
The Value of Deep Learning Image Reconstruction in Improving the Quality of Low-Dose Chest CT Images

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Image Acquisition
2.3. Algorithm Training and Image Reconstruction
2.4. Radiation Dose
2.5. Objective Image Analysis
2.6. Subjective Image Analysis
2.7. Statistical Analysis
3. Results
3.1. Radiation Dose
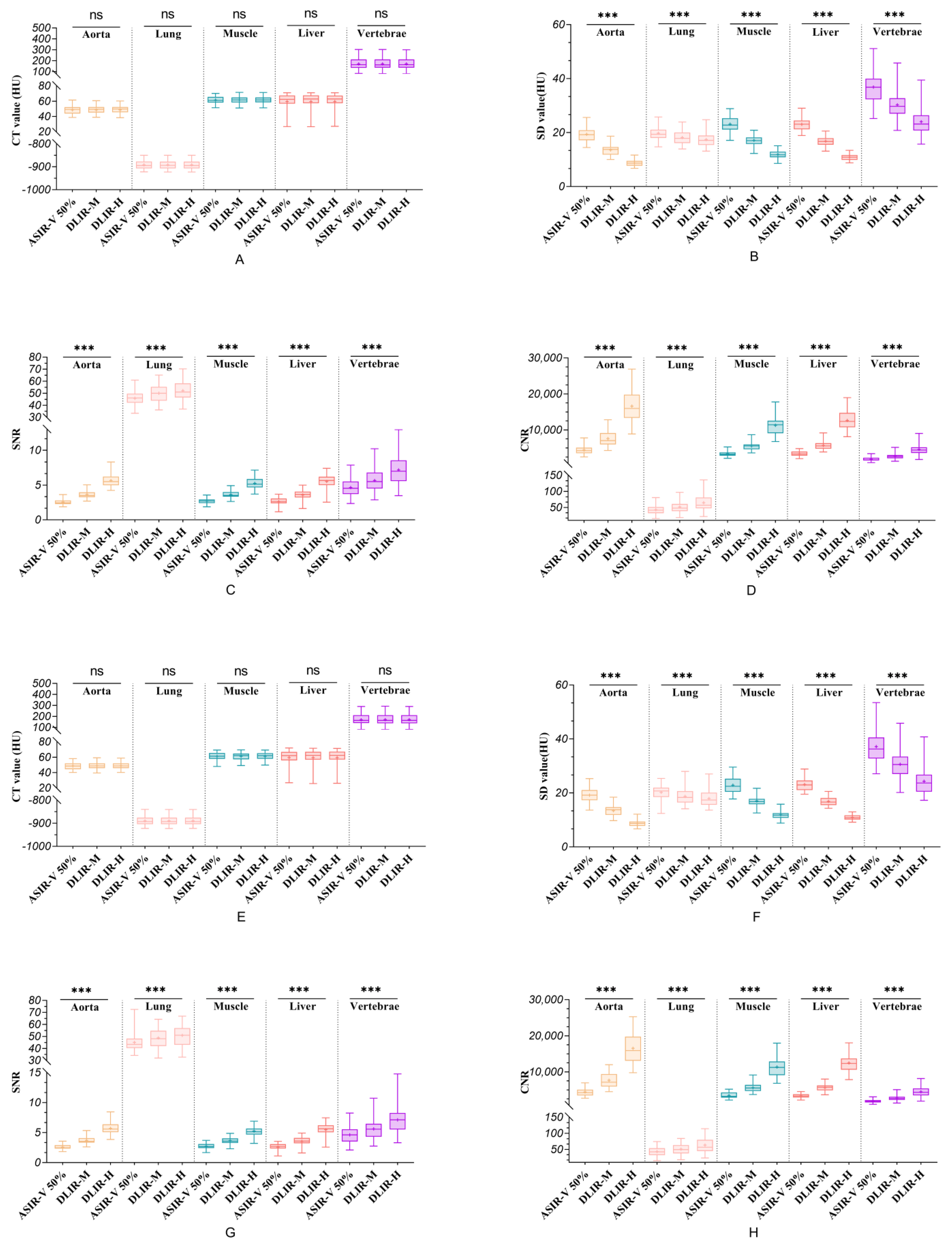
3.2. Objective Analysis
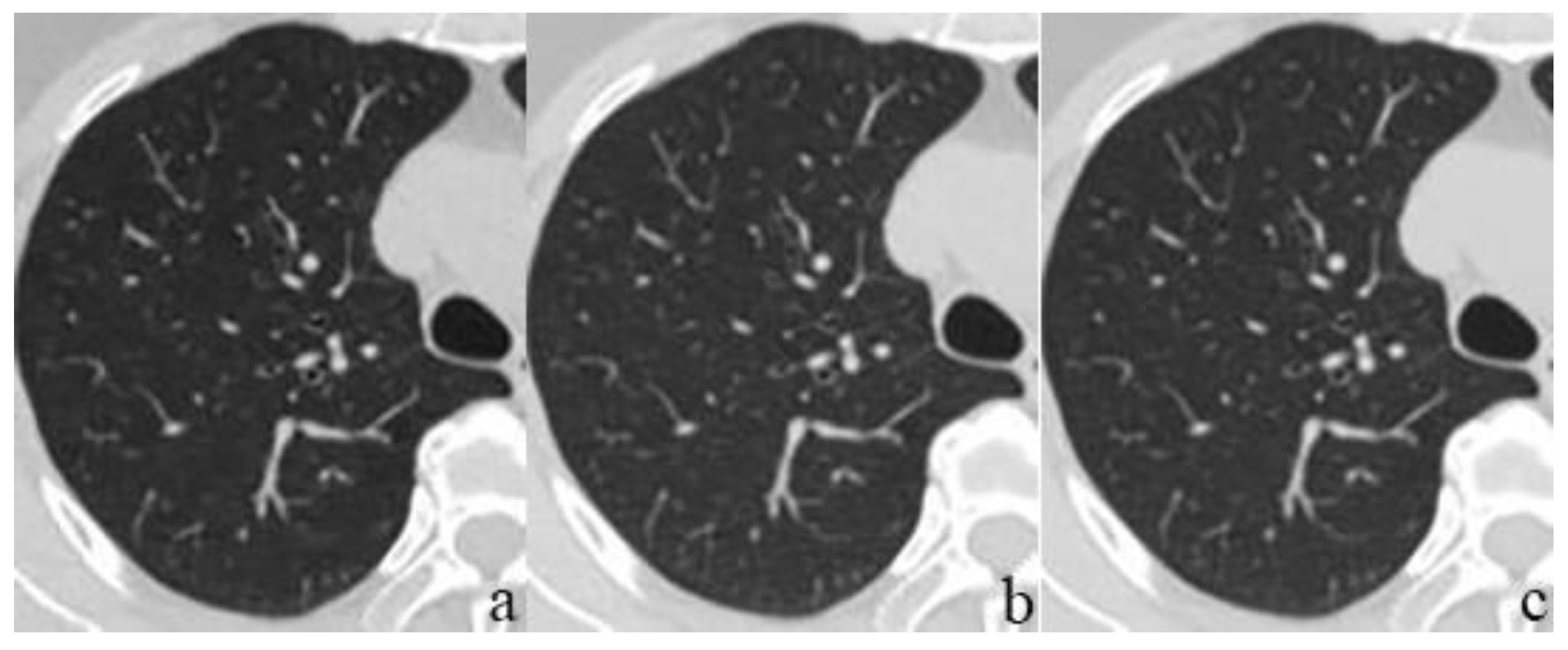
3.3. Subjective Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Research Team; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Goldman, L.W. Principles of CT: Radiation dose and image quality. J. Nucl. Med. Technol. 2007, 35, 213–225. [Google Scholar] [CrossRef] [Green Version]
- Baskan, O.; Erol, C.; Ozbek, H.; Paksoy, Y. Effect of radiation dose reduction on image quality in adult head CT with noise-suppressing reconstruction system with a 256 slice MDCT. J. Appl. Clin. Med. Phys. 2015, 16, 5360. [Google Scholar] [CrossRef]
- Singh, S.; Kalra, M.K.; Gilman, M.D.; Hsieh, J.; Pien, H.H.; Digumarthy, S.R.; Shepard, J.A. Adaptive statistical iterative reconstruction technique for radiation dose reduction in chest CT: A pilot study. Radiology 2011, 259, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Desai, G.S.; Uppot, R.N.; Yu, E.W.; Kambadakone, A.R.; Sahani, D.V. Impact of iterative reconstruction on image quality and radiation dose in multidetector CT of large body size adults. Eur. Radiol. 2012, 22, 1631–1640. [Google Scholar] [CrossRef]
