
Construction and Validation of Mortality Risk Nomograph Model for Severe/Critical Patients with COVID-19
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Data
2.1.1. Inclusion Criteria
Enrollment Criteria for Patients in Wuhan
Enrollment Criteria for Patients in Shanghai
2.1.2. Exclusion Criteria
2.2. Data Collection and Grouping
2.3. Statistical methods
3. Results
3.1. Analysis of Baseline Data of Patients
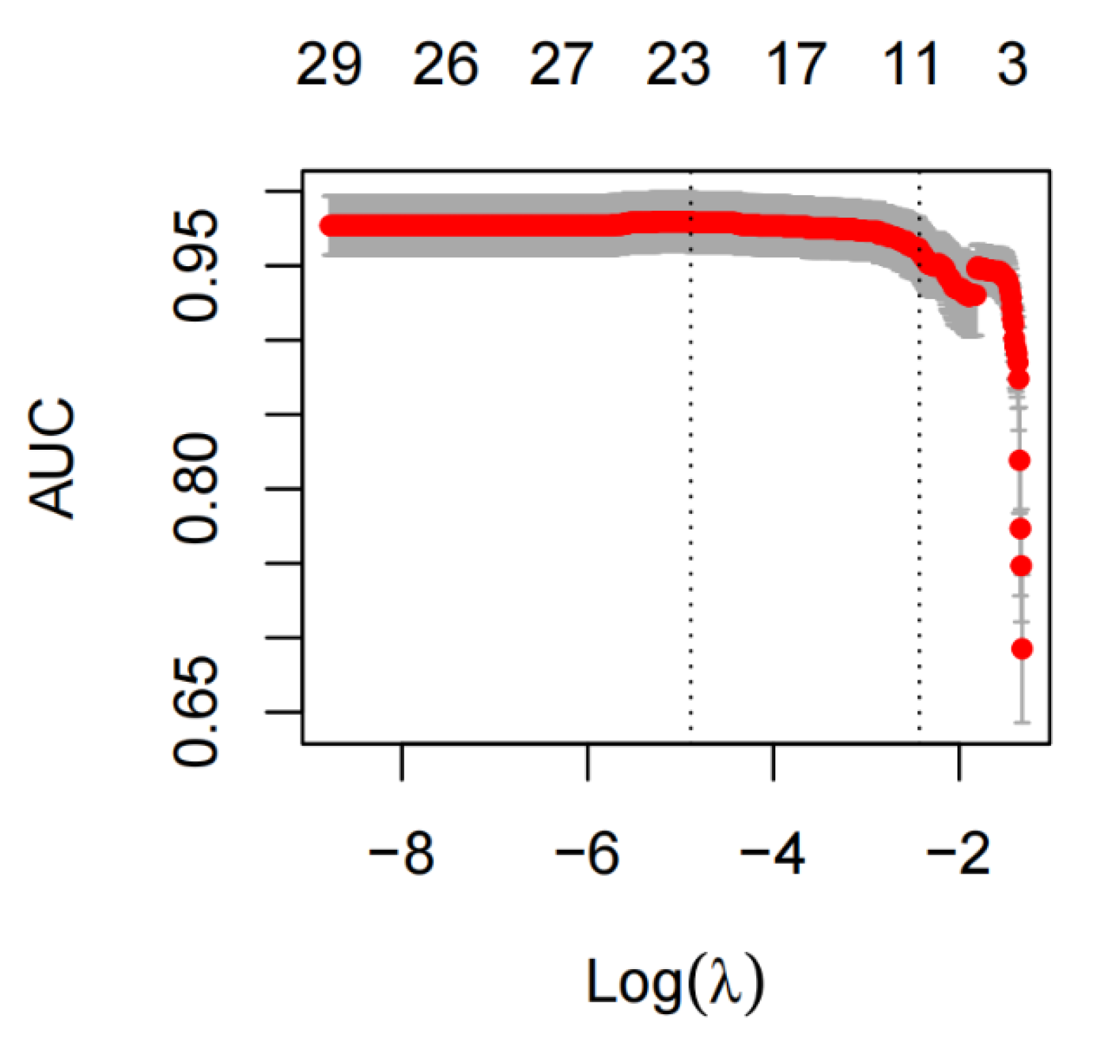
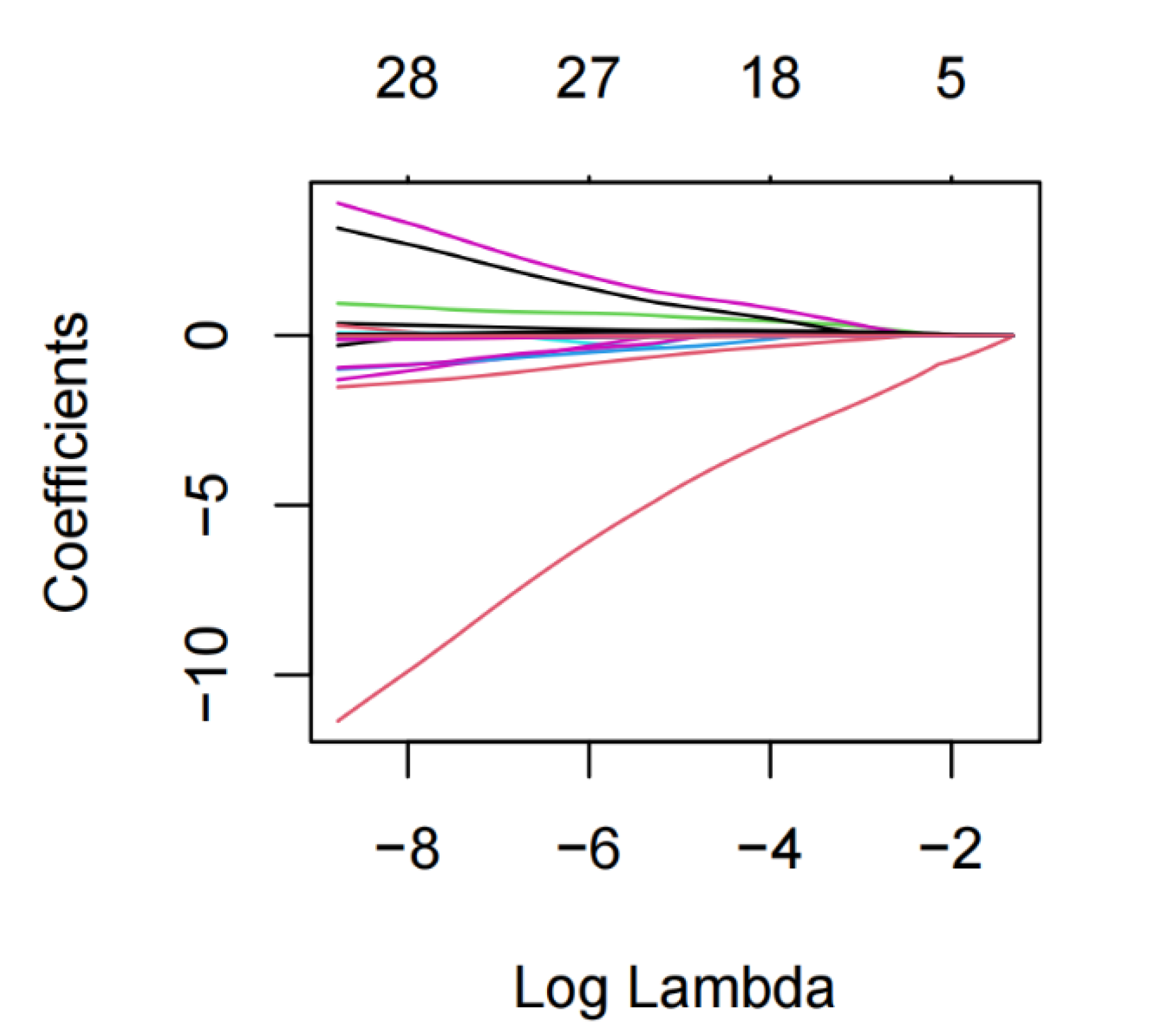
3.2. Lasso and Logistic Regression Analysis
