
Thyroid Cancer and Psoriasis: A Nested Case–Control Study

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seib, C.D.; Sosa, J.A. Evolving Understanding of the Epidemiology of Thyroid Cancer. Endocrinol. Metab. Clin. 2019, 48, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Won, H.-R.; Koo, B.S. Active Surveillance or Surgery in Papillary Thyroid Microcarcinoma: An Ongoing Controversy. Clin. Exp. Otorhinolaryngol. 2022, 15, 123–124. [Google Scholar] [CrossRef] [PubMed]
- Takano, T. Natural history of thyroid cancer. Endocr. J. 2017, 64, 237–244. [Google Scholar] [CrossRef]
- Myung, S.-K.; Lee, C.W.; Lee, J.; Kim, J.; Kim, H.S. Risk Factors for Thyroid Cancer: A Hospital-Based Case-Control Study in Korean Adults. Cancer Res. Treat. 2017, 49, 70–78. [Google Scholar] [CrossRef]
- Crnčić, T.B.; Tomaš, M.I.; Girotto, N.; Ivanković, S.G. Risk Factors for Thyroid Cancer: What Do We Know So Far? Acta Clin. Croat. 2020, 59, 66–72. [Google Scholar] [CrossRef]
- Guarino, V.; Castellone, M.D.; Avilla, E.; Melillo, R.M. Thyroid cancer and inflammation. Mol. Cell. Endocrinol. 2010, 321, 94–102. [Google Scholar] [CrossRef]
- Li, H.; Qian, J. Association of diabetes mellitus with thyroid cancer risk: A meta-analysis of cohort studies. Medicine 2017, 96, e8230. [Google Scholar] [CrossRef]
- Fussey, J.M.; Beaumont, R.N.; Wood, A.R.; Vaidya, B.; Smith, J.; Tyrrell, J. Does Obesity Cause Thyroid Cancer? A Mendelian Randomization Study. J. Clin. Endocrinol. Metab. 2020, 105, e2398–e2407. [Google Scholar] [CrossRef]
- Lee, J.; Jung, K.J.; Kim, T.-G.; Lee, M.-G.; Oh, J.; Jee, S.H. Risk of malignancy in patients with psoriasis: A 15-year nationwide population-based prospective cohort study in Korea. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2296–2304. [Google Scholar] [CrossRef]
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef]
