
Heart Failure and Cardiomyopathies: CT and MR from Basics to Advanced Imaging
 , , , , , , , ,
, , , , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- HF is not a single clinical entity, but it is a complex syndrome theoretically deriving from functional or structural cardiac insults that alter the heart pump. Current criteria combine similar indicators; however, the prevalence of the disease may be underestimated because the diagnosis is accomplished only when the syndrome is clinically evident [24,25,26,27,28].
- Different descriptors have been used in recent years to describe HF (e.g., right, left, or biventricular involvement, cardiac output abnormalities, timing of onset). The most important classification (followed by current guidelines and clinical trials) differentiates between HF with preserved ejection fraction (EF) (HFpEF; i.e., EF > 50%) or reduced EF (HFrEF; i.e., EF < 40%), or with medium involvement of the EF (HFmEF, i.e., EF ranging from 41 to 50%).
- 3.
2. CMR and CCTA Imaging
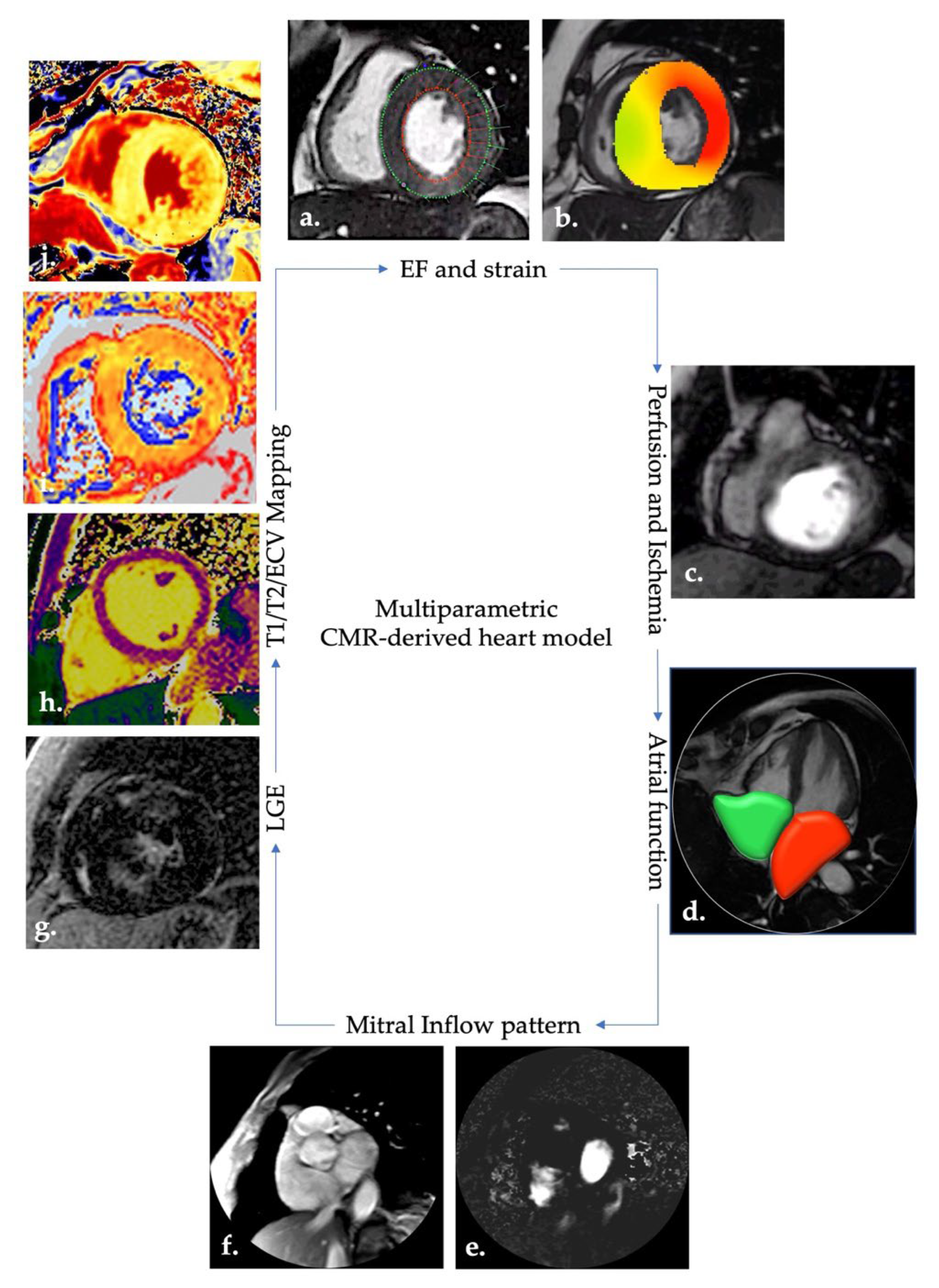
- CMR allows a holistic approach to cardiac patients.
- 2.
- 3.
- Finally, non-invasive stress imaging is class IIb for the study of vitality and ischemia in patients with CAD considered eligible for revascularization [29].
2.1. HF Markers and CMR-CCTA Findings
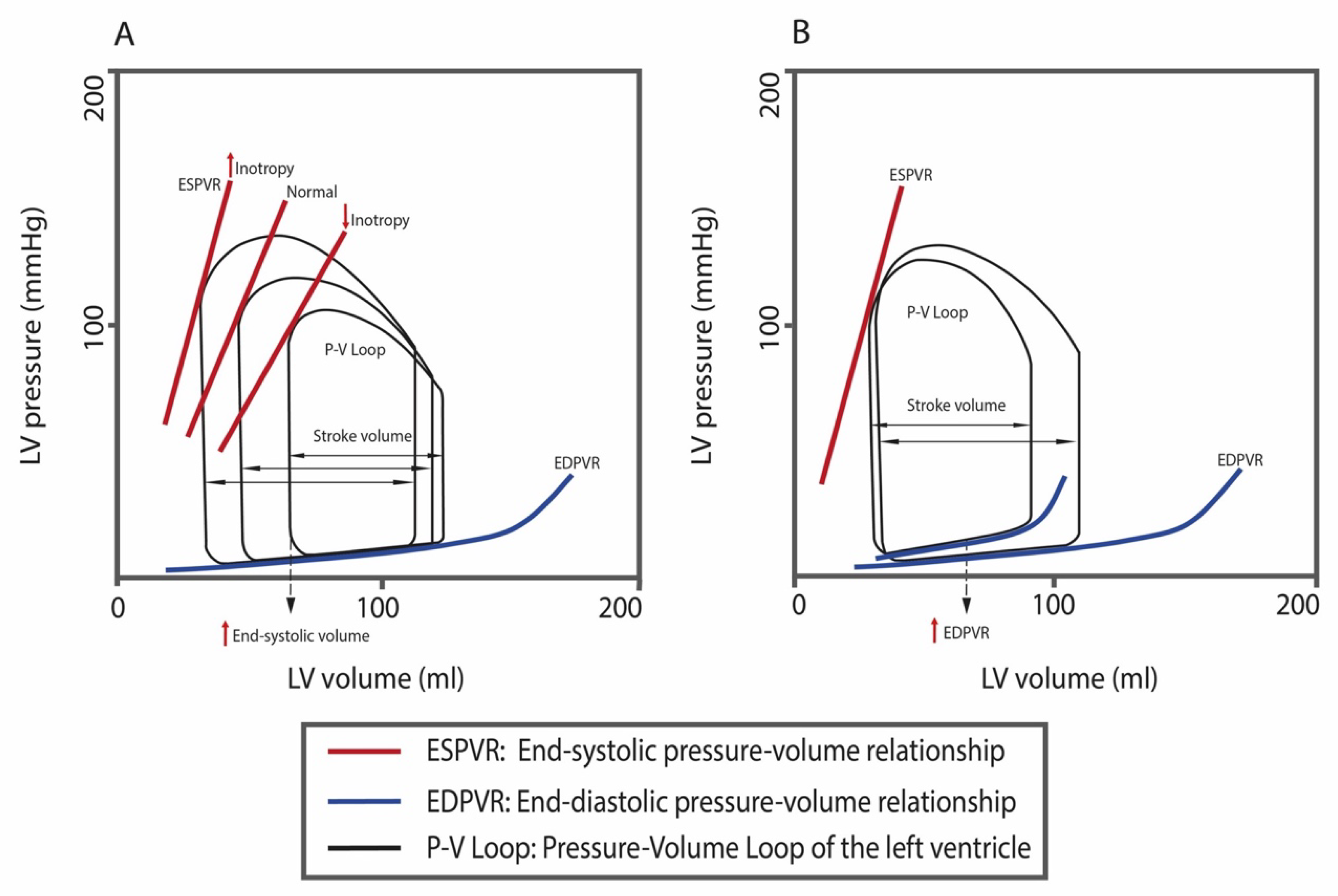
2.1.1. Cardiac Function and Geometry
2.1.2. Subclinical Deformation Anomalies (Myocardial Strain)
2.1.3. Interstitial Matrix, LGE, T1, T2, and ECV Mapping
2.1.4. Transvalvular Inflow Pattern
2.1.5. Left Atrial Volumes and Function
2.1.6. Ischemia
2.1.7. Lung Involvement
3. Cardiomyopathies (CMs) and HF
3.1. Ischemic Heart Disease (IHD)
3.1.1. Acute Coronary Syndrome
3.1.2. Chronic Coronary Syndrome (CCS)
3.1.3. Imaging Tips
3.2. Dilated Cardiomyopathy (DCM)
Imaging Tips
3.3. Hypertrophic Cardiomyopathy (HCM)
Imaging Tips
3.4. Restrictive Cardiomyopathy (RCM)
Imaging Tips
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Braunwald, E. Shattuck lecture—Cardiovascular medicine at the turn of the millennium: Triumphs, concerns, and opportunities. N. Engl. J. Med. 1997, 337, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L. Epidemiology of heart failure. Circ. Res. 2013, 113, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L. The changing landscape of heart failure hospitalizations. J. Am. Coll. Cardiol. 2013, 61, 1268–1270. [Google Scholar] [CrossRef]
- Zakeri, R.; Chamberlain, A.M.; Roger, V.L.; Redfield, M.M. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: A community-based study. Circulation 2013, 128, 1085–1093. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Roger, V.L. Understanding the epidemic of heart failure: Past, present, and future. Curr. Heart Fail Rep. 2014, 11, 404–415. [Google Scholar] [CrossRef]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef]
- Groenewegen, A.; Zwartkruis, V.W.; Cekic, B.; de Boer, R.A.; Rienstra, M.; Hoes, A.W.; Rutten, F.H.; Hollander, M. Incidence of atrial fibrillation, ischaemic heart disease and heart failure in patients with diabetes. Cardiovasc. Diabetol. 2021, 20, 123. [Google Scholar] [CrossRef]
- Roger, V.L. Epidemiology of Heart Failure: A Contemporary Perspective. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- Upadhya, B.; Willard, J.J.; Lovato, L.C.; Rocco, M.V.; Lewis, C.E.; Oparil, S.; Cushman, W.C.; Bates, J.T.; Bello, N.A.; Aurigemma, G.; et al. Incidence and Outcomes of Acute Heart Failure with Preserved versus Reduced Ejection Fraction in SPRINT. Circ. Heart Fail. 2021, 14, e008322. [Google Scholar] [CrossRef]
- Costa, R.; Trepa, M.; Oliveira, M.; Frias, A.; Campinas, A.; Luz, A.; Santos, M.; Torres, S. Heart Failure Incidence Following ST-Elevation Myocardial Infarction. Am. J. Cardiol. 2022, 164, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.J.; O’Driscoll, J.M. Exercise Training in Heart failure with Preserved and Reduced Ejection Fraction: A Systematic Review and Meta-Analysis. Sports Med. Open 2022, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, incidence and survival of heart failure: A systematic review. Heart 2022, 108. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.; Jones, W.S.; Udell, J.A.; Hannan, K.; Bhatt, D.L.; Anker, S.D.; Petrie, M.C.; Vedin, O.; Butler, J.; Hernandez, A.F. Acute Decompensated Heart Failure in the Setting of Acute Coronary Syndrome. JACC Heart Fail. 2022, 10, 404–414. [Google Scholar] [CrossRef]
- Kamil, S.; Sehested, T.S.G.; Houlind, K.; Lassen, J.F.; Gislason, G.H.; Dominguez, H. Incidence of myocardial infarction, heart failure, and cardiovascular mortality in patients with peripheral artery disease: Trends between 1997 and 2016. Eur. Heart J. Qual. Care Clin. Outcomes 2022, qcac022. [Google Scholar] [CrossRef]
- Marume, K.; Ogata, S.; Kaichi, R.; Nakai, M.; Ishii, M.; Mori, T.; Komaki, S.; Kusaka, H.; Toida, R.; Kurogi, K.; et al. Incidence Rate of Hospitalization for Heart Failure in a Japanese City—An Updated Reference for Japan’s Aging Society. Circ. Rep. 2022, 4, 116–122. [Google Scholar] [CrossRef]
- Odegaard, K.M.; Lirhus, S.S.; Melberg, H.O.; Hallen, J.; Halvorsen, S. A nationwide registry study on heart failure in Norway from 2008 to 2018: Variations in lookback period affect incidence estimates. BMC Cardiovasc. Disord. 2022, 22, 88. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, A.V.; Weston, S.A.; Killian, J.M.; Schulte, P.J.; Roger, V.L.; Redfield, M.M.; Blecker, S.B.; Dunlay, S.M. Development of Advanced Heart Failure: A Population-Based Study. Circ. Heart Fail. 2022, 15, e009218. [Google Scholar] [CrossRef]
- Sidney, S.; Quesenberry, C.P., Jr.; Jaffe, M.G.; Sorel, M.; Go, A.S.; Rana, J.S. Heterogeneity in national U.S. mortality trends within heart disease subgroups, 2000–2015. BMC Cardiovasc. Disord. 2017, 17, 192. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Alvarez, B.; Abou Jokh Casas, C.; Agra Bermejo, R.; Cordero, A.; Cid Alvarez, A.B.; Rodriguez Manero, M.; Bouzas Cruz, N.; Garcia Acuna, J.M.; Salgado Barreiro, A.; Gonzalez-Juanatey, J.R. Sex-related differences in long-term mortality and heart failure in a contemporary cohort of patients with NSTEACS. The cardiochus-HSUJ registry. Eur. J. Intern. Med. 2020, 81, 26–31. [Google Scholar] [CrossRef]
- Bottle, A.; Newson, R.; Faitna, P.; Hayhoe, B.; Cowie, M.R. Changes in heart failure management and long-term mortality over 10 years: Observational study. Open Heart 2022, 9, e001888. [Google Scholar] [CrossRef]
- Gori, M.; Marini, M.; De Maria, R.; Gonzini, L.; Gorini, M.; Cassaniti, L.; Benvenuto, M.; Municino, A.; Navazio, A.; Ammirati, E.; et al. Age-related changes in clinical characteristics and outcomes of chronic heart failure outpatients in a cardiology setting. A report from the Italian Network on Heart Failure. Int. J. Cardiol. 2022, 346, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Van Nuys, K.E.; Xie, Z.; Tysinger, B.; Hlatky, M.A.; Goldman, D.P. Innovation in Heart Failure Treatment: Life Expectancy, Disability, and Health Disparities. JACC Heart Fail 2018, 6, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Fuster, V.; Harrington, R.A.; Narula, J.; Eapen, Z.J. Hurst’s The Heart, 14th ed.; McGraw Hill Education: New York, NY, USA, 2017. [Google Scholar]
- Arrigo, M.; Nijst, P.; Rudiger, A. Optimising Heart Failure Therapies in the Acute Setting. Card. Fail. Rev. 2018, 4, 38–42. [Google Scholar] [CrossRef]
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Prim. 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Brito, D.; Vaqar, S.; Chhabra, L. Congestive Heart Failure; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Masip, J.; Frank Peacok, W.; Arrigo, M.; Rossello, X.; Platz, E.; Cullen, L.; Mebazaa, A.; Price, S.; Bueno, H.; Di Somma, S.; et al. Acute Heart Failure in the 2021 ESC Heart Failure Guidelines: A scientific statement from the Association for Acute CardioVascular Care (ACVC) of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force, M.; McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Stough, W.G.; Yancy, C.W.; Young, J.B.; Fonarow, G.C.; et al. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006, 296, 2217–2226. [Google Scholar] [CrossRef]
- Albert, N.M.; Fonarow, G.C.; Abraham, W.T.; Chiswell, K.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; et al. Predictors of delivery of hospital-based heart failure patient education: A report from OPTIMIZE-HF. J. Card. Fail. 2007, 13, 189–198. [Google Scholar] [CrossRef]
- Fonarow, G.C. Strategies to improve the use of evidence-based heart failure therapies: OPTIMIZE-HF. Rev. Cardiovasc. Med. 2004, 5 (Suppl. 1), S45–S54. [Google Scholar]