- Geyer, L.L.; Schoepf, U.J.; Meinel, F.G.; Nance, J.W., Jr.; Bastarrika, G.; Leipsic, J.A.; Paul, N.S.; Rengo, M.; Laghi, A.; De Cecco, C.N. State of the art: Iterative CT reconstruction techniques. Radiology 2015, 276, 339–357. [Google Scholar] [CrossRef]
- Padole, A.; Ali Khawaja, R.D.; Kalra, M.K.; Singh, S. CT radiation dose and iterative reconstruction techniques. AJR Am. J. Roentgenol. 2015, 204, W384–W392. [Google Scholar] [CrossRef]
- Akagi, M.; Nakamura, Y.; Higaki, T.; Narita, K.; Honda, Y.; Zhou, J.; Yu, Z.; Akino, N.; Awai, K. Deep learning reconstruction improves image quality of abdominal ultra-high-resolution CT. Eur. Radiol. 2019, 29, 6163–6171. [Google Scholar] [CrossRef] [PubMed]
- Higaki, T.; Nakamura, Y.; Tatsugami, F.; Nakaura, T.; Awai, K. Improvement of image quality at CT and MRI using deep learning. Jpn. J. Radiol. 2019, 37, 73–80. [Google Scholar] [CrossRef]
- Hsieh, J.; Liu, E.; Nett, B.; Tang, J.; Thibault, J.-B.; Sahney, S. A New Era of Image Reconstruction: TrueFidelityTM Technical White Paper on Deep Learning Image Reconstruction. 2019. Available online: https://www.semanticscholar.org/paper/A-new-era-of-image-reconstruction%3A-TrueFidelityTM-Hsieh-Liu/d0f8e1e8868e9f8ed22ad5972420139551552e91 (accessed on 20 August 2022).