- Jensen, P.; Skov, L. Psoriasis and Obesity. Dermatology 2016, 232, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Pezzolo, E.; Naldi, L. The relationship between smoking, psoriasis and psoriatic arthritis. Expert Rev. Clin. Immunol. 2019, 15, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Svanström, C.; Lonne-Rahm, S.-B.; Nordlind, K. Psoriasis and alcohol. Psoriasis Targets Ther. 2019, 9, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Loft, N.D.; Vaengebjerg, S.; Skov, L. Cancer risk in patients with psoriasis: Should we be paying more attention? Expert Rev. Clin. Immunol. 2020, 16, 479–492. [Google Scholar] [CrossRef] [PubMed]
- Vaengebjerg, S.; Skov, L.; Egeberg, A.; Loft, N.D. Prevalence, Incidence, and Risk of Cancer in Patients with Psoriasis and Psoriatic Arthritis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 421–429. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, H.; Han, K.D.; Kim, H.-N.; Park, Y.M.; Lee, J.Y.; Park, Y.-G.; Lee, Y.B. Cancer risk in 892 089 patients with psoriasis in Korea: A nationwide population-based cohort study. J. Dermatol. 2019, 46, 95–102. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.-Y.; Park, S.K.; Khang, Y.-H.; Kim, H.C.; Park, J.H.; Kang, H.-J.; Do, C.-H.; Song, J.-S.; Lee, E.-J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Yoo, D.M.; Chang, J.; Lee, H.-J.; Park, B.; Choi, H.G. Hearing Impairment Increases Economic Inequality. Clin. Exp. Otorhinolaryngol. 2021, 14, 278–286. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Li, F.; Thomas, L.E. Addressing Extreme Propensity Scores via the Overlap Weights. Am. J. Epidemiol. 2019, 188, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Thomas, L.E.; Li, F.; Pencina, M.J. Overlap Weighting: A Propensity Score Method That Mimics Attributes of a Randomized Clinical Trial. JAMA 2020, 323, 2417. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Schonbach, M.; Coffman, D.L.; Williams, J.S. Variable Selection for Propensity Score Estimation via Balancing Covariates. Epidemiology 2015, 26, e14–e15. [Google Scholar] [CrossRef] [PubMed]
- Derwahl, M.; Nicula, D. Estrogen and its role in thyroid cancer. Endocr. Relat. Cancer 2014, 21, T273–T283. [Google Scholar] [CrossRef]
