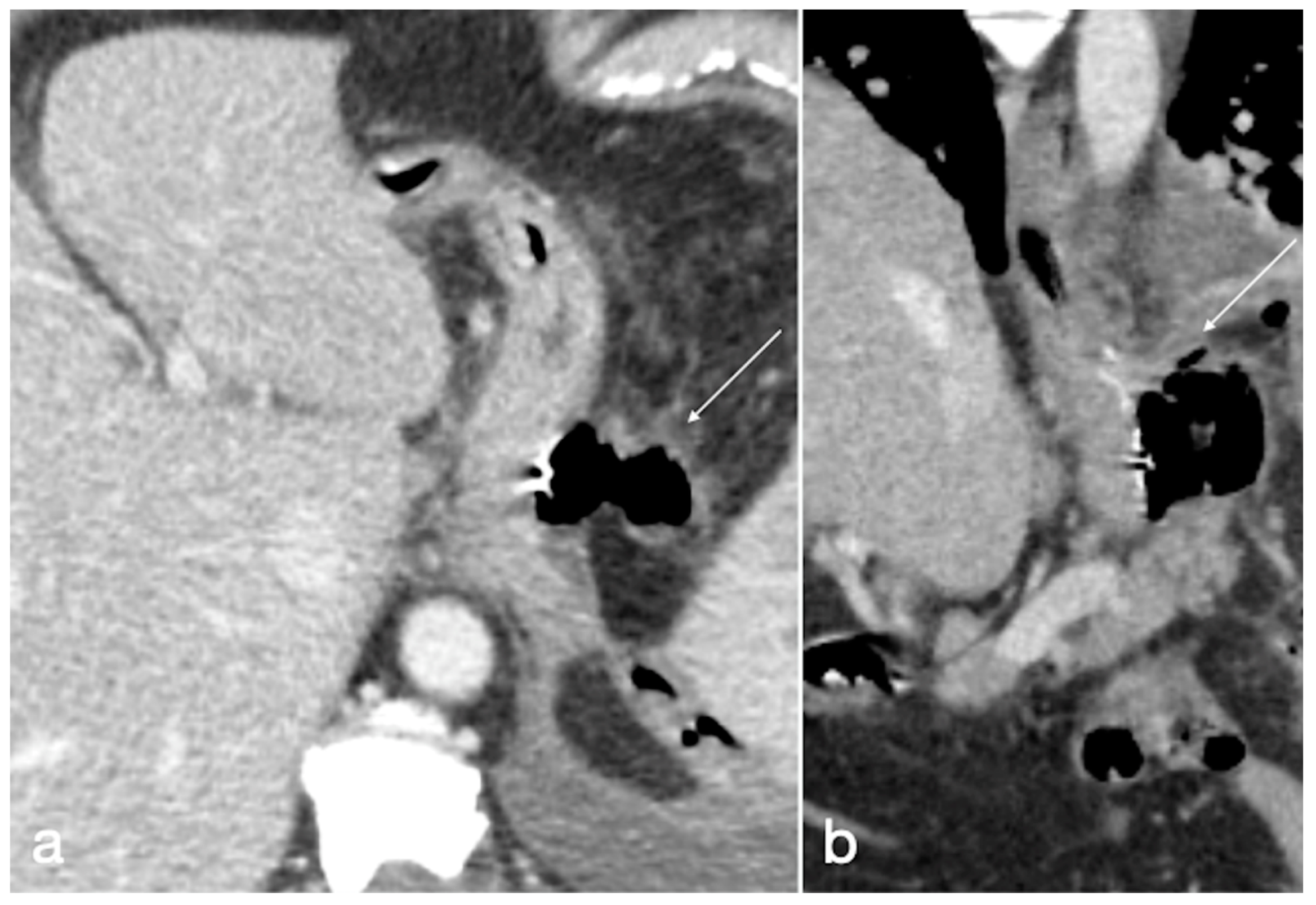
- Fistula
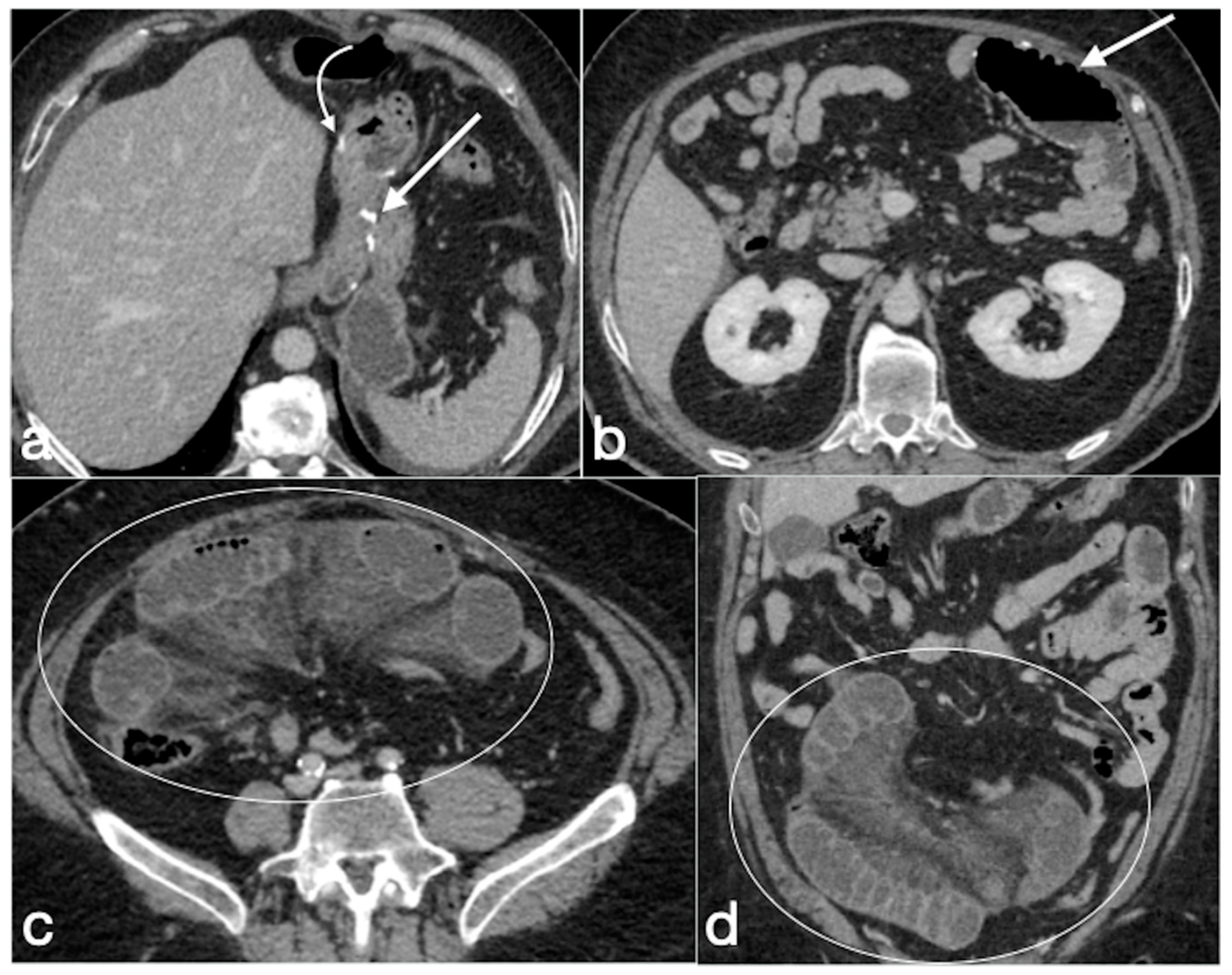
- Internal hernia
- Marginal ulcers
- Intussusception
