
Nutritional Status at Diagnosis as Predictor of Survival from Childhood Cancer: A Review of the Literature
 , , ,
, , ,
Abstract
:1. Introduction
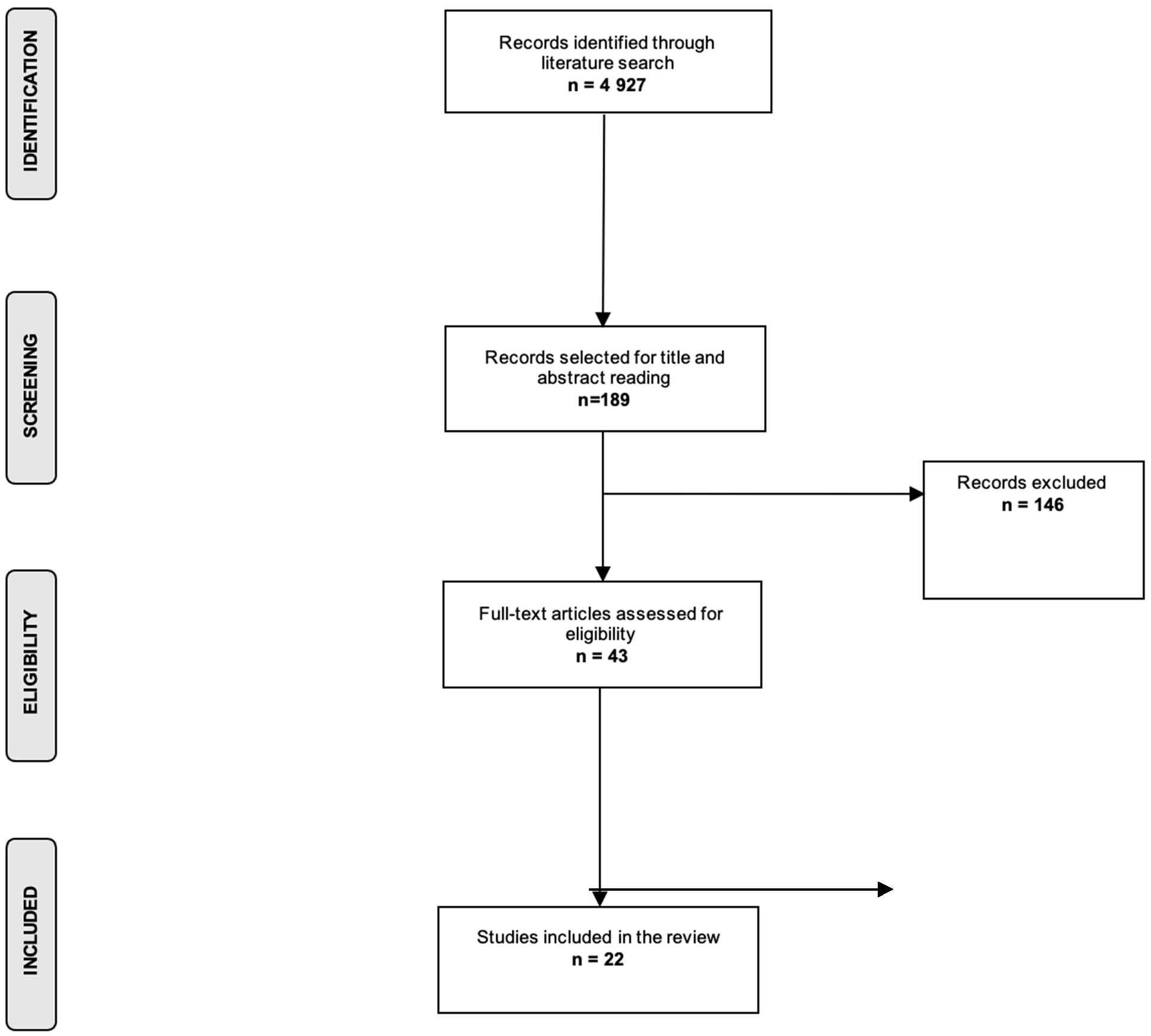
2. Methods
3. Results
3.1. Hematological Malignancies
3.2. Ewing Sarcoma
3.3. Osteosarcoma
3.4. Rhabdomyosarcoma
3.5. Other Cancer Sites
4. Discussion
4.1. Undernutrition and Cancer Outcomes
4.2. Overnutrition and Cancer Outcomes
4.3. Nutritional Interventions
4.4. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; IICC-3 Contributors; et al. International incidence of childhood cancer, 2001–2010: A population-based registry study. Lancet Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef]
- American Cancer Society’s (ACS) publications. Cancer Facts & Figures 2020 and Cancer Facts & Figures 2016, and the ACS Website (January 2020). 2020. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2020.html (accessed on 1 January 2020).
