

Calprotectin Levels and Neutrophil Count Are Prognostic Markers of Mortality in COVID-19 Patients
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Samples and Biochemical Analyses
2.2. Statistical Analysis
3. Results
3.1. Biomarker Association to Fatal Outcome
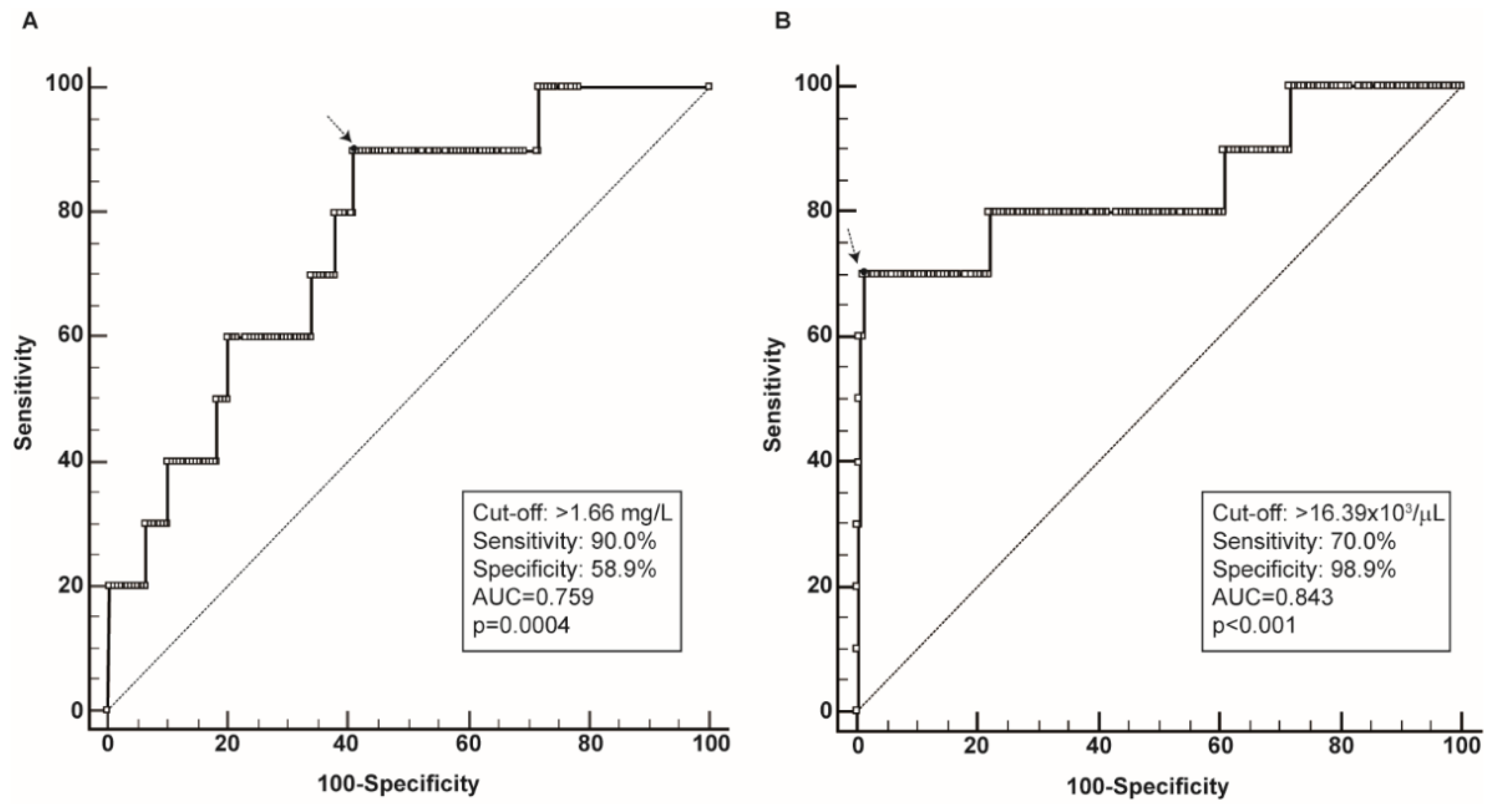
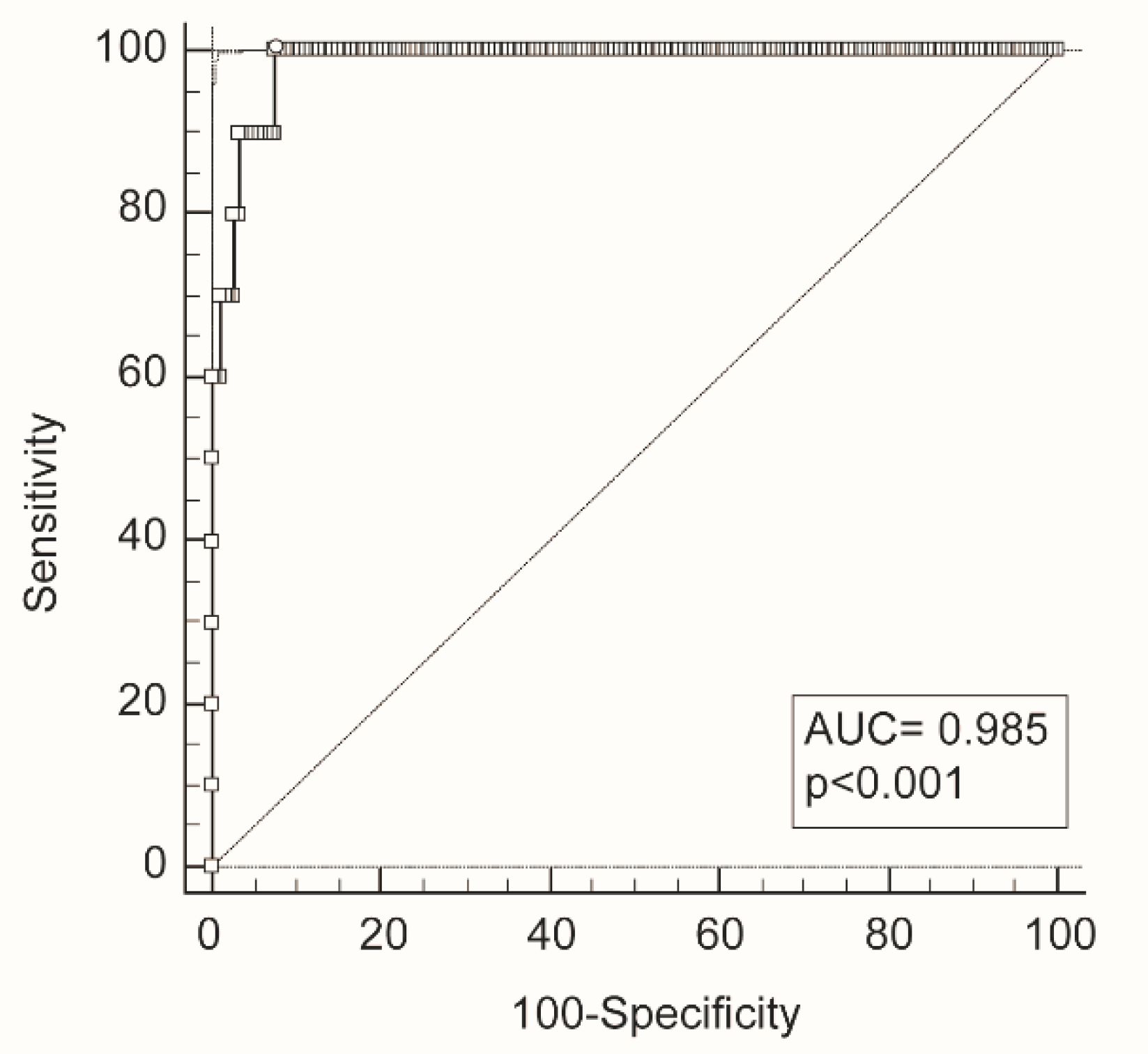
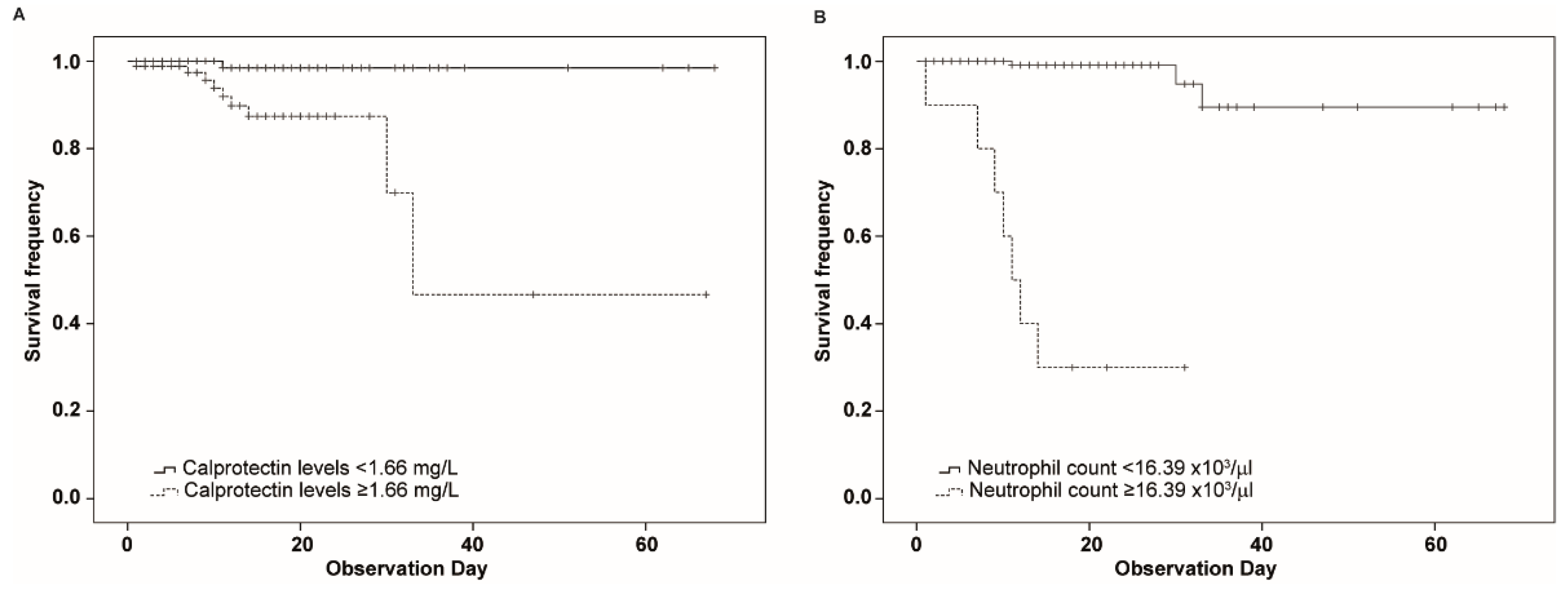
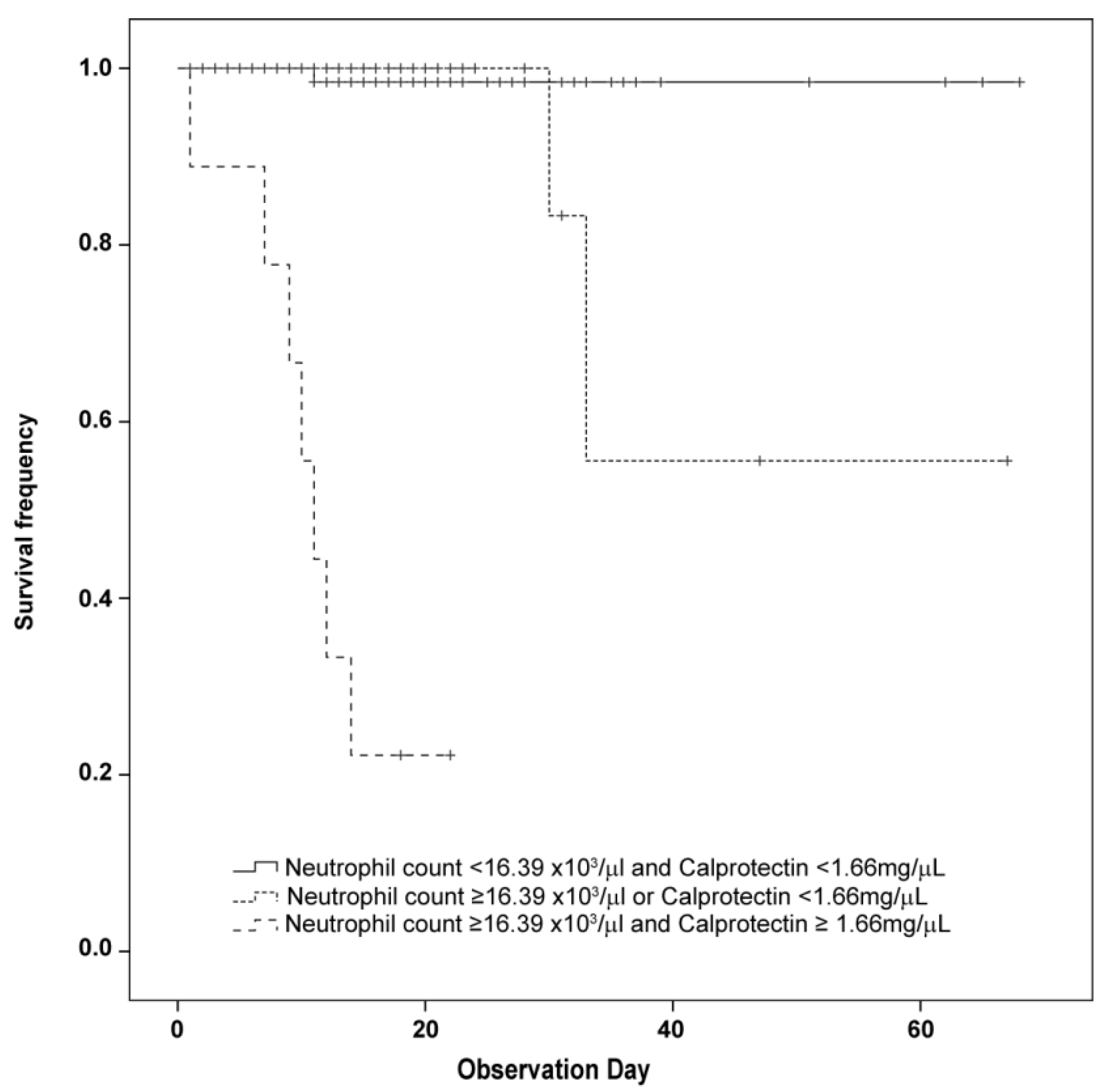
3.2. Identification of Cut-Off and Survival Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ye, Q.; Wang, B.; Mao, J. The Pathogenesis and Treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; June, C.H. Cytokine Release Syndrome in Severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loomba, R.S.; Villarreal, E.G.; Farias, J.S.; Aggarwal, G.; Aggarwal, S.; Flores, S. Serum Biomarkers for Prediction of Mortality in Patients with COVID-19. Ann. Clin. Biochem. 2022, 59, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Wibowo, A.; Pranata, R.; Akbar, M.R.; Purnomowati, A.; Martha, J.W. Prognostic Performance of Troponin in COVID-19: A Diagnostic Meta-Analysis and Meta-Regression. Int. J. Infect. Dis. 2021, 105, 312–318. [Google Scholar] [CrossRef] [PubMed]
- de Falco, R.; Vargas, M.; Palma, D.; Savoia, M.; Miscioscia, A.; Pinchera, B.; Vano, M.; Servillo, G.; Gentile, I.; Fortunato, G. B-Type Natriuretic Peptides and High-Sensitive Troponin I as COVID-19 Survival Factors: Which One Is the Best Performer? J. Clin. Med. 2021, 10, 2726. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, Biochemical and Immune Biomarker Abnormalities Associated with Severe Illness and Mortality in Coronavirus Disease 2019 (COVID-19): A Meta-Analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-Analysis. BMJ Evid. Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers Associated with COVID-19 Disease Progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Wang, S.; Song, R.; Wang, Z.; Jing, Z.; Wang, S.; Ma, J. S100A8/A9 in Inflammation. Front. Immunol. 2018, 9, 1298. [Google Scholar] [CrossRef] [Green Version]
- Romand, X.; Bernardy, C.; Nguyen, M.V.C.; Courtier, A.; Trocme, C.; Clapasson, M.; Paclet, M.-H.; Toussaint, B.; Gaudin, P.; Baillet, A. Systemic Calprotectin and Chronic Inflammatory Rheumatic Diseases. Jt. Bone Spine 2019, 86, 691–698. [Google Scholar] [CrossRef]
- Wirtz, T.H.; Buendgens, L.; Weiskirchen, R.; Loosen, S.H.; Haehnsen, N.; Puengel, T.; Abu Jhaisha, S.; Brozat, J.F.; Hohlstein, P.; Koek, G.; et al. Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients. Diagnostics 2020, 10, 990. [Google Scholar] [CrossRef]
- Sprenkeler, E.G.G.; Zandstra, J.; van Kleef, N.D.; Goetschalckx, I.; Verstegen, B.; Aarts, C.E.M.; Janssen, H.; Tool, A.T.J.; van Mierlo, G.; van Bruggen, R.; et al. S100A8/A9 Is a Marker for the Release of Neutrophil Extracellular Traps and Induces Neutrophil Activation. Cells 2022, 11, 236. [Google Scholar] [CrossRef] [PubMed]
- Infantino, M.; Manfredi, M.; Alessio, M.G.; Previtali, G.; Grossi, V.; Benucci, M.; Faraone, A.; Fortini, A.; Grifoni, E.; Masotti, L.; et al. Clinical Utility of Circulating Calprotectin to Assist Prediction and Monitoring of COVID-19 Severity: An Italian Study. J. Med. Virol. 