
Intra- and Inter-Reader Variations in Lung Nodule Measurements: Influences of Nodule Size, Location, and Observers
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Nodule Selection
2.2. CT Scanning
2.3. Linear and Volumetric Measurements of the Nodule
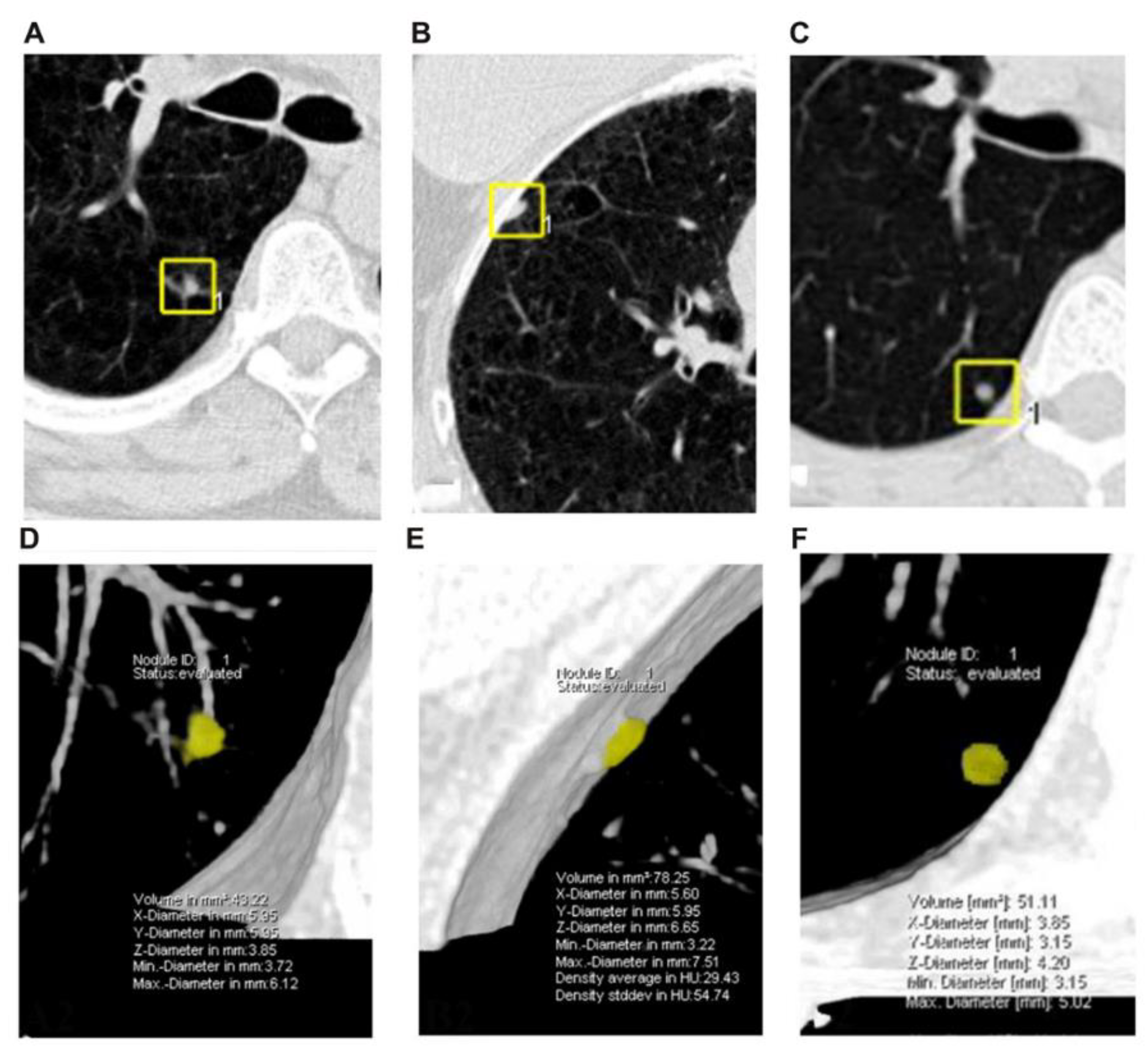
2.4. Definitions of Nodules
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients and Nodules
3.2. Intraclass Correlation Coefficients
3.3. Bland-Altman Plots for All Measurements
3.4. Bland-Altman Plots Deriving from Different Nodule Size
3.5. Bland-Altman Plots Deriving from Different Nodule Types
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted LifeYears for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar]
- Gasparri, R.; Guaglio, A.; Spaggiari, L. Early Diagnosis of Lung Cancer: The Urgent Need of a Clinical Test. J. Clin. Med. 2022, 11, 4398. [Google Scholar] [CrossRef]
- Hoffman, R.M.; Atallah, R.P.; Struble, R.D.; Badgett, R.G. Lung Cancer Screening with Low-Dose CT: A Meta-Analysis. J. Gen. Intern. Med. 2020, 35, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Oudkerk, M.; Liu, S.Y.; Heuvelmans, M.A.; Walter, J.E.; Field, J.K. Lung cancer LDCT screening and mortality reduction—Evidence, pitfalls and future perspectives. Nat. Rev. Clin. Oncol. 2021, 18, 135–151. [Google Scholar] [CrossRef]
- Becker, N.; Motsch, E.; Trotter, A.; Heussel, C.P.; Delorme, S. Lung cancer mortality reduction by LDCT screening—Results from the randomized German LUSI trial. Int. J. Cancer 2019, 146, 1503–1513. [Google Scholar] [CrossRef]
- Wood, D.E.; Kazerooni, E.A.; Aberle, D.; Berman, A.; Brown, L.M.; Eapen, G.A.; Ettinger, D.S.; Ferguson, J.S.; Hou, L.; Kadaria, D.; et al. NCCN Guidelines® Insights: Lung Cancer Screening, Version 1.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 754–764. [Google Scholar] [CrossRef]
- Macmahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef]
- Han, D.; Heuvelmans, M.A.; Oudkerk, M. Volume versus diameter assessment of small pulmonary nodules in CT lung cancer screening. Transl. Lung Cancer Res. 2017, 6, 52–61. [Google Scholar] [CrossRef]
- Devaraj, A.; van Ginneken, B.; Nair, A.; Baldwin, D. Use of Volumetry for Lung Nodule Management: Theory and Practice. Radiology 2017, 284, 630–644. [Google Scholar] [CrossRef] [PubMed]