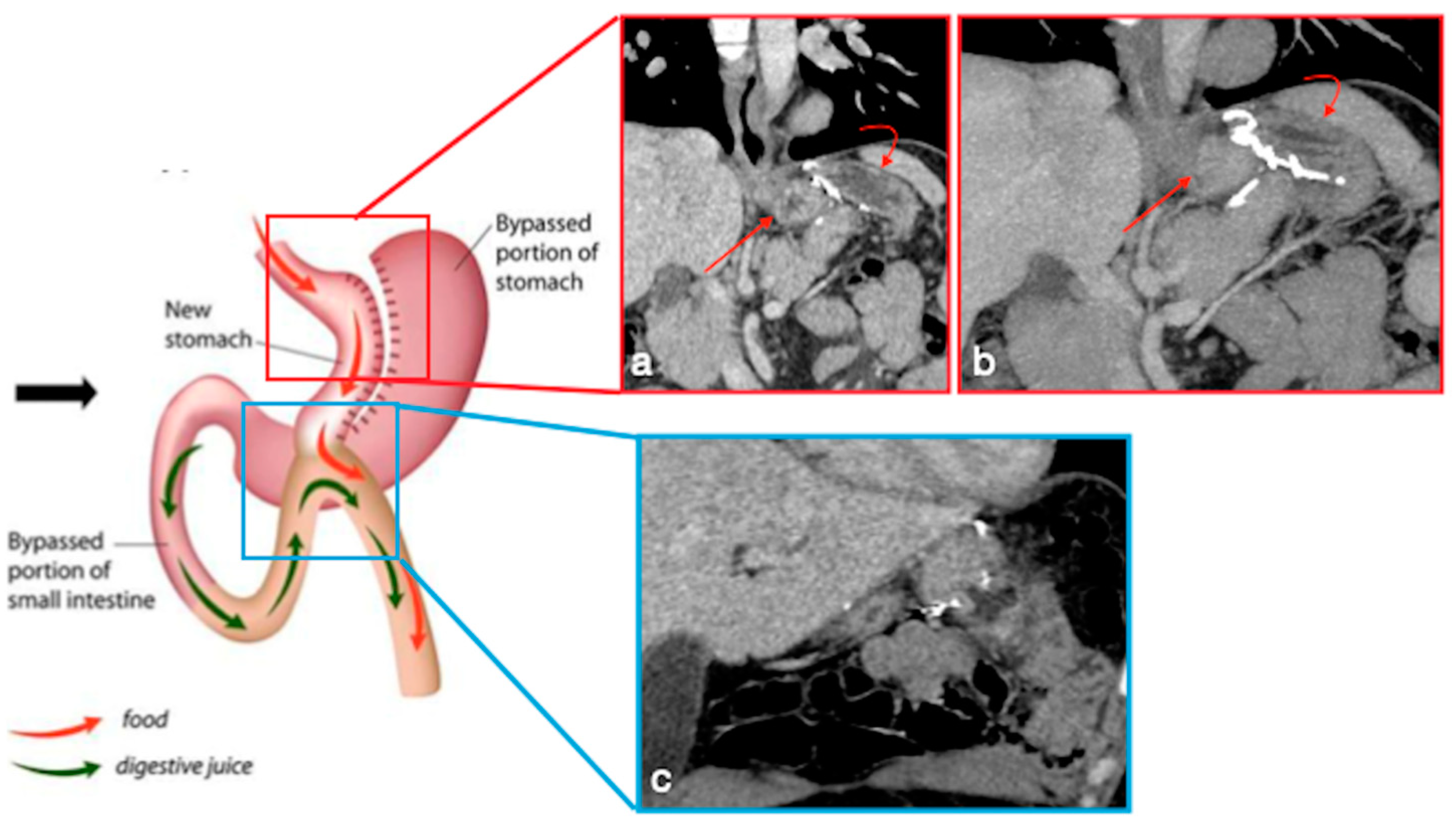
3.3.5. OAGB-MGB
- Marginal ulcers
- Internal hernia
- Anastomotic stenosis
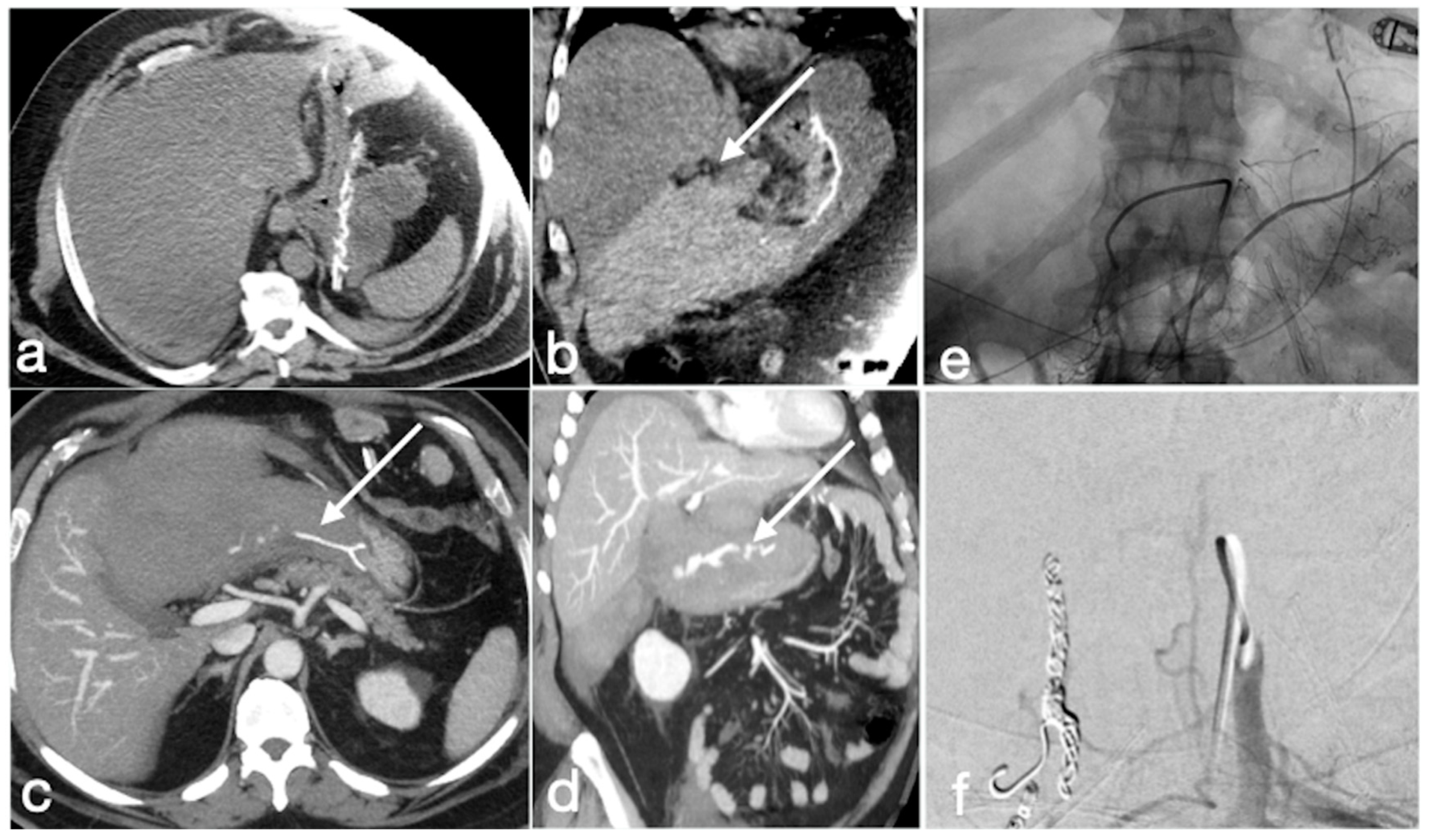