- Boffetta, P.; Gridley, G.; Lindelöf, B. Cancer Risk in a Population-Based Cohort of Patients Hospitalized for Psoriasis in Sweden. J. Investig. Dermatol. 2001, 117, 1531–1537. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Krueger, J.G.; Lebwohl, M.G. Systemic immune mechanisms in atopic dermatitis and psoriasis with implications for treatment. Exp. Dermatol. 2018, 27, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Felicetti, F.; Catalano, M.G.; Fortunati, N. Thyroid Autoimmunity and Cancer. Front. Horm. Res. 2017, 48, 97–109. [Google Scholar] [CrossRef]
- Baldini, E.; Odorisio, T.; Sorrenti, S.; Catania, A.; Tartaglia, F.; Carbotta, G.; Pironi, D.; Rendina, R.; D’Armiento, E.; Persechino, S.; et al. Vitiligo and Autoimmune Thyroid Disorders. Front. Endocrinol. 2017, 8, 290. [Google Scholar] [CrossRef]
- Baldini, E.; Odorisio, T.; Tuccilli, C.; Persechino, S.; Sorrenti, S.; Catania, A.; Pironi, D.; Carbotta, G.; Giacomelli, L.; Arcieri, S.; et al. Thyroid diseases and skin autoimmunity. Rev. Endocr. Metab. Disord. 2018, 19, 311–323. [Google Scholar] [CrossRef]
- Kano, Y.; Chiba, M.; Yagita, A.; Shiohara, T. Complete resolution of psoriasis vulgaris after excision of thyroid cancer. Int. J. Dermatol. 2008, 36, 280–282. [Google Scholar] [CrossRef]
- Hung, S.-H.; Chung, S.-D.; Lin, H.-C. Thyroxin Use Is Associated With Increased Risk of Thyroid Cancer in Patients With Hypothyroidism. J. Clin. Pharmacol. 2018, 58, 29–33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | After Overlap Weighting Adjustment | Before Overlap Weighting Adjustment | ||||
|---|---|---|---|---|---|---|
| Thyroid Cancer | Control | Standardized Difference | Thyroid Cancer | Control | Standardized Difference | |
| Age (n, %) | 0.00 | 0.00 | ||||
| 40–44 | 63 (1.79) | 63 (1.79) | 128 (1.88) | 512 (1.88) | ||
| 45–49 | 417 (11.83) | 417 (11.83) | 837 (12.27) | 3348 (12.27) | ||
| 50–54 | 842 (23.86) | 842 (23.86) | 1623 (23.79) | 6492 (23.79) | ||
| 55–59 | 875 (24.80) | 875 (24.80) | 1672 (24.51) | 6688 (24.51) | ||
| 60–64 | 645 (18.26) | 645 (18.26) | 1194 (17.50) | 4776 (17.50) | ||
| 65–69 | 373 (10.57) | 373 (10.57) | 746 (10.94) | 2984 (10.94) | ||
| 70–74 | 218 (6.18) | 218 (6.18) | 433 (6.35) | 1732 (6.35) | ||
| 75–79 | 70 (1.97) | 70 (1.97) | 144 (2.11) | 576 (2.11) | ||
| 80–84 | 25 (0.69) | 25 (0.69) | 43 (0.63) | 172 (0.63 | ||
| 85+ | 2 (0.05) | 2 (0.05) | 2 (0.03) | 8 (0.03) | ||