- Bankier, A.A.; MacMahon, H.; Goo, J.M.; Rubin, G.D.; Schaefer-Prokop, C.M.; Naidich, D.P. Recommendations for Measuring Pulmonary Nodules at CT: A Statement from the Fleischner Society. Radiology 2017, 285, 584–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gierada, D.S.; Rydzak, C.E.; Zei, M.; Rhea, L. Improved Interobserver Agreement on Lung-RADS Classification of Solid Nodules Using Semiautomated CT Volumetry. Radiology 2020, 297, 200302. [Google Scholar] [CrossRef]
- Sui, X.; Meinel, F.G.; Song, W.; Xu, X.; Wang, Z.; Wang, Y.; Jin, Z.; Chen, J.; Vliegenthart, R.; Schoepf, U.J. Detection and size measurements of pulmonary nodules in ultra-low-dose CT with iterative reconstruction compared to low dose CT. Eur. J. Radiol. 2016, 85, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Ying, R.Z.; Ooijen, P.; Dorrius, M.; Heuvelmans, M.; Oudkerk, M. Comparison of three software systems for semi-automatic volumetry of pulmonary nodules on baseline and follow-up CT examinations. Acta Radiol. 2014, 55, 691–698. [Google Scholar]
- Willemink, M.J.; Leiner, T.; Budde, R.P.J.; de Kort, F.P.L.; Vliegenthart, R.; van Ooijen, P.M.A.; Oudkerk, M.; de Jong, P.A. Systematic error in lung nodule volumetry: Effect of iterative reconstruction versus filtered back projection at different CT parameters. Ajr Am. J. Roentgenol. 2012, 199, 1241–1246. [Google Scholar] [CrossRef]
- WHO. WHO Handbook for Reporting Results of Cancer Treatment; World Health Organization Offset Publication: Geneva, Switzerland, 1979; p. 48. [Google Scholar]
- James, K.; Eisenhauer, E.; Christian, M.; Terenziani, M.; Vena, D.; Muldal, A.; Therasse, P. Measuring response in solid tumors: Unidimensional versus bidimensional measurement. J. Natl. Cancer Inst. 1999, 91, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.M.; Joa, J.A.; Cabrales, L.E.; Pupo, A.E.; Schneider, B.; Kondakci, S.; Ciria, H.M.; Reyes, J.B.; Jarque, M.V.; Mateus, M.A.; et al. Is cancer a pure growth curve or does it follow a kinetics of dynamical structural transformation? BMC Cancer 2017, 17, 174. [Google Scholar] [CrossRef]