- Johnston, W.; Erdmann, F.; Newton, R.; Steliarova-Foucher, E.; Schüz, J.; Roman, E. Childhood cancer: Estimating regional and global incidence. Cancer Epidemiol. 2020, 71, 101662. [Google Scholar] [CrossRef] [PubMed]
- Force, L.M.; Abdollahpour, I.; Advani, S.M.; Agius, D.; Ahmadian, E.; Alahdab, F.; Alam, T.; Alebel, A.; Alipour, V.; Allen, C.A.; et al. The global burden of childhood and adolescent cancer in 2017: An analysis of the Global Burden of Disease Study 2017. Lancet Oncol. 2019, 20, 1211–1225. [Google Scholar] [CrossRef]
- Erdmann, F.; Frederiksen, L.E.; Bonaventure, A.; Mader, L.; Hasle, H.; Robison, L.L.; Winther, J.F. Childhood cancer: Survival, treatment modalities, late effects and improvements over time. Cancer Epidemiol. 2020, 71, 101733. [Google Scholar] [CrossRef] [PubMed]
- Gibson, T.M.; Mostoufi-Moab, S.; Stratton, K.L.; Leisenring, W.M.; Barnea, D.; Chow, E.J.; Donaldson, S.S.; Howell, R.M.; Hudson, M.M.; Mahajan, A.; et al. Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970–99: A report from the Childhood Cancer Survivor Study cohort. Lancet Oncol. 2018, 19, 1590–1601. [Google Scholar] [CrossRef]
- World Health Organization. Double Burden of Malnutrition. Available online: https://www.who.int/nutrition/double-burden-malnutrition/en/ (accessed on 15 September 2018).
- Rogers, P.C.; Melnick, S.J.; Ladas, E.J.; Halton, J.; Baillargeon, J.; Sacks, N. Children’s Oncology Group (COG) Nutrition Committee. Pediatr. Blood Cancer 2008, 50, 447–450. [Google Scholar] [CrossRef]
- Co-Reyes, E.; Li, R.; Huh, W.; Chandra, J. Malnutrition and obesity in pediatric oncology patients: Causes, consequences, and interventions. Pediatr. Blood Cancer 2012, 59, 1160–1167. [Google Scholar] [CrossRef]
- Brinksma, A.; Huizinga, G.; Sulkers, E.; Kamps, W.; Roodbol, P.; Tissing, W. Malnutrition in childhood cancer patients: A review on its prevalence and possible causes. Crit. Rev. Oncol. Hematol. 2012, 83, 249–275. [Google Scholar] [CrossRef]
- Iniesta, R.R.; Paciarotti, I.; Davidson, I.; McKenzie, J.M.; Brougham, M.F.; Wilson, D.C. Nutritional status of children and adolescents with cancer in Scotland: A prospective cohort study. Clin. Nutr. ESPEN 2019, 32, 96–106. [Google Scholar] [CrossRef]
- Ladas, E.J.; Sacks, N.; Meacham, L.; Henry, D.; Enriquez, L.; Lowry, G.; Hawkes, R.; Dadd, G.; Rogers, P. A Multidisciplinary Review of Nutrition Considerations in the Pediatric Oncology Population: A Perspective from Children’s Oncology Group. Nutr. Clin. Pract. 2005, 20, 377–393. [Google Scholar] [CrossRef]
- Hamilton, E.C.; Curtin, T.; Slack, R.S.; Ge, C.; Slade, A.D.; Hayes-Jordan, A.; Lally, K.P.; Austin, M.T. Surgical Feeding Tubes in Pediatric and Adolescent Cancer Patients: A Single-institution Retrospective Review. J. Pediatr. Hematol. Oncol. 2017, 39, e342–e348. [Google Scholar] [CrossRef] [PubMed]
- Brinksma, A.; Sanderman, R.; Roodbol, P.F.; Sulkers, E.; Burgerhof, J.G.M.; De Bont, E.S.J.M.; Tissing, W.J.E. Malnutrition is associated with worse health-related quality of life in children with cancer. Support. Care Cancer 2015, 23, 3043–3052. [Google Scholar] [CrossRef] [PubMed]
