
Clinical Sensitivity, Specificity and Epidemiology of SARS-CoV-2 Serological Testing Using the Biozek COVID-19 Test


Abstract
:1. Introduction
2. Materials and Methods
2.1. Test Characteristics and Procedures
2.2. Specimens for Calculating Clinical Sensitivity and Specificity of the Biozek COVID-19 Test
2.3. Specimens for Analyzing Sequential Samples of PCR Positive Persons
2.4. Specimens for Analyzing the Association between Patient-Reported Symptoms between Negative and Seropositive (Non-Hospitalized) Patients
2.5. Statistical Analysis
3. Results
3.1. Validation Biozek COVID-19 Test
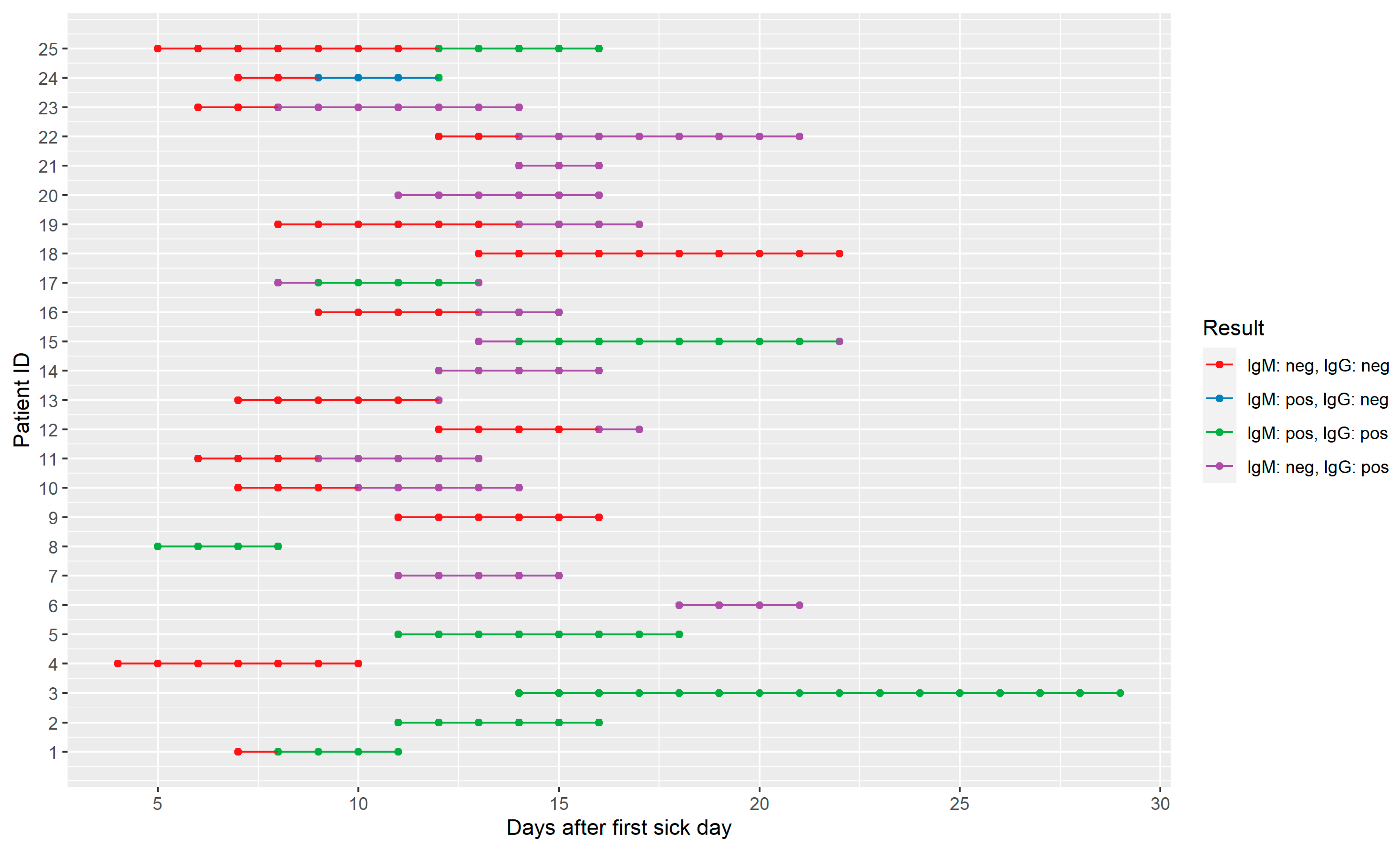
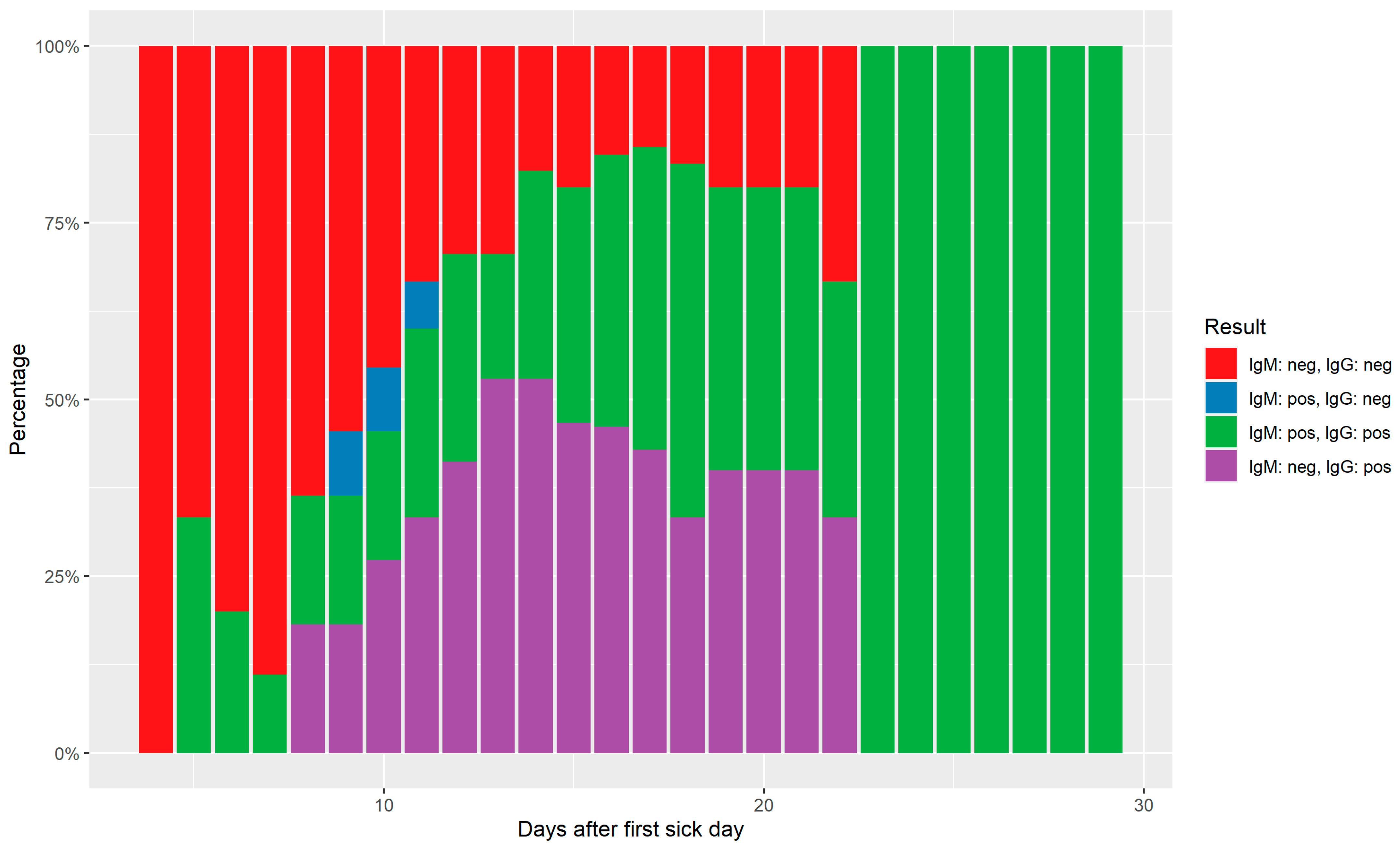
3.2. Serodynamics of PCR Positive Persons
3.3. Association Model between Patient Reported Symptoms and Seropositivity
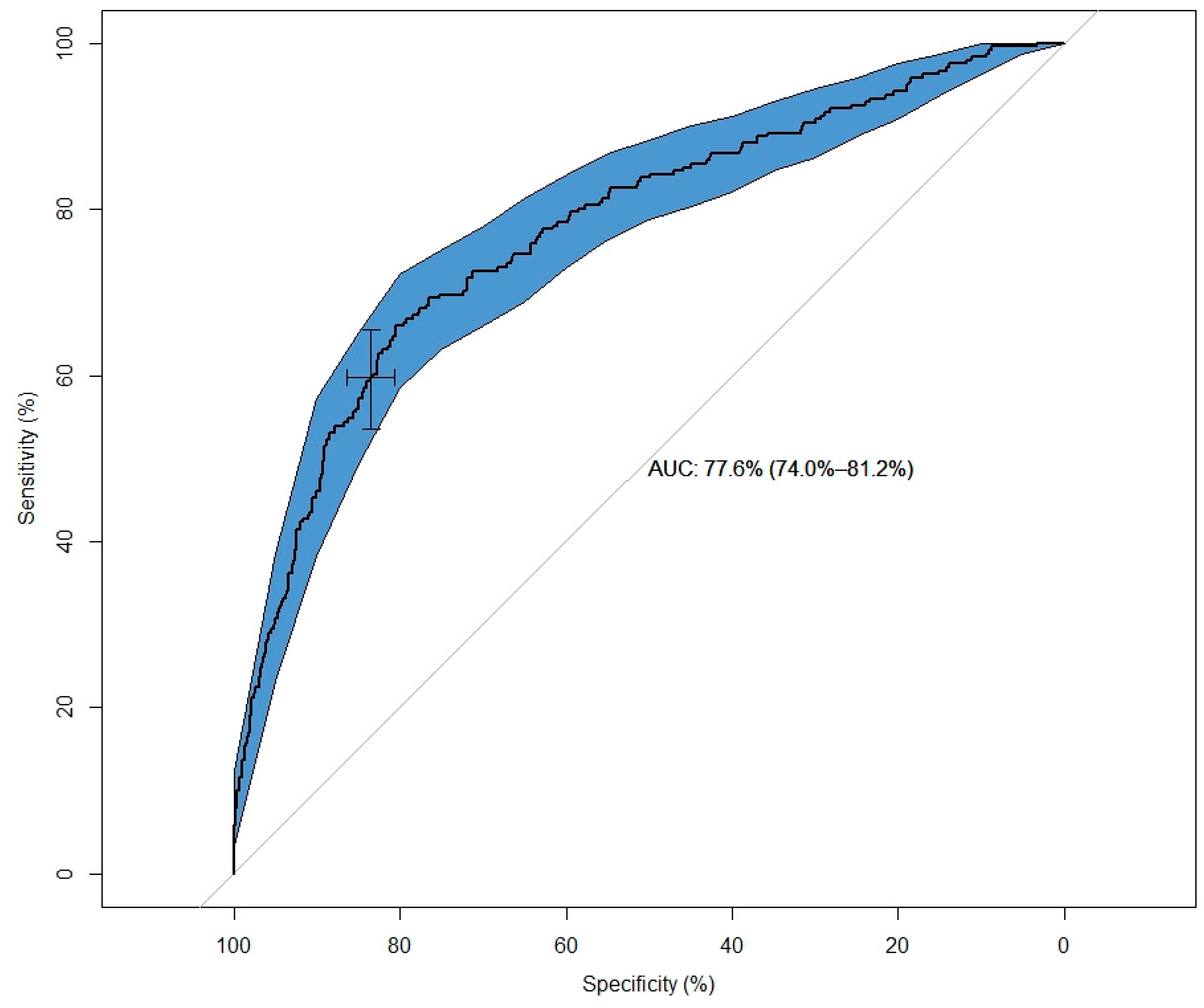
3.4. Prediction Model for SARS-CoV-2 Seropositivity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartsch, S.M.; Ferguson, M.C.; McKinnell, J.A.; O’Shea, K.J.; Wedlock, P.T.; Siegmund, S.S.; Lee, B.Y. The Potential Health Care Costs and Resource Use Associated with COVID-19 In the United States. Health Aff. 2020, 39, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Jo, M.W.; Go, D.S.; Kim, R.; Lee, S.W.; Ock, M.; Kim, Y.E.; Oh, I.