- Fonarow, G.C.; Abraham, W.T.; Albert, N.M.; Gattis, W.A.; Gheorghiade, M.; Greenberg, B.; O’Connor, C.M.; Yancy, C.W.; Young, J. Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF): Rationale and design. Am. Heart J. 2004, 148, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Abraham, W.T.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Pieper, K.; Sun, J.L.; Yancy, C.W.; et al. Factors identified as precipitating hospital admissions for heart failure and clinical outcomes: Findings from OPTIMIZE-HF. Arch. Intern. Med. 2008, 168, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Fonarow, G.C.; Committee, A.S.A. Quality of care and outcomes in acute decompensated heart failure: The ADHERE Registry. Curr. Heart Fail. Rep. 2004, 1, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Yancy, C.W.; Heywood, J.T.; ADHERE Scientific Advisory Committee, Study Group, and Investigators. Adherence to heart failure quality-of-care indicators in US hospitals: Analysis of the ADHERE Registry. Arch. Intern. Med. 2005, 165, 1469–1477. [Google Scholar] [CrossRef]
- Yancy, C.W.; Lopatin, M.; Stevenson, L.W.; De Marco, T.; Fonarow, G.C.; ADHERE Scientific Advisory Committee and Investigators. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: A report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J. Am. Coll. Cardiol. 2006, 47, 76–84. [Google Scholar] [CrossRef]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef]
- Lund, L.H.; Claggett, B.; Liu, J.; Lam, C.S.; Jhund, P.S.; Rosano, G.M.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Pfeffer, M.A.; et al. Heart failure with mid-range ejection fraction in CHARM: Characteristics, outcomes and effect of candesartan across the entire ejection fraction spectrum. Eur. J. Heart Fail. 2018, 20, 1230–1239. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef]
- Ciancarella, P.; Ciliberti, P.; Santangelo, T.P.; Secchi, F.; Stagnaro, N.; Secinaro, A. Noninvasive imaging of congenital cardiovascular defects. Radiol. Med. 2020, 125, 1167–1185. [Google Scholar] [CrossRef]
- De Rubeis, G.; Marchitelli, L.; Spano, G.; Catapano, F.; Cilia, F.; Galea, N.; Carbone, I.; Catalano, C.; Francone, M. Radiological outpatient’ visits to avoid inappropriate cardiac CT examinations: An 8-year experience report. Radiol. Med. 2021, 126, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Francone, M.; Andreini, D.; Buffa, V.; Cademartiri, F.; Carbone, I.; Clemente, A.; Guaricci, A.I.; Guglielmo, M.; Indolfi, C.; et al. SIRM-SIC appropriateness criteria for the use of Cardiac Computed Tomography. Part 1: Congenital heart diseases, primary prevention, risk assessment before surgery, suspected CAD in symptomatic patients, plaque and epicardial adipose tissue characterization, and functional assessment of stenosis. Radiol. Med. 2021, 126, 1236–1248. [Google Scholar] [CrossRef]
- La Grutta, L.; Toia, P.; Grassedonio, E.; Pasta, S.; Albano, D.; Agnello, F.; Maffei, E.; Cademartiri, F.; Bartolotta, T.V.; Galia, M.; et al. TAVI imaging: Over the echocardiography. Radiol. Med. 2020, 125, 1148–1166. [Google Scholar] [CrossRef]
- Valente, T.; Pignatiello, M.; Sica, G.; Bocchini, G.; Rea, G.; Cappabianca, S.; Scaglione, M. Hemopericardium in the acute clinical setting: Are we ready for a tailored management approach on the basis of MDCT findings? Radiol. Med. 2021, 126, 527–543. [Google Scholar] [CrossRef]
- Silva, M.; Milanese, G.; Cobelli, R.; Manna, C.; Rasciti, E.; Poggesi, S.; Sverzellati, N. CT angiography for pulmonary embolism in the emergency department: Investigation of a protocol by 20 ml of high-concentration contrast medium. Radiol. Med. 2020, 125, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Moroni, C.; Cavigli, E.; Bindi, A.; Caviglioli, C.; Nazerian, P.; Vanni, S.; Miele, V.; Bartolucci, M. Prognostic value of CT pulmonary angiography parameters in acute pulmonary embolism. Radiol. Med. 2021, 126, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M. Role of Cardiac MR Imaging in Cardiomyopathies. J. Nucl. Med. 2015, 56 (Suppl. 4), 39S–45S. [Google Scholar] [CrossRef] [PubMed]
- Takehara, Y. 4D Flow when and how? Radiol. Med. 2020, 125, 838–850. [Google Scholar] [CrossRef]
- Di Cesare, E.; Carerj, S.; Palmisano, A.; Carerj, M.L.; Catapano, F.; Vignale, D.; Di Cesare, A.; Milanese, G.; Sverzellati, N.; Francone, M.; et al. Multimodality imaging in chronic heart failure. Radiol. Med. 2021, 126, 231–242. [Google Scholar] [CrossRef]
- Pontone, G.; Di Cesare, E.; Castelletti, S.; De Cobelli, F.; De Lazzari, M.; Esposito, A.; Focardi, M.; Di Renzi, P.; Indolfi, C.; Lanzillo, C.; et al. Appropriate use criteria for cardiovascular magnetic resonance imaging (CMR): SIC-SIRM position paper part 1 (ischemic and congenital heart diseases, cardio-oncology, cardiac masses and heart transplant). Radiol. Med. 2021, 126, 365–379. [Google Scholar] [CrossRef]
- Russo, V.; Lovato, L.; Ligabue, G. Cardiac MRI: Technical basis. Radiol. Med. 2020, 125, 1040–1055. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, P.; Ruscitti, P.; Cannizzaro, E.; Berardicurti, O.; Conforti, A.; Di Cesare, A.; Di Cola, I.; Giacomelli, R.; Splendiani, A.; Barile, A.; et al. Unenhanced Cardiac Magnetic Resonance may improve detection and prognostication of an occult heart involvement in asymptomatic patients with systemic sclerosis. Sci. Rep. 2022, 12, 5125. [Google Scholar] [CrossRef]
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of myocardial fibrosis with cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2011, 57, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Ajmone Marsan, N.; Bax, J.J. Cardiomyopathies: Myocardial fibrosis assessed by CMR to predict events in HCM. Nat. Rev. Cardiol. 2010, 7, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Osorio, J. New CMR approach to measure diffuse myocardial fibrosis. Nat. Rev. Cardiol. 2010, 7, 542. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Babu-Naravan, S.V.; Chahal, N.S.; Senior, R.; Li, W. Characterisation of left ventricular myocardial fibrosis in adult congenital heart disease by contrast and deformation echocardiography validated by CMR. Int. J. Cardiol. 2013, 166, e16–e18. [Google Scholar] [CrossRef]
- Fontana, M.; Barison, A.; Botto, N.; Panchetti, L.; Ricci, G.; Milanesi, M.; Poletti, R.; Positano, V.; Siciliano, G.; Passino, C.; et al. CMR-verified interstitial myocardial fibrosis as a marker of subclinical cardiac involvement in LMNA mutation carriers. JACC Cardiovasc. Imaging 2013, 6, 124–126. [Google Scholar] [CrossRef]
- Karamitsos, T.D.; Neubauer, S. Detecting diffuse myocardial fibrosis with CMR: The future has only just begun. JACC Cardiovasc. Imaging 2013, 6, 684–686. [Google Scholar] [CrossRef]
- Moravsky, G.; Ofek, E.; Rakowski, H.; Butany, J.; Williams, L.; Ralph-Edwards, A.; Wintersperger, B.J.; Crean, A. Myocardial fibrosis in hypertrophic cardiomyopathy: Accurate reflection of histopathological findings by CMR. JACC Cardiovasc. Imaging 2013, 6, 587–596. [Google Scholar] [CrossRef]
- Su, M.Y.; Lin, L.Y.; Tseng, Y.H.; Chang, C.C.; Wu, C.K.; Lin, J.L.; Tseng, W.Y. CMR-verified diffuse myocardial fibrosis is associated with diastolic dysfunction in HFpEF. JACC Cardiovasc. Imaging 2014, 7, 991–997. [Google Scholar] [CrossRef]
- Ntusi, N.A.B.; Piechnik, S.K.; Francis, J.M.; Ferreira, V.M.; Matthews, P.M.; Robson, M.D.; Wordsworth, P.B.; Neubauer, S.; Karamitsos, T.D. Diffuse Myocardial Fibrosis and Inflammation in Rheumatoid Arthritis: Insights From CMR T1 Mapping. JACC Cardiovasc. Imaging 2015, 8, 526–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lurz, J.A.; Luecke, C.; Lang, D.; Besler, C.; Rommel, K.P.; Klingel, K.; Kandolf, R.; Adams, V.; Schone, K.; Hindricks, G.; et al. CMR-Derived Extracellular Volume Fraction as a Marker for Myocardial Fibrosis: The Importance of Coexisting Myocardial Inflammation. JACC Cardiovasc. Imaging 2018, 11, 38–45. [Google Scholar] [CrossRef]
- Tahir, E.; Starekova, J.; Muellerleile, K.; von Stritzky, A.; Munch, J.; Avanesov, M.; Weinrich, J.M.; Stehning, C.; Bohnen, S.; Radunski, U.K.; et al. Myocardial Fibrosis in Competitive Triathletes Detected by Contrast-Enhanced CMR Correlates with Exercise-Induced Hypertension and Competition History. JACC Cardiovasc. Imaging 2018, 11, 1260–1270. [Google Scholar] [CrossRef]
- Foussier, C.; Barral, P.A.; Jerosh-Herold, M.; Gariboldi, V.; Rapacchi, S.; Gallon, A.; Bartoli, A.; Bentatou, Z.; Guye, M.; Bernard, M.; et al. Quantification of diffuse myocardial fibrosis using CMR extracellular volume fraction and serum biomarkers of collagen turnover with histologic quantification as standard of reference. Diagn. Interv. Imaging 2021, 102, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Wu, T.; Wang, W.; Cheng, W.; Wan, S.; Tian, H.; Chen, T.; Sun, J.; Ren, Y. CMR-Verified Myocardial Fibrosis Is Associated with Subclinical Diastolic Dysfunction in Primary Aldosteronism Patients. Front. Endocrinol. 2021, 12, 672557. [Google Scholar] [CrossRef]
- Daghighi, S.; Chan, A.; Nazarlou, A.; Hasan, Z.; Halimi, M.; Akbarzadeh, F.; Kazemi, D.; Daghighi, M.H.; Fouladi, D.F. Clinical and histopathological outcome of cervical and chest MRI involving non-MRI-conditional cardiac pacemakers: A study using sheep models. Radiol. Med. 2020, 125, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, L.; Mazzocchi, S.; Giomi, A.; Milli, M.; Carpi, R. An operational approach to the execution of MR examinations in patients with CIED. Radiol. Med. 2020, 125, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Seitun, S.; Clemente, A.; Maffei, E.; Toia, P.; La Grutta, L.; Cademartiri, F. Prognostic value of cardiac CT. Radiol. Med. 2020, 125, 1135–1147. [Google Scholar] [CrossRef] [PubMed]
