
Determination of the Accuracy of Salivary Biomarkers for Periodontal Diagnosis
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
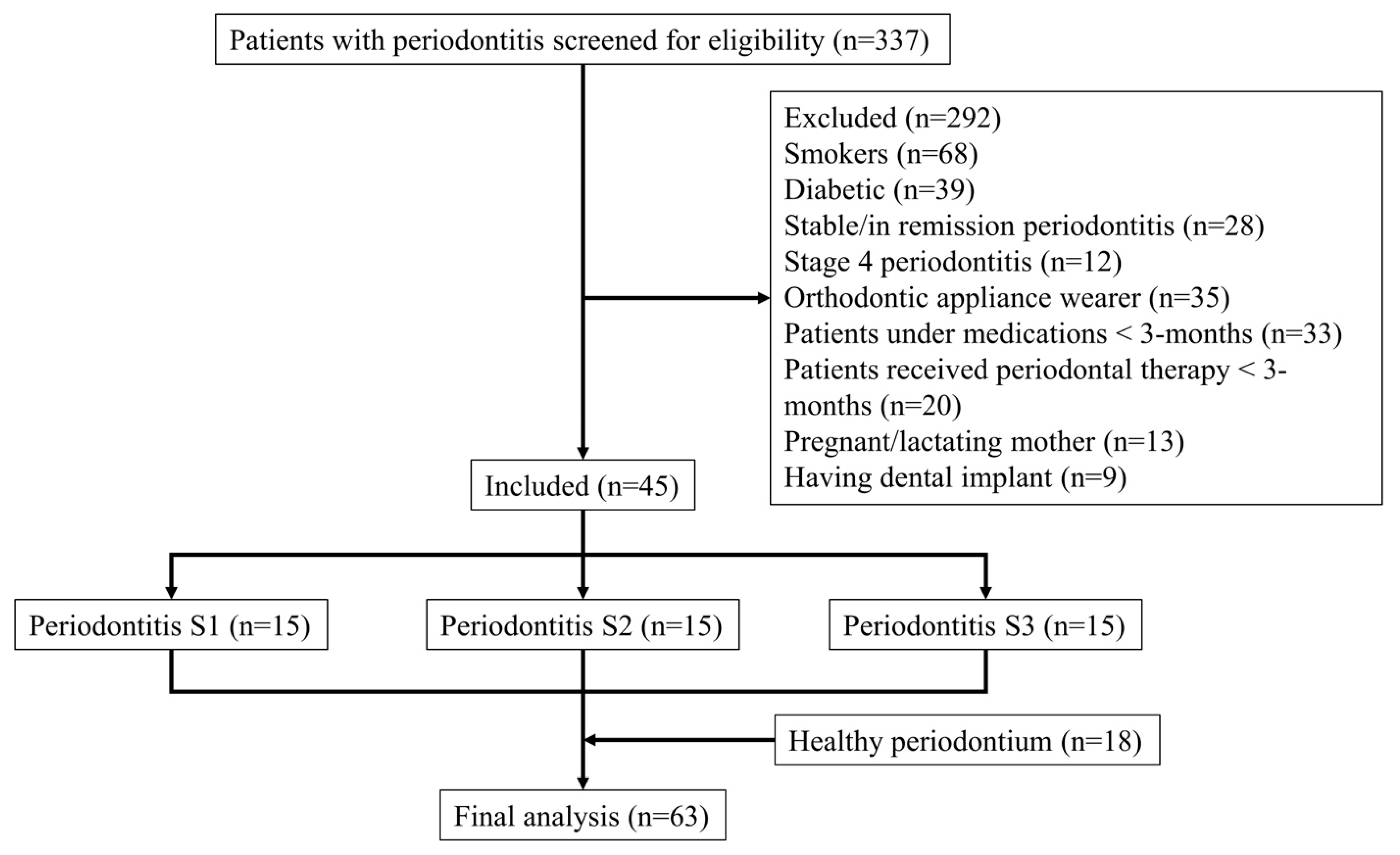
2.1. Study Design
2.2. Study Population
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Periodontal Parameters
2.6. Calibration and Outcome Measures
2.7. Salivary Sample Collection and Analysis
2.8. Pilot Study and Sample Size Calculation
2.9. Statistical Analysis
3. Results
3.1. Study Population
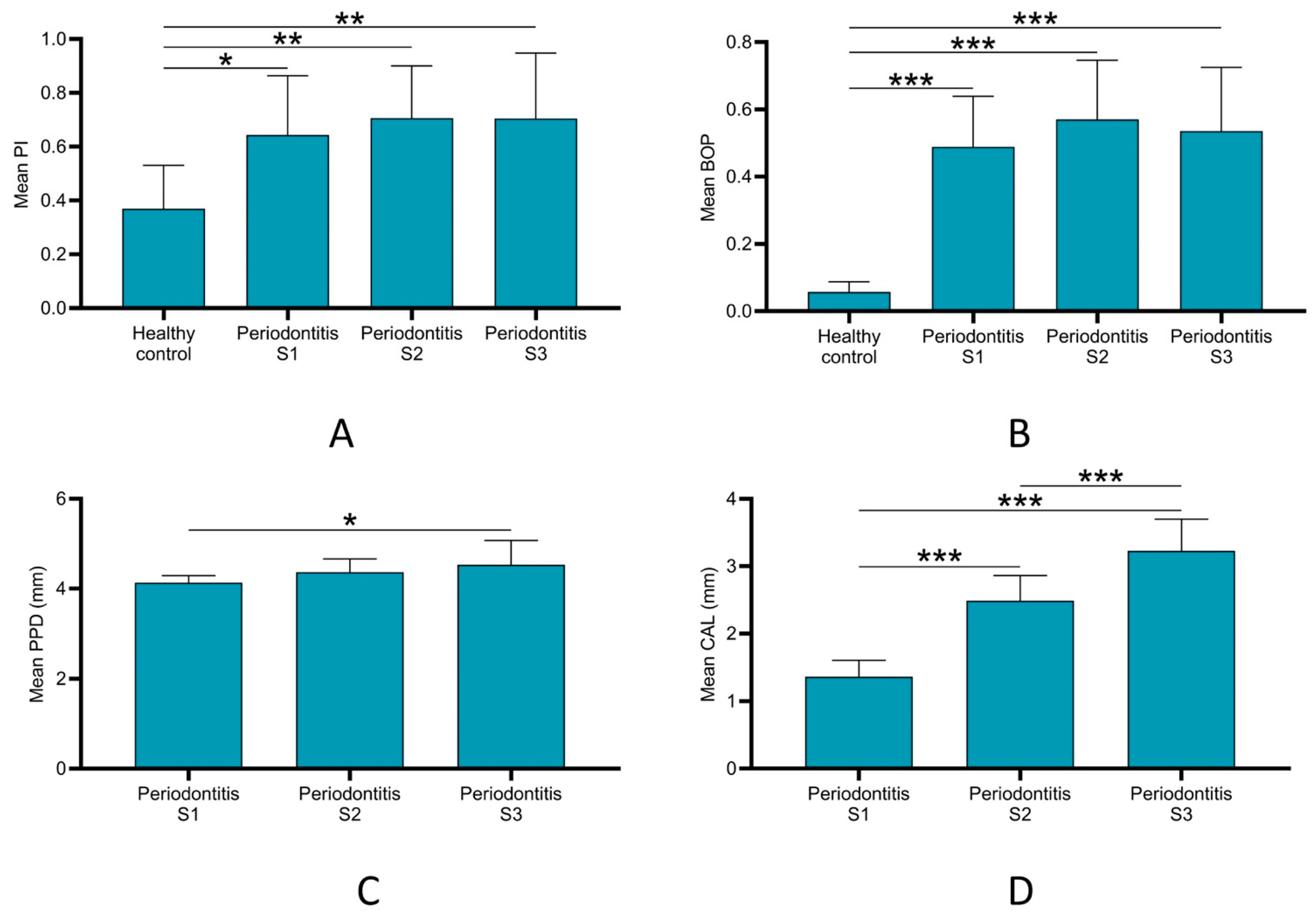
3.2. Periodontal Parameters
3.3. Salivary Biomarkers Levels
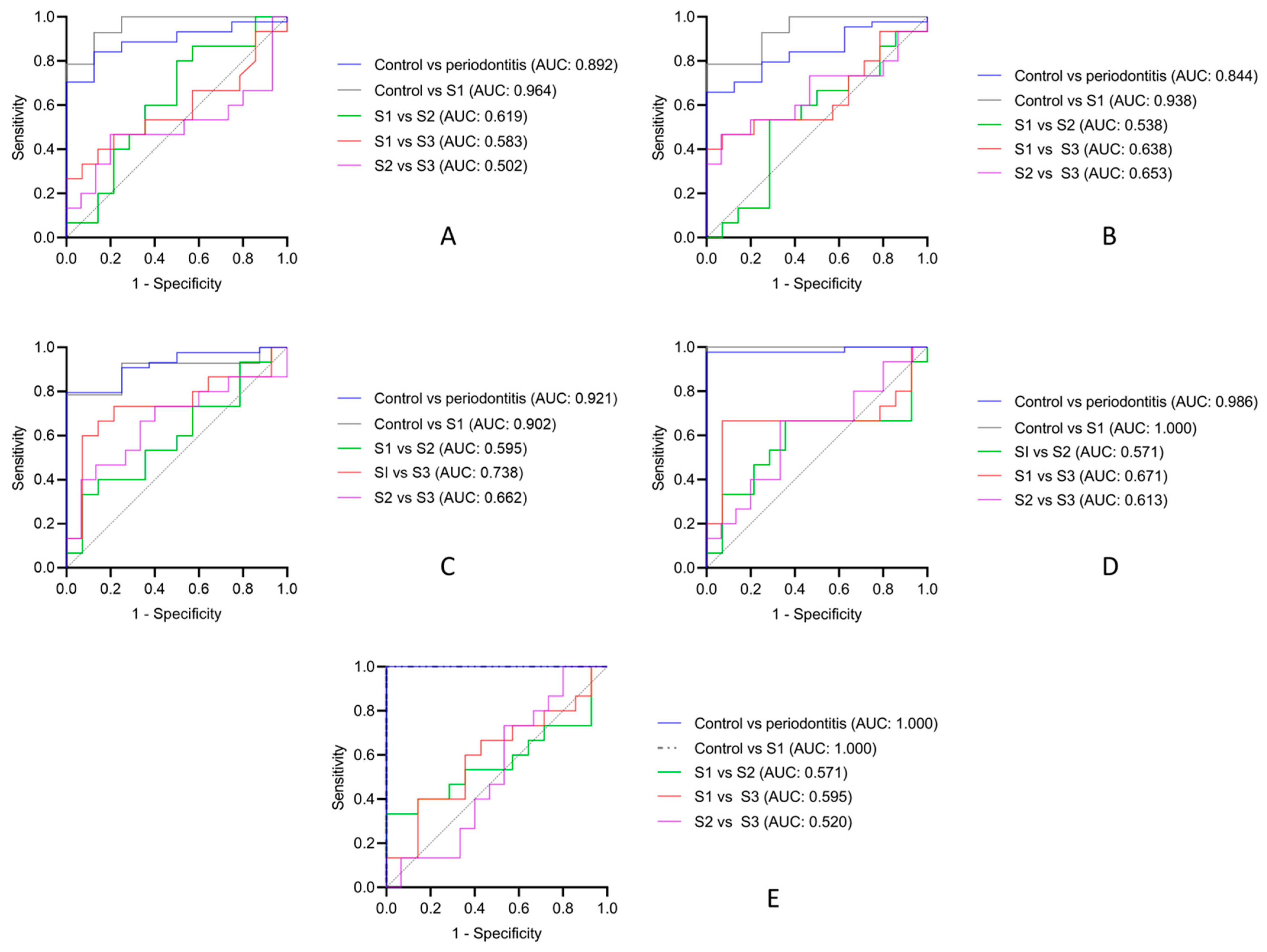
3.4. Diagnostic Accuracy of Salivary Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G. Immunomicrobial pathogenesis of periodontitis: Keystones, pathobionts, and host response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahlin, Å.; Papias, A.; Jansson, H.; Norderyd, O. Secular trends over 40 years of periodontal health and disease in individuals aged 20-80 years in Jönköping, Sweden: Repeated cross-sectional studies. J. Clin. Periodontol. 2018, 45, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, I.; Duane, B. Periodontal disease has an impact on patients’ quality of life. Evid. Based Dent. 2018, 19, 14–15. [Google Scholar] [CrossRef]
- Chapple, I.L. Time to take periodontitis seriously. BMJ 2014, 348, g2645. [Google Scholar] [CrossRef]
- Chapple, I.L.; Van der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary prevention of periodontitis: Managing gingivitis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S71–S76. [Google Scholar] [CrossRef]