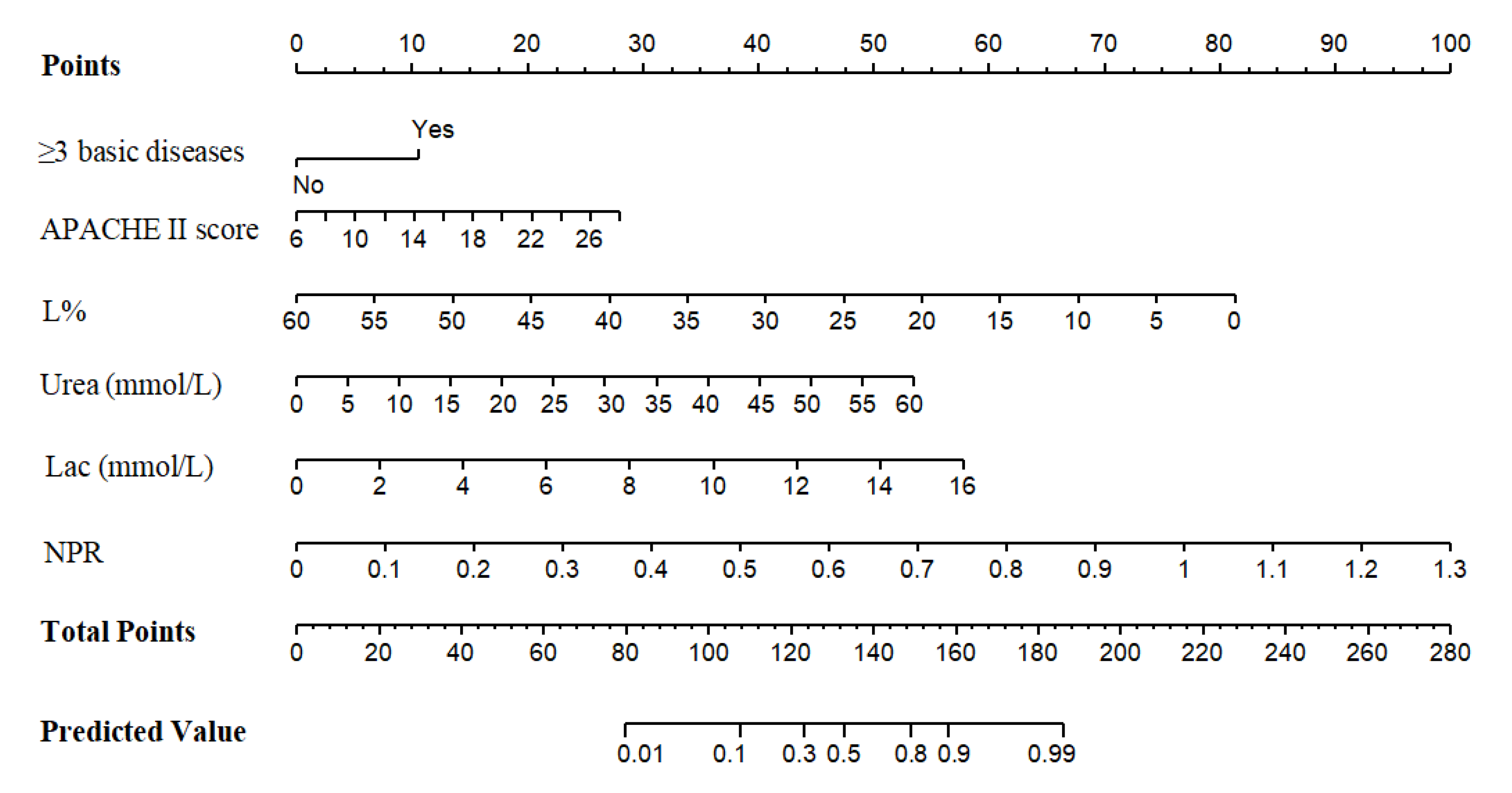
3.3. Establishment of Nomogram Model
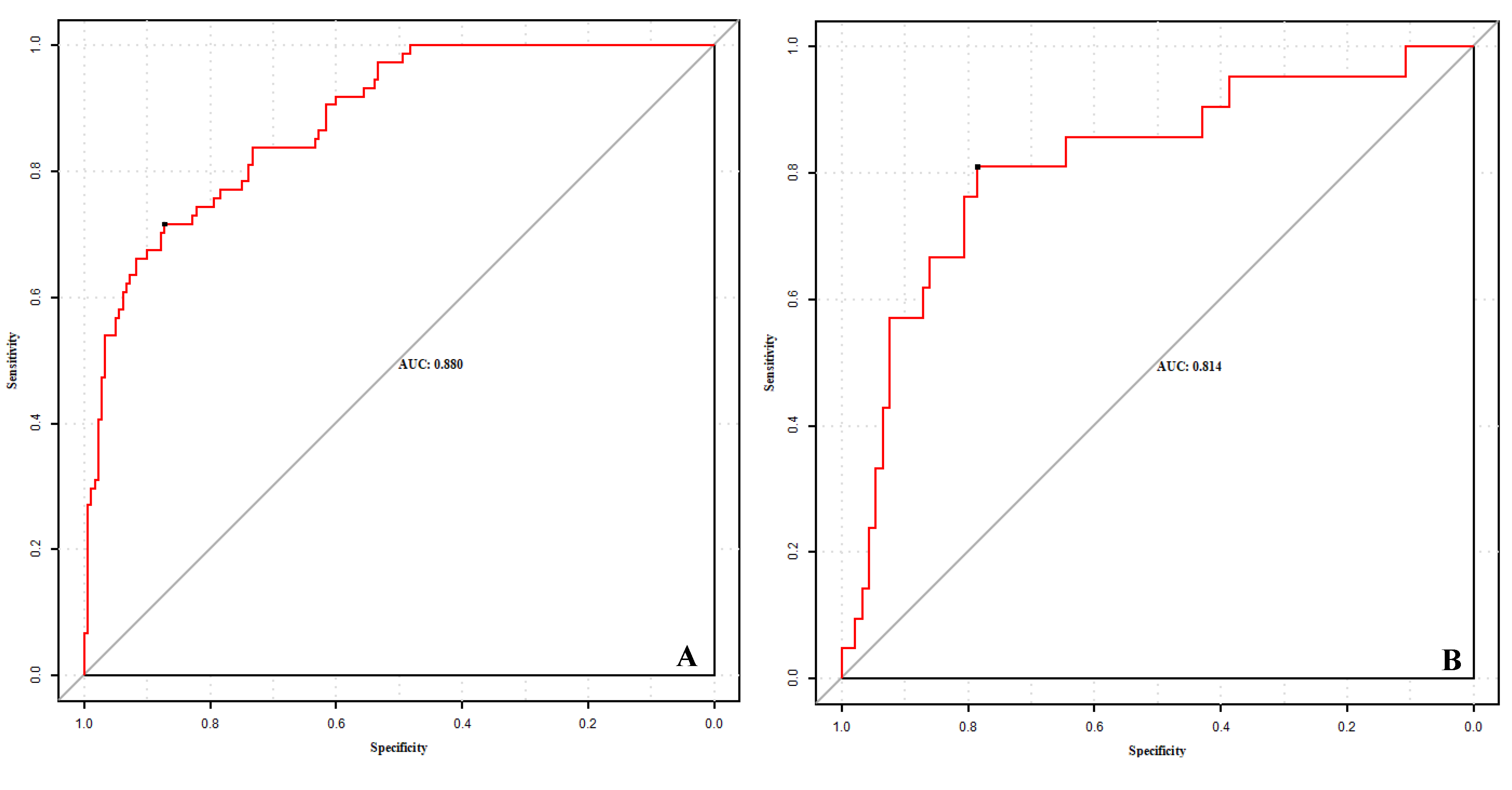
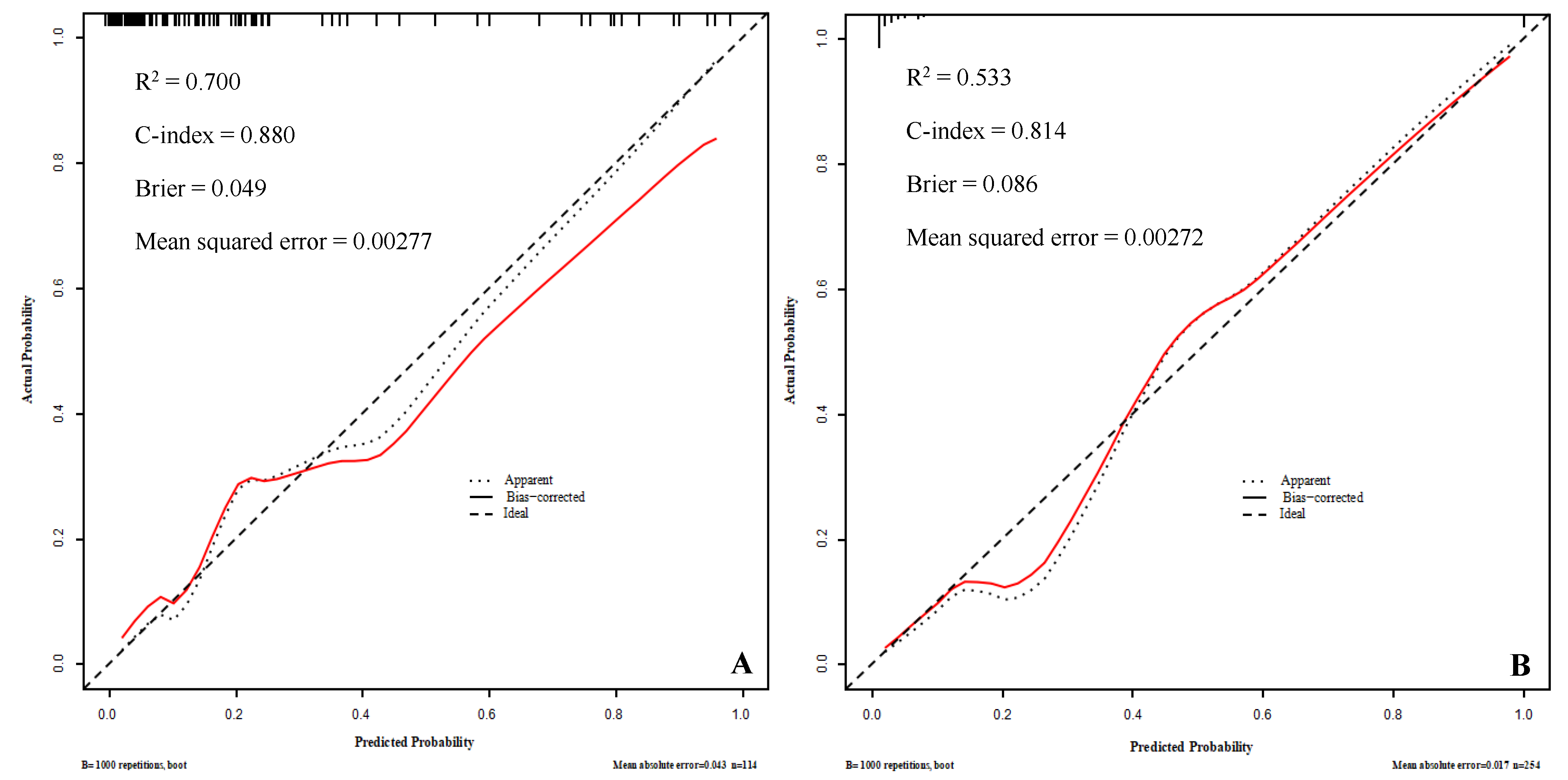
3.4. Internal and External Validation of the Model
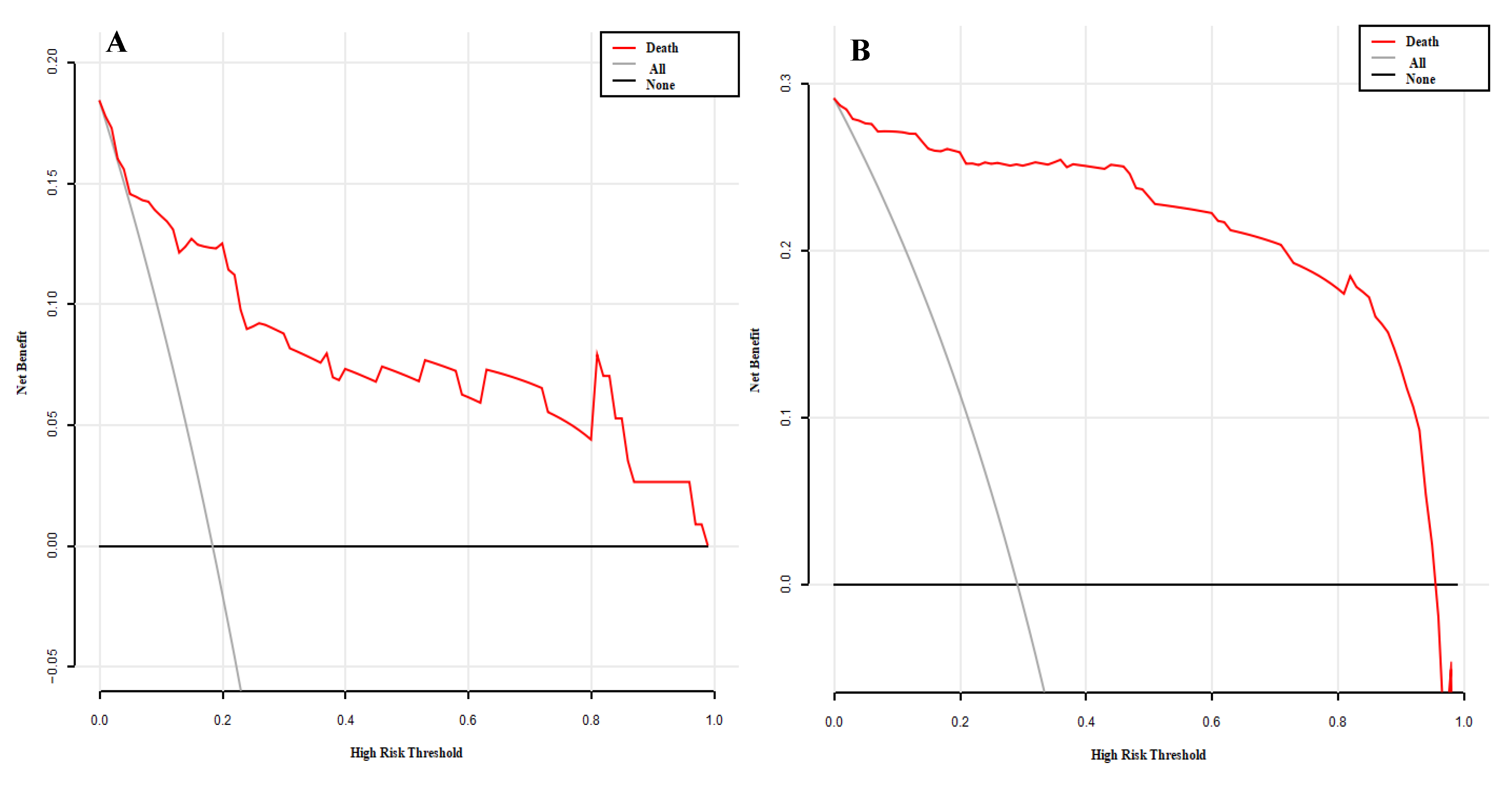
3.5. Clinical Decision Curve Analysis (Figure 6)

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Song, P.; Karako, T. COVID-19: Real-time dissemination of scientific information to fight a public health emergency of international concern. Biosci. Trends 2020, 14, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Song, Q.Q.; Zhao, H.; Fang, L.Q.; Liu, W.; Zheng, C.; Zhang, Y. Estimation of epidemiological parameters of early infectious diseases of COVID-19. Chin. J. Epidemiol. 2020, 41, 461–465. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Berenguer, J.; Borobia, A.M.; Ryan, P.; Rodríguez-Baño, J.; Bellón, J.M.; Jarrín, I.; Carratalà, J.; Pachón, J.; Carcas, A.J.; Yllescas, M.; et al. Development and validation of a prediction model for 30-day mortality in hospitalised patients with COVID-19: The COVID-19 SEIMC score. Thorax 2021, 76, 920–929. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Bahena-López, J.P.; Antonio-Villa, N.E.; Vargas-Vázquez, A.; González-Díaz, A.; Márquez-Salinas, A.; Fermín-Martínez, C.A.; Naveja, J.J.; Aguilar-Salinas, C.A. Predicting Mortality Due to SARS-CoV-2: A Mechanistic Score Relating Obesity and Diabetes to COVID-19 Outcomes in Mexico. J. Clin. Endocrinol. Metab. 2020, 105, dgaa346. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Du, H.; Li, J.; Wang, Y.; Wu, X.; Wang, C.; Zhang, Y.; Zhang, G.; Zhao, Y.; Kang, W.; et al. Early prediction and identification for severe patients during the pandemic of COVID-19: A severe COVID-19 risk model constructed by multivariate logistic regression analysis. J. Glob. Health 2020, 10, 020510. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients with COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- People’s Medical Publishing House (PMPH). Guidance for Corona Virus Disease 2019: Prevention, Control, Diagnosis and Management; National Health Commission (NHC): Beijing, China, 2020; ISBN 978-7-117-29817-9.