- Seker, M. Prevalence and morphologic features of dual left anterior descending artery subtypes in coronary CT angiography. Radiol. Med. 2020, 125, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Marano, R.; Rovere, G.; Savino, G.; Flammia, F.C.; Carafa, M.R.P.; Steri, L.; Merlino, B.; Natale, L. CCTA in the diagnosis of coronary artery disease. Radiol. Med. 2020, 125, 1102–1113. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Sarai, M.; Narula, J.; Ozaki, Y. Coronary CT angiography and high-risk plaque morphology. Cardiovasc. Interv. Ther. 2013, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Ito, H.; Sarai, M.; Kondo, T.; Kawai, H.; Nagahara, Y.; Harigaya, H.; Kan, S.; Anno, H.; Takahashi, H.; et al. Plaque Characterization by Coronary Computed Tomography Angiography and the Likelihood of Acute Coronary Events in Mid-Term Follow-Up. J. Am. Coll. Cardiol. 2015, 66, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, P.; Cannizzaro, E.; Bruno, F.; Schicchi, N.; Fogante, M.; Agostini, A.; De Donato, M.C.; De Cataldo, C.; Giovagnoni, A.; Barile, A.; et al. Coronary artery disease (CAD) extension-derived risk stratification for asymptomatic diabetic patients: Usefulness of low-dose coronary computed tomography angiography (CCTA) in detecting high-risk profile patients. Radiol. Med. 2020, 125, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; Lopez-Sendon, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef]
- Ledda, R.E.; Milanese, G.; Cademartiri, F.; Maffei, E.; Benedetti, G.; Goldoni, M.; Silva, M.; Sverzellati, N. Association of hepatic steatosis with epicardial fat volume and coronary artery disease in symptomatic patients. Radiol. Med. 2021, 126, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart. J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Chow, B.J.W.; Coyle, D.; Hossain, A.; Laine, M.; Hanninen, H.; Ukkonen, H.; Rajda, M.; Larose, E.; Hartikainen, J.; Mielniczuk, L.; et al. Computed tomography coronary angiography for patients with heart failure (CTA-HF): A randomized controlled trial (IMAGE-HF 1C). Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Schicchi, N.; Fogante, M.; Palumbo, P.; Agliata, G.; Esposto Pirani, P.; Di Cesare, E.; Giovagnoni, A. The sub-millisievert era in CTCA: The technical basis of the new radiation dose approach. Radiol. Med. 2020, 125, 1024–1039. [Google Scholar] [CrossRef]
- Schicchi, N.; Mari, A.; Fogante, M.; Esposto Pirani, P.; Agliata, G.; Tosi, N.; Palumbo, P.; Cannizzaro, E.; Bruno, F.; Splendiani, A.; et al. In vivo radiation dosimetry and image quality of turbo-flash and retrospective dual-source CT coronary angiography. Radiol. Med. 2020, 125, 117–127. [Google Scholar] [CrossRef]
- Agostini, A.; Floridi, C.; Borgheresi, A.; Badaloni, M.; Esposto Pirani, P.; Terilli, F.; Ottaviani, L.; Giovagnoni, A. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual-source CT using a tin filter for spectral shaping at 100 kVp for CoronaVirus Disease 2019 (COVID-19) patients: A feasibility study. Radiol. Med. 2020, 125, 365–373. [Google Scholar] [CrossRef]
- Cristofaro, M.; Busi Rizzi, E.; Piselli, P.; Pianura, E.; Petrone, A.; Fusco, N.; Di Stefano, F.; Schinina, V. Image quality and radiation dose reduction in chest CT in pulmonary infection. Radiol. Med. 2020, 125, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Cicero, G.; Ascenti, G.; Albrecht, M.H.; Blandino, A.; Cavallaro, M.; D’Angelo, T.; Carerj, M.L.; Vogl, T.J.; Mazziotti, S. Extra-abdominal dual-energy CT applications: A comprehensive overview. Radiol. Med. 2020, 125, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Leiner, T.; Bogaert, J.; Friedrich, M.G.; Mohiaddin, R.; Muthurangu, V.; Myerson, S.; Powell, A.J.; Raman, S.V.; Pennell, D.J. SCMR Position Paper (2020) on clinical indications for cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2020, 22, 76. [Google Scholar] [CrossRef]
- Chuang, M.L.; Gona, P.; Hautvast, G.L.; Salton, C.J.; Breeuwer, M.; O’Donnell, C.J.; Manning, W.J. CMR reference values for left ventricular volumes, mass, and ejection fraction using computer-aided analysis: The Framingham Heart Study. J. Magn. Reson. Imaging 2014, 39, 895–900. [Google Scholar] [CrossRef]
- Kawel-Boehm, N.; Hetzel, S.J.; Ambale-Venkatesh, B.; Captur, G.; Francois, C.J.; Jerosch-Herold, M.; Salerno, M.; Teague, S.D.; Valsangiacomo-Buechel, E.; van der Geest, R.J.; et al. Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 87. [Google Scholar] [CrossRef]
- Carr, J.C. Editorial for: “Biventricular Reference Values by Body Surface Area, Age, and Gender in a Large Cohort of Well-Treated Beta-Thalassemia Major Patients without Heart Damage Using a Multiparametric CMR Approach”. J. Magn. Reson. Imaging 2021, 53, 71–72. [Google Scholar] [CrossRef]
- Csecs, I.; Garcia, M.J. Reference CMR values of atrial size and function: Are they similar in the east and the west? Int. J. Cardiol. 2022, 358, 134–135. [Google Scholar] [CrossRef] [PubMed]
- Marchal, P.; Lairez, O.; Cognet, T.; Chabbert, V.; Barrier, P.; Berry, M.; Mejean, S.; Roncalli, J.; Rousseau, H.; Carrie, D.; et al. Relationship between left ventricular sphericity and trabeculation indexes in patients with dilated cardiomyopathy: A cardiac magnetic resonance study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Van Assen, M.; Muscogiuri, G.; Caruso, D.; Lee, S.J.; Laghi, A.; De Cecco, C.N. Artificial intelligence in cardiac radiology. Radiol. Med. 2020, 125, 1186–1199. [Google Scholar] [CrossRef] [PubMed]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’Ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. Radiol. Med. 2021, 126, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Kirienko, M.; Ninatti, G.; Cozzi, L.; Voulaz, E.; Gennaro, N.; Barajon, I.; Ricci, F.; Carlo-Stella, C.; Zucali, P.; Sollini, M.; et al. Computed tomography (CT)-derived radiomic features differentiate prevascular mediastinum masses as thymic neoplasms versus lymphomas. Radiol Med. 2020, 125, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, B.C.; Fentanes, E.; Choi, A.D.; Branch, K.R.; Thomas, D.M. Myocardial Assessment with Cardiac CT: Ischemic Heart Disease and Beyond. Curr. Cardiovasc. Imaging Rep. 2018, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Pierpaolo, P.; Rolf, S.; Manuel, B.-P.; Davide, C.; Dresselaers, T.; Claus, P.; Bogaert, J. Left ventricular global myocardial strain assessment: Are CMR feature-tracking algorithms useful in the clinical setting? Radiol. Med. 2020, 125, 444–450. [Google Scholar] [CrossRef]
- Voigt, J.U.; Cvijic, M. 2- and 3-Dimensional Myocardial Strain in Cardiac Health and Disease. JACC Cardiovasc. Imaging 2019, 12, 1849–1863. [Google Scholar] [CrossRef]
- Geyer, H.; Caracciolo, G.; Abe, H.; Wilansky, S.; Carerj, S.; Gentile, F.; Nesser, H.J.; Khandheria, B.; Narula, J.; Sengupta, P.P. Assessment of myocardial mechanics using speckle tracking echocardiography: Fundamentals and clinical applications. J. Am. Soc. Echocardiogr. 2010, 23, 351–369, quiz 453–355. [Google Scholar] [CrossRef]
- Feisst, A.; Kuetting, D.L.R.; Dabir, D.; Luetkens, J.; Homsi, R.; Schild, H.H.; Thomas, D. Influence of observer experience on cardiac magnetic resonance strain measurements using feature tracking and conventional tagging. Int. J. Cardiol. Heart Vasc. 2018, 18, 46–51. [Google Scholar] [CrossRef]
- Zhang, Y.; Mui, D.; Chirinos, J.A.; Zamani, P.; Ferrari, V.A.; Chen, Y.; Han, Y. Comparing cardiovascular magnetic resonance strain software packages by their abilities to discriminate outcomes in patients with heart failure with preserved ejection fraction. J. Cardiovasc. Magn. Reson. 2021, 23, 55. [Google Scholar] [CrossRef]
- Palumbo, P.; Masedu, F.; De Cataldo, C.; Cannizzaro, E.; Bruno, F.; Pradella, S.; Arrigoni, F.; Valenti, M.; Splendiani, A.; Barile, A.; et al. Real-world clinical validity of cardiac magnetic resonance tissue tracking in primitive hypertrophic cardiomyopathy. Radiol. Med. 2021, 126, 1532–1543. [Google Scholar] [CrossRef]
- Romano, S.; Judd, R.M.; Kim, R.J.; Heitner, J.F.; Shah, D.J.; Shenoy, C.; Evans, K.; Romer, B.; Salazar, P.; Farzaneh-Far, A. Feature-Tracking Global Longitudinal Strain Predicts Mortality in Patients with Preserved Ejection Fraction: A Multicenter Study. JACC Cardiovasc. Imaging 2020, 13, 940–947. [Google Scholar] [CrossRef]
- Romano, S.; Judd, R.M.; Kim, R.J.; Kim, H.W.; Klem, I.; Heitner, J.F.; Shah, D.J.; Jue, J.; White, B.E.; Indorkar, R.; et al. Feature-Tracking Global Longitudinal Strain Predicts Death in a Multicenter Population of Patients with Ischemic and Nonischemic Dilated Cardiomyopathy Incremental to Ejection Fraction and Late Gadolinium Enhancement. JACC Cardiovasc. Imaging 2018, 11, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Houard, L.; Benaets, M.B.; de Meester de Ravenstein, C.; Rousseau, M.F.; Ahn, S.A.; Amzulescu, M.S.; Roy, C.; Slimani, A.; Vancraeynest, D.; Pasquet, A.; et al. Additional Prognostic Value of 2D Right Ventricular Speckle-Tracking Strain for Prediction of Survival in Heart Failure and Reduced Ejection Fraction: A Comparative Study with Cardiac Magnetic Resonance. JACC Cardiovasc Imaging 2019, 12, 2373–2385. [Google Scholar] [CrossRef] [PubMed]