- Alshehri, A.A.M.; Alshehri, F.D.A.; Hakami, K.Y.A.; Assiri, Z.A.A.; Alshehri, A.A.M.; Alqahtani, Z.A.Z. Awareness and knowledge of periodontal disease among Saudi primary school teachers in Aseer region. J. Indian Soc. Periodontol. 2017, 21, 403–408. [Google Scholar]
- Preshaw, P.M. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015, 15, S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandra, S.S.; Mehta, D.S.; Sandesh, N.; Baliga, V.; Amarnath, J. Periodontal probing systems: A review of available equipment. Compend. Contin. Educ. Dent. 2011, 32, 71–77. [Google Scholar]
- Kleinberg, I.; Kaufman, H.W.; Wolff, M. Measurement of tooth hypersensitivity and oral factors involved in its development. Arch. Oral Biol. 1994, 39, S63–S71. [Google Scholar] [CrossRef]
- Ko, T.J.; Byrd, K.M.; Kim, S.A. The Chairside Periodontal Diagnostic Toolkit: Past, Present, and Future. Diagnostics 2021, 11, 932. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S68–S77. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. S1), S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eickholz, P.; Kim, T.S.; Benn, D.K.; Staehle, H.J. Validity of radiographic measurement of interproximal bone loss. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 99–106. [Google Scholar] [CrossRef]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.R.; Sakellari, D. Active MMP-8 (aMMP-8) as a Grading and Staging Biomarker in the Periodontitis Classification. Diagnostics 2020, 10, 61. [Google Scholar] [CrossRef] [Green Version]
- Javaid, M.A.; Ahmed, A.S.; Durand, R.; Tran, S.D. Saliva as a diagnostic tool for oral and systemic diseases. J. Oral Biol. Craniofac. Res. 2016, 6, 66–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Tjäderhane, L.; Salo, T. Matrix metalloproteinases (MMPs) in oral diseases. Oral Dis. 2004, 10, 311–318. [Google Scholar] [CrossRef]