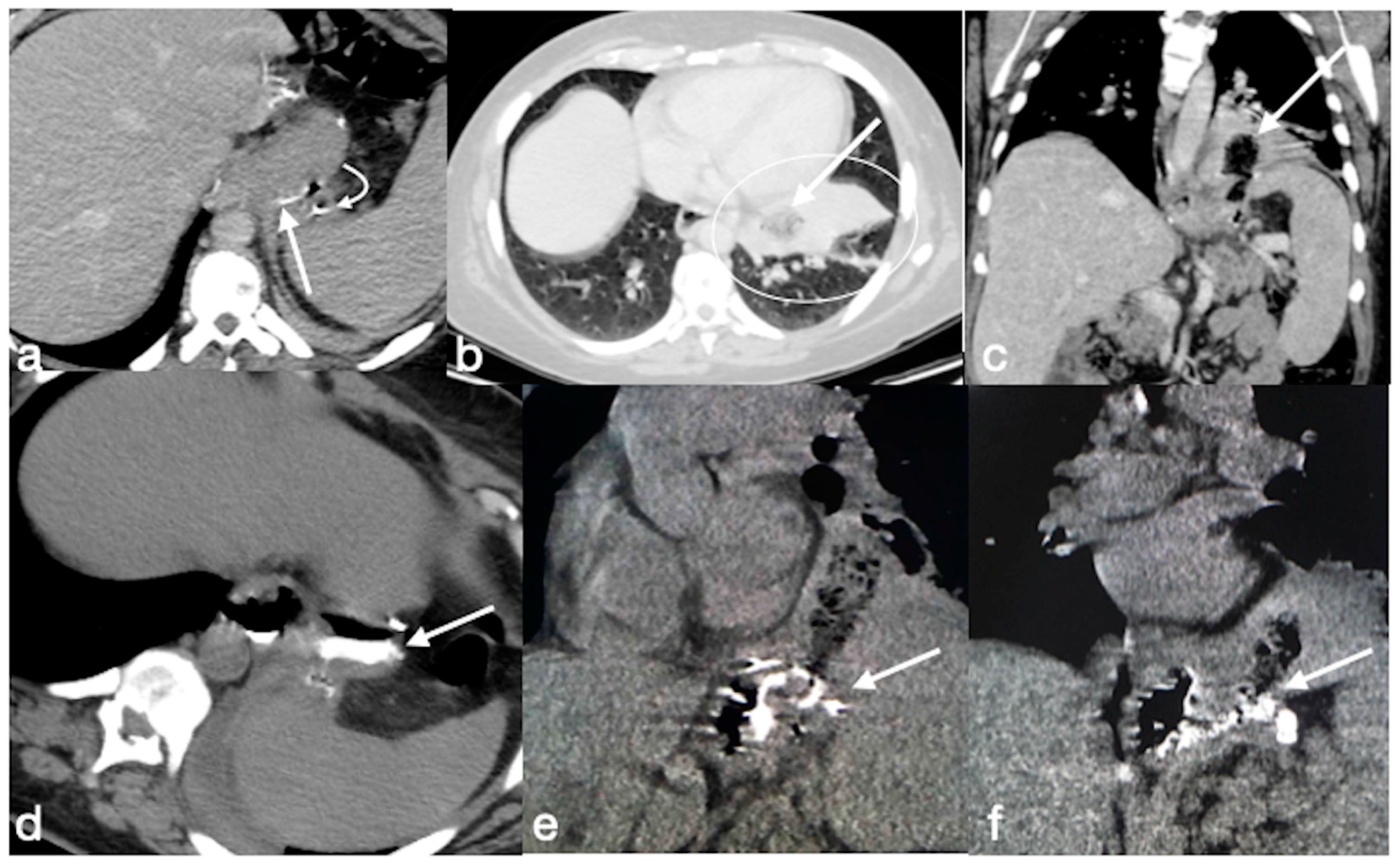
3.4. Unexpected Complication
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- American Society for Metabolic and Bariatric Surgery (ASMBS). 2019. Available online: https://asmbs.org/resources/bariatric-surgery-guidelines-and-recommendations (accessed on 23 October 2022).