-H.; Yoon, S.-J.; Park, H. The Burden of Disease due to COVID-19 in Korea Using Disability-Adjusted Life Years. J. Korean Med. Sci. 2020, 35, e199. [Google Scholar] [CrossRef]
- Salathé, M.; Althaus, C.L.; Neher, R.; Stringhini, S.; Hodcroft, E.; Fellay, J.; Zwahlen, M.; Senti, G.; Battegay, M.; Wilder-Smith, A.; et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med. Wkly. 2020, 19, w20225. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Chang, L.; Wang, L. Laboratory testing of SARS-CoV, MERS-CoV, and SARS-CoV-2 (2019-nCoV): Current status, challenges, and countermeasures. Rev. Med. Virol. 2020, 30, e2106. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Wang, Y.; Tong, Z.; Liu, X. Retest positive for SARS-CoV-2 RNA of “recovered” patients with COVID-19: Persistence, sampling issues, or re-infection? J. Med. Virol. 2020, 92, 2263–2265. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Poon, B.H.; Kiat Puar, T.H.; Shan Quah, J.L.; Loh, W.J.; Wong, Y.J.; Tan, T.Y. COVID-19 and the Risk to Health Care Workers: A Case Report. Ann. Intern. Med. 2020, 172, 766–767. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; et al. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Place, S.; Van Laethem, Y.; Cabaraux, P.; Mat, Q.; Huet, K.; Plzak, J.; Horoi, M.; Hans, S.; et al. COVID-19 Task Force of YO-IFOS. Clinical and epidemiological characteristics of 1420 European patients with mild-to-moderate coronavirus disease 2019. J. Intern. Med. 2020, 288, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Huijskens, M.J.A.J.; Castel, R.; Vermeer, H.J.; Verheijen, F.M. Evaluation of Diabetes Care parameters in capillary blood collected with a novel sampling device. Pract. Lab. Med. 2019, 17, e00135. [Google Scholar] [CrossRef] [PubMed]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef]
- Wu, J.L.; Tseng, W.P.; Lin, C.H.; Lee, T.F.; Chung, M.Y.; Huang, C.H.; Chen, S.-Y.; Hsueh, P.-R.; Chen, S.-C. Four point-of-care lateral flow immunoassays for diagnosis of COVID-19 and for assessing dynamics of antibody responses to SARS-CoV-2. J. Infect. 2020, 81, 435–442. [Google Scholar] [CrossRef]
- Hoffman, T.; Nissen, K.; Krambrich, J.; Rönnberg, B.; Akaberi, D.; Esmaeilzadeh, M.; Salaneck, E.; Lindahl, J.; Lundkvist, A. Evaluation of a COVID-19 IgM and IgG rapid test; an efficient tool for assessment of past exposure to SARS-CoV-2. Infect. Ecol. Epidemiol. 2020, 10, 1754538. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Lin, R.T.P.; Renia, L.; Ng, L.F.P. Serological Approaches for COVID-19: Epidemiologic Perspective on Surveillance and Control. Front. Immunol. 2020, 11, 879. [Google Scholar] [CrossRef]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W.; et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med. Virol. 2020, 92, 1518–1524. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, S.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. ENE-COVID Study Group. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 525–544. [Google Scholar] [CrossRef]
- RIVM.nl. Bilthoven: National Institute for Public Health and the Environment. 2021. Available online: https://www.rivm.nl/en/pienter-corona-study/results (accessed on 1 June 2021).