- General Office of the National Health Commission. Notice on Printing and Distributing the Diagnosis and treatment Plan for COVID-19 (Trial Version 9) [EB/OL]; State Health Commission of the People’s Republic of China: Beijing, China. Available online: http://www.nhc.gov.cn/yzygj/s7653p/202203/b74ade1ba4494583805a3d2e40093d88.shtml (accessed on 14 March 2022).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Gu, H.Q.; Liu, Y.; Zhang, G.; Yang, H.; Hu, H.; Lu, C.; Li, Y.; Wang, L.; Zhao, Y.; et al. A model to predict the risk of mortality in severely ill COVID-19 patients. Comput. Struct. Biotechnol. J. 2021, 19, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Eur. Urol. 2015, 67, 1142–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.W.; Cui, L.P.; Liu, Z.Y.; Luo, X.L. Regularized sparse model. Chin. J. Comput. 2015, 38, 1307–1325. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-Cov-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Yang, J.Z.; Bai, W.H.; Li, Z.Y.; Sun, L.F.; Yan, J.J.; Zhou, C.L.; Tang, B.P. Prognostic value of serum amyloid A in patients with COVID-19. Infection 2020, 48, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Training Set (n = 254) | Validation Set (n = 113) | ||||||
|---|---|---|---|---|---|---|---|---|
| Death Group (n = 74) | Survival Group (n = 180) | Z/χ2 Value | p-Value | Death Group (n = 21) | Survival Group (n = 92) | Z/χ2 Value | p-Value | |
| Male/Female (cases) | 48/26 | 102/78 | 1.458 | 0.227 | 12/9 | 43/49 | 0.714 | 0.389 |
| Age [n (%)] | 70.0 (56.8, 78.5) | 62.0 (69.0, 77.0) | −4.002 | <0.001 | 86.0 (76.5, 91.0) | 82.0 (72.0, 89.0) | −1.332 | 0.183 |
| 18–65 Years | 24 (31.6%) | 88 (48.9%) | 6.506 | 0.011 | 4 (19.0%) | 65 (70.7%) | 19.150 | <0.001 |
| ≥65 Years | 50 (68.4%) | 92 (51.1%) | 17 (81.0%) | 27 (29.3%) | ||||
| COVID-19 Severe/Critical (cases) | 12/62 | 107/73 | 39.354 | <0.001 | 10/11 | 79/13 | 14.954 | <0.001 |
| Course of Disease [d, M (QL, QU)] | 16.0 (11.8, 24.0) | 28.0 (17.0, 42.0) | −4.662 | <0.001 | 11.0 (7.0, 15.0) | 8.0 (7.0, 13.5) | −0.836 | 0.403 |
| Time of Nucleic Acid Turning Negative (d) | 12.0 (10.0, 19.0) | 13.0 (9.0, 19.0) | −0.027 | 0.979 | 6.5 (5.0, 7.3) | 5.0 (5.0, 7.0) | −1.416 | 0.157 |
| Clinical Manifestation [n (%)] | ||||||||
| Fever | 60 (81.1%) | 156 (86.7%) | 1.286 | 0.257 | 14 (66.7%) | 39 (42.4%) | 4.046 | 0.044 |
| Cough | 36 (48.6%) | 123 (68.3%) | 8.679 | 0.003 | 15 (71.4%) | 58 (63.0%) | 0.526 | 0.468 |
| Weakness | 23 (31.1%) | 77 (42.8%) | 3.006 | 0.083 | 8 (38.1%) | 28 (30.4%) | 0.462 | 0.497 |
| Diarrhea | 10 (13.5%) | 18 (10.0%) | 0.660 | 0.417 | 1 (4.8%) | 3 (3.3%) | 0.000 a | 1.000 |
| Dyspnea | 25 (33.8%) | 30 (16.7%) | 9.057 | 0.003 | 4 (19.0%) | 9 (9.8%) | 1.442 | 0.230 |
| Consciousness Disorder | 5 (6.8%) | 6 (3.3%) | 1.483 | 0.223 | 10 (47.6%) | 20 (21.7%) | 5.872 | 0.015 |
| Other | 7 (9.5%) | 15 (8.3%) | 0.084 | 0.772 | 2 (9.5%) | 3 (3.3%) | 0.451 a | 0.502 |
| Comorbidities [n (%)] | ||||||||
| Chronic Lung Disease | 11 (14.9%) | 18 (10.0%) | 1.227 | 0.268 | 18 (85.7%) | 46 (48.9%) | 9.407 | 0.002 |
| Hypertension | 30 (40.5%) | 63 (35.0%) | 0.694 | 0.405 | 11 (52.4%) | 51 (55.4%) | 0.064 | 0.800 |