| Sex (n, %) | 0.00 | 0.00 | ||||
| Male | 726 (20.57) | 726 (20.57) | 1513 (22.18) | 6052 (22.18) | ||
| Female | 2803 (79.43) | 2804 (79.43) | 5309 (77.82) | 21,236 (77.82) | ||
| Income (n, %) | 0.00 | 0.00 | ||||
| 1 (lowest) | 446 (12.63) | 446 (12.63) | 852 (12.49) | 3408 (12.49) | ||
| 2 | 418 (11.85) | 418 (11.85) | 803 (11.77) | 3212 (11.77) | ||
| 3 | 537 (15.22) | 537 (15.22) | 1040 (15.24) | 4160 (15.24) | ||
| 4 | 745 (21.10) | 745 (21.10) | 1433 (21.01) | 5732 (21.01) | ||
| 5 (highest) | 1383 (39.20) | 1383 (39.20) | 2694 (39.49) | 10,776 (39.49) | ||
| Region of residence (n, %) | 0.00 | 0.00 | ||||
| Urban | 1697 (48.07) | 1697 (48.07) | 3221 (47.21) | 12,884 (47.21) | ||
| Rural | 1833 (51.93) | 1833 (51.93) | 3601 (52.79) | 14,404 (52.79) | ||
| Obesity † (n, %) | 0.00 | 0.13 | ||||
| Underweight | 56 (1.58) | 56 (1.58) | 93 (1.36) | 578 (2.12) | ||
| Normal | 1212 (34.35) | 1212 (34.35) | 2210 (32.40) | 10,107 (37.04) | ||
| Overweight | 984 (27.89) | 984 (27.89) | 1936 (28.38) | 7453 (27.31) | ||
| Obese I | 1141 (32.32) | 1141 (32.32) | 2301 (33.73) | 8248 (30.23) | ||
| Obese II | 136 (3.86) | 136 (3.86) | 282 (4.13) | 902 (3.31) | ||
| Smoking status (n, %) | 0.00 | 0.08 | ||||
| Nonsmoker | 3069 (86.95) | 3069 (86.95) | 5904 (86.54) | 23,182 (84.95) | ||
| Past smoker | 252 (7.15) | 252 (7.15) | 520 (7.62) | 1945 (7.13) | ||
| Current smoker | 208 (5.90) | 208 (5.90) | 398 (5.83) | 2161 (7.92) | ||
| Alcohol consumption (n, %) | 0.00 | 0.04 | ||||
| <1 time a week | 2660 (75.37) | 2660 (75.37) | 5158 (75.61) | 20,176 (73.94) | ||
| ≥1 time a week | 869 (24.63) | 869 (24.63) | 1664 (24.39) | 7112 (26.06) | ||
| SBP (Mean, SD) | 124.14 (11.29) | 124.14 (5.74) | 0.00 | 124.59 (15.74) | 123.89 (16.17) | 0.04 |
| DBP (Mean, SD) | 77.04 (7.38) | 77.04 (3.76) | 0.00 | 77.41 (10.32) | 76.77 (10.48) | 0.06 |
| FBG (Mean, SD) | 98.14 (16.35) | 98.14 (8.51) | 0.00 | 98.00 (23.09) | 98.67 (26.09) | 0.03 |
| Total cholesterol (Mean, SD) | 199.61 (27.40) | 199.61 (13.55) | 0.00 | 198.76 (38.05) | 201.47 (37.94) | 0.07 |
| CCI score (Mean, SD) | 0.46 (0.61) | 0.46 (0.34) | 0.00 | 0.48 (0.87) | 0.42 (0.89) | 0.44 |