- Fu, A.B.; Hodgman, E.I.; Burkhalter, L.S.; Renkes, R.; Slone, T.; Alder, A.C. Long-term central venous access in a pediatric leukemia population. J. Surg. Res. 2016, 205, 419–425. [Google Scholar] [CrossRef]
- Li, M.-J.; Chang, H.-H.; Yang, Y.-L.; Lu, M.-Y.; Shao, P.-L.; Fu, C.-M.; Chou, A.-K.; Liu, Y.-L.; Lin, K.-H.; Huang, L.-M.; et al. Infectious complications in children with acute lymphoblastic leukemia treated with the Taiwan Pediatric Oncology Group protocol: A 16-year tertiary single-institution experience. Pediatr. Blood Cancer 2017, 64, e26535. [Google Scholar] [CrossRef]
- Abla, O.; Ribeiro, R.C.; Testi, A.M.; Montesinos, P.; Creutzig, U.; Sung, L.; Di Giuseppe, G.; Stephens, D.; Feusner, J.H.; Powell, B.L.; et al. Predictors of thrombohemorrhagic early death in children and adolescents with t(15;17)-positive acute promyelocytic leukemia treated with ATRA and chemotherapy. Ann. Hematol. 2017, 96, 1449–1456. [Google Scholar] [CrossRef]
- Orgel, E.; Genkinger, J.M.; Aggarwal, D.; Sung, L.; Nieder, M.; Ladas, E.J. Association of body mass index and survival in pediatric leukemia: A meta-analysis. Am. J. Clin. Nutr. 2016, 103, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Amankwah, E.K.; Saenz, A.M.; Hale, G.A.; Brown, P.A. Association between body mass index at diagnosis and pediatric leukemia mortality and relapse: A systematic review and meta-analysis. Leuk. Lymphoma 2016, 57, 1140–1148. [Google Scholar] [CrossRef]
- Saenz, A.M.; Stapleton, S.; Hernandez, R.G.; Hale, G.A.; Goldenberg, N.A.; Schwartz, S.; Amankwah, E.K. Body Mass Index at Pediatric Leukemia Diagnosis and the Risks of Relapse and Mortality: Findings from a Single Institution and Meta-analysis. J. Obes. 2018, 2018, 7048078. [Google Scholar] [CrossRef]
- Hirose, E.Y.; de Molla, V.C.; Gonçalves, M.V.; Pereira, A.D.; Szor, R.S.; da Fonseca, A.R.B.M.; Fatobene, G.; Serpa, M.G.; Xavier, E.M.; Tucunduva, L.; et al. The impact of pretransplant malnutrition on allogeneic hematopoietic stem cell transplantation outcomes. Clin. Nutr. ESPEN 2019, 33, 213–219. [Google Scholar] [CrossRef]
- Ren, G.; Cai, W.; Wang, L.; Huang, J.; Yi, S.; Lu, L.; Wang, J. Impact of body mass index at different transplantation stages on postoperative outcomes in patients with hematological malignancies: A meta-analysis. Bone Marrow Transplant. 2018, 53, 708–721. [Google Scholar] [CrossRef]
- Ghafoor, T. Prognostic factors in pediatric Hodgkin lymphoma: Experience from a developing country. Leuk. Lymphoma 2020, 61, 344–350. [Google Scholar] [CrossRef]
- González, H.R.; Mejía, S.A.; Ortiz, J.O.C.; Gutiérrez, A.P.O.; López, J.E.B.; Quintana, J.E.F. Malnutrition in paediatric patients with leukaemia and lymphoma: A retrospective cohort study. Ecancermedicalscience 2021, 15, 1327. [Google Scholar] [CrossRef] [PubMed]
- Bs, J.M.S.; Cyrus, J.; Horvai, A.; Hazard, F.K.G.; Neuhaus, J.; Matthay, K.K.; Goldsby, R.; Marina, N.; DuBois, S.G. Predictors of acute chemotherapy-associated toxicity in patients with Ewing sarcoma. Pediatr. Blood Cancer 2012, 59, 611–616. [Google Scholar] [CrossRef]