| Diabetes | 13 (24.1%) | 31 (17.2%) | 1.277 | 0.258 | 8 (38.1%) | 26 (28.3%) | 0.786 | 0.375 |
| Cardiovascular Disease | 11 (14.9%) | 24 (13.3%) | 0.104 | 0.748 | 12 (57.1%) | 31 (33.7%) | 3.988 | 0.046 |
| Cerebrovascular Disease | 7 (9.5%) | 15 (8.3%) | 0.084 | 0.772 | 10 (47.6%) | 28 (30.4%) | 2.262 | 0.133 |
| Chronic Kidney Disease | 12 (16.2%) | 15 (8.3%) | 3.430 | 0.064 | 11 (52.4%) | 14 (15.2%) | 13.706 | <0.001 |
| Malignancy | 9 (12.2%) | 24 (13.3%) | 0.064 | 0.801 | 2 (9.5%) | 3 (3.3%) | 0.451 a | 0.502 |
| ≥3 Basic Diseases | 14 (18.9%) | 17 (9.4%) | 4.393 | 0.036 | 13 (61.9%) | 21 (22.8%) | 12.412 | <0.001 |
| Treatment [n (%)] | ||||||||
| Mechanical Ventilation | 31 (41.9%) | 18 (10.0%) | 34.257 | <0.001 | 14 (66.7%) | 19 (20.7%) | 17.509 | <0.001 |
| ECMO | 3 (4.1%) | 4 (2.2) | 0.151 a | 0698 | 2 (9.5%) | 0 (0.0%) | - | 0.033 b |
| APACHE II score [points, M (QL, QU)] | 17.0 (16.0, 21.0) | 16.0 (15.0, 18.0) | −3.495 | <0.001 | 20.0 (17.5, 26.0) | 16.0 (12.0, 18.0) | −4.843 | <0.001 |
| Characteristic [M (QL, QU)] | Training Set (n = 254) | Validation Set (n = 113) | ||||||
|---|---|---|---|---|---|---|---|---|
| Death Group (n = 74) | Survival Group (n = 180) | Z Value | p-Value | Death Group (n = 21) | Survival Group (n = 92) | Z Value | p-Value | |
| WBC (×109/L) | 13.3 (9.9, 17.2) | 5.7 (4.2, 7.7) | −9.407 | <0.001 | 9.9 (6.8, 14.2) | 6.1 (4.5, 10.8) | −2.160 | 0.031 |
| N% | 88.6 (82.3, 93.9) | 73.2 (62.2, 82.6) | −7.734 | <0.001 | 83.0 (65.2, 87.0) | 79.7 (64.3, 88.2) | −0.212 | 0.832 |
| N (×109/L) | 12,0 (8.1, 16.5) | 4.3 (2.6, 6.6) | −9.496 | <0.001 | 6.9 (4.3, 10.5) | 4.7 (2.7, 9.5) | −1.725 | 0.084 |
| L (×109/L) | 0.7 (0.4, 1.1) | 0.9 (0.6, 1.2) | −3.393 | 0.001 | 0.6 (0.3, 0.9) | 0.8 (0.5, 1.4) | −0.793 | 0.428 |
| L% | 5.1 (2.9, 7.7) | 12.7 (8.4, 18.6) | −8.802 | <0.001 | 12.0 (6.9, 21.6) | 14.1 (9.7, 20.6) | −0.793 | 0.428 |
| NLR | 18.0 (9.3, 34.1) | 4.3 (2.4, 8.0) | −9.115 | <0.001 | 10.0 (5.0, 20.9) | 5.4 (2.0, 15.8) | −2.361 | 0.018 |
| Hb (g/L) | 108.0 (89.0, 127.3) | 124.0 (111.0, 135.0) | −4.273 | <0.001 | 99.0 (86.0, 125.0) | 121.0 (102.0, 136.0) | −2.000 | 0.046 |
| PLT (×109/L) | 131.5 (64.3, 203.0) | 191.0 (143.0, 257.0) | −4.648 | <0.001 | 115.0 (79.5, 187.0) | 183.0 (133.0, 231.0) | −2.592 | 0.010 |
| NPR | 0.2 (0.1, 0.4) | 0.02 (0.01, 0.03) | −10.018 | <0.001 | 0.05 (0.03, 0.13) | 0.03 (0.02, 0.05) | −3.088 | 0.002 |
| CRP (mg/L) | 31.4 (11.8, 70.6) | 12.6 (0.5, 61.9) | −2.612 | 0.009 | 95.0 (27.5, 171.0) | 25.4 (7.1, 88.0) | −2.394 | 0.017 |
| SAA (mg/L) | 134.7 (63.6, 200.0) | 47.7 (11.5, 126.9) | −4.426 | <0.001 | 146.2 (52.7, 248.1) | 82.0 (10.4, 225.1) | −1.601 | 0.109 |
| PCT (μg/L) | 2.3 (0.8, 5.6) | 0.1 (0.04, 0.19) | −10.414 | <0.001 | 1.6 (0.3, 8.0) | 0.5 (0.4, 1.0) | −4.493 | <0.001 |
| ALT (U/L) | 51.0 (21.8, 121.0) | 30.0 (21.0, 51.0) | −3.583 | <0.001 | 26.0 (14.0, 40.5) | 19.0 (14.5, 29.5) | −1.174 | 0.240 |
| AST (U/L) | 81.0 (40.0, 159.8) | 33.0 (23.0, 45.8) | −7.115 | <0.001 | 41.0 (23.5, 52.5) | 30.0 (20.5, 49.5) | −1.324 | 0.185 |
| TBIL (μmol/L) | 21.0 (16.0, 37.1) | 10.4 (8.4, 15.6) | −7.012 | <0.001 | 14.7 (11.5, 16.9) | 11.2 (9.3, 16.6) | −1.590 | 0.112 |