- Cohen, R.V.; Shikora, S.; Petry, T.; Caravatto, P.P.; Le Roux, C.W. The Diabetes Surgery Summit II Guidelines: A Disease-Based Clinical Recommendation. Obes. Surg. 2016, 26, 1989–1991. [Google Scholar] [CrossRef] [PubMed]
- Clayton, R.D.; Carucci, L.R. Imaging following bariatric surgery: Roux-en-Y gastric bypass, laparoscopic adjustable gastric banding and sleeve gastrectomy. Br. J. Radiol. 2018, 91, 20180031. [Google Scholar] [CrossRef] [PubMed]
- Arterburn, D.E.; Telem, D.A.; Kushner, R.F.; Courcoulas, A.P. Benefits and Risks of Bariatric Surgery in Adults: A Review. JAMA 2020, 324, 879–887. [Google Scholar] [CrossRef]
- Levine, M.S.; Carucci, L.R. Imaging of Bariatric Surgery: Normal Anatomy and Postoperative Complications. Radiology 2014, 270, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.B.M.; Greenslade, J.; Martin, D.; Talbot, M.; Loi, K.; Hopkins, G. Portomesenteric vein thrombosis in sleeve gastrectomy: A 10-year review. Surg. Obes. Relat. Dis. 2018, 14, 271–275. [Google Scholar] [CrossRef]
- Morandeira, C.; Bárcena, M.; Bilbao, A.; Pérez, M.; Ibáñez, A.; Isusi, M.; Lecumberri, G. Studying the complications of bariatric surgery with intravenous contrast-enhanced multidetector computed tomography. Radiología 2018, 60, 143–151. [Google Scholar] [CrossRef]
- Akalestou, E.; Miras, A.D.; Rutter, G.A.; le Roux, C.W. Mechanisms of Weight Loss After Obesity Surgery. Endocr. Rev. 2022, 43, 19–34. [Google Scholar] [CrossRef]
- Lim, R.; Beekley, A.; Johnson, D.C.; Davis, K.A. Early and late complications of bariatric operation. Trauma Surg. Acute Care Open 2018, 3, e000219. [Google Scholar] [CrossRef] [Green Version]
- Abu Dayyeh, B.K. Intragastric Balloons for Obesity Management. Gastroenterol. Hepatol. 2017, 13, 737–739. [Google Scholar]
- Shah, S.; Shah, V.; Ahmed, A.R.; Blunt, D.M. Imaging in bariatric surgery: Service set-up, post-operative anatomy and complications. Br. J. Radiol. 2011, 84, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Stahl, J.M.; Malhotra, S. Obesity Surgery Indications and Contraindications. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Benaiges, D.; Más-Lorenzo, A.; Goday, A.; Ramon, J.M.; Chillarón, J.J.; Pedro-Botet, J.; Roux, J.A.F.-L. Laparoscopic sleeve gastrectomy: More than a restrictive bariatric surgery procedure? World J. Gastroenterol. 2015, 21, 11804–11814. [Google Scholar] [CrossRef] [PubMed]
- Noel, P.; Eddbali, I.; Nedelcu, M. Laparoscopic Clip Gastroplasty with the BariClip. Obes. Surg. 2020, 30, 5182–5183. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Hong, S.S.; Hwang, J.; Hur, K.Y. Mini-Gastric Bypass to Control Morbid Obesity and Diabetes Mellitus: What Radiologists Need to Know. Korean J. Radiol. 2015, 16, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Robert, M.; Espalieu, P.; Pelascini, E.; Caiazzo, R.; Sterkers, A.; Khamphommala, L.; Poghosyan, T.; Chevallier, J.-M.; Malherbe, V.; Chouillard, E.; et al. Efficacy and safety of one anastomosis gastric bypass versus Roux-en-Y gastric bypass for obesity (YOMEGA): A multicentre, randomised, open-label, non-inferiority trial. Lancet 2019, 393, 1299–1309. [Google Scholar] [CrossRef]
- Scaglione, M.; Basilico, R.; Pizzi, A.D.; Iacobellis, F.; Dick, E.; Wirth, S.; Linsenmaier, U.; Calli, C.; Berger, F.H.; Nieboer, K.H.; et al. The practice of emergency radiology throughout Europe: A survey from the European Society of Emergency Radiology on volume, staffing, equipment, and scheduling. Eur. Radiol. 2021, 31, 2994–3001. [Google Scholar] [CrossRef]