- Greffier, J.; Hamard, A.; Pereira, F.; Barrau, C.; Pasquier, H.; Beregi, J.P.; Frandon, J. Image quality and dose reduction opportunity of deep learning image reconstruction algorithm for CT: A phantom study. Eur. Radiol. 2020, 30, 3951–3959. [Google Scholar] [CrossRef]
- Gordic, S.; Morsbach, F.; Schmidt, B.; Allmendinger, T.; Flohr, T.; Husarik, D.; Baumueller, S.; Raupach, R.; Stolzmann, P.; Leschka, S.; et al. Ultralow-dose chest computed tomography for pulmonary nodule detection: First performance evaluation of single energy scanning with spectral shaping. Investig. Radiol. 2014, 49, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Gulliksrud, K.; Stokke, C.; Martinsen, A.C. How to measure CT image quality: Variations in CT-numbers, uniformity and low contrast resolution for a CT quality assurance phantom. Phys. Med. 2014, 30, 521–526. [Google Scholar] [CrossRef]
- Bankier, A.A.; Kressel, H.Y. Through the Looking Glass revisited: The need for more meaning and less drama in the reporting of dose and dose reduction in CT. Radiology 2012, 265, 4–8. [Google Scholar] [CrossRef]
- American Association of Physicists in Medicine. Lung Cancer Screening CT Protocols Version 5.1. 2019. Available online: https://www.aapm.org/pubs/CTProtocols/documents/LungCancerScreeningCT.pdf (accessed on 13 October 2022).