| DBIL (μmol/L) | 10.7 (7.4, 21.0) | 4.0 (3.0, 5.8) | −8.266 | <0.001 | 5.6 (3.2, 7.8) | 2.8 (2.2, 3.9) | −3.573 | <0.001 |
| ALB (g/L) | 30.2 (27.9, 33.2) | 36.0 (32.8, 38.4) | −7.728 | <0.001 | 30.0 (28.5, 33.5) | 37.0 (30.0, 39.0) | −3.094 | 0.002 |
| Urea (mmol/L) | 16.7 (9.1, 31.2) | 4.9 (3.9, 7.3) | −9.112 | <0.001 | 12.3 (7.7, 21.0) | 8.3 (5.6, 11.7) | −3.023 | 0.003 |
| Cr (μmol/L) | 121.5 (62.8, 337.8) | 61.0 (51.0, 78.0) | −5.987 | <0.001 | 102.0 (69.5, 137.0) | 77.0 (63.0, 105.5) | −2.632 | 0.008 |
| eGFR (ml/min) | 51.7 (15.3, 93.2) | 98.9 (85.9, 107.4) | −7.383 | <0.001 | 56.0 (39.5, 80.0) | 80.0 (54.0, 91.5) | −2.358 | 0.018 |
| Lac (mmol/L) | 2.9 (2.1, 4.2) | 1.9 (1.4, 2.5) | −6.942 | <0.001 | 2.6 (2.1, 4.1) | 1.5 (1.1, 2.0) | −4.442 | <0.001 |
| BNP (ng/L) | 1619.0 (392.1, 2196.5) | 326.9 (133.7, 682.2) | −6.314 | <0.001 | 638.0 (197.0, 899.0) | 115.0 (45.5, 238.0) | −4.543 | <0.001 |
| cTnI (gl/L) | 0.7 (0.1, 3.5) | 0.1 (0.1, 0.3) | −3.647 | <0.001 | 0.2 (0.1, 0.3) | 0.1 (0.1, 0.2) | −3.583 | <0.001 |
| PT (s) | 12.4 (12.6, 16.8) | 13.0 (11.8, 83.8) | −0.132 | 0.895 | 12.9 (12.3, 13.3) | 11.7 (11.0, 12.4) | −3.797 | <0.001 |
| APTT (s) | 32.0 (26.2, 36.3) | 28.9 (26.2, 32.6) | −2.923 | 0.003 | 33.7 (27.3, 36.3) | 30.6 (28.2, 34.8) | −0.716 | 0.474 |
| D-dimer (mg/L) | 6.4 (2.3, 22.6) | 1.4 (0.6, 4.1) | −6.524 | <0.001 | 4.5 (1.7, 8.4) | 1.1 (0.5, 3.4) | −3.827 | <0.001 |
| Variable | β | SE | Wald | p | OR | 95%CI |
|---|---|---|---|---|---|---|
| Age ≥ 65 | 1.424 | 0.74 | 3.697 | 0.054 | 4.153 | 0.973~17.728 |
| ≥3 Basic Diseases | 1.732 | 0.757 | 5.242 | 0.022 | 15.653 | 1.283~24.904 |
| APACHE II Score | 0.190 | 0.095 | 4.012 | 0.045 | 1.209 | 1.004~1.456 |
| L% | −0.253 | 0.079 | 10.253 | 0.001 | 0.777 | 0.665~0.907 |
| Urea | 0.177 | 0.060 | 8.715 | 0.003 | 1.193 | 1.061~1.342 |
| D-dimer | 0.002 | 0.019 | 0.009 | 0.925 | 1.002 | 0.966~1.039 |
| Lac | 0.750 | 0.221 | 11.491 | 0.001 | 2.117 | 1.372~3.266 |
| NPR | 11.333 | 4.960 | 5.220 | 0.022 | 8.056 | 5.008~13.819 |
| NLR | −0.001 | 0.007 | 0.048 | 0.826 | 0.999 | 0.985~1.012 |
| WBC | 0.032 | 0.074 | 0.183 | 0.669 | 1.032 | 0.893~1.193 |
| cTnI | −0.029 | 0.013 | 4.961 | 0.056 | 0.971 | 0.947~0.997 |
| Constant | −8.309 | 1.989 | 17.448 | 0.000 | 0.000 | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, L.; Bai, W.-H.; Yang, J.-J.; Chou, P.; Ning, W.-S.; Cai, Q.; Zhou, C.-L. Construction and Validation of Mortality Risk Nomograph Model for Severe/Critical Patients with COVID-19. Diagnostics 2022, 12, 2562. https://doi.org/10.3390/diagnostics12102562
Cheng L, Bai W-H, Yang J-J, Chou P, Ning W-S, Cai Q, Zhou C-L. Construction and Validation of Mortality Risk Nomograph Model for Severe/Critical Patients with COVID-19. Diagnostics. 2022; 12(10):2562. https://doi.org/10.3390/diagnostics12102562
Chicago/Turabian StyleCheng, Li, Wen-Hui Bai, Jing-Jing Yang, Peng Chou, Wan-Shan Ning, Qiang Cai, and Chen-Liang Zhou. 2022. "Construction and Validation of Mortality Risk Nomograph Model for Severe/Critical Patients with COVID-19" Diagnostics 12, no. 10: 2562. https://doi.org/10.3390/diagnostics12102562