| Hypothyroidism (n, %) | 1233 (34.93) | 1233 (34.93) | 0.00 | 3813 (55.89) | 2289 (8.39) | 1.18 |
| Goiter (n, %) | 1375 (38.97) | 1375 (38.97) | 0.00 | 3832 (56.17) | 3062 (11.22) | 1.08 |
| Thyrotoxicosis (n, %) | 315 (8.92) | 315 (8.92) | 0.00 | 697 (10.22) | 1294 (4.74) | 0.21 |
| Thyroiditis (n, %) | 340 (9.62) | 340 (9.62) | 0.00 | 619 (9.07) | 1230 (4.51) | 0.18 |
| Psoriasis (n, %) | 0.01 | 0.00 | ||||
| No | 3479 (98.58) | 3480 (98.59) | 6730 (98.65) | 26,924 (98.67) | ||
| Yes | 50 (1.42) | 50 (1.41) | 92 (1.35) | 364 (1.33) | ||
| Characteristics | N of Thyroid Cancer | N of Control | Odd Ratios for Thyroid Cancer (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude † | p Value | Overlap Weighted Model † | p Value | |
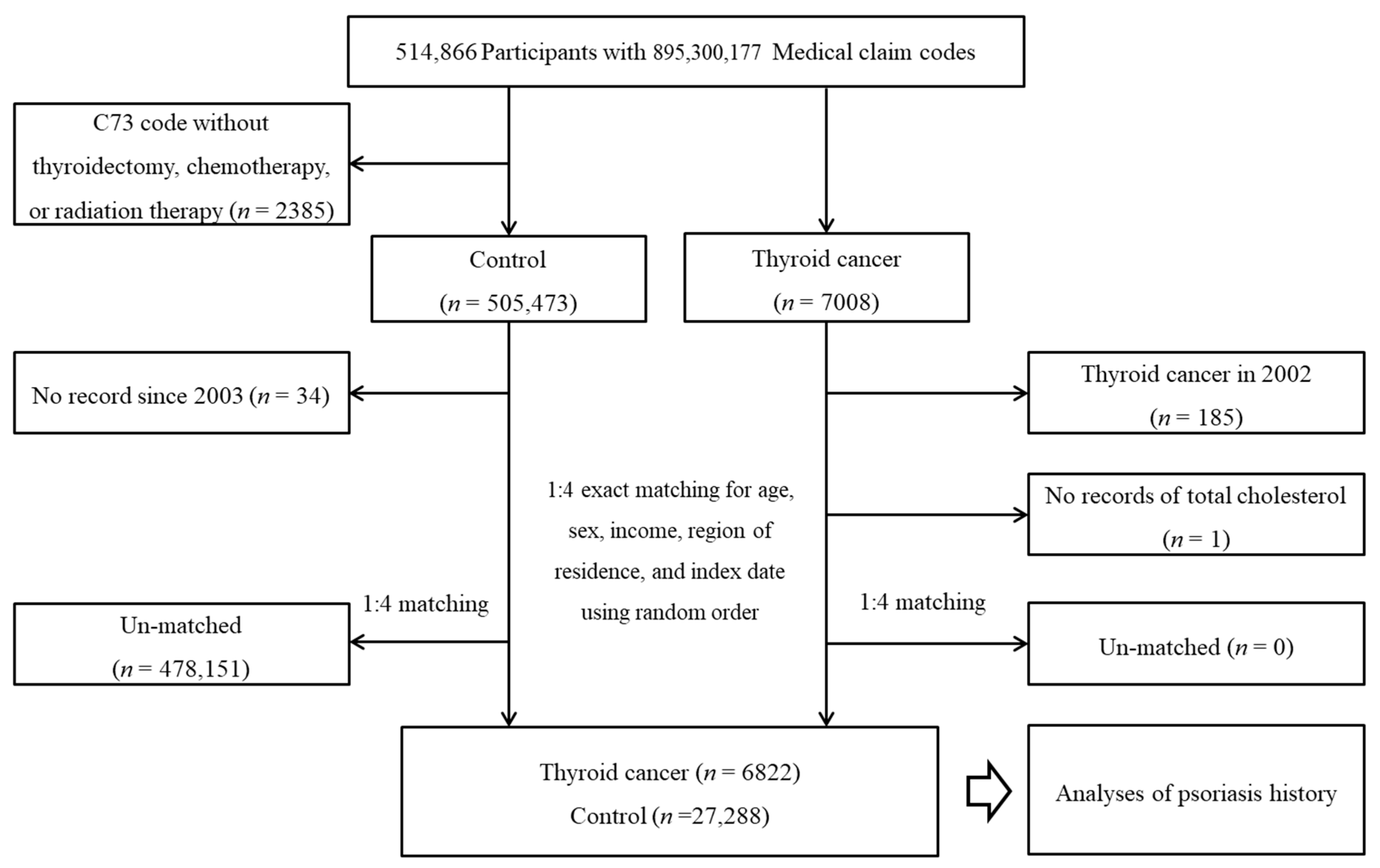
| Total participants (n = 34,110) | ||||||
| Control | 6730/6822 (98.7) | 26,924/27,288 (98.7) | 1 | 1 | ||
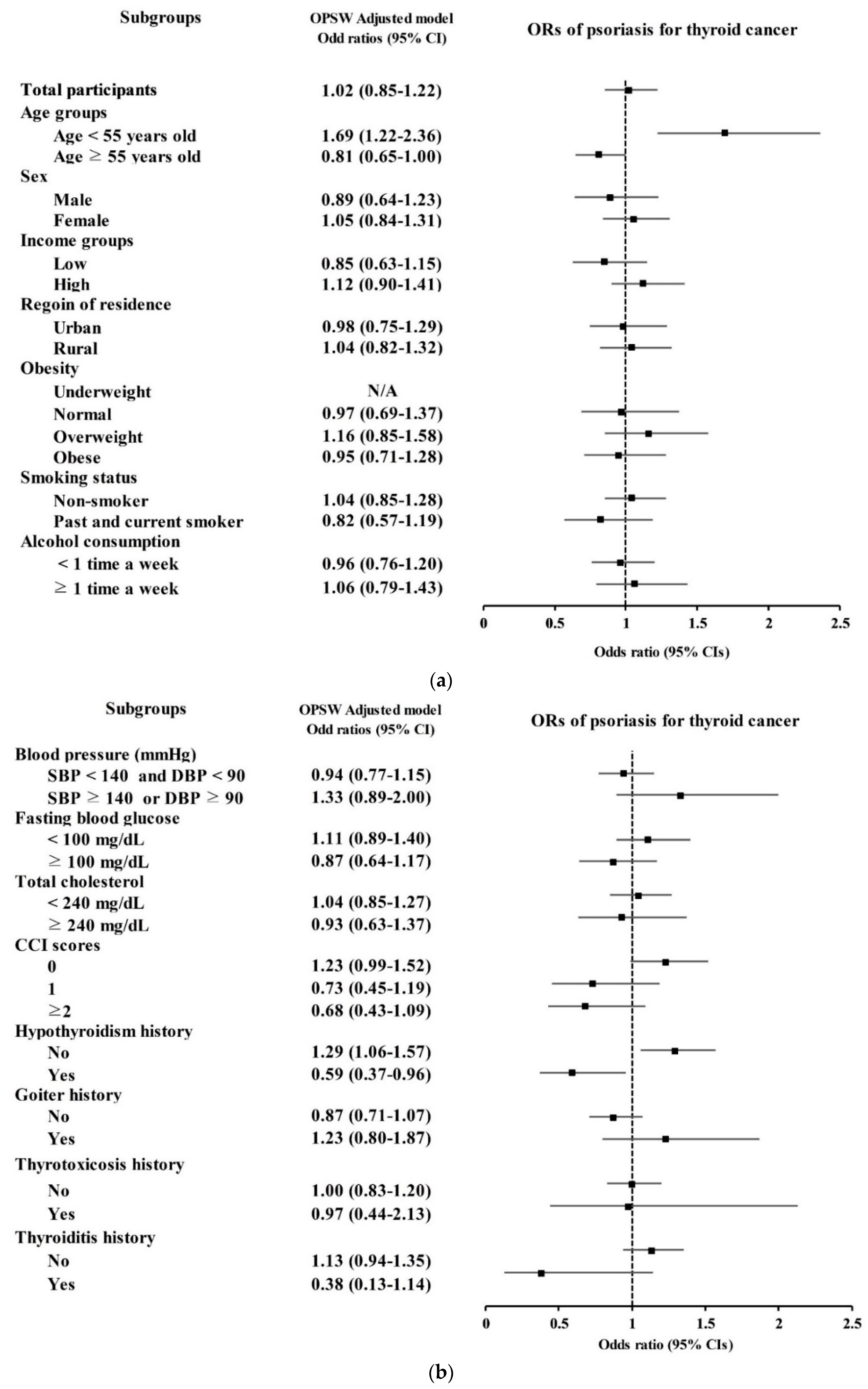
| Psoriasis | 92/6822 (1.3) | 364/27,288 (1.3) | 1.01 (0.80–1.27) | 0.925 | 1.02 (0.85–1.22) | 0.865 |
| Age < 55 years old (n = 12,940) | ||||||
| Control | 2552/2588 (98.6) | 10,250/10,352 (99.0) | 1 | 1 | ||
| Psoriasis | 36/2588 (1.4) | 102/10,352 (1.0) | 1.42 (0.97–2.08) | 0.073 | 1.69 (1.22–2.36) | 0.002 * |
| Age ≥ 55 years old (n = 21,170) | ||||||
| Control | 4178/4234 (98.7) | 16,674/16,936 (98.5) | 1 | 1 | ||
| Psoriasis | 56/4234 (1.3) | 262/16,936 (1.5) | 0.85 (0.64–1.14) | 0.284 | 0.81 (0.65–1.00) | 0.054 |
| Male (n = 7565) | ||||||
| Control | 1482/1513 (98.0) | 5925/6052 (97.9) | 1 | 1 | ||
| Psoriasis | 31/1513 (2.0) | 127/6052 (2.1) | 0.98 (0.66–1.45) | 0.905 | 0.89 (0.64–1.23) | 0.486 |
| Female (n = 26,545) | ||||||
| Control | 5248/5309 (98.9) | 20,999/21,236 (98.9) | 1 | 1 | ||
| Psoriasis | 61/5309 (1.1) | 237/21,236 (1.1) | 1.03 (0.78–1.37) | 0.837 | 1.05 (0.84–1.31) | 0.653 |
| Low-income group (n = 13,475) | ||||||
| Control | 2663/2695 (98.8) | 10,626/10,780 (98.6) | 1 | 1 | ||
| Psoriasis | 32/2695 (1.2) | 154/10,780 (1.4) | 0.83 (0.57–1.22) | 0.338 | 0.85 (0.63–1.15) | 0.286 |
| High-income group (n = 20,635) | ||||||
| Control | 4067/4127 (98.5) | 16,298/16,508 (98.7) | 1 | 1 | ||