- Goldstein, G.; Shemesh, E.; Frenkel, T.; Jacobson, J.M.; Toren, A. Abnormal body mass index at diagnosis in patients with Ewing sarcoma is associated with inferior tumor necrosis. Pediatr. Blood Cancer 2015, 62, 1892–1896. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.R.; Vijarnsorn, C.; Potts, J.; Milner, R.; Sandor, G.G.; Fryer, C. Anthracycline induced cardiac toxicity in pediatric Ewing sarcoma: A longitudinal study. Pediatr. Blood Cancer 2013, 60, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, P.; Seidel, K.; Krailo, M.; Mascarenhas, L.; Meyers, P.; Marina, N.; Conrad, E.U.; Hawkins, D.S. Body mass index (BMI) at diagnosis is associated with surgical wound complications in patients with localized osteosarcoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2011, 57, 939–942. [Google Scholar] [CrossRef] [PubMed]
- Altaf, S.; Enders, F.; Jeavons, E.; Krailo, M.; Barkauskas, D.A.; Meyers, P.; Arndt, C. High-BMI at diagnosis is associated with inferior survival in patients with osteosarcoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2013, 60, 2042–2046. [Google Scholar] [CrossRef]
- Rodeberg, D.A.; Stoner, J.A.; Garcia-Henriquez, N.; Randall, R.L.; Spunt, S.L.; Arndt, C.A.; Kao, S.; Paidas, C.N.; Million, L.; Hawkins, D.S. Tumor volume and patient weight as predictors of outcome in children with intermediate risk rhabdomyosarcoma: A report from Children’s Oncology Group. Cancer 2011, 117, 2541–2550. [Google Scholar] [CrossRef]
- Burke, M.E.; Lyden, E.R.; Meza, J.L.; Ladas, E.J.; Dasgupta, R.; Wiegner, E.A.; Arndt, C.A. Does body mass index at diagnosis or weight change during therapy predict toxicity or survival in intermediate risk rhabdomyosarcoma? A report from the Children’s Oncology Group soft tissue sarcoma committee. Pediatr. Blood Cancer 2013, 60, 748–753. [Google Scholar] [CrossRef]
- Fernandez, C.V.; Anderson, J.; Breslow, N.E.; Dome, J.S.; Grundy, P.; Perlman, E.; Green, D.M.; The National Wilms Tumor Study Group/Children’s Oncology Group. Anthropomorphic measurements and event-free survival in patients with favorable histology Wilms tumor: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2009, 52, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Small, A.G.; Thwe, L.M.; Byrne, J.A.; Lau, L.; Chan, A.; Craig, E.M.; Cowell, C.T.; Garnett, S.P. Neuroblastoma, Body Mass Index, and Survival: A retrospective analysis. Medicine 2015, 94, e713. [Google Scholar] [CrossRef] [PubMed]
- Yariş, N.; Akyüz, C.; Coşkun, T.; Kutluk, T.; Büyükpamukçu, M. Nutritional status of children with cancer and its effects on survival. Turk. J. Pediatr. 2002, 44, 35–39. [Google Scholar] [PubMed]
- Tenardi, R.D.; Frühwald, M.C.; Jürgens, H.; Hertroijs, D.; Bauer, J. Nutritional status of children and young adults with Ewing sarcoma or osteosarcoma at diagnosis and during multimodality therapy. Pediatr. Blood Cancer 2012, 59, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Triarico, S.; Rinninella, E.; Natale, L.; Brizi, M.G.; Cintoni, M.; Raoul, P.; Maurizi, P.; Attinà, G.; Mastrangelo, S.; et al. Clinical Impact of Nutritional Status and Sarcopenia in Pediatric Patients with Bone and Soft Tissue Sarcomas: A Pilot Retrospective Study (SarcoPed). Nutrients 2022, 14, 383. [Google Scholar] [CrossRef] [PubMed]