2022, 94, 5758–5765. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.L.; Navaz, S.A.; Kanthi, Y.; Albesa, R.; Mahler, M.; Knight, J.S.; Zuo, Y. Circulating Calprotectin as a Predictive and Severity Biomarker in Patients with COVID-19. Diagnostics 2022, 12, 1324. [Google Scholar] [CrossRef] [PubMed]
- Kaya, T.; Yaylacı, S.; Nalbant, A.; Yıldırım, İ.; Kocayiğit, H.; Çokluk, E.; Şekeroğlu, M.R.; Köroğlu, M.; Güçlü, E. Serum Calprotectin as a Novel Biomarker for Severity of COVID-19 Disease. Ir. J. Med. Sci. 2022, 191, 59–64. [Google Scholar] [CrossRef]
- Mao, Q.; Wang, C.; Wen, W.; Zhou, M.; Tang, J.; Chen, C.; Cheng, Y.; Wu, Q.; Zhang, X.; Feng, Z.; et al. A Meta-Analysis of the Association between Calprotectin and the Severity of COVID-19. J. Infect. 2022, 84, e31–e33. [Google Scholar] [CrossRef] [PubMed]
- Mellett, L.; Khader, S.A. S100A8/A9 in COVID-19 Pathogenesis: Impact on Clinical Outcomes. Cytokine Growth Factor Rev. 2022, 63, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An Immune-Based Biomarker Signature Is Associated with Mortality in COVID-19 Patients. JCI Insight 2021, 6, 144455. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.-H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An Inflammatory Cytokine Signature Predicts COVID-19 Severity and Survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Ducastel, M.; Chenevier-Gobeaux, C.; Ballaa, Y.; Meritet, J.-F.; Brack, M.; Chapuis, N.; Pene, F.; Carlier, N.; Szwebel, T.-A.; Roche, N.; et al. Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19. Int. J. Mol. Sci. 2021, 22, 7462. [Google Scholar] [CrossRef]