| Psoriasis | 60/4127 (1.5) | 210/16,508 (1.3) | 1.14 (0.86–1.53) | 0.358 | 1.12 (0.90–1.41) | 0.318 |
| Urban resident (n = 16,105) | ||||||
| Control | 3182/3221 (98.8) | 12,717/12,884 (98.7) | 1 | 1 | ||
| Psoriasis | 39/3221 (1.2) | 167/12,884 (1.3) | 0.93 (0.66–1.33) | 0.705 | 0.98 (0.75–1.29) | 0.892 |
| Rural resident (n = 18,005) | ||||||
| Control | 3548/3601 (98.5) | 14,207/14,404 (98.6) | 1 | 1 | ||
| Psoriasis | 53/3601 (1.5) | 197/14,404 (1.4) | 1.08 (0.79–1.46) | 0.633 | 1.04 (0.82–1.32) | 0.737 |
| Characteristics | N of Thyroid Cancer | N of Control | Odd Ratios for Thyroid Cancer (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude † | p Value | Overlap Weighted Model † | p Value | |
| Obesity | ||||||
| Underweight (n = 764) | 0/186 (0.0) | 8/578 (1.4) | N/A | N/A | ||
| Normal (n = 12,317) | 23/2210 (1.0) | 112/10,107 (1.1) | 0.94 (0.60–1.48) | 0.787 | 0.97 (0.69–1.37) | 0.883 |
| Overweight (n = 9389) | 33/1936 (1.7) | 104/7453 (1.4) | 1.23 (0.83–1.82) | 0.313 | 1.16 (0.85–1.58) | 0.353 |
| Obese (n = 11,733) | 36/2583 (1.4) | 140/9150 (1.5) | 0.91 (0.63–1.32) | 0.615 | 0.95 (0.71–1.28) | 0.745 |
| Smoking status | ||||||
| Nonsmoker (n = 29,086) | 68/5904 (1.2) | 270/23,182 (1.2) | 0.99 (0.76–1.29) | 0.934 | 1.04 (0.85–1.28) | 0.692 |
| Past and current smoker (n = 5024) | 24/918 (2.6) | 94/4106 (2.3) | 1.15 (0.73–1.80) | 0.557 | 0.82 (0.57–1.19) | 0.303 |
| Alcohol consumption | ||||||
| <1 time a week (n = 25,334) | 55/5158 (1.1) | 241/20,176 (1.2) | 0.89 (0.66–1.20) | 0.445 | 0.96 (0.76–1.20) | 0.696 |
| ≥1 time a week (n = 8776) | 37/1664 (2.2) | 123/7112 (1.7) | 1.29 (0.89–1.87) | 0.176 | 1.06 (0.79–1.43) | 0.690 |
| Blood pressure (mmHg) | ||||||
| SBP < 140 and DBP < 90 (n = 27,315) | 70/5455 (1.3) | 292/21,860 (1.3) | 0.96 (0.74–1.25) | 0.764 | 0.94 (0.77–1.15) | 0.56 |
| SBP ≥ 140 or DBP ≥ 90 (n = 6795) | 22/1367 (1.6) | 72/5428 (1.3) | 1.22 (0.75–1.97) | 0.424 | 1.33 (0.89–2.00) | 0.166 |
| Fasting blood glucose (mg/dL) | ||||||
| <100 (n = 22,864) | 62/4591 (1.4) | 233/18,273 (1.3) | 1.06 (0.80–1.41) | 0.681 | 1.11 (0.89–1.40) | 0.347 |
| ≥100 (n = 11,246) | 30/2231 (1.3) | 131/9015 (1.5) | 0.92 (0.62–1.38) | 0.700 | 0.87 (0.64–1.17) | 0.360 |