- Zeng, W.; Zeng, L.M.; Xu, X.; Hu, S.X.; Liu, K.L.; Zhang, J.G.; Peng, W.L.; Xia, C.C.; Li, Z.L. Noise reduction effect of deep-learning-based image reconstruction algorithms in thin-section chest CT. Sichuan Da Xue Xue Bao Yi Xue Ban 2021, 52, 286–292. [Google Scholar] [CrossRef]
- Kim, J.H.; Yoon, H.J.; Lee, E.; Kim, I.; Cha, Y.K.; Bak, S.H. Validation of deep-learning image reconstruction for low-dose chest computed tomography scan: Emphasis on image quality and noise. Korean J. Radiol. 2021, 22, 131–138. [Google Scholar] [CrossRef]
- Lim, K.; Kwon, H.; Cho, J.; Oh, J.; Yoon, S.; Kang, M.; Ha, D.; Lee, J.; Kang, E. Initial phantom study comparing image quality in computed tomography using adaptive statistical iterative reconstruction and new adaptive statistical iterative reconstruction v. J. Comput. Assist. Tomogr. 2015, 39, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Yu, N.; Jia, Y.; Yu, Y.; Duan, H.; Han, D.; Ma, G.; Ren, C.; He, T. Assessment of noise reduction potential and image quality improvement of a new generation adaptive statistical iterative reconstruction (ASIR-V) in chest CT. Br. J. Radiol. 2018, 91, 20170521. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Liu, Z.; Hu, Z.; He, T.; Li, D.; Yu, N.; Jia, Y.; Shi, H. Clinical value of a new generation adaptive statistical iterative reconstruction (ASIR-V) in the diagnosis of pulmonary nodule in low-dose chest CT. Br. J. Radiol. 2019, 92, 20180909. [Google Scholar] [CrossRef]
- Wang, Y.N.; Du, Y.; Shi, G.F.; Wang, Q.; Li, R.X.; Qi, X.H.; Cai, X.J.; Zhang, X. A preliminary evaluation study of applying a deep learning image reconstruction algorithm in low-kilovolt scanning of upper abdomen. J. Xray Sci. Technol. 2021, 29, 687–695. [Google Scholar] [CrossRef]
- Sun, J.; Li, H.; Li, J.; Yu, T.; Li, M.; Zhou, Z.; Peng, Y. Improving the image quality of pediatric chest CT angiography with low radiation dose and contrast volume using deep learning image reconstruction. Quant. Imaging Med. Surg. 2021, 11, 3051–3058. [Google Scholar] [CrossRef]
- Cao, L.; Liu, X.; Li, J.; Qu, T.; Chen, L.; Cheng, Y.; Hu, J.; Sun, J.; Guo, J. A study of using a deep learning image reconstruction to improve the image quality of extremely low-dose contrast-enhanced abdominal CT for patients with hepatic lesions. Br. J. Radiol. 2021, 94, 20201086. [Google Scholar] [CrossRef]
- Cheng, Y.; Han, Y.; Li, J.; Fan, G.; Cao, L.; Li, J.; Jia, X.; Yang, J.; Guo, J. Low-dose CT urography using deep learning image reconstruction: A prospective study for comparison with conventional CT urography. Br. J. Radiol. 2021, 94, 20201291. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CT Value (HU) | ASIR-V 50% | DLIR-M | DLIR-H | p | p | ||
|---|---|---|---|---|---|---|---|
| ASIR-V 50% vs. DLIR-M | ASIR-V 50% vs. DLIR-H | DLIR-M vs. DLIR-H | |||||
| Aorta | |||||||
| ICC | 0.948 | 0.951 | 0.955 | ||||
| Reader 1 | 48.64 ± 5.47 | 48.76 ± 5.35 | 48.72 ± 5.36 | 0.515 † | 1.000 | 1.000 | 1.000 |
| Reader 2 | 48.64 ± 5.04 | 48.79 ± 4.99 | 48.78 ± 4.91 | 0.394 † | 0.891 | 1.000 | 1.000 |
| Lung | |||||||
| ICC | 0.960 | 0.958 | 0.961 | ||||
| Reader 1 | −891.66 ± 18.06 | −891.65 ± 17.82 | −891.63 ± 17.88 | 0.866 † | 1.000 | 1.000 | 1.000 |