- Kraigher-Krainer, E.; Shah, A.M.; Gupta, D.K.; Santos, A.; Claggett, B.; Pieske, B.; Zile, M.R.; Voors, A.A.; Lefkowitz, M.P.; Packer, M.; et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2014, 63, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Fang, Z.; Wang, H.; Schoepf, U.J.; Emrich, T.; Giovagnoli, D.; Biles, E.; Zhou, Z.; Du, Z.; Liu, T.; et al. Quantitative analysis of three-dimensional left ventricular global strain using coronary computed tomography angiography in patients with heart failure: Comparison with 3T cardiac MR. Eur. J. Radiol. 2021, 135, 109485. [Google Scholar] [CrossRef] [PubMed]
- Craft, J.; Li, Y.; Bhatti, S.; Cao, J.J. How to do left atrial late gadolinium enhancement: A review. Radiol. Med. 2021, 126, 1159–1169. [Google Scholar] [CrossRef]
- Karamitsos, T.D.; Francis, J.M.; Myerson, S.; Selvanayagam, J.B.; Neubauer, S. The role of cardiovascular magnetic resonance imaging in heart failure. J. Am. Coll. Cardiol. 2009, 54, 1407–1424. [Google Scholar] [CrossRef]
- Palmisano, A.; Vignale, D.; Benedetti, G.; Del Maschio, A.; De Cobelli, F.; Esposito, A. Late iodine enhancement cardiac computed tomography for detection of myocardial scars: Impact of experience in the clinical practice. Radiol. Med. 2020, 125, 128–136. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carr-White, G.; Jabbour, A.; Yu, C.Y.; Gebker, R.; Kelle, S.; Hinojar, R.; Doltra, A.; Varma, N.; Child, N.; et al. T1-Mapping and Outcome in Nonischemic Cardiomyopathy: All-Cause Mortality and Heart Failure. JACC Cardiovasc. Imaging 2016, 9, 40–50. [Google Scholar] [CrossRef]
- Palmisano, A.; Darvizeh, F.; Cundari, G.; Rovere, G.; Ferrandino, G.; Nicoletti, V.; Cilia, F.; De Vizio, S.; Palumbo, R.; Esposito, A.; et al. Advanced cardiac imaging in athlete’s heart: Unravelling the grey zone between physiologic adaptation and pathology. Radiol. Med. 2021, 126, 1518–1531. [Google Scholar] [CrossRef]
- Vita, T.; Grani, C.; Abbasi, S.A.; Neilan, T.G.; Rowin, E.; Kaneko, K.; Coelho-Filho, O.; Watanabe, E.; Mongeon, F.P.; Farhad, H.; et al. Comparing CMR Mapping Methods and Myocardial Patterns Toward Heart Failure Outcomes in Nonischemic Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2019, 12, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Liguori, C.; Farina, D.; Vaccher, F.; Ferrandino, G.; Bellini, D.; Carbone, I. Myocarditis: Imaging up to date. Radiol. Med. 2020, 125, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, A.T.; Gil, K.E.; Varghese, J.; Simonetti, O.P.; Zareba, K.M. T2 mapping in myocardial disease: A comprehensive review. J. Cardiovasc. Magn. Reson. 2022, 24, 33. [Google Scholar] [CrossRef] [PubMed]
- Foti, G.; Mantovani, W.; Faccioli, N.; Crivellari, G.; Romano, L.; Zorzi, C.; Carbognin, G. Identification of bone marrow edema of the knee: Diagnostic accuracy of dual-energy CT in comparison with MRI. Radiol. Med. 2021, 126, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Pelgrim, G.J.; Handayani, A.; Dijkstra, H.; Prakken, N.H.; Slart, R.H.; Oudkerk, M.; Van Ooijen, P.M.; Vliegenthart, R.; Sijens, P.E. Quantitative Myocardial Perfusion with Dynamic Contrast-Enhanced Imaging in MRI and CT: Theoretical Models and Current Implementation. Biomed. Res. Int. 2016, 2016, 1734190. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.Y.; Rochitte, C.E.; Arbab-Zadeh, A.; Dewey, M.; George, R.T.; Miller, J.M.; Niinuma, H.; Yoshioka, K.; Kitagawa, K.; Sakuma, H.; et al. Prognostic Value of Combined CT Angiography and Myocardial Perfusion Imaging versus Invasive Coronary Angiography and Nuclear Stress Perfusion Imaging in the Prediction of Major Adverse Cardiovascular Events: The CORE320 Multicenter Study. Radiology 2017, 284, 55–65. [Google Scholar] [CrossRef]
- Tanabe, Y.; Kurata, A.; Matsuda, T.; Yoshida, K.; Baruah, D.; Kido, T.; Mochizuki, T.; Rajiah, P. Computed tomographic evaluation of myocardial ischemia. Jpn. J. Radiol. 2020, 38, 411–433. [Google Scholar] [CrossRef]
- Grandhi, G.R.; Batlle, J.C.; Maroules, C.D.; Janowitz, W.; Pena, C.S.; Ziffer, J.A.; Macedo, R.; Nasir, K.; Cury, R.C. Combined stress myocardial CT perfusion and coronary CT angiography as a feasible strategy among patients presenting with acute chest pain to the emergency department. J. Cardiovasc. Comput. Tomogr. 2021, 15, 129–136. [Google Scholar] [CrossRef]
- Nous, F.M.A.; Geisler, T.; Kruk, M.B.P.; Alkadhi, H.; Kitagawa, K.; Vliegenthart, R.; Hell, M.M.; Hausleiter, J.; Nguyen, P.K.; Budde, R.P.J.; et al. Dynamic Myocardial Perfusion CT for the Detection of Hemodynamically Significant Coronary Artery Disease. JACC Cardiovasc. Imaging 2022, 15, 75–87. [Google Scholar] [CrossRef]
- Albano, D.; Bruno, F.; Agostini, A.; Angileri, S.A.; Benenati, M.; Bicchierai, G.; Cellina, M.; Chianca, V.; Cozzi, D.; Danti, G.; et al. Dynamic contrast-enhanced (DCE) imaging: State of the art and applications in whole-body imaging. Jpn. J. Radiol. 2022, 40, 341–366. [Google Scholar] [CrossRef]
- Ohta, Y.; Kitao, S.; Yunaga, H.; Fujii, S.; Mukai, N.; Yamamoto, K.; Ogawa, T. Myocardial Delayed Enhancement CT for the Evaluation of Heart Failure: Comparison to MRI. Radiology 2018, 288, 682–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, R.X.; Shao, J.; Jiang, J.S.; Ruan, X.W.; Huang, S.; Zhang, Q.; Hu, C.H. Myocardial extracellular volume fraction quantitation using cardiac dual-energy CT with late iodine enhancement in patients with heart failure without coronary artery disease: A single-center prospective study. Eur. J. Radiol. 2021, 140, 109743. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Haass, M.; Zugck, C.; Krueger, C.; Unnebrink, K.; Zimmermann, R.; Kuebler, W.; Kuecherer, H. Prognostic value of Doppler echocardiographic mitral inflow patterns: Implications for risk stratification in patients with chronic congestive heart failure. J. Am. Coll. Cardiol. 2001, 37, 1049–1055. [Google Scholar] [CrossRef]
- Xie, G.Y.; Berk, M.R.; Smith, M.D.; DeMaria, A.N. Relation of Doppler transmitral flow patterns to functional status in congestive heart failure. Am. Heart J. 1996, 131, 766–771. [Google Scholar] [CrossRef]
- Rathi, V.K.; Doyle, M.; Yamrozik, J.; Williams, R.B.; Caruppannan, K.; Truman, C.; Vido, D.; Biederman, R.W. Routine evaluation of left ventricular diastolic function by cardiovascular magnetic resonance: A practical approach. J. Cardiovasc. Magn. Reson. 2008, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Memon, M.M.; Murad, M.H.; Vaduganathan, M.; Greene, S.J.; Hall, M.; Triposkiadis, F.; Lam, C.S.P.; Shah, A.M.; Butler, J.; et al. Left atrial function in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Eur. J. Heart Fail. 2020, 22, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Satchithananda, D.K.; Mamas, M.A. The importance of interactions between atrial fibrillation and heart failure. Clin. Med. 2016, 16, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Cikes, M.; Planinc, I.; Claggett, B.; Cunningham, J.; Milicic, D.; Sweitzer, N.; Senni, M.; Gori, M.; Linssen, G.; Shah, S.J.; et al. Atrial Fibrillation in Heart Failure with Preserved Ejection Fraction: The Paragon-Hf Trial. JACC Heart Fail. 2022, 10, 336–346. [Google Scholar] [CrossRef]
- Khan, M.A.; Yang, E.Y.; Zhan, Y.; Judd, R.M.; Chan, W.; Nabi, F.; Heitner, J.F.; Kim, R.J.; Klem, I.; Nagueh, S.F.; et al. Association of left atrial volume index and all-cause mortality in patients referred for routine cardiovascular magnetic resonance: A multicenter study. J. Cardiovasc. Magn. Reson. 2019, 21, 4. [Google Scholar] [CrossRef]
- Olsen, F.J.; Bertelsen, L.; de Knegt, M.C.; Christensen, T.E.; Vejlstrup, N.; Svendsen, J.H.; Jensen, J.S.; Biering-Sorensen, T. Multimodality Cardiac Imaging for the Assessment of Left Atrial Function and the Association with Atrial Arrhythmias. Circ. Cardiovasc. Imaging 2016, 9, e004947. [Google Scholar] [CrossRef]
- Markman, T.M.; Habibi, M.; Venkatesh, B.A.; Zareian, M.; Wu, C.; Heckbert, S.R.; Bluemke, D.A.; Lima, J.A.C. Association of left atrial structure and function and incident cardiovascular disease in patients with diabetes mellitus: Results from multi-ethnic study of atherosclerosis (MESA). Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Matulevicius, S.A.; Ayers, C.R.; Berry, J.D.; Patel, P.C.; Markham, D.W.; Levine, B.D.; Chin, K.M.; de Lemos, J.A.; Peshock, R.M.; et al. Left atrial structure and function and clinical outcomes in the general population. Eur. Heart J. 2013, 34, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Lessick, J.; Mutlak, D.; Mutlak, M.; Sheik-Muhamad, R.; Naami, R.; Efraim, R.; Abadi, S.; Aronson, D. Left atrial function by cardiac computed tomography is a predictor of heart failure and cardiovascular death. Eur. Radiol. 2022, 32, 132–142. [Google Scholar] [CrossRef]