- Birra, D.; Benucci, M.; Landolfi, L.; Merchionda, A.; Loi, G.; Amato, P.; Licata, G.; Quartuccio, L.; Triggiani, M.; Moscato, P. COVID 19: A clue from innate immunity. Immunol. Res. 2020, 68, 161–168. [Google Scholar] [CrossRef]
- Corman, V.M.; Albarrak, A.M.; Omrani, A.S.; Albarrak, M.M.; Farah, M.E.; Almasri, M.; Muth, D.; Sieberg, A.; Meyer, B.; Assiri, A.M.; et al. Viral Shedding and Antibody Response in 37 Patients with Middle East Respiratory Syndrome Coronavirus Infection. Clin. Infect. Dis. 2016, 62, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Peiris, J.S.; Chu, C.M.; Cheng, V.C.; Chan, K.S.; Hung, I.F.; Poon, L.L.; Law, K.I.; Tang, B.S.F.; Hon, T.Y.W.; Chan, G.S.; et al. Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: A prospective study. Lancet 2003, 361, 1767–1772. [Google Scholar] [CrossRef] [Green Version]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Mustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Menni, C.; Sudre, C.H.; Steves, C.J.; Ourselin, S.; Spector, T.D. Quantifying additional COVID-19 symptoms will save lives. Lancet 2020, 395, e107–e108. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| IgM | IgG | Total | |||
|---|---|---|---|---|---|
| Pos | Neg | Pos | Neg | ||
| Severe cases | 12 | 35 | 31 | 16 | 47 |
| Mild/asymptomatic cases | 5 | 45 | 46 | 4 | 50 |
| Total cases | 17 | 80 | 77 | 20 | 97 |
| Random negative controls | 1 | 9 | 0 | 10 | 10 |
| Other acute respiratory infections | 0 | 7 | 0 | 7 | 7 |
| Non-SARS-CoV-2 corona infections | 0 | 12 | 0 | 12 | 12 |
| Negative SARS-CoV-2 PCR patients | 0 | 190 | 1 | 189 | 190 |
| Total controls | 1 | 218 | 1 | 218 | 219 |
| Mean Number of Days between First Sick Day and Testing (Range) | Sensitivity | Sensitivity (≥10 Days) | Specificity | |
|---|---|---|---|---|
| Severe cases | 14 (2–90) | |||
| IgM | 25.5% | 30.0% | 99.5% | |
| IgG | 66.0% | 90.0% | 99.5% | |
| IgM and IgG | 68.1% | 90.0% | 99.1% | |
| Mild/asymptomatic cases | 50 (0–117) | |||
| IgM | 10.0% | 10.2% | 99.5% | |
| IgG | 92.0% | 91.8% | 99.5% | |
| IgM and IgG | 92.0% | 91.8% | 99.1% | |
| Combined severe and asymptomatic cases | 32 (0–117) | |||
| IgM | 17.5% | 17.7% | 99.5% | |
| IgG | 79.4% | 91.1% | 99.5% | |
| IgM and IgG | 80.4% | 91.1% | 99.1% |
| Variable | IgM: Neg & IgG: Neg | IgG: Pos | Total | OR (Univariable) | OR (Multivariable) | |
|---|---|---|---|---|---|---|
| Age | Mean (SD) | 45.6 (15.1) | 48.3 (13.7) | 46.3 (14.8) | 1.01 (1.01–1.02, p < 0.001) | 1.02 (1.01–1.03, p < 0.001) |
| Time between onset of symptoms and testing | Mean (SD) | 48.4 (22.8) | 39.2 (15.0) | 46.0 (21.4) | 0.97 (0.97–0.98, p < 0.001) | 0.97 (0.96–0.97, p < 0.001) |