- Gonçalves, P.F.; Huang, H.; McAninley, S.; Alfant, B.; Harrison, P.; Aukhil, I.; Walker, C.; Shaddox, L.M. Periodontal treatment reduces matrix metalloproteinase levels in localized aggressive periodontitis. J. Periodontol. 2013, 84, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nędzi-Góra, M.; Kostrzewa-Janicka, J.; Górska, R. Elastase and metalloproteinase-9 concentrations in saliva in patients with chronic periodontitis. Cent. Eur. J. Immunol. 2014, 39, 357–364. [Google Scholar] [CrossRef]
- Sorsa, T.; Gursoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontology 2000 2016, 70, 142–163. [Google Scholar] [CrossRef] [PubMed]
- Popat, R.P.; Bhavsar, N.V.; Popat, P.R. Gingival crevicular fluid levels of Matrix Metalloproteinase-1 (MMP-1) and Tissue Inhibitor of Metalloproteinase-1 (TIMP-1) in periodontal health and disease. Singapore Dent. J. 2014, 35, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Rautava, J.; Gürsoy, U.K.; Kullström, A.; Könönen, E.; Sorsa, T.; Tervahartiala, T.; Gürsoy, M. An Oral Rinse Active Matrix Metalloproteinase-8 Point-of-Care Immunotest May Be Less Accurate in Patients with Crohn’s Disease. Biomolecules 2020, 10, 395. [Google Scholar] [CrossRef] [Green Version]
- Bostanci, N.; Mitsakakis, K.; Afacan, B.; Bao, K.; Johannsen, B.; Baumgartner, D.; Müller, L.; Kotolová, H.; Emingil, G.; Karpíšek, M. Validation and verification of predictive salivary biomarkers for oral health. Sci. Rep. 2021, 11, 6406. [Google Scholar] [CrossRef] [PubMed]