- Elgendy, I.Y.; Mahtta, D.; Pepine, C.J. Medical Therapy for Heart Failure Caused by Ischemic Heart Disease. Circ. Res. 2019, 124, 1520–1535. [Google Scholar] [CrossRef]
- Corcoran, D.; Young, R.; Adlam, D.; McConnachie, A.; Mangion, K.; Ripley, D.; Cairns, D.; Brown, J.; Bucciarelli-Ducci, C.; Baumbach, A.; et al. Coronary microvascular dysfunction in patients with stable coronary artery disease: The CE-MARC 2 coronary physiology sub-study. Int. J. Cardiol. 2018, 266, 7–14. [Google Scholar] [CrossRef]
- Ford, T.J.; Stanley, B.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc. Interv. 2020, 13, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Danad, I.; Szymonifka, J.; Twisk, J.W.R.; Norgaard, B.L.; Zarins, C.K.; Knaapen, P.; Min, J.K. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: A meta-analysis. Eur. Heart. J. 2017, 38, 991–998. [Google Scholar] [CrossRef]
- Buffa, V.; Di Renzi, P. CMR in the diagnosis of ischemic heart disease. Radiol. Med. 2020, 125, 1114–1123. [Google Scholar] [CrossRef]
- Takx, R.A.; Blomberg, B.A.; El Aidi, H.; Habets, J.; de Jong, P.A.; Nagel, E.; Hoffmann, U.; Leiner, T. Diagnostic accuracy of stress myocardial perfusion imaging compared to invasive coronary angiography with fractional flow reserve meta-analysis. Circ. Cardiovasc. Imaging 2015, 8, e002666. [Google Scholar] [CrossRef] [PubMed]
- Carotti, M.; Salaffi, F.; Sarzi-Puttini, P.; Agostini, A.; Borgheresi, A.; Minorati, D.; Galli, M.; Marotto, D.; Giovagnoni, A. Chest CT features of coronavirus disease 2019 (COVID-19) pneumonia: Key points for radiologists. Radiol. Med. 2020, 125, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, M.; Notaro, M.; Rea, G.; Iacobellis, F.; Delli Paoli, V.; Acampora, C.; Ianniello, S.; Brunese, L.; Romano, L.; Vallone, G. The lung ultrasound: Facts or artifacts? In the era of COVID-19 outbreak. Radiol. Med. 2020, 125, 738–753. [Google Scholar] [CrossRef]
- Frongillo, E.; Gaudioso, G.; Feragalli, B. Ultrasound and interstitial lung disease: Use and limitations. Radiol. Med. 2020, 125, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Giannitto, C.; Sposta, F.M.; Repici, A.; Vatteroni, G.; Casiraghi, E.; Casari, E.; Ferraroli, G.M.; Fugazza, A.; Sandri, M.T.; Chiti, A.; et al. Chest CT in patients with a moderate or high pretest probability of COVID-19 and negative swab. Radiol. Med. 2020, 125, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Cappabianca, S.; Fusco, R.; de Lisio, A.; Paura, C.; Clemente, A.; Gagliardi, G.; Lombardi, G.; Giacobbe, G.; Russo, G.M.; Belfiore, M.P.; et al. Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis. Radiol. Med. 2021, 126, 643. [Google Scholar] [CrossRef]
- Falcinelli, L.; Mendichi, M.; Chierchini, S.; Tenti, M.V.; Bellavita, R.; Saldi, S.; Ingrosso, G.; Reggioli, V.; Bini, V.; Aristei, C. Pulmonary function in stereotactic body radiotherapy with helical tomotherapy for primary and metastatic lung lesions. Radiol. Med. 2021, 126, 163–169. [Google Scholar] [CrossRef]
- Masselli, G.; Almberger, M.; Tortora, A.; Capoccia, L.; Dolciami, M.; D’Aprile, M.R.; Valentini, C.; Avventurieri, G.; Bracci, S.; Ricci, P. Role of CT angiography in detecting acute pulmonary embolism associated with COVID-19 pneumonia. Radiol. Med. 2021, 126, 1553–1560. [Google Scholar] [CrossRef]
- Mirabile, A.; Lucarelli, N.M.; Sollazzo, E.P.; Stabile Ianora, A.A.; Sardaro, A.; Mirabile, G.; Lorusso, F.; Racanelli, V.; Maggialetti, N.; Scardapane, A. CT pulmonary angiography appropriateness in a single emergency department: Does the use of revised Geneva score matter? Radiol. Med. 2021, 126, 1544–1552. [Google Scholar] [CrossRef]
- Batouty, N.M.; Sobh, D.M.; Gadelhak, B.; Sobh, H.M.; Mahmoud, W.; Tawfik, A.M. Left superior vena cava: Cross-sectional imaging overview. Radiol. Med. 2020, 125, 237–246. [Google Scholar] [CrossRef]
- Danti, G.; Berti, V.; Abenavoli, E.; Briganti, V.; Linguanti, F.; Mungai, F.; Pradella, S.; Miele, V. Diagnostic imaging of typical lung carcinoids: Relationship between MDCT, (111)In-Octreoscan and (18)F-FDG-PET imaging features with Ki-67 index. Radiol. Med. 2020, 125, 715–729. [Google Scholar] [CrossRef]
- Refai, M.; Andolfi, M.; Barbisan, F.; Roncon, A.; Guiducci, G.M.; Xiume, F.; Salati, M.; Tiberi, M.; Giovagnoni, A.; Paci, E. Computed tomography-guided microcoil placement for localizing small pulmonary nodules before uniportal video-assisted thoracoscopic resection. Radiol. Med. 2020, 125, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Huang, Y.; Song, W.; Zheng, F.; Wang, X.; Xu, X.; Wang, Z.; Jiang, J.; Jin, Z. Clinical features of pulmonary cryptococcosis in thin-section CT in immunocompetent and non-AIDS immunocompromised patients. Radiol. Med. 2020, 125, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Yang, Z.; Gong, L.; Jiang, S.; Wang, L.; Zhang, H. Classification of lung nodules based on CT images using squeeze-and-excitation network and aggregated residual transformations. Radiol. Med. 2020, 125, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Ustabasioglu, F.E.; Solak, S.; Kula, O.; Gunay, B.; Serez, B.; Tuncbilek, N. The relationship between computed tomographic obstruction index and pulmonary vein cross-sectional area in acute pulmonary embolism. Radiol. Med. 2020, 125, 265–271. [Google Scholar] [CrossRef]
- Gaia, C.; Maria Chiara, C.; Silvia, L.; Chiara, A.; Maria Luisa, D.C.; Giulia, B.; Silvia, P.; Lucia, C.; Alessandra, T.; Annarita, S.; et al. Chest CT for early detection and management of coronavirus disease (COVID-19): A report of 314 patients admitted to Emergency Department with suspected pneumonia. Radiol. Med. 2020, 125, 931–942. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Polovina, M.; Bauersachs, J.; Arad, M.; Gal, T.B.; Lund, L.H.; Felix, S.B.; Arbustini, E.; Caforio, A.L.P.; Farmakis, D.; et al. Heart failure in cardiomyopathies: A position paper from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 553–576. [Google Scholar] [CrossRef]
- Palumbo, P.; Cannizzaro, E.; Di Cesare, A.; Bruno, F.; Schicchi, N.; Giovagnoni, A.; Splendiani, A.; Barile, A.; Masciocchi, C.; Di Cesare, E. Cardiac magnetic resonance in arrhythmogenic cardiomyopathies. Radiol. Med. 2020, 125, 1087–1101. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Gallone, G.; Palmisano, A.; Marchitelli, L.; Catapano, F.; Francone, M. The current landscape of imaging recommendations in cardiovascular clinical guidelines: Toward an imaging-guided precision medicine. Radiol. Med. 2020, 125, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Rovere, G.; Meduri, A.; Savino, G.; Flammia, F.C.; Lo Piccolo, F.; Carafa, M.R.P.; Larici, A.R.; Natale, L.; Merlino, B.; Marano, R. Practical instructions for using drugs in CT and MR cardiac imaging. Radiol. Med. 2021, 126, 356–364. [Google Scholar] [CrossRef]
- Cleland, J.G.; McGowan, J. Heart failure due to ischaemic heart disease: Epidemiology, pathophysiology and progression. J. Cardiovasc. Pharmacol. 1999, 33 (Suppl. 3), S17–S29. [Google Scholar] [CrossRef] [PubMed]
- Bowling, C.B.; Sanders, P.W.; Allman, R.M.; Rogers, W.J.; Patel, K.; Aban, I.B.; Rich, M.W.; Pitt, B.; White, M.; Bakris, G.C.; et al. Effects of enalapril in systolic heart failure patients with and without chronic kidney disease: Insights from the SOLVD Treatment trial. Int. J. Cardiol. 2013, 167, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Shaw, L.J.; Min, J.K.; Page, C.B.; Berman, D.S.; Chaitman, B.R.; Picard, M.H.; Kwong, R.Y.; O’Brien, S.M.; Huang, Z.; et al. Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity. Circulation 2021, 144, 1024–1038. [Google Scholar] [CrossRef] [PubMed]
- Newby, D.E.; Williams, M.C.; Dweck, M.R. Forget Ischemia: It’s All About the Plaque. Circulation 2021, 144, 1039–1041. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, E.J.; Lee, K.L.; Jones, R.H.; Al-Khalidi, H.R.; Hill, J.A.; Panza, J.A.; Michler, R.E.; Bonow, R.O.; Doenst, T.; Petrie, M.C.; et al. Coronary-Artery Bypass Surgery in Patients with Ischemic Cardiomyopathy. N. Engl. J. Med. 2016, 374, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- Pezel, T.; Silva, L.M.; Bau, A.A.; Teixiera, A.; Jerosch-Herold, M.; Coelho-Filho, O.R. What Is the Clinical Impact of Stress CMR After the ISCHEMIA Trial? Front. Cardiovasc. Med. 2021, 8, 683434. [Google Scholar] [CrossRef]
- Mukherjee, D. Myocardial Infarction with Nonobstructive Coronary Arteries: A Call for Individualized Treatment. J. Am. Heart Assoc. 2019, 8, e013361. [Google Scholar] [CrossRef]
- Niccoli, G.; Scalone, G.; Crea, F. Acute myocardial infarction with no obstructive coronary atherosclerosis: Mechanisms and management. Eur. Heart J. 2015, 36, 475–481. [Google Scholar] [CrossRef]
- Occhipinti, G.; Bucciarelli-Ducci, C.; Capodanno, D. Diagnostic pathways in myocardial infarction with non-obstructive coronary artery disease (MINOCA). Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 813–822. [Google Scholar] [CrossRef]