- de Guadiana Romualdo, L.G.; Mulero, M.D.R.; Olivo, M.H.; Rojas, C.R.; Arenas, V.R.; Morales, M.G.; Abellán, A.B.; Conesa-Zamora, P.; García-García, J.; Hernández, A.C.; et al. Circulating Levels of GDF-15 and Calprotectin for Prediction of in-Hospital Mortality in COVID-19 Patients: A Case Series. J. Infect. 2021, 82, e40–e42. [Google Scholar] [CrossRef] [PubMed]
- Nevejan, L.; Strypens, T.; Van Nieuwenhove, M.; Boel, A.; Cattoir, L.; Meeus, P.; Bossuyt, X.; De Neve, N.; Van Hoovels, L. Prognostic Value of Circulating Calprotectin Levels on the Clinical Course of COVID-19 Differs between Serum, Heparin, EDTA and Citrate Sample Types. Clin. Chim. Acta 2022, 525, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Bauer, W.; Diehl-Wiesenecker, E.; Ulke, J.; Galtung, N.; Havelka, A.; Hegel, J.K.; Tauber, R.; Somasundaram, R.; Kappert, K. Outcome Prediction by Serum Calprotectin in Patients with COVID-19 in the Emergency Department. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Udeh, R.; Advani, S.; de Guadiana Romualdo, L.G.; Dolja-Gore, X. Calprotectin, an Emerging Biomarker of Interest in COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 775. [Google Scholar] [CrossRef] [PubMed]
- García de Guadiana-Romualdo, L.; Rodríguez Rojas, C.; Morell-García, D.; Andaluz-Ojeda, D.; Rodríguez Mulero, M.D.; Rodríguez-Borja, E.; Ballesteros-Vizoso, A.; Calvo, M.D.; Albert-Botella, L.; Pozo Giráldez, A.; et al. Circulating Levels of Calprotectin, a Signature of Neutrophil Activation in Prediction of Severe Respiratory Failure in COVID-19 Patients: A Multicenter, Prospective Study (CalCov Study). Inflamm. Res. 2022, 71, 57–67. [Google Scholar] [CrossRef]