- Salminen, A.; Gursoy, U.K.; Paju, S.; Hyvärinen, K.; Mäntylä, P.; Buhlin, K.; Könönen, E.; Nieminen, M.S.; Sorsa, T.; Sinisalo, J.; et al. Salivary biomarkers of bacterial burden, inflammatory response, and tissue destruction in periodontitis. J. Clin. Periodontol. 2014, 41, 442–450. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Mühlemann, H.R.; Son, S. Gingival sulcus bleeding--a leading symptom in initial gingivitis. Helv. Odontol. Acta 1971, 15, 107–113. [Google Scholar]
- Hefti, A.F.; Preshaw, P.M. Examiner alignment and assessment in clinical periodontal research. Periodontol 2000 2012, 59, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Granger, D.A.; Johnson, S.B.; Szanton, S.L.; Out, D.; Schumann, L.L. Incorporating salivary biomarkers into nursing research: An overview and review of best practices. Biol. Res. Nurs. 2012, 14, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charan, J.; Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirtcliff, E.A.; Granger, D.A.; Schwartz, E.; Curran, M.J. Use of salivary biomarkers in biobehavioral research: Cotton-based sample collection methods can interfere with salivary immunoassay results. Psychoneuroendocrinology 2001, 26, 165–173. [Google Scholar] [CrossRef]
- Chiappin, S.; Antonelli, G.; Gatti, R.; De Palo, E.F. Saliva specimen: A new laboratory tool for diagnostic and basic investigation. Clin. Chim. Acta 2007, 383, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Ríos, P.; Hernández, M.; Garrido, M.; Tervahartiala, T.; Leppilahti, J.M.; Kuula, H.; Heikkinen, A.M.; Mäntylä, P.; Rathnayake, N.; Nwhator, S. Oral fluid matrix metalloproteinase (MMP)-8 as a diagnostic tool in chronic periodontitis. Met. Med. 2016, 3, 11–18. [Google Scholar]