- Scalone, G.; Niccoli, G.; Crea, F. Editor’s Choice- Pathophysiology, diagnosis and management of MINOCA: An update. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 54–62. [Google Scholar] [CrossRef]
- Dastidar, A.G.; Rodrigues, J.C.L.; Johnson, T.W.; De Garate, E.; Singhal, P.; Baritussio, A.; Scatteia, A.; Strange, J.; Nightingale, A.K.; Angelini, G.D.; et al. Myocardial Infarction with Nonobstructed Coronary Arteries: Impact of CMR Early after Presentation. JACC Cardiovasc. Imaging 2017, 10, 1204–1206. [Google Scholar] [CrossRef] [PubMed]
- SOLVD Investigators; Yusuf, S.; Pitt, B.; Davis, C.E.; Hood, W.B.; Cohn, J.N. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N. Engl. J. Med. 1991, 325, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Braunwald, E.; Moye, L.A.; Basta, L.; Brown, E.J., Jr.; Cuddy, T.E.; Davis, B.R.; Geltman, E.M.; Goldman, S.; Flaker, G.C.; et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N. Engl. J. Med. 1992, 327, 669–677. [Google Scholar] [CrossRef]
- Anzai, T. Post-infarction inflammation and left ventricular remodeling: A double-edged sword. Circ. J. 2013, 77, 580–587. [Google Scholar] [CrossRef]
- Suleiman, M.; Khatib, R.; Agmon, Y.; Mahamid, R.; Boulos, M.; Kapeliovich, M.; Levy, Y.; Beyar, R.; Markiewicz, W.; Hammerman, H.; et al. Early inflammation and risk of long-term development of heart failure and mortality in survivors of acute myocardial infarction predictive role of C-reactive protein. J. Am. Coll. Cardiol. 2006, 47, 962–968. [Google Scholar] [CrossRef]
- Brown, E.J., Jr.; Kloner, R.A.; Schoen, F.J.; Hammerman, H.; Hale, S.; Braunwald, E. Scar thinning due to ibuprofen administration after experimental myocardial infarction. Am. J. Cardiol. 1983, 51, 877–883. [Google Scholar] [CrossRef]
- Silverman, H.S.; Pfeifer, M.P. Relation between use of anti-inflammatory agents and left ventricular free wall rupture during acute myocardial infarction. Am. J. Cardiol. 1987, 59, 363–364. [Google Scholar] [CrossRef]
- Hammerman, H.; Kloner, R.A.; Schoen, F.J.; Brown, E.J., Jr.; Hale, S.; Braunwald, E. Indomethacin-induced scar thinning after experimental myocardial infarction. Circulation 1983, 67, 1290–1295. [Google Scholar] [CrossRef] [PubMed]
- Hafezi-Moghadam, A.; Simoncini, T.; Yang, Z.; Limbourg, F.P.; Plumier, J.C.; Rebsamen, M.C.; Hsieh, C.M.; Chui, D.S.; Thomas, K.L.; Prorock, A.J.; et al. Acute cardiovascular protective effects of corticosteroids are mediated by non-transcriptional activation of endothelial nitric oxide synthase. Nat. Med. 2002, 8, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Abbate, A.; Kontos, M.C.; Grizzard, J.D.; Biondi-Zoccai, G.G.; Van Tassell, B.W.; Robati, R.; Roach, L.M.; Arena, R.A.; Roberts, C.S.; Varma, A.; et al. Interleukin-1 blockade with anakinra to prevent adverse cardiac remodeling after acute myocardial infarction (Virginia Commonwealth University Anakinra Remodeling Trial [VCU-ART] Pilot study). Am. J. Cardiol. 2010, 105, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: An update. Eur. Heart J. 2014, 35, 1101–1111. [Google Scholar] [CrossRef] [Green Version]
- Masi, S.; Rizzoni, D.; Taddei, S.; Widmer, R.J.; Montezano, A.C.; Luscher, T.F.; Schiffrin, E.L.; Touyz, R.M.; Paneni, F.; Lerman, A.; et al. Assessment and pathophysiology of microvascular disease: Recent progress and clinical implications. Eur. Heart J. 2021, 42, 2590–2604. [Google Scholar] [CrossRef] [PubMed]
- Padro, T.; Manfrini, O.; Bugiardini, R.; Canty, J.; Cenko, E.; De Luca, G.; Duncker, D.J.; Eringa, E.C.; Koller, A.; Tousoulis, D.; et al. ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on ‘coronary microvascular dysfunction in cardiovascular disease’. Cardiovasc. Res. 2020, 116, 741–755. [Google Scholar] [CrossRef] [PubMed]
- Sechtem, U.; Brown, D.; Godo, S.; Lanza, G.A.; Shimokawa, H.; Sidik, N. Coronary microvascular dysfunction in stable ischaemic heart disease (non-obstructive coronary artery disease and obstructive coronary artery disease). Cardiovasc. Res. 2020, 116, 771–786. [Google Scholar] [CrossRef] [PubMed]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.T.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankstein, R.; et al. Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction. Eur. Heart J. 2018, 39, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Centonze, M.; Steidler, S.; Casagranda, G.; Alfonsi, U.; Spagnolli, F.; Rozzanigo, U.; Palumbo, D.; Faletti, R.; De Cobelli, F. Cardiac-CT and cardiac-MR cost-effectiveness: A literature review. Radiol. Med. 2020, 125, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, R.; Osawa, K.; Kurata, A.; Miyoshi, T. Role of coronary computed tomography angiography (CTA) post the ISCHEMIA trial: Precision prevention based on coronary CTA-derived coronary atherosclerosis. J. Cardiol. 2021, 27, R713–R715. [Google Scholar] [CrossRef]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Bartorelli, A.L.; Bertella, E.; Antonioli, L.; Formenti, A.; Cortinovis, S.; Veglia, F.; Annoni, A.; et al. A long-term prognostic value of coronary CT angiography in suspected coronary artery disease. JACC Cardiovasc. Imaging 2012, 5, 690–701. [Google Scholar] [CrossRef]
- Pontone, G.; Andreini, D.; Bartorelli, A.L.; Bertella, E.; Cortinovis, S.; Mushtaq, S.; Foti, C.; Annoni, A.; Formenti, A.; Baggiano, A.; et al. A long-term prognostic value of CT angiography and exercise ECG in patients with suspected CAD. JACC Cardiovasc. Imaging 2013, 6, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Hadamitzky, M.; Freissmuth, B.; Meyer, T.; Hein, F.; Kastrati, A.; Martinoff, S.; Schomig, A.; Hausleiter, J. Prognostic value of coronary computed tomographic angiography for prediction of cardiac events in patients with suspected coronary artery disease. JACC Cardiovasc. Imaging 2009, 2, 404–411. [Google Scholar] [CrossRef]
- Hadamitzky, M.; Distler, R.; Meyer, T.; Hein, F.; Kastrati, A.; Martinoff, S.; Schomig, A.; Hausleiter, J. Prognostic value of coronary computed tomographic angiography in comparison with calcium scoring and clinical risk scores. Circ. Cardiovasc. Imaging 2011, 4, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, P.S.; Hoffmann, U.; Patel, M.R.; Mark, D.B.; Al-Khalidi, H.R.; Cavanaugh, B.; Cole, J.; Dolor, R.J.; Fordyce, C.B.; Huang, M.; et al. Outcomes of anatomical versus functional testing for coronary artery disease. N. Engl. J. Med. 2015, 372, 1291–1300. [Google Scholar] [CrossRef]
- Hoffmann, U.; Ferencik, M.; Udelson, J.E.; Picard, M.H.; Truong, Q.A.; Patel, M.R.; Huang, M.; Pencina, M.; Mark, D.B.; Heitner, J.F.; et al. Prognostic Value of Noninvasive Cardiovascular Testing in Patients with Stable Chest Pain: Insights From the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation 2017, 135, 2320–2332. [Google Scholar] [CrossRef]
- Investigators, S.-H.; Newby, D.E.; Adamson, P.D.; Berry, C.; Boon, N.A.; Dweck, M.R.; Flather, M.; Forbes, J.; Hunter, A.; Lewis, S.; et al. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N. Engl. J. Med. 2018, 379, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, P.; Cannizzaro, E.; Di Cesare, A.; Bruno, F.; Arrigoni, F.; Splendiani, A.; Barile, A.; Masciocchi, C.; Di Cesare, E. Stress Perfusion Cardiac Magnetic Resonance in Long-Standing Non-Infarcted Chronic Coronary Syndrome with Preserved Systolic Function. Diagnostics 2022, 12, 786. [Google Scholar] [CrossRef]
- Kim, R.J.; Wu, E.; Rafael, A.; Chen, E.L.; Parker, M.A.; Simonetti, O.; Klocke, F.J.; Bonow, R.O.; Judd, R.M. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N. Engl. J. Med. 2000, 343, 1445–1453. [Google Scholar] [CrossRef]
- Kwong, R.Y.; Ge, Y.; Steel, K.; Bingham, S.; Abdullah, S.; Fujikura, K.; Wang, W.; Pandya, A.; Chen, Y.Y.; Mikolich, J.R.; et al. Cardiac Magnetic Resonance Stress Perfusion Imaging for Evaluation of Patients with Chest Pain. J. Am. Coll. Cardiol. 2019, 74, 1741–1755. [Google Scholar] [CrossRef]
- Ge, Y.; Antiochos, P.; Steel, K.; Bingham, S.; Abdullah, S.; Chen, Y.Y.; Mikolich, J.R.; Arai, A.E.; Bandettini, W.P.; Shanbhag, S.M.; et al. Prognostic Value of Stress CMR Perfusion Imaging in Patients with Reduced Left Ventricular Function. JACC Cardiovasc. Imaging 2020, 13, 2132–2145. [Google Scholar] [CrossRef]
- Schwitter, J. The SPINS Trial: Building Evidence and a Consequence? J. Am. Coll. Cardiol. 2019, 74, 1756–1759. [Google Scholar] [CrossRef]
- Patel, A.R.; Salerno, M.; Kwong, R.Y.; Singh, A.; Heydari, B.; Kramer, C.M. Stress Cardiac Magnetic Resonance Myocardial Perfusion Imaging: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 78, 1655–1668. [Google Scholar] [CrossRef]
- Ge, Y.; Steel, K.; Antiochos, P.; Bingham, S.; Abdullah, S.; Mikolich, J.R.; Arai, A.E.; Bandettini, W.P.; Shanbhag, S.M.; Patel, A.R.; et al. Stress CMR in patients with obesity: Insights from the Stress CMR Perfusion Imaging in the United States (SPINS) registry. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 518–527. [Google Scholar] [CrossRef]