- Shi, H.; Zuo, Y.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Woodward, W.; Lezak, S.P.; Lugogo, N.L.; et al. Neutrophil Calprotectin Identifies Severe Pulmonary Disease in COVID-19. J. Leukoc. Biol. 2021, 109, 67–72. [Google Scholar] [CrossRef]
- Schulte-Schrepping, J.; Reusch, N.; Paclik, D.; Baßler, K.; Schlickeiser, S.; Zhang, B.; Krämer, B.; Krammer, T.; Brumhard, S.; Bonaguro, L.; et al. Severe COVID-19 Is Marked by a Dysregulated Myeloid Cell Compartment. Cell 2020, 182, 1419–1440.e23. [Google Scholar] [CrossRef]
- Khartabil, T.A.; Russcher, H.; van der Ven, A.; de Rijke, Y.B. A Summary of the Diagnostic and Prognostic Value of Hemocytometry Markers in COVID-19 Patients. Crit. Rev. Clin. Lab. Sci. 2020, 57, 415–431. [Google Scholar] [CrossRef]
- Silvin, A.; Chapuis, N.; Dunsmore, G.; Goubet, A.-G.; Dubuisson, A.; Derosa, L.; Almire, C.; Hénon, C.; Kosmider, O.; Droin, N.; et al. Elevated Calprotectin and Abnormal Myeloid Cell Subsets Discriminate Severe from Mild COVID-19. Cell 2020, 182, 1401–1418.e18. [Google Scholar] [CrossRef]
- Biernacki, T.; Kokas, Z.; Sandi, D.; Füvesi, J.; Fricska-Nagy, Z.; Faragó, P.; Kincses, T.Z.; Klivényi, P.; Bencsik, K.; Vécsei, L. Emerging Biomarkers of Multiple Sclerosis in the Blood and the CSF: A Focus on Neurofilaments and Therapeutic Considerations. Int. J. Mol. Sci. 2022, 23, 3383. [Google Scholar] [CrossRef]