- Reginelli, A.; Iacobellis, F.; Berritto, D.; Gagliardi, G.; Di Grezia, G.; Rossi, M.; Fonio, P.; Grassi, R. Mesenteric ischemia: The importance of differential diagnosis for the surgeon. BMC Surg. 2013, 13, S51. [Google Scholar] [CrossRef] [Green Version]
- Brillantino, A.; Lanza, M.; Antropoli, M.; Amendola, A.; Squillante, S.; Bottino, V.; Renzi, A.; Castriconi, M. Usefulness of damage control approach in patients with limited acute mesenteric ischemia: A prospective study of 85 patients. Updat. Surg. 2022, 74, 337–342. [Google Scholar] [CrossRef]
- Cobianchi, L.; Mas, F.D.; Massaro, M.; Fugazzola, P.; Coccolini, F.; Kluger, Y.; Leppäniemi, A.; Moore, E.E.; Sartelli, M.; Angelos, P.; et al. Team dynamics in emergency surgery teams: Results from a first international survey. World J. Emerg. Surg. 2021, 16, 47. [Google Scholar] [CrossRef]
- Woodfield, J.; Deo, P.; Davidson, A.; Chen, T.Y.T.; van Rij, A. Patient reporting of complications after surgery: What impact does documenting postoperative problems from the perspective of the patient using telephone interview and postal questionnaires have on the identification of complications after surgery? BMJ Open 2019, 9, e028561. [Google Scholar] [CrossRef]
- Koek, S.A.; Hammond, J. Gastric outlet obstruction secondary to orbera intragastric balloon. J. Surg. Case Rep. 2018, 2018, rjy284. [Google Scholar] [CrossRef] [PubMed]
- Kannan, R.Y.; Nutt, M. Are intra-gastric adjustable balloon system safe? A case series. Int. J. Surg. Case Rep. 2013, 4, 936–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, I.K.; Chun, H.J.; Jeen, Y.T. Gastric Perforation Caused by an Intragastric Balloon: Endoscopic Findings. Clin. Endosc. 2017, 50, 602–604. [Google Scholar] [CrossRef] [Green Version]
- Faggian, A.; Berritto, D.; Iacobellis, F.; Reginelli, A.; Cappabianca, S.; Grassi, R. Imaging Patients with Alimentary Tract Perforation: Literature Review. Semin. Ultrasound CT MRI 2016, 37, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Chun, H.J.; Choi, H.S.; Kim, E.S.; Keum, B.; Jeen, Y.T. Current status of intragastric balloon for obesity treatment. World J. Gastroenterol. 2016, 22, 5495–5504. [Google Scholar] [CrossRef] [PubMed]
- Sonavane, S.K.; Menias, C.O.; Kantawala, K.P.; Shanbhogue, A.K.; Prasad, S.R.; Eagon, J.C.; Sandrasegaran, K. Laparoscopic Adjustable Gastric Banding: What Radiologists Need to Know. RadioGraphics 2012, 32, 1161–1178. [Google Scholar] [CrossRef]
- Singhal, R.; Bryant, C.; Kitchen, M.; Khan, K.S.; Deeks, J.; Guo, B.; Super, P. Band slippage and erosion after laparoscopic gastric banding: A meta-analysis. Surg. Endosc. 2010, 24, 2980–2986. [Google Scholar] [CrossRef]
- Kicska, G.; Levine, M.S.; Raper, S.E.; Williams, N.N. Gastric Volvulus After Laparoscopic Adjustable Gastric Banding for Morbid Obesity. Am. J. Roentgenol. 2007, 189, 1469–1472. [Google Scholar] [CrossRef]
- Gero, D.; Raptis, D.A.; Vleeschouwers, W.; Van Veldhuisen, S.L.; Martin, A.S.; Xiao, Y.; Galvao, M.; Giorgi, M.; Benois, M.; Espinoza, F.; et al. Defining Global Benchmarks in Bariatric Surgery: A Retrospective Multicenter Analysis of Minimally Invasive Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Ann. Surg. 2019, 270, 859–867. [Google Scholar] [CrossRef]
- Nedelcu, M.; Skalli, M.; Delhom, E.; Fabre, J.M.; Nocca, D. New CT Scan Classification of Leak After Sleeve Gastrectomy. Obes. Surg. 2013, 23, 1341–1343. [Google Scholar] [CrossRef]