- Gursoy, U.K.; Könönen, E.; Pradhan-Palikhe, P.; Tervahartiala, T.; Pussinen, P.J.; Suominen-Taipale, L.; Sorsa, T. Salivary MMP-8, TIMP-1, and ICTP as markers of advanced periodontitis. J. Clin. Periodontol. 2010, 37, 487–493. [Google Scholar] [CrossRef]
- Gul, S.S.; Abdulkareem, A.A.; Sha, A.M.; Rawlinson, A. Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases. Diagnostics 2020, 10, 838. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Groups | Healthy Control | Periodontitis S1 | Periodontitis S2 | Periodontitis S3 | |
|---|---|---|---|---|---|
| n, % | 63, 100 | 18, 28.6 | 15, 23.8 | 15, 23.8 | 15, 23.8 |
| Age (years) | |||||
| Mean ± SD | 29.75 ± 10.93 | 28.75 ± 4.464 | 22.00 ± 6.803 | 28.40 ± 10.55 | 39.40 ± 10.46 |
| Median | 28 | 28.50 | 31 | 34 | 40 |
| Range | 18 to 55 | 18 to 35 | 23 to 35 | 26 to 52 | 25 to 55 |
| Sex § | |||||
| Male | 31, 49.1 | 8, 44.4% | 6, 40.0 | 7, 46.7 | 10, 66.7 |
| Female | 32, 50.9 | 10, 55.6% | 9, 60.0 | 8, 53.3 | 5, 33.3 |
| Salivary Biomarkers § | Control | Periodontitis S1 | Periodontitis S2 | Periodontitis S3 | Periodontitis (All Groups) |
|---|---|---|---|---|---|
| MMP-8 (ng/mL) | 1677 | 4188 ** | 3469 * | 3337 * | 4079 ** |
| MMP-9 (ng/mL) | 3292 | 5617 * | 16031 * | 4144 | 5850 * |
| TIMP-1 (ng/mL) | 6538 | 3861 | 3636 * | 2254 *** | 3446 ** |
| MMP-8/TIMP-1 | 0.209 | 1.265 ** | 0.936 ** | 2.093 *** | 1.265 *** |
| MMP-9/TIMP-1 | 0.484 | 1.776 ** | 3.164 *** | 2.769 *** | 2.296 *** |
| Biomarker | Sensitivity | Specificity | AUC | 95% CI | Cut-Off Point | p Value |
|---|---|---|---|---|---|---|