- Kadenczki, O.; Nagy, A.; Kiss, C. Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary. Int. J. Environ. Res. Public Health 2021, 18, 1478. [Google Scholar] [CrossRef] [PubMed]
- Loeffen, E.A.H.; Brinksma, A.; Miedema, K.G.E.; de Bock, G.H.; Tissing, W.J.E. Clinical implications of malnutrition in childhood cancer patients—infections and mortality. Support. Care Cancer 2015, 23, 143–150. [Google Scholar] [CrossRef]
- Triarico, S.; Rinninella, E.; Cintoni, M.; Capozza, A.M.; Mastrangelo, S.; Mele, M.C.; Ruggiero, A. Impact of malnutrition on survival and infections among pediatric patients with cancer: A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1165–1175. [Google Scholar]
- De Araujo, O.L.; Da Trindade, K.M.; Trompieri, N.M.; Fontenele, J.B.; Felix, F.H.C. Analysis of survival and prognostic factors of pediatric patients with brain tumor. J. Pediatr. 2011, 87, 425–432. [Google Scholar] [CrossRef]
- Lee, J.W.; Cho, B. Prognostic factors and treatment of pediatric acute lymphoblastic leukemia. Korean J. Pediatr. 2017, 60, 129–137. [Google Scholar] [CrossRef]
- Okui, T. Socioeconomic Predictors of Trends in Cancer Mortality among Municipalities in Japan, 2010–2019. Asian Pac. J. Cancer Prev. 2021, 22, 499–508. [Google Scholar] [CrossRef]
- Porojnicu, A.C.; Dahlback, A.; Moan, J. Sun Exposure and Cancer Survival in Norway: Changes in the Risk of Death with Season of Diagnosis and Latitude. In Sunlight, Vitamin D and Skin Cancer; Springer: New York, NY, USA, 2008; pp. 43–54. [Google Scholar] [CrossRef]
- Barr, R.D.; Stevens, M. The influence of nutrition on clinical outcomes in children with cancer. Pediatr. Blood Cancer 2020, 67, e28117. [Google Scholar] [CrossRef] [PubMed]
- Viani, K.; Trehan, A.; Manzoli, B.; Schoeman, J. Assessment of nutritional status in children with cancer: A narrative review. Pediatr. Blood Cancer 2020, 67, e28211. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Jürgens, H.; Frühwald, M.C. Important Aspects of Nutrition in Children with Cancer. Adv. Nutr. Int. Rev. J. 2011, 2, 67–77. [Google Scholar] [CrossRef]
- Fanzani, A.; Conraads, V.M.; Penna, F.; Martinet, W. Molecular and cellular mechanisms of skeletal muscle atrophy: An update. J. Cachex-Sarcopenia Muscle 2012, 3, 163–179. [Google Scholar] [CrossRef]
- Prado, C.M.; Antoun, S.; Sawyer, M.B.; Baracos, E.V. Two faces of drug therapy in cancer: Drug-related lean tissue loss and its adverse consequences to survival and toxicity. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 250–254. [Google Scholar] [CrossRef]
- Tah, P.C.; Shanita, S.N.; Poh, B.K. Nutritional status among pediatric cancer patients: A comparison between hematological malignancies and solid tumors. J. Spéc. Pediatr. Nurs. 2012, 17, 301–311. [Google Scholar] [CrossRef]
- Hopkins, J.; Sawyer, M.B. A review of body composition and pharmacokinetics in oncology. Expert Rev. Clin. Pharmacol. 2017, 10, 947–956. [Google Scholar] [CrossRef]