- Chelala, L.; Hossain, R.; Kazerooni, E.A.; Christensen, J.D.; Dyer, D.S.; White, C.S. Lung-RADS Version 1.1: Challenges and a Look Ahead, From the AJR Special Series on Radiology Reporting and Data Systems. AJR Am. J. Roentgenol. 2021, 216, 1411–1422. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Gould, M.K.; Fletcher, J.; Iannettoni, M.; Lynch, W.R.; Midthun, D.E.; Naidich, D.P.; Ost, D.E. Evaluation of Patients with Pulmonary Nodules: When Is It Lung Cancer? ACCP Evidence-Based Clinical Practice Guidelines (2nd edition). Chest 2007, 132, IL. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.K.; Donington, J.; Lynch, W.R.; Mazzone, P.J.; Midthun, D.E.; Naidich, D.P.; Wiener, R.S. Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, e93S–e120S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, S.R.; Jhaveri, K.S.; Sanjay, S.; Hahn, P.F.; Halpern, E.F.; Sumner, J.E. CT tumor measurement for therapeutic response assessment: Comparison of unidimensional, bidimensional, and volumetric techniques initial observations. Radiology 2002, 225, 416. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Rodriguez, J.; Diaz-Gonzalez, J.A.; Garzon, C.; Gurpide, A.; Arbea, L.; Gil-Bazo, I.; Navarro, V.; Cambeiro, M.; Nicolas, A.I.; et al. Comparison of unidimensional and bidimensional measurements in metastatic non-small cell lung cancer. Br. J. Cancer 2002, 87, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Fraioli, F.; Bertoletti, L.; Napoli, A.; Calabrese, F.A.; Masciangelo, R.; Cortesi, E.; Catalano, C.; Passariello, R. Volumetric evaluation of therapy response in patients with lung metastases. Preliminary results with a computer system (CAD) and comparison with unidimensional measurements. Radiol. Med. 2006, 111, 365–375. [Google Scholar] [CrossRef]
- Revel, M.P.; Lefort, C.; Bissery, A.; Bienvenu, M.; Aycard, L.; Chatellier, G.; Frija, G. Pulmonary nodules: Preliminary experience with three-dimensional evaluation. Radiology 2004, 231, 459–466. [Google Scholar] [CrossRef]
- Ko, J.P.; Marcus, R.; Bomsztyk, E.; Babb, J.S.; Stefanescu, C.; Kaur, M.; Naidich, D.P.; Rusinek, H. Effect of blood vessels on measurement of nodule volume in a chest phantom. Radiology 2006, 239, 79–85. [Google Scholar] [CrossRef]
- Goodman, L.R.; Gulsun, M.; Washington, L.; Nagy, P.G.; Piacsek, K.L. Inherent variability of CT lung nodule measurements in vivo using semiautomated volumetric measurements. AJR Am. J. Roentgenol. 2006, 186, 989–994. [Google Scholar] [CrossRef]