- Pezel, T.; Garot, P.; Hovasse, T.; Unterseeh, T.; Champagne, S.; Kinnel, M.; Toupin, S.; Louvard, Y.; Morice, M.C.; Sanguineti, F.; et al. Vasodilatation stress cardiovascular magnetic resonance imaging: Feasibility, workflow and safety in a large prospective registry of more than 35,000 patients. Arch. Cardiovasc. Dis. 2021, 114, 490–503. [Google Scholar] [CrossRef]
- Marcos-Garces, V.; Gavara, J.; Monmeneu, J.V.; Lopez-Lereu, M.P.; Bosch, M.J.; Merlos, P.; Perez, N.; Rios-Navarro, C.; De Dios, E.; Bonanad, C.; et al. Vasodilator Stress CMR and All-Cause Mortality in Stable Ischemic Heart Disease: A Large Retrospective Registry. JACC Cardiovasc. Imaging 2020, 13, 1674–1686. [Google Scholar] [CrossRef]
- Nagel, E.; Greenwood, J.P.; McCann, G.P.; Bettencourt, N.; Shah, A.M.; Hussain, S.T.; Perera, D.; Plein, S.; Bucciarelli-Ducci, C.; Paul, M.; et al. Magnetic Resonance Perfusion or Fractional Flow Reserve in Coronary Disease. N. Engl. J. Med. 2019, 380, 2418–2428. [Google Scholar] [CrossRef]
- Ibanez, B.; Aletras, A.H.; Arai, A.E.; Arheden, H.; Bax, J.; Berry, C.; Bucciarelli-Ducci, C.; Croisille, P.; Dall’Armellina, E.; Dharmakumar, R.; et al. Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 74, 238–256. [Google Scholar] [CrossRef]
- Shore, S.; Grau-Sepulveda, M.V.; Bhatt, D.L.; Heidenreich, P.A.; Eapen, Z.J.; Hernandez, A.F.; Yancy, C.W.; Fonarow, G.C. Characteristics, Treatments, and Outcomes of Hospitalized Heart Failure Patients Stratified by Etiologies of Cardiomyopathy. JACC Heart Fail. 2015, 3, 906–916. [Google Scholar] [CrossRef]
- Augusto, J.B.; Eiros, R.; Nakou, E.; Moura-Ferreira, S.; Treibel, T.A.; Captur, G.; Akhtar, M.M.; Protonotarios, A.; Gossios, T.D.; Savvatis, K.; et al. Dilated cardiomyopathy and arrhythmogenic left ventricular cardiomyopathy: A comprehensive genotype-imaging phenotype study. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 326–336. [Google Scholar] [CrossRef]
- Chen, W.; Qian, W.; Zhang, X.; Li, D.; Qian, Z.; Xu, H.; Liao, S.; Chen, X.; Wang, Y.; Hou, X.; et al. Ring-like late gadolinium enhancement for predicting ventricular tachyarrhythmias in non-ischaemic dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1130–1138. [Google Scholar] [CrossRef]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef]
- Fuster, V.; Gersh, B.J.; Giuliani, E.R.; Tajik, A.J.; Brandenburg, R.O.; Frye, R.L. The natural history of idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1981, 47, 525–531. [Google Scholar] [CrossRef]
- Halliday, B.P.; Wassall, R.; Lota, A.S.; Khalique, Z.; Gregson, J.; Newsome, S.; Jackson, R.; Rahneva, T.; Wage, R.; Smith, G.; et al. Withdrawal of pharmacological treatment for heart failure in patients with recovered dilated cardiomyopathy (TRED-HF): An open-label, pilot, randomised trial. Lancet 2019, 393, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, Y.; Takata, J.; Kitaoka, H.; Kubo, T.; Baba, Y.; Hoshikawa, E.; Hamada, T.; Okawa, M.; Hitomi, N.; Sato, K.; et al. Long-term prognosis of dilated cardiomyopathy revisited: An improvement in survival over the past 20 years. Circ. J. 2006, 70, 376–383. [Google Scholar] [CrossRef]
- Merlo, M.; Pyxaras, S.A.; Pinamonti, B.; Barbati, G.; Di Lenarda, A.; Sinagra, G. Prevalence and prognostic significance of left ventricular reverse remodeling in dilated cardiomyopathy receiving tailored medical treatment. J. Am. Coll. Cardiol. 2011, 57, 1468–1476. [Google Scholar] [CrossRef]
- Wilcox, J.E.; Fonarow, G.C.; Yancy, C.W.; Albert, N.M.; Curtis, A.B.; Heywood, J.T.; Inge, P.J.; McBride, M.L.; Mehra, M.R.; O’Connor, C.M.; et al. Factors associated with improvement in ejection fraction in clinical practice among patients with heart failure: Findings from IMPROVE HF. Am. Heart J. 2012, 163, 49–56 e42. [Google Scholar] [CrossRef]
- Corrado, D.; van Tintelen, P.J.; McKenna, W.J.; Hauer, R.N.W.; Anastastakis, A.; Asimaki, A.; Basso, C.; Bauce, B.; Brunckhorst, C.; Bucciarelli-Ducci, C.; et al. Arrhythmogenic right ventricular cardiomyopathy: Evaluation of the current diagnostic criteria and differential diagnosis. Eur. Heart J. 2020, 41, 1414–1429. [Google Scholar] [CrossRef]
- Holmstrom, M.; Kivisto, S.; Helio, T.; Jurkko, R.; Kaartinen, M.; Antila, M.; Reissell, E.; Kuusisto, J.; Karkkainen, S.; Peuhkurinen, K.; et al. Late gadolinium enhanced cardiovascular magnetic resonance of lamin A/C gene mutation related dilated cardiomyopathy. J. Cardiovasc. Magn. Reson. 2011, 13, 30. [Google Scholar] [CrossRef]
- Hong, Y.J.; Park, H.S.; Park, J.K.; Han, K.; Park, C.H.; Kim, T.K.; Yoo, S.J.; Lee, J.Y.; Kim, P.K.; Hur, J.; et al. Early Detection and Serial Monitoring of Anthracycline-Induced Cardiotoxicity Using T1-mapping Cardiac Magnetic Resonance Imaging: An Animal Study. Sci. Rep. 2017, 7, 2663. [Google Scholar] [CrossRef]
- Jordan, J.H.; Sukpraphrute, B.; Melendez, G.C.; Jolly, M.P.; D’Agostino, R.B., Jr.; Hundley, W.G. Early Myocardial Strain Changes During Potentially Cardiotoxic Chemotherapy May Occur as a Result of Reductions in Left Ventricular End-Diastolic Volume: The Need to Interpret Left Ventricular Strain with Volumes. Circulation 2017, 135, 2575–2577. [Google Scholar] [CrossRef]
- Kongbundansuk, S.; Hundley, W.G. Noninvasive imaging of cardiovascular injury related to the treatment of cancer. JACC Cardiovasc. Imaging 2014, 7, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Pradella, S.; Grazzini, G.; De Amicis, C.; Letteriello, M.; Acquafresca, M.; Miele, V. Cardiac magnetic resonance in hypertrophic and dilated cardiomyopathies. Radiol. Med. 2020, 125, 1056–1071. [Google Scholar] [CrossRef]
- Maron, B.J.; Rowin, E.J.; Casey, S.A.; Link, M.S.; Lesser, J.R.; Chan, R.H.; Garberich, R.F.; Udelson, J.E.; Maron, M.S. Hypertrophic Cardiomyopathy in Adulthood Associated with Low Cardiovascular Mortality with Contemporary Management Strategies. J. Am. Coll. Cardiol. 2015, 65, 1915–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treibel, T.A.; Kozor, R.; Menacho, K.; Castelletti, S.; Bulluck, H.; Rosmini, S.; Nordin, S.; Maestrini, V.; Fontana, M.; Moon, J.C. Left Ventricular Hypertrophy Revisited: Cell and Matrix Expansion Have Disease-Specific Relationships. Circulation 2017, 136, 2519–2521. [Google Scholar] [CrossRef] [PubMed]
- Melacini, P.; Basso, C.; Angelini, A.; Calore, C.; Bobbo, F.; Tokajuk, B.; Bellini, N.; Smaniotto, G.; Zucchetto, M.; Iliceto, S.; et al. Clinicopathological profiles of progressive heart failure in hypertrophic cardiomyopathy. Eur. Heart J. 2010, 31, 2111–2123. [Google Scholar] [CrossRef] [PubMed]
- Maron, M.S.; Rowin, E.J.; Olivotto, I.; Casey, S.A.; Arretini, A.; Tomberli, B.; Garberich, R.F.; Link, M.S.; Chan, R.H.M.; Lesser, J.R.; et al. Contemporary Natural History and Management of Nonobstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 1399–1409. [Google Scholar] [CrossRef] [PubMed]
- Maron, M.S.; Olivotto, I.; Betocchi, S.; Casey, S.A.; Lesser, J.R.; Losi, M.A.; Cecchi, F.; Maron, B.J. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N. Engl. J. Med. 2003, 348, 295–303. [Google Scholar] [CrossRef]
- Efthimiadis, G.K.; Pagourelias, E.D.; Parcharidou, D.; Gossios, T.; Kamperidis, V.; Theofilogiannakos, E.K.; Pappa, Z.; Meditskou, S.; Hadjimiltiades, S.; Pliakos, C.; et al. Clinical characteristics and natural history of hypertrophic cardiomyopathy with midventricular obstruction. Circ. J. 2013, 77, 2366–2374. [Google Scholar] [CrossRef]
- Rowin, E.J.; Maron, B.J.; Kiernan, M.S.; Casey, S.A.; Feldman, D.S.; Hryniewicz, K.M.; Chan, R.H.; Harris, K.M.; Udelson, J.E.; DeNofrio, D.; et al. Advanced heart failure with preserved systolic function in nonobstructive hypertrophic cardiomyopathy: Under-recognized subset of candidates for heart transplant. Circ. Heart Fail. 2014, 7, 967–975. [Google Scholar] [CrossRef]
- Olivotto, I.; Maron, B.J.; Appelbaum, E.; Harrigan, C.J.; Salton, C.; Gibson, C.M.; Udelson, J.E.; O’Donnell, C.; Lesser, J.R.; Manning, W.J.; et al. Spectrum and clinical significance of systolic function and myocardial fibrosis assessed by cardiovascular magnetic resonance in hypertrophic cardiomyopathy. Am. J. Cardiol. 2010, 106, 261–267. [Google Scholar] [CrossRef]
- O’Hanlon, R.; Grasso, A.; Roughton, M.; Moon, J.C.; Clark, S.; Wage, R.; Webb, J.; Kulkarni, M.; Dawson, D.; Sulaibeekh, L.; et al. Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2010, 56, 867–874. [Google Scholar] [CrossRef]
- Harris, K.M.; Spirito, P.; Maron, M.S.; Zenovich, A.G.; Formisano, F.; Lesser, J.R.; Mackey-Bojack, S.; Manning, W.J.; Udelson, J.E.; Maron, B.J. Prevalence, clinical profile, and significance of left ventricular remodeling in the end-stage phase of hypertrophic cardiomyopathy. Circulation 2006, 114, 216–225. [Google Scholar] [CrossRef]