| Reader 2 | −889.88 ± 19.30 | −890.00 ± 19.12 | −889.88 ± 19.14 | 0.622 † | 1.000 | 1.000 | 1.000 |
| Muscle | |||||||
| ICC | 0.926 | 0.921 | 0.925 | ||||
| Reader 1 | 61.55 ± 4.65 | 61.67 ± 4.90 | 61.66 ± 4.83 | 0.681 † | 1.000 | 1.000 | 1.000 |
| Reader 2 | 61.27 ± 4.81 | 61.21 ± 4.94 | 61.28 ± 4.83 | 0.804 † | 1.000 | 1.000 | 0.780 |
| Liver | |||||||
| ICC | 0.987 | 0.990 | 0.992 | ||||
| Reader 1 | 62.40 (10.82) | 62.90 (10.45) | 63.05 (10.03) | 0.717 ‡ | 1.000 | 1.000 | 1.000 |
| Reader 2 | 62.13 (11.08) | 62.46 (10.27) | 62.41 (10.20) | 0.763 ‡ | 1.000 | 1.000 | 1.000 |
| Vertebrae | |||||||
| ICC | 0.993 | 0.994 | 0.995 | ||||
| Reader 1 | 170.50 ± 52.68 | 170.69 ± 53.25 | 170.53 ± 53.03 | 0.662 † | 1.000 | 1.000 | 0.790 |
| Reader 2 | 170.15 ± 52.04 | 170.32 ± 52.91 | 170.23 ± 52.77 | 0.750 † | 1.000 | 1.000 | 1.000 |
| Noise (HU) | ASIR-V 50% | DLIR-M | DLIR-H | p | p | ||
|---|---|---|---|---|---|---|---|
| ASIR-V 50% vs. DLIR-M | ASIR-V 50% vs. DLIR-H | DLIR-M vs. DLIR-H | |||||
| Aorta | |||||||
| ICC | 0.921 | 0.934 | 0.932 | ||||
| Reader 1 | 19.35 ± 2.70 | 13.58 ± 1.96 | 8.74 ± 1.22 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 19.16 ± 2.66 | 13.42 ± 1.96 | 8.69 ± 1.20 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Lung | |||||||
| ICC | 0.815 | 0.716 | 0.751 | ||||
| Reader 1 | 19.79 ± 2.59 | 18.18 ± 2.44 | 17.45 ± 2.51 | <0.001 † | <0.001 | <0.001 | 0.001 |
| Reader 2 | 20.22 ± 2.93 | 18.75 ± 3.04 | 17.94 ± 2.93 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Muscle | |||||||
| ICC | 0.902 | 0.851 | 0.817 | ||||
| Reader 1 | 23.13 ± 2.93 | 17.10 ± 1.80 | 11.89 ± 1.44 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 22.87 ± 3.08 | 17.01 ± 2.09 | 11.87 ± 1.60 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Liver | |||||||
| ICC | 0.906 | 0.862 | 0.834 | ||||
| Reader 1 | 23.07 ± 2.35 | 16.81 ± 1.75 | 10.86 ± 1.08 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 23.13 ± 2.21 | 16.86 ± 1.61 | 10.91 ± 0.99 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Vertebrae | |||||||
| ICC | 0.937 | 0.896 | 0.896 | ||||
| Reader 1 | 36.82 (7.66) | 29.72 (5.69) | 23.16 (5.68) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 36.28 (7.81) | 30.50 (6.47) | 23.69 (6.31) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| SNR | ASIR-V 50% | DLIR-M | DLIR-H | p | p | ||
|---|---|---|---|---|---|---|---|
| ASIR-V 50% vs. DLIR-M | ASIR-V 50% vs. DLIR-H | DLIR-M vs. DLIR-H | |||||
| Aorta | |||||||
| ICC | 0.911 | 0.913 | 0.925 | ||||
| Reader 1 | 2.46 (0.53) | 3.50 (0.72) | 5.51 (1.24) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 2.47 (0.59) | 3.56 (0.74) | 5.60 (1.29) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Lung | |||||||
| ICC | 0.757 | 0.739 | 0.790 | ||||
| Reader 1 | 45.80 ± 6.03 | 49.95 ± 7.01 | 52.12 ± 7.54 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 43.37 (7.94) | 48.05 (12.79) | 50.95 (13.96) | <0.001 ‡ | 0.018 | <0.001 | <0.001 |
| Muscle | |||||||
| ICC | 0.893 | 0.837 | 0.817 | ||||
| Reader 1 | 2.70 ± 0.38 | 3.64 ± 0.47 | 5.26 ± 0.77 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 2.73 ± 0.43 | 3.65 ± 0.55 | 5.26 ± 0.85 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Liver | |||||||