- Hoed, M.A.H.D.; Pluijm, S.M.F.; De Groot-Kruseman, H.A.; Winkel, M.L.T.; Fiocco, M.; Akker, E.V.D.; Hoogerbrugge, P.; Berg, H.V.D.; Leeuw, J.; Bruin, M.; et al. The negative impact of being underweight and weight loss on survival of children with acute lymphoblastic leukemia. Haematologica 2015, 100, 62–69. [Google Scholar] [CrossRef]
- Horowitz, N.S.; Wright, A.A. Impact of obesity on chemotherapy management and outcomes in women with gynecologic malignancies. Gynecol. Oncol. 2015, 138, 201–206. [Google Scholar] [CrossRef]
- Silvestris, N.; Argentiero, A.; Natalicchio, A.; D’Oronzo, S.; Beretta, G.; Acquati, S.; Adinolfi, V.; Di Bartolo, P.; Danesi, R.; Faggiano, A.; et al. Antineoplastic dosing in overweight and obese cancer patients: An Associazione Italiana Oncologia Medica (AIOM)/Associazione Medici Diabetologi (AMD)/Società Italiana Endocrinologia (SIE)/Società Italiana Farmacologia (SIF) multidisciplinary consensus position paper. ESMO Open 2021, 6, 100153. [Google Scholar] [CrossRef]
- Quail, D.F.; Dannenberg, A.J. The obese adipose tissue microenvironment in cancer development and progression. Nat. Rev. Endocrinol. 2019, 15, 139–154. [Google Scholar] [CrossRef] [PubMed]
- LeWitt, M.S.; Dent, M.S.; Hall, K. The Insulin-Like Growth Factor System in Obesity, Insulin Resistance and Type 2 Diabetes Mellitus. J. Clin. Med. 2014, 3, 1561–1574. [Google Scholar] [CrossRef] [PubMed]
- Al-Mansoori, L.; Al-Jaber, H.; Prince, M.S.; Elrayess, M.A. Role of Inflammatory Cytokines, Growth Factors and Adipokines in Adipogenesis and Insulin Resistance. Inflammation 2022, 45, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Stone, T.W.; McPherson, M.; Gail Darlington, L. Obesity and Cancer: Existing and New Hypotheses for a Causal Connection. EBioMedicine 2018, 30, 14–28. [Google Scholar] [CrossRef]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef]
- Casabonne, D.; Benavente, Y.; Costas, L.; Robles, C.; Gonzalez-Barca, E.; Banda, E.; Alonso, E.; Aymerich, M.; Campo, E.; Marcos-Gragera, R.; et al. Insulin-like growth factor levels and chronic lymphocytic leukaemia: Results from the MCC -Spain and EpiLymph-Spain studies. Br. J. Haematol. 2019, 185, 608–612. [Google Scholar] [CrossRef]
- Orgel, E.; Sea, J.L.; Mittelman, S.D. Mechanisms by Which Obesity Impacts Survival from Acute Lymphoblastic Leukemia. J. Natl. Cancer Inst. Monogr. 2019, 2019, 152–156. [Google Scholar] [CrossRef]
- Fabozzi, F.; Trovato, C.M.; Diamanti, A.; Mastronuzzi, A.; Zecca, M.; Tripodi, S.I.; Masetti, R.; Leardini, D.; Muratore, E.; Barat, V.; et al. Management of Nutritional Needs in Pediatric Oncology: A Consensus Statement. Cancers 2022, 14, 3378. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Totadri, S.; Trehan, A.; Mahajan, D.; Viani, K.; Barr, R.; Ladas, E.J. Validation of an algorithmic nutritional approach in children undergoing chemotherapy for cancer. Pediatr. Blood Cancer 2019, 66, e27980. [Google Scholar] [CrossRef]