- Volterrani, L.; Mazzei, M.A.; Scialpi, M.; Carcano, M.; Carbone, S.F.; Ricci, V.; Guazzi, G.; Lupattelli, L. Three-dimensional analysis of pulmonary nodules by MSCT with Advanced Lung Analysis (ALA1) software. La Radiol. Med. 2006, 111, 343–354. [Google Scholar] [CrossRef]
- Bolte, H.; Jahnke, T.; Schafer, F.K.; Wenke, R.; Hoffmann, B.; Freitag-Wolf, S.; Dicken, V.; Kuhnigk, J.M.; Lohmann, J.; Voss, S.; et al. Interobserver-variability of lung nodule volumetry considering different segmentation algorithms and observer training levels. Eur. J. Radiol. 2007, 64, 285–295. [Google Scholar] [CrossRef]
- Bogot, N.R.; Kazerooni, E.A.; Kelly, A.M.; Quint, L.E.; Desjardins, B.; Nan, B. Interobserver and intraobserver variability in the assessment of pulmonary nodule size on CT using film and computer display methods. Acad. Radiol. 2005, 12, 948–956. [Google Scholar] [CrossRef] [PubMed]
- Revel, M.P.; Bissery, A.; Bienvenu, M.; Aycard, L.; Lefort, C.; Frija, G. Are two-dimensional CT measurements of small noncalcified pulmonary nodules reliable? Radiology 2004, 231, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, Z.; Shan, F.; Shi, Y.; Xing, W.; Shi, L.; Zhang, X. Intra-observer and inter-observer agreements for the measurement of dual-input whole tumor computed tomography perfusion in patients with lung cancer: Influences of the size and inner-air density of tumors. Thorac. Cancer 2017, 8, 427–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measurements | Reader A | Reader B | |
|---|---|---|---|
| A1 | A2 | ||
| Longest diameter (mm) | 6.4 ± 2.5 (3.4–18.3) | 6.4 ± 2.6 (3.1–18.1) | 6.3 ± 2.5 (3.0–18.0) |
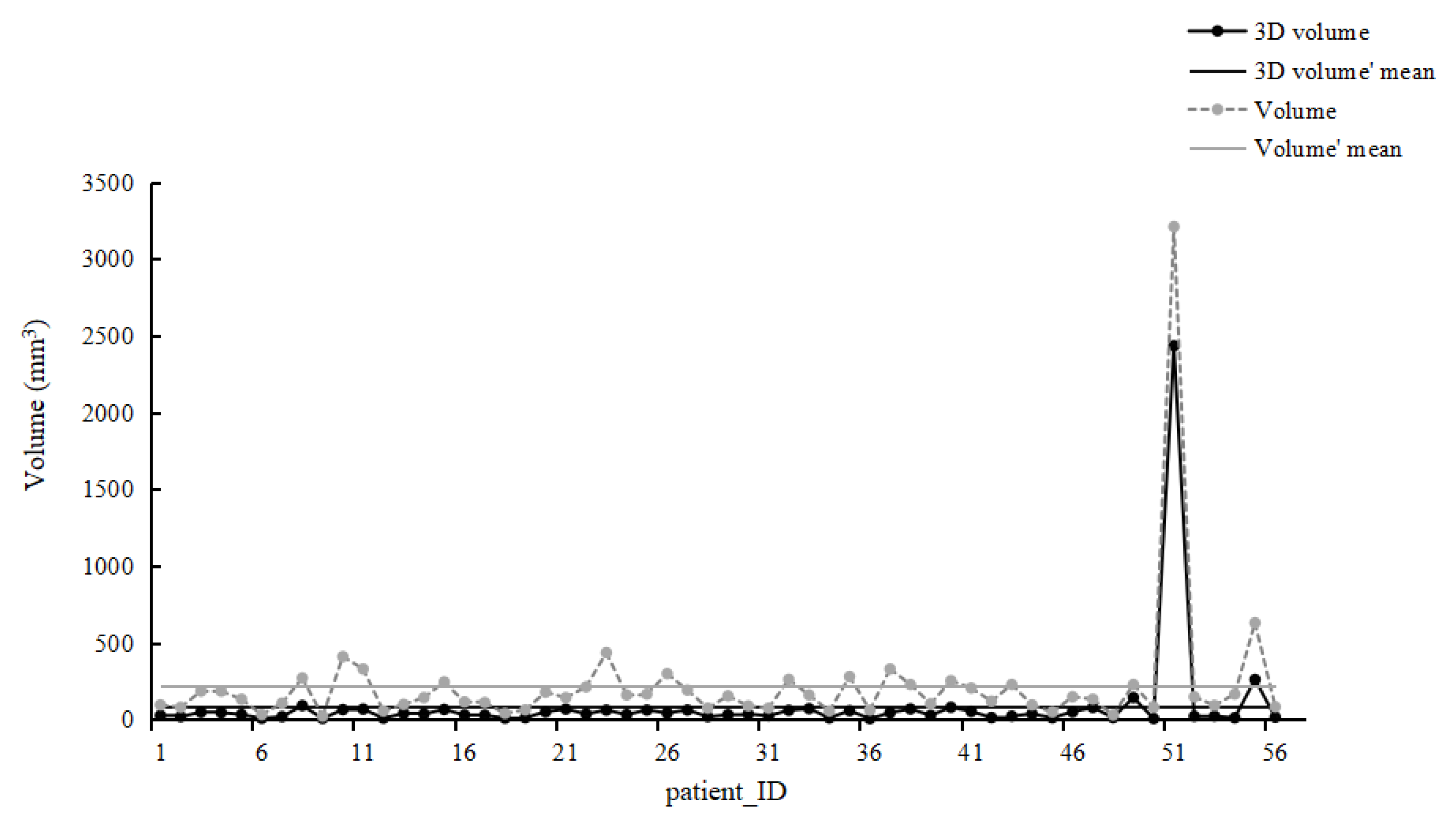
| The calculated volume of the nodule (mm3) | 222.6 ± 457.5 (20.6–3208.9) | 224.7 ± 482.4 (15.6–3104.8) | 212.9 ± 433.8 (14.1–3053.6) |
| 3D semiautomatic volume (mm3) | 86.8 ± 278.4 (4.89–2433.9) | 86.7 ± 278.5 (4.9–2436.3) | 83.5 ± 252.4 (4.4–2179.6) |
| Measurement Comparisons | Overall | By Size(mm) | By Type | |||||
|---|---|---|---|---|---|---|---|---|
| <6 | ≥6 and <8 | ≥8 | Isolated | Juxta-Vascular | Juxta-Pleural | |||
| A1 * | ||||||||
| c_volume-volume ** | 0.916 | 0.773 | 0.552 | 0.989 | 0.968 | 0.639 | 0.794 | |