- Levy, J.L.; Levine, M.S.; Rubesin, S.E.; Williams, N.N.; Dumon, K.R. Stenosis of gastric sleeve after laparoscopic sleeve gastrectomy: Clinical, radiographic and endoscopic findings. Br. J. Radiol. 2018, 91, 20170702. [Google Scholar] [CrossRef] [PubMed]
- Chandler, R.C.; Srinivas, G.; Chintapalli, K.N.; Schwesinger, W.H.; Prasad, S.R. Imaging in Bariatric Surgery: A Guide to Postsurgical Anatomy and Common Complications. Am. J. Roentgenol. 2008, 190, 122–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoraki, J.; Mazzini, G.S.; Shah, A.S.; Del Prado, P.A.; Wolfe, L.G.; Campos, G.M. Early small bowel obstruction after laparoscopic gastric bypass: A surgical emergency. Surg. Obes. Relat. Dis. 2018, 14, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Rondelli, F.; Bugiantella, W.; Desio, M.; Vedovati, M.C.; Boni, M.; Avenia, N.; Guerra, A. Antecolic or Retrocolic Alimentary Limb in Laparoscopic Roux-en-Y Gastric Bypass? A Meta-Analysis. Obes. Surg. 2016, 26, 182–195. [Google Scholar] [CrossRef]
- Oor, J.E.; Goense, L.; Wiezer, M.J.; Derksen, W.J. Incidence and treatment of intussusception following Roux-en-Y gastric bypass: A systematic review and meta-analysis. Surg. Obes. Relat. Dis. 2021, 17, 1017–1028. [Google Scholar] [CrossRef]
- Al Harakeh, A.B.; Kallies, K.J.; Borgert, A.J.; Kothari, S.N. Bowel obstruction rates in antecolic/antegastric versus retrocolic/retrogastric Roux limb gastric bypass: A meta-analysis. Surg. Obes. Relat. Dis. 2016, 12, 194–198. [Google Scholar] [CrossRef]
- Alban, E.A.D.; García, C.A.; Ospina, L.M.; Munevar, H.E. Imaging after Bariatric Surgery: When Interpretation Is a Challenge, from Normal to Abnormal. Obes. Surg. 2018, 28, 2923–2931. [Google Scholar] [CrossRef]
- Paroz, A.; Calmes, J.M.; Giusti, V.; Suter, M. Internal Hernia after Laparoscopic Roux-en-Y Gastric Bypass for Morbid Obesity: A Continuous Challenge in Bariatric Surgery. Obes. Surg. 2006, 16, 1482–1487. [Google Scholar] [CrossRef]
- Lockhart, M.E.; Tessler, F.N.; Canon, C.L.; Smith, J.K.; Larrison, M.C.; Fineberg, N.S.; Roy, B.P.; Clements, R.H. Internal Hernia After Gastric Bypass: Sensitivity and Specificity of Seven CT Signs with Surgical Correlation and Controls. Am. J. Roentgenol. 2007, 188, 745–750. [Google Scholar] [CrossRef]
- Reginelli, A.; Mandato, Y.; Solazzo, A.; Berritto, D.; Iacobellis, F.; Grassi, R. Errors in the Radiological Evaluation of the Alimentary Tract: Part II. Semin. Ultrasound CT MRI 2012, 33, 308–317. [Google Scholar] [CrossRef] [Green Version]
- Iannuccilli, J.; Grand, D.; Murphy, B.; Evangelista, P.; Roye, G.; Mayo-Smith, W. Sensitivity and specificity of eight CT signs in the preoperative diagnosis of internal mesenteric hernia following Roux-en-Y gastric bypass surgery. Clin. Radiol. 2009, 64, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Goudsmedt, F.; Deylgat, B.; Coenegrachts, K.; Van De Moortele, K.; Dillemans, B. Internal Hernia After Laparoscopic Roux-en-Y Gastric Bypass: A Correlation Between Radiological and Operative Findings. Obes. Surg. 2015, 25, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Duane, T.M.; Wohlgemuth, S.; Ruffin, K. Intussusception after Roux-en-Y gastric bypass. Am. Surg. 2000, 66, 82–84. [Google Scholar] [CrossRef]
- Somma, F.; Faggian, A.; Serra, N.; Gatta, G.; Iacobellis, F.; Berritto, D.; Reginelli, A.; Di Mizio, V.; Cappabianca, S.; Di Mizio, R.; et al. Bowel intussusceptions in adults: The role of imaging. Radiol. Med. 2015, 120, 105–117. [Google Scholar] [CrossRef]