- Elbarbary, N.S.; Ismail, E.A.R.; Farahat, R.K.; El-Hamamsy, M. ω-3 fatty acids as an adjuvant therapy ameliorates methotrexate-induced hepatotoxicity in children and adolescents with acute lymphoblastic leukemia: A randomized placebo-controlled study. Nutrition 2016, 32, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Hagag, A.; AbdElaal, A.; Elfaragy, M.; Hassan, S.; Elzamarany, E. Therapeutic Value of Black Seed Oil in Methotrexate Hepatotoxicity in Egyptian Children with Acute Lymphoblastic Leukemia. Infect. Disord. Drug Targets 2015, 15, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; Smith, M.; Henderson, M.; Reid, U.; Lewis, I.; Kinsey, S.; Allgar, V.; Bowers, D.; Picton, S.V. The effect of high-dose enteral glutamine on the incidence and severity of mucositis in paediatric oncology patients. Eur. J. Clin. Nutr. 2009, 63, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Mukherjee, P.; Kiebish, A.M.; Markis, W.T.; Mantis, J.G.; Seyfried, T.N. The calorically restricted ketogenic diet, an effective alternative therapy for malignant brain cancer. Nutr. Metab. 2007, 4, 5. [Google Scholar] [CrossRef]
- Touyz, L.M.; Cohen, J.; Neville, K.A.; Wakefield, C.E.; Garnett, S.P.; Mallitt, K.-A.; Grech, A.M.; Cohn, R.J. Changes in body mass index in long-term survivors of childhood acute lymphoblastic leukemia treated without cranial radiation and with reduced glucocorticoid therapy. Pediatr. Blood Cancer 2017, 64, e26344. [Google Scholar] [CrossRef]
- Fleming, C.A.; Cohen, J.; Murphy, A.; Wakefield, C.E.; Cohn, R.J.; Naumann, F.L. Parent feeding interactions and practices during childhood cancer treatment. A qualitative investigation. Appetite 2015, 89, 219–225. [Google Scholar] [CrossRef]
- Zhang, F.F.; Liu, S.; Chung, M.; Kelly, M.J. Growth patterns during and after treatment in patients with pediatric ALL: A meta-analysis. Pediatr. Blood Cancer 2015, 62, 1452–1460. [Google Scholar] [CrossRef]
- Chaput, C.; Beaulieu-Gagnon, S.; Bélanger, V.; Drouin, S.; Bertout, L.; Lafrance, L.; Olivier, C.; Robitaille, M.; Laverdière, C.; Sinnett, D.; et al. Research- and Practice-Based Nutrition Education and Cooking Workshops in Pediatric Oncology: Protocol for Implementation and Development of Curriculum. JMIR Res. Protoc. 2018, 7, e2. [Google Scholar] [CrossRef]
- Beaulieu-Gagnon, S.; Bélanger, V.; Meloche, C.; Curnier, D.; Sultan, S.; Laverdière, C.; Sinnett, D.; Marcil, V. Nutrition education and cooking workshops for families of children with cancer: A feasibility study. BMC Nutr. 2019, 5, 52. [Google Scholar] [CrossRef]
- Bélanger, V.; Delorme, J.; Napartuk, M.; Bouchard, I.; Meloche, C.; Curnier, D.; Sultan, S.; Laverdière, C.; Sinnett, D.; Marcil, V. Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study. Nutrients 2022, 14, 1024. [Google Scholar] [CrossRef]
- Li, R.; Raber, M.; Chandra, J.; Tee, S.-H.; Balter, K. Developing a Healthy Web-Based Cookbook for Pediatric Cancer Patients and Survivors: Rationale and Methods. JMIR Res. Protoc. 2015, 4, e37. [Google Scholar] [CrossRef] [PubMed]
- Wartenberg, L.; Raber, M.; Chandra, J. Unique features of a web-based nutrition website for childhood cancer populations: Availability, features, and content. (Preprint). J. Med. Internet Res. 2021, 23, e24515. [Google Scholar] [CrossRef]