| ICC | 0.976 | 0.965 | 0.961 | ||||
| Reader 1 | 2.65 (0.68) | 3.65 (0.83) | 5.67 (1.22) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 2.68 (0.71) | 3.59 (0.89) | 5.65 (1.18) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Vertebrae | |||||||
| ICC | 0.971 | 0.966 | 0.943 | ||||
| Reader 1 | 4.66 ± 1.32 | 5.67 ± 1.65 | 7.18 ± 2.09 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 4.63 (2.02) | 5.58 (2.17) | 7.12 (2.76) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| CNR | ASIR-V 50% | DLIR-M | DLIR-H | p | p | ||
|---|---|---|---|---|---|---|---|
| ASIR-V 50% vs. DLIR-M | ASIR-V 50% vs. DLIR-H | DLIR-M vs. DLIR-H | |||||
| Aorta | |||||||
| ICC | 0.953 | 0.948 | 0.938 | ||||
| Reader 1 | 4220.40 (1543.54) | 7023.38 (3140.01) | 15,958.01 (6466.08) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 4234.37 (1612.33) | 7126.66 (3468.47) | 15,880.75 (6711.26) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Lung | |||||||
| ICC | 0.869 | 0.893 | 0.924 | ||||
| Reader 1 | 41.75 (19.53) | 48.10 (22.55) | 57.13 (33.65) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 42.78 (21.31) | 49.55 (25.71) | 57.05 (34.88) | <0.001 ‡ | 0.009 | <0.001 | <0.001 |
| Muscle | |||||||
| ICC | 0.948 | 0.932 | 0.900 | ||||
| Reader 1 | 3239.26 (888.57) | 5560.85 (1350.57) | 11,430.93 (3465.19) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 3202.04 (1440.15) | 5533.11 (1680.58) | 11,239.74 (3792.47) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Liver | |||||||
| ICC | 0.926 | 0.864 | 0.862 | ||||
| Reader 1 | 3353.37 ± 648.20 | 5673.28 ± 1184.25 | 12,621.82 ± 2547.01 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Reader 2 | 3343.94 ± 620.62 | 5624.45 ± 1051.58 | 12,459.73 ± 2273.57 | <0.001 † | <0.001 | <0.001 | <0.001 |
| Vertebrae | |||||||
| ICC | 0.921 | 0.833 | 0.791 | ||||
| Reader 1 | 1716.03 (757.72) | 2641.56 (895.71) | 4391.59 (1575.93) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Reader 2 | 1797.66 (641.32) | 2618.25 (916.38) | 4304.24 (1915.51) | <0.001 ‡ | <0.001 | <0.001 | <0.001 |
| Subjective Scores | ASIR-V 50% | DLIR-M | DLIR-H | p |
|---|---|---|---|---|
| Soft tissue | ||||
| Reader 1 | 3 (0) | 4 (0) | 5 (0) | <0.001 |
| Reader 2 | 3 (0) | 4 (0) | 5 (0) | <0.001 |
| Lung tissue | ||||
| Reader 1 | 4 (0) | 4 (0) | 4 (0) | 0.121 |
| Reader 2 | 4 (0) | 4 (0) | 4 (0) | 0.069 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, J.-M.; Miao, L.; Liang, X.; Liu, Z.-H.; Zhang, L.; Li, M. The Value of Deep Learning Image Reconstruction in Improving the Quality of Low-Dose Chest CT Images. Diagnostics 2022, 12, 2560. https://doi.org/10.3390/diagnostics12102560
Jiang J-M, Miao L, Liang X, Liu Z-H, Zhang L, Li M. The Value of Deep Learning Image Reconstruction in Improving the Quality of Low-Dose Chest CT Images. Diagnostics. 2022; 12(10):2560. https://doi.org/10.3390/diagnostics12102560
Chicago/Turabian StyleJiang, Jiu-Ming, Lei Miao, Xin Liang, Zhuo-Heng Liu, Li Zhang, and Meng Li. 2022. "The Value of Deep Learning Image Reconstruction in Improving the Quality of Low-Dose Chest CT Images" Diagnostics 12, no. 10: 2560. https://doi.org/10.3390/diagnostics12102560