- Lee, W.J.; Yu, P.J.; Wang, W.; Chen, T.C.; Wei, P.L.; Huang, M.T. Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: A prospective randomized controlled clinical trial. Ann. Surg. 2005, 242, 20. [Google Scholar] [CrossRef] [PubMed]
- Kular, K.S.; Manchanda, N.; Rutledge, R. A 6-year experience with 1,054 mini-gastric bypasses- first study from Indian subcontinent. Obes. Surg. 2014, 24, 1430–1435. [Google Scholar] [CrossRef]
- Clarke, M.G.; Wong, K.; Pearless, L.; Booth, M. Laparoscopic Silastic Ring Mini-gastric Bypass: A Single Centre Experience. Obes. Surg. 2013, 23, 1852–1857. [Google Scholar] [CrossRef]
- Mahawar, K.; Kumar, P.; Carr, W.; Jennings, N.; Schroeder, N.; Balupuri, S.; Small, P. Current status of mini-gastric bypass. J. Minimal Access Surg. 2016, 12, 305–310. [Google Scholar] [CrossRef]
- Genser, L.; Carandina, S.; Soprani, A. Petersen’s internal hernia complicating a laparoscopic omega loop gastric bypass. Surg. Obes. Relat. Dis. 2015, 11, e33–e34. [Google Scholar] [CrossRef] [Green Version]
- Liagre, A.; Benois, M.; Queralto, M.; Boudrie, H.; Van Haverbeke, O.; Juglard, G.; Martini, F.; Petrucciani, N. Ten-year outcome of one-anastomosis gastric bypass with a biliopancreatic limb of 150 cm versus Roux-en-Y gastric bypass: A single-institution series of 940 patients. Surg. Obes. Relat. Dis. 2022, 18, 1228–1238. [Google Scholar] [CrossRef]
- Scavone, G.; Caltabiano, D.C.; Gulino, F.; Raciti, M.V.; Giarrizzo, A.; Biondi, A.; Piazza, L.; Scavone, A. Laparoscopic mini/one anastomosis gastric bypass: Anatomic features, imaging, efficacy and postoperative complications. Updat. Surg. 2020, 72, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Musella, M.; Susa, A.; Manno, E.; De Luca, M.; Greco, F.; Raffaelli, M.; Cristiano, S.; Milone, M.; Bianco, P.; Vilardi, A.; et al. Complications Following the Mini/One Anastomosis Gastric Bypass (MGB/OAGB): A Multi-institutional Survey on 2678 Patients with a Mid-term (5 Years) Follow-up. Obes. Surg. 2017, 27, 2956–2967. [Google Scholar] [CrossRef] [PubMed]
- Scavone, G.; Castelli, F.; Caltabiano, D.C.; Raciti, M.V.; Ini’, C.; Basile, A.; Piazza, L.; Scavone, A. Imaging features in management of laparoscopic mini/one anastomosis gastric bypass post-surgical complications. Heliyon 2021, 7, e07705. [Google Scholar] [CrossRef] [PubMed]























Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacobellis, F.; Dell’Aversano Orabona, G.; Brillantino, A.; Di Serafino, M.; Rengo, A.; Crivelli, P.; Romano, L.; Scaglione, M. Common, Less Common, and Unexpected Complications after Bariatric Surgery: A Pictorial Essay. Diagnostics 2022, 12, 2637. https://doi.org/10.3390/diagnostics12112637
Iacobellis F, Dell’Aversano Orabona G, Brillantino A, Di Serafino M, Rengo A, Crivelli P, Romano L, Scaglione M. Common, Less Common, and Unexpected Complications after Bariatric Surgery: A Pictorial Essay. Diagnostics. 2022; 12(11):2637. https://doi.org/10.3390/diagnostics12112637
Chicago/Turabian StyleIacobellis, Francesca, Giuseppina Dell’Aversano Orabona, Antonio Brillantino, Marco Di Serafino, Alessandro Rengo, Paola Crivelli, Luigia Romano, and Mariano Scaglione. 2022. "Common, Less Common, and Unexpected Complications after Bariatric Surgery: A Pictorial Essay" Diagnostics 12, no. 11: 2637. https://doi.org/10.3390/diagnostics12112637