| A2 | ||||||||
| c_volume-volume | 0.900 | 0.739 | 0.542 | 0.966 | 0.981 | 0.635 | 0.721 | |
| B1 | ||||||||
| c_volume-volume | 0.901 | 0.742 | 0.540 | 0.984 | 0.979 | 0.632 | 0.747 | |
| Overall | ||||||||
| c_volume-volume | 0.905 | 0.748 | 0.546 | 0.977 | 0.976 | 0.642 | 0.748 | |
| Measurement Comparisons | Overall | By Size (mm) | By Type | ||||
|---|---|---|---|---|---|---|---|
| <6 mm | ≥6 and<8 mm | ≥8 mm | Isolated | Juxta-Vascular | Juxta-Pleura | ||
| Intra-reader | |||||||
| A1diameter-A2 diameter * | 0.997 | 0.980 | 0.977 | 0.994 | 0.998 | 0.995 | 0.997 |
| A1 volume-A2 volume * | 1.000 | 0.999 | 0.999 | 1.000 | 1.000 | 0.999 | 1.000 |
| A1_c_volume-A2_c_volume * | 0.992 | 0.983 | 0.984 | 0.988 | 0.994 | 0.999 | 0.991 |
| Inter-reader | |||||||
| A1 diameter-B1 diameter | 0.995 | 0.941 | 0.942 | 0.996 | 0.995 | 0.989 | 0.996 |
| A1volume-B1 volume | 0.994 | 0.987 | 0.987 | 0.994 | 1.000 | 0.986 | 0.993 |
| A1_c_volume-B1_c_volume | 0.998 | 0.944 | 0.958 | 0.997 | 0.986 | 0.992 | 0.999 |
| Measurement Comparisons | Mean Difference % (95% CI) | 95% Limits of Agreement |
|---|---|---|
| Intra-reader | ||
| A1 diameter -A2 diameter * | −0.5 (−1.13, 0.13) | −6.2, 5.2 |
| A1 volume-A2 volume * | 0.2 (−0.25, 0.73) | −4.1, 4.6 |
| A1_c_volume-A2_c_volume * | −1.5 (−3.36, 0.39) | −18.3, 15.3 |
| Inter-reader | ||
| A1 diameter -B1 diameter | −1.5 (−2.48, −0.44) | −10.6, 7.7 |
| A1 volume-B1 volume | −1 (−3.19, 1.25) | −20.9, 18.9 |
| A1_c_volume-B1_c_volume | −4.3 (−7.35, −1.33) | −31.4, 22.7 |
| Measurement Comparisons | <6 mm | ≥6 and <8 mm | ≥8 mm | |||
|---|---|---|---|---|---|---|
| Mean Difference % (95% CI) | 95% Limits of Agreement | Mean Difference % (95% CI) | 95% Limits of Agreement | Mean Difference % (95% CI) | 95% Limits of Agreement | |
| Intra-reader | ||||||
| A1 diameter-A2 diameter | −1 (−2.03, 0.13) | −7.7, 5.8 | 0.2 (−0.57, 0.95) | −3.7, 4.1 | −0.6 (−2.19, 0.97) | −5.7, 4.5 |
| A1 volume-A2 volume | 0.2 (−0.21, 0.68) | −2.5, 3.0 | 0 (−0.96, 0.91) | −4.8, 4.8 | 0.9 (−1.30, 3.02) | −6.1, 7.9 |
| A1_c_volume-A2_c_volume | −2.8 (−6.03, 0.38) | −22.7, 17.1 | 0.6 (−1.71, 2.83) | −11.1, 12.3 | −1.8 (−6.57, 2.90) | −17.2, 13.5 |
| Inter-reader | ||||||
| A1 diameter-B1 diameter | −2 (−3.90, −0.15) | −13.6, 9.6 | −0.4(−1.61, 0.87) | −6.8, 6.0 | −2.1 (−3.13, −1.02) | −5.5, 1.3 |