- Touyz, L.M.; Cohen, J.; Garnett, S.P.; Grech, A.M.; Gohil, P.; Cohn, R.J.; Wakefield, C.E. Acceptability and feasibility of a parent-targeted dietary intervention in young survivors of childhood cancer: “Reboot”. Pediatr. Blood Cancer 2020, 67, e28533. [Google Scholar] [CrossRef] [PubMed]
- Chargi, N.; Bashiri, F.; Wendrich, A.W.; Smid, E.J.; de Jong, P.A.; Huitema, A.D.R.; Devriese, L.A.; de Bree, R. Image-based analysis of skeletal muscle mass predicts cisplatin dose-limiting toxicity in patients with locally advanced head and neck cancer. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 3685–3694. [Google Scholar] [CrossRef] [PubMed]
- Hilmi, M.; Jouinot, A.; Burns, R.; Pigneur, F.; Mounier, R.; Gondin, J.; Neuzillet, C.; Goldwasser, F. Body composition and sarcopenia: The next-generation of personalized oncology and pharmacology? Pharmacol. Ther. 2019, 196, 135–159. [Google Scholar] [CrossRef] [PubMed]
- Celik, E.; Suzan, V.; Samanci, N.S.; Suzan, A.A.; Karadag, M.; Sahin, S.; Aslan, M.S.; Yavuzer, H.; Demirci, N.S.; Doventas, A.; et al. Sarcopenia assessment by new EWGSOP2 criteria for predicting chemotherapy dose-limiting toxicity in patients with gastrointestinal tract tumors. Eur. Geriatr. Med. 2022, 13, 267–274. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Ai, L.; Zhang, H.; Li, G.; Wang, Z.; Jiang, X.; Yan, G.; Liu, Y.; Wang, C.; et al. Linear Skeletal Muscle Index and Muscle Attenuation May Be New Prognostic Factors in Colorectal Carcinoma Treated by Radical Resection. Front. Oncol. 2022, 12, 839899. [Google Scholar] [CrossRef]
- Division of Nutrition PA and ONC for CDP and HP. Obesity Is a Common, Serious, and Costly Disease. 2022. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 1 January 2020).


{kind=link}
| Cancer Site | N Studies | Outcomes |
|---|---|---|
| Leukemia | Meta-analyses (N = 5); 5 more recent original studies |
|
| Hodgkin lymphoma | 2 |
|
| Ewing sarcoma | 3 |
|
| Osteosarcoma | 2 |
|
| Rhabdomyosarcoma | 2 |
|
| Neuroblastoma and Wilms tumors | 2 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karalexi, M.A.; Markozannes, G.; Tagkas, C.F.; Katsimpris, A.; Tseretopoulou, X.; Tsilidis, K.K.; Spector, L.G.; Schüz, J.; Siahanidou, T.; Petridou, E.T.; et al. Nutritional Status at Diagnosis as Predictor of Survival from Childhood Cancer: A Review of the Literature. Diagnostics 2022, 12, 2357. https://doi.org/10.3390/diagnostics12102357
Karalexi MA, Markozannes G, Tagkas CF, Katsimpris A, Tseretopoulou X, Tsilidis KK, Spector LG, Schüz J, Siahanidou T, Petridou ET, et al. Nutritional Status at Diagnosis as Predictor of Survival from Childhood Cancer: A Review of the Literature. Diagnostics. 2022; 12(10):2357. https://doi.org/10.3390/diagnostics12102357
Chicago/Turabian StyleKaralexi, Maria A., Georgios Markozannes, Christos F. Tagkas, Andreas Katsimpris, Xanthippi Tseretopoulou, Konstantinos K. Tsilidis, Logan G. Spector, Joachim Schüz, Tania Siahanidou, Eleni Th. Petridou, and et al. 2022. "Nutritional Status at Diagnosis as Predictor of Survival from Childhood Cancer: A Review of the Literature" Diagnostics 12, no. 10: 2357. https://doi.org/10.3390/diagnostics12102357