- Limongelli, G.; Masarone, D.; Frisso, G.; Iacomino, M.; Ferrara, I.; Rea, A.; Gravino, R.; Bossone, E.; Salvatore, F.; Calabro, R.; et al. Clinical and genetic characterization of patients with hypertrophic cardiomyopathy and right atrial enlargement. J. Cardiovasc. Med. 2017, 18, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seydelmann, N.; Liu, D.; Kramer, J.; Drechsler, C.; Hu, K.; Nordbeck, P.; Schneider, A.; Stork, S.; Bijnens, B.; Ertl, G.; et al. High-Sensitivity Troponin: A Clinical Blood Biomarker for Staging Cardiomyopathy in Fabry Disease. J. Am. Heart. Assoc. 2016, 5, e002839. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; O’Mahony, C.; Hughes, D.; Rahman, M.S.; Coats, C.; Murphy, E.; Lachmann, R.; Mehta, A.; Elliott, P.M. Clinical and genetic predictors of major cardiac events in patients with Anderson-Fabry Disease. Heart 2015, 101, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Linhart, A.; Kampmann, C.; Zamorano, J.L.; Sunder-Plassmann, G.; Beck, M.; Mehta, A.; Elliott, P.M.; European, F.O.S.I. Cardiac manifestations of Anderson-Fabry disease: Results from the international Fabry outcome survey. Eur. Heart J. 2007, 28, 1228–1235. [Google Scholar] [CrossRef]
- Charron, P.; Villard, E.; Sebillon, P.; Laforet, P.; Maisonobe, T.; Duboscq-Bidot, L.; Romero, N.; Drouin-Garraud, V.; Frebourg, T.; Richard, P.; et al. Danon’s disease as a cause of hypertrophic cardiomyopathy: A systematic survey. Heart 2004, 90, 842–846. [Google Scholar] [CrossRef]
- Maron, M.S.; Maron, B.J. Clinical Impact of Contemporary Cardiovascular Magnetic Resonance Imaging in Hypertrophic Cardiomyopathy. Circulation 2015, 132, 292–298. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging. J. Nucl. Cardiol. 2019, 26, 2065–2123. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 2 of 2-Diagnostic criteria and appropriate utilization. J. Nucl. Cardiol. 2020, 27, 659–673. [Google Scholar] [CrossRef]
- Thompson, R.B.; Chow, K.; Khan, A.; Chan, A.; Shanks, M.; Paterson, I.; Oudit, G.Y. T(1) mapping with cardiovascular MRI is highly sensitive for Fabry disease independent of hypertrophy and sex. Circ. Cardiovasc. Imaging 2013, 6, 637–645. [Google Scholar] [CrossRef]
- Pan, J.A.; Kerwin, M.J.; Salerno, M. Native T1 Mapping, Extracellular Volume Mapping, and Late Gadolinium Enhancement in Cardiac Amyloidosis: A Meta-Analysis. JACC Cardiovasc. Imaging 2020, 13, 1299–1310. [Google Scholar] [CrossRef]
- Vidula, M.K.; Bravo, P.E. Multimodality imaging for the diagnosis of infiltrative cardiomyopathies. Heart 2022, 108, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Todiere, G.; Pisciella, L.; Barison, A.; Del Franco, A.; Zachara, E.; Piaggi, P.; Re, F.; Pingitore, A.; Emdin, M.; Lombardi, M.; et al. Abnormal T2-STIR magnetic resonance in hypertrophic cardiomyopathy: A marker of advanced disease and electrical myocardial instability. PLoS ONE 2014, 9, e111366. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kuhl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Galea, N.; Polizzi, G.; Gatti, M.; Cundari, G.; Figuera, M.; Faletti, R. Cardiovascular magnetic resonance (CMR) in restrictive cardiomyopathies. Radiol. Med. 2020, 125, 1072–1086. [Google Scholar] [CrossRef] [PubMed]
- Kushwaha, S.S.; Fallon, J.T.; Fuster, V. Restrictive cardiomyopathy. N. Engl. J. Med. 1997, 336, 267–276. [Google Scholar] [CrossRef]
- Geske, J.B.; Anavekar, N.S.; Nishimura, R.A.; Oh, J.K.; Gersh, B.J. Differentiation of Constriction and Restriction: Complex Cardiovascular Hemodynamics. J. Am. Coll. Cardiol. 2016, 68, 2329–2347. [Google Scholar] [CrossRef]
- Kubo, T.; Gimeno, J.R.; Bahl, A.; Steffensen, U.; Steffensen, M.; Osman, E.; Thaman, R.; Mogensen, J.; Elliott, P.M.; Doi, Y.; et al. Prevalence, clinical significance, and genetic basis of hypertrophic cardiomyopathy with restrictive phenotype. J. Am. Coll. Cardiol. 2007, 49, 2419–2426. [Google Scholar] [CrossRef]
- Charron, P.; Elliott, P.M.; Gimeno, J.R.; Caforio, A.L.P.; Kaski, J.P.; Tavazzi, L.; Tendera, M.; Maupain, C.; Laroche, C.; Rubis, P.; et al. The Cardiomyopathy Registry of the EURObservational Research Programme of the European Society of Cardiology: Baseline data and contemporary management of adult patients with cardiomyopathies. Eur. Heart J. 2018, 39, 1784–1793. [Google Scholar] [CrossRef]
- Pereira, N.L.; Grogan, M.; Dec, G.W. Spectrum of Restrictive and Infiltrative Cardiomyopathies: Part 1 of a 2-Part Series. J. Am. Coll. Cardiol. 2018, 71, 1130–1148. [Google Scholar] [CrossRef]
- Pereira, N.L.; Grogan, M.; Dec, G.W. Spectrum of Restrictive and Infiltrative Cardiomyopathies: Part 2 of a 2-Part Series. J. Am. Coll. Cardiol. 2018, 71, 1149–1166. [Google Scholar] [CrossRef]
- Murphy, C.J.; Oudit, G.Y. Iron-overload cardiomyopathy: Pathophysiology, diagnosis, and treatment. J. Card. Fail. 2010, 16, 888–900. [Google Scholar] [CrossRef] [PubMed]
- Skinner, M.; Anderson, J.; Simms, R.; Falk, R.; Wang, M.; Libbey, C.; Jones, L.A.; Cohen, A.S. Treatment of 100 patients with primary amyloidosis: A randomized trial of melphalan, prednisone, and colchicine versus colchicine only. Am. J. Med. 1996, 100, 290–298. [Google Scholar] [CrossRef]
- Kyle, R.A.; Gertz, M.A. Primary systemic amyloidosis: Clinical and laboratory features in 474 cases. Semin. Hematol. 1995, 32, 45–59. [Google Scholar] [PubMed]
- Mogensen, J.; Arbustini, E. Restrictive cardiomyopathy. Curr. Opin. Cardiol. 2009, 24, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Zurlo, M.G.; De Stefano, P.; Borgna-Pignatti, C.; Di Palma, A.; Piga, A.; Melevendi, C.; Di Gregorio, F.; Burattini, M.G.; Terzoli, S. Survival and causes of death in thalassaemia major. Lancet 1989, 2, 27–30. [Google Scholar] [CrossRef]
- Yazaki, Y.; Isobe, M.; Hiroe, M.; Morimoto, S.; Hiramitsu, S.; Nakano, T.; Izumi, T.; Sekiguchi, M.; Central Japan Heart Study, G. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am. J. Cardiol. 2001, 88, 1006–1010. [Google Scholar] [CrossRef]
- Kremastinos, D.T.; Tsetsos, G.A.; Tsiapras, D.P.; Karavolias, G.K.; Ladis, V.A.; Kattamis, C.A. Heart failure in beta thalassemia: A 5-year follow-up study. Am. J. Med. 2001, 111, 349–354. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Airaksinen, J.; Vihinen, T.; Miettinen, H.; Ylitalo, K.; Kaikkonen, K.; Tuohinen, S.; Haataja, P.; Kerola, T.; et al. Cardiac sarcoidosis: Epidemiology, characteristics, and outcome over 25 years in a nationwide study. Circulation 2015, 131, 624–632. [Google Scholar] [CrossRef]
- Cheng, H.; Zhao, S.; Jiang, S.; Lu, M.; Yan, C.; Ling, J.; Zhang, Y.; Liu, Q.; Ma, N.; Yin, G.; et al. The relative atrial volume ratio and late gadolinium enhancement provide additive information to differentiate constrictive pericarditis from restrictive cardiomyopathy. J. Cardiovasc. Magn. Reson. 2011, 13, 15. [Google Scholar] [CrossRef]
- Cappannoli, L.; Ciliberti, G.; Restivo, A.; Palumbo, P.; D’Alo, F.; Sanna, T.; Crea, F.; D’Amario, D. ‘Here comes the story of the Hurricane’: A case report of AL cardiac amyloidosis and myocardial bridging. Eur. Heart J. Case. Rep. 2022, 6, ytac225. [Google Scholar] [CrossRef]
- Kotecha, T.; Martinez-Naharro, A.; Treibel, T.A.; Francis, R.; Nordin, S.; Abdel-Gadir, A.; Knight, D.S.; Zumbo, G.; Rosmini, S.; Maestrini, V.; et al. Myocardial Edema and Prognosis in Amyloidosis. J. Am. Coll. Cardiol. 2018, 71, 2919–2931. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 1 of 2-Evidence Base and Standardized Methods of Imaging. J. Card. Fail. 2019, 25, e1–e39. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 2 of 2-Diagnostic Criteria and Appropriate Utilization. J. Card. Fail. 2019, 25, 854–865. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. J. Heart. Fail. 2021, 23, 512–526. [Google Scholar] [CrossRef]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef]
- Wicks, E.C.; Menezes, L.J.; Elliott, P.M. Improving the diagnostic accuracy for detecting cardiac sarcoidosis. Expert. Rev. Cardiovasc. Ther. 2015, 13, 223–236. [Google Scholar] [CrossRef]
- Wicks, E.C.; Menezes, L.J.; Barnes, A.; Mohiddin, S.A.; Sekhri, N.; Porter, J.C.; Booth, H.L.; Garrett, E.; Patel, R.S.; Pavlou, M.; et al. Diagnostic accuracy and prognostic value of simultaneous hybrid 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging in cardiac sarcoidosis. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 757–767. [Google Scholar] [CrossRef]
- Kremastinos, D.T.; Farmakis, D. Iron overload cardiomyopathy in clinical practice. Circulation 2011, 124, 2253–2263. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palumbo, P.; Cannizzaro, E.; Palumbo, M.M.; Di Cesare, A.; Bruno, F.; Acanfora, C.; Arceri, A.; Evangelista, L.; Arrigoni, F.; Grassi, F.; et al. Heart Failure and Cardiomyopathies: CT and MR from Basics to Advanced Imaging. Diagnostics 2022, 12, 2298. https://doi.org/10.3390/diagnostics12102298
Palumbo P, Cannizzaro E, Palumbo MM, Di Cesare A, Bruno F, Acanfora C, Arceri A, Evangelista L, Arrigoni F, Grassi F, et al. Heart Failure and Cardiomyopathies: CT and MR from Basics to Advanced Imaging. Diagnostics. 2022; 12(10):2298. https://doi.org/10.3390/diagnostics12102298
Chicago/Turabian StylePalumbo, Pierpaolo, Ester Cannizzaro, Maria Michela Palumbo, Annamaria Di Cesare, Federico Bruno, Chiara Acanfora, Antonella Arceri, Laura Evangelista, Francesco Arrigoni, Francesca Grassi, and et al. 2022. "Heart Failure and Cardiomyopathies: CT and MR from Basics to Advanced Imaging" Diagnostics 12, no. 10: 2298. https://doi.org/10.3390/diagnostics12102298