- Lindblom, J.; Mohan, C.; Parodis, I. Diagnostic, Predictive and Prognostic Biomarkers in Systemic Lupus Erythematosus: Current Insights. Curr. Opin. Rheumatol. 2022, 34, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Fredman, G.; MacNamara, K.C. Atherosclerosis Is a Major Human Killer and Non-Resolving Inflammation Is a Prime Suspect. Cardiovasc. Res. 2021, 117, 2563–2574. [Google Scholar] [CrossRef] [PubMed]
- Di Taranto, M.D.; Morgante, A.; Bracale, U.M.; D’Armiento, F.P.; Porcellini, M.; Bracale, G.; Fortunato, G.; Salvatore, F. Altered Expression of Inflammation-Related Genes in Human Carotid Atherosclerotic Plaques. Atherosclerosis 2012, 220, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Neupane, R.; Jin, X.; Sasaki, T.; Li, X.; Murohara, T.; Cheng, X.W. Immune Disorder in Atherosclerotic Cardiovascular Disease—Clinical Implications of Using Circulating T-Cell Subsets as Biomarkers. Circ. J. 2019, 83, 1431–1438. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 195) | Surviving (n = 185) | Non-Surviving (n = 10) | Significance | |
|---|---|---|---|---|
| Age, years | 55 (34–67) | 51 (33–66) | 77 (62–85) | p < 0.001 |
| Sex, number of males (%) | 94 (48.2%) | 86 (46.5%) | 8 (80.0%) | ns |
| Serum Calprotectin (mg/L) | 1.32 (0.58–3.91) | 1.28 (0.54–3.60) | 4.26 (2.01–9.84) | p = 0.006 |
| C-reactive protein (mg/L) | 17.8 (3.73–54.64) | 16.80 (3.60–47.92) | 62.16 (8.45–78.62) | ns (p = 0.127) |
| Neutrophil count (×103/µL) | 6.38 (4.80–9.07) | 6.26 (4.73–8.49) | 20.26 (8.29–30.26) | p = 0.0003 |
| Decreased lung function, n, (%) | 170 (87.2%) | 164 (88.6%) | 6 (60.0%) | p = 0.026 |
| Diabetes n, (%) | 155 (79.5%) | 149 (80.5%) | 6 (60.0%) | ns |
| Heart disease n, (%) | 187 (95.9%) | 179 (96.8%) | 8 (80.0%) | ns |