| A1 volume-B1 volume | −0.7 (−4.04, 2.57) | −21.3, 19.8 | −1.2 (−5.31, 2.94) | −22.4, 20.1 | −1.2 (−6.02, 3.57) | −16.8, 14.3 |
| A1_c_volume-B1_c_volume | −6 (−11.52, −0.51) | −40.2, 28.2 | −1.1 (−4.82, 2.55) | −20.1, 17.9 | −6.2 (−9.37, −3.05) | −16.5, 4.0 |
| Measurement Comparisons | Isolated | Juxta-Vascular | Juxta-Pleural | |||
|---|---|---|---|---|---|---|
| Mean Difference % (95% CI) | 95% Limits of Agreement | Mean Difference % (95%CI) | 95% Limits of Agreement | Mean Difference % (95% CI) | 95% Limits of Agreement | |
| Intra-reader | ||||||
| A1 diameter-A2 diameter * | −0.4 (−0.96, 0.26) | −3.6, 2.9 | −1.5 (−3.52, 0.50) | −9.7, 6.7 | −0.1 (−1.07, 0.96) | −5.7, 5.6 |
| A1 volume-A2 volume * | 0.9 (0.026, 1.78) | −3.8, 5.6 | −0.3 (−0.98, 0.37) | −3.0, 2.4 | −0.1 (−0.91, 0.77) | −4.7, 4.6 |
| A1_c_volume-A2_c_volume * | −1.1 (−2.88, 0.77) | −10.8, 8.7 | −4.5 (−10.41, 1.44) | −28.6, 19.6 | −0.2 (−3.21, 2.87) | −17.0, 16.6 |
| Inter-reader | ||||||
| A1 diameter-B1 diameter | −2.1 (−3.24, −0.92) | −8.3, 4.1 | −2.6 (−5.33, 0.10) | −13.7, 8.4 | −0.2 (−2.01 1.61) | −10.2, 9.8 |
| A1 volume-B1 volume | −0.8 (−4.20, 2.69) | −19.2, 17.6 | −2.6 (−7.27, 1.97) | −21.4, 16.1 | −0.2 (−4.21, 3.79) | −22.3, 21.9 |
| A1_c_volume-B1_c_volume | −6.2 (−9.65, −2.76) | −24.6, 12.2 | −7.7 (−15.66, 0.21) | −40, 24.5 | −0.6 (−5.99, 4.70) | −30.2, 28.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Huang, H.; Zhang, J.; Wang, X.; Han, M.; Ding, C.; Wang, J. Intra- and Inter-Reader Variations in Lung Nodule Measurements: Influences of Nodule Size, Location, and Observers. Diagnostics 2022, 12, 2319. https://doi.org/10.3390/diagnostics12102319
Chen H, Huang H, Zhang J, Wang X, Han M, Ding C, Wang J. Intra- and Inter-Reader Variations in Lung Nodule Measurements: Influences of Nodule Size, Location, and Observers. Diagnostics. 2022; 12(10):2319. https://doi.org/10.3390/diagnostics12102319
Chicago/Turabian StyleChen, Hong, Haozhe Huang, Jianye Zhang, Xuexue Wang, Mengyang Han, Chanjun Ding, and Jinhong Wang. 2022. "Intra- and Inter-Reader Variations in Lung Nodule Measurements: Influences of Nodule Size, Location, and Observers" Diagnostics 12, no. 10: 2319. https://doi.org/10.3390/diagnostics12102319