| Total cholesterol (mg/dL) | ||||||
| <240 (n = 29,100) | 76/5898 (1.3) | 311/23,202 (1.3) | 0.96 (0.75–1.24) | 0.759 | 1.04 (0.85–1.27) | 0.722 |
| ≥240 (n = 5010) | 16/924 (1.7) | 53/4086 (1.3) | 1.34 (0.76–2.36) | 0.307 | 0.93 (0.63–1.37) | 0.703 |
| CCI scores | ||||||
| 0 (n = 22,996) | 56/3760 (1.5) | 245/19,236 (1.3) | 1.17 (0.87–1.57) | 0.288 | 1.23 (0.99–1.52) | 0.063 |
| 1 (n = 5413) | 14/1234 (1.1) | 63/4179 (1.5) | 0.75 (0.42–1.34) | 0.333 | 0.73 (0.45–1.19) | 0.208 |
| ≥2 (n = 5701) | 22/1828 (1.2) | 56/3873 (1.4) | 0.83 (0.51–1.36) | 0.463 | 0.68 (0.43–1.09) | 0.111 |
| Hypothyroidism history | ||||||
| No (n = 28,008) | 53/3009 (1.8) | 327/24,999 (1.3) | 1.35 (1.01–1.81) | 0.043 * | 1.29 (1.06–1.57) | 0.012 * |
| Yes (n = 6102) | 39/3813 (1.0) | 37/2289 (1.6) | 0.63 (0.40–0.99) | 0.045 * | 0.59 (0.37–0.96) | 0.034 * |
| Goiter history | ||||||
| No (n = 27,216) | 37/2990 (1.2) | 330/24,226 (1.4) | 0.91 (0.64–1.28) | 0.577 | 0.87 (0.71–1.07) | 0.181 |
| Yes (n = 6894) | 55/3832 (1.4) | 34/3062 (1.1) | 1.30 (0.84–1.99) | 0.236 | 1.23 (0.80–1.87) | 0.340 |
| Thyrotoxicosis history | ||||||
| No (n = 32,119) | 84/6125 (1.4) | 347/25,994 (1.3) | 1.03 (0.81–1.31) | 0.822 | 1.00 (0.83–1.20) | 0.994 |
| Yes (n = 1991) | 8/697 (1.1) | 17/1294 (1.3) | 0.87 (0.37–2.03) | 0.751 | 0.97 (0.44–2.13) | 0.944 |
| Thyroiditis history | ||||||
| No (n = 32,261) | 86/6203 (1.4) | 345/26,058 (1.3) | 1.05 (0.83–1.33) | 0.696 | 1.13 (0.94–1.35) | 0.205 |
| Yes (n = 1849) | 6/619 (1.0) | 19/1230 (1.5) | 0.62 (0.25–1.57) | 0.317 | 0.38 (0.13–1.14) | 0.085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Chung, J.; Choi, H.G. Thyroid Cancer and Psoriasis: A Nested Case–Control Study. Diagnostics 2022, 12, 2297. https://doi.org/10.3390/diagnostics12102297
Kim SY, Yoo DM, Chung J, Choi HG. Thyroid Cancer and Psoriasis: A Nested Case–Control Study. Diagnostics. 2022; 12(10):2297. https://doi.org/10.3390/diagnostics12102297
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Juyong Chung, and Hyo Geun Choi. 2022. "Thyroid Cancer and Psoriasis: A Nested Case–Control Study" Diagnostics 12, no. 10: 2297. https://doi.org/10.3390/diagnostics12102297