| Hypertension n, (%) | 145 (74.4%) | 139 (75.1%) | 6 (60.0%) | ns |
| Hospitalization days | 13 (7–21) | 13 (7–21) | 11 (8–18) | ns |
| Variables | Model 1 OR (95% CI) significance | Model 2 OR (95% CI) significance | Model 3 OR (95% CI) significance |
|---|---|---|---|
| Sex | ns | ns | ns |
| Age | 1.186 (1.059–1.329) p = 0.003 | 1.085 (1.026–1.148) p = 0.004 | 1.111 (1.018–1.213) p = 0.018 |
| Calprotectin levels | 1.874 (1.312–2.677) p = 0.001 | - | - |
| C-reactive protein | - | 1.002 (0.992–1.013) ns (p = 0.678) | - |
| Neutrophil count | - | - | 1.364 (1.163–1.600) p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardiero, G.; Palma, D.; Vano, M.; Anastasio, C.; Pinchera, B.; Ferrandino, M.; Gianfico, C.; Gentile, L.; Savoia, M.; Gentile, I.; et al. Calprotectin Levels and Neutrophil Count Are Prognostic Markers of Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2554. https://doi.org/10.3390/diagnostics12102554
Cardiero G, Palma D, Vano M, Anastasio C, Pinchera B, Ferrandino M, Gianfico C, Gentile L, Savoia M, Gentile I, et al. Calprotectin Levels and Neutrophil Count Are Prognostic Markers of Mortality in COVID-19 Patients. Diagnostics. 2022; 12(10):2554. https://doi.org/10.3390/diagnostics12102554
Chicago/Turabian StyleCardiero, Giovanna, Daniela Palma, Martina Vano, Claudia Anastasio, Biagio Pinchera, Martina Ferrandino, Carlo Gianfico, Luca Gentile, Marcella Savoia, Ivan Gentile, and et al. 2022. "Calprotectin Levels and Neutrophil Count Are Prognostic Markers of Mortality in COVID-19 Patients" Diagnostics 12, no. 10: 2554. https://doi.org/10.3390/diagnostics12102554