| Control vs. periodontitis | ||||||
| MMP-8 (ng/mL) | 0.886 | 0.750 | 0.892 | 0.800 to 0.984 | 1992 | 0.0001 |
| MMP-9 (ng/mL) | 0.800 | 0.750 | 0.844 | 0.730 to 0.956 | 3606 | 0.002 |
| TIMP-1 (ng/mL) | 0.909 | 0.750 | 0.920 | 0.842 to 0.998 | 5994 | 0.0001 |
| MMP-8/TIMP-1 | 0.977 | 1.000 | 0.986 | 0.956 to 1.000 | 0.464 | 0.0001 |
| MMP-9/TIMP-1 | 1.000 | 1.000 | 1.000 | 1.000 to 1.000 | 0.712 | 0.0001 |
| Control vs. periodontitis S1 | ||||||
| MMP-8 (ng/mL) | 0.929 | 0.875 | 0.964 | 0.895 to 1.00 | 2190 | 0.0001 |
| MMP-9 (ng/mL) | 0.929 | 0.75 | 0.938 | 0.841 to 1.00 | 3606 | 0.001 |
| TIMP-1 (ng/mL) | 0.786 | 1.000 | 0.902 | 0.767 to 1.00 | 4734 | 0.002 |
| MMP-8/TIMP-1 | 1.000 | 1.000 | 1.000 | 1.00 to 1.00 | 0.464 | 0.0001 |
| MMP-9/TIMP-1 | 1.000 | 1.000 | 1.000 | 1.00 to 1.00 | 0.712 | 0.0001 |
| S1 vs. S3 | ||||||
| TIMP-1 (ng/mL) | 0.733 | 0.786 | 0.738 | 0.544 to 0.931 | 3228 | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammed, H.A.; Abdulkareem, A.A.; Zardawi, F.M.; Gul, S.S. Determination of the Accuracy of Salivary Biomarkers for Periodontal Diagnosis. Diagnostics 2022, 12, 2485. https://doi.org/10.3390/diagnostics12102485
Mohammed HA, Abdulkareem AA, Zardawi FM, Gul SS. Determination of the Accuracy of Salivary Biomarkers for Periodontal Diagnosis. Diagnostics. 2022; 12(10):2485. https://doi.org/10.3390/diagnostics12102485
Chicago/Turabian StyleMohammed, Hiba Abdullah, Ali Abbas Abdulkareem, Faraedon Mostafa Zardawi, and Sarhang Sarwat Gul. 2022. "Determination of the Accuracy of Salivary Biomarkers for Periodontal Diagnosis" Diagnostics 12, no. 10: 2485. https://doi.org/10.3390/diagnostics12102485