| Sex | Female | 1365 (52.4) | 428 (48.7) | 1793 (51.4) | ||
| Male | 1242 (47.6) | 451 (51.3) | 1693 (48.6) | 1.16 (0.99–1.35, p = 0.060) | 1.19 (0.99–1.44, p = 0.068) | |
| Fever | No | 1513 (58.0) | 345 (39.2) | 1858 (53.3) | ||
| Yes | 1094 (42.0) | 534 (60.8) | 1628 (46.7) | 2.14 (1.83–2.50, p < 0.001) | 1.70 (1.40–2.07, p < 0.001) | |
| Sneezing | No | 1510 (57.9) | 559 (63.6) | 2069 (59.4) | ||
| Yes | 1097 (42.1) | 320 (36.4) | 1417 (40.6) | 0.79 (0.67–0.92, p = 0.003) | 0.70 (0.57–0.85, p < 0.001) | |
| Runny nose | No | 932 (35.7) | 324 (36.9) | 1256 (36.0) | ||
| Yes | 1675 (64.3) | 555 (63.1) | 2230 (64.0) | 0.95 (0.81–1.12, p = 0.553) | 0.87 (0.71–1.07, p = 0.197) | |
| Sore throat | No | 1038 (39.8) | 442 (50.3) | 1480 (42.5) | ||
| Yes | 1569 (60.2) | 437 (49.7) | 2006 (57.5) | 0.65 (0.56–0.76, p < 0.001) | 0.48 (0.39–0.59, p < 0.001) | |
| Short breath | No | 1429 (54.8) | 426 (48.5) | 1855 (53.2) | ||
| Yes | 1178 (45.2) | 453 (51.5) | 1631 (46.8) | 1.29 (1.11–1.50, p = 0.001) | 0.82 (0.67–0.99, p = 0.045) | |
| Loss of smell | No | 2016 (77.3) | 312 (35.5) | 2328 (66.8) | ||
| Yes | 591 (22.7) | 567 (64.5) | 1158 (33.2) | 6.20 (5.26–7.32, p < 0.001) | 6.82 (5.61–8.31, p < 0.001) | |
| Itchy skin | No | 2308 (88.5) | 769 (87.5) | 3077 (88.3) | ||
| Yes | 299 (11.5) | 110 (12.5) | 409 (11.7) | 1.10 (0.87–1.39, p = 0.405) | 1.07 (0.81–1.42, p = 0.617) | |
| Diarrhea | No | 1692 (64.9) | 539 (61.3) | 2231 (64.0) | ||
| Yes | 915 (35.1) | 340 (38.7) | 1255 (36.0) | 1.17 (1.00–1.37, p = 0.056) | 1.14 (0.93–1.40, p = 0.209) | |
| Abdominal pain | No | 1820 (69.8) | 690 (78.5) | 2510 (72.0) | ||
| Yes | 787 (30.2) | 189 (21.5) | 976 (28.0) | 0.63 (0.53–0.76, p < 0.001) | 0.58 (0.46–0.73, p < 0.001) | |
| Headache | No | 867 (33.3) | 246 (28.0) | 1113 (31.9) | ||
| Yes | 1740 (66.7) | 633 (72.0) | 2373 (68.1) | 1.28 (1.08–1.52, p = 0.004) | 1.12 (0.90–1.40, p = 0.323) | |
| Tired | No | 548 (21.0) | 110 (12.5) | 658 (18.9) | ||
| Yes | 2059 (79.0) | 769 (87.5) | 2828 (81.1) | 1.86 (1.50–2.33, p < 0.001) | 1.04 (0.78–1.40, p = 0.789) | |
| Contact with ILI | No | 1275 (48.9) | 334 (38.0) | 1609 (46.2) | ||
| Yes | 1332 (51.1) | 545 (62.0) | 1877 (53.8) | 1.56 (1.34–1.83, p < 0.001) | 1.46 (1.21–1.76, p < 0.001) | |
| Location with many people | No | 774 (29.7) | 220 (25.0) | 994 (28.5) | ||
| Yes | 1833 (70.3) | 659 (75.0) | 2492 (71.5) | 1.26 (1.06–1.51, p = 0.008) | 1.16 (0.93–1.45, p = 0.182) | |
| Foreign country | No | 1700 (65.2) | 478 (54.4) | 2178 (62.5) | ||
| Yes | 907 (34.8) | 401 (45.6) | 1308 (37.5) | 1.57 (1.35–1.84, p < 0.001) | 1.67 (1.38–2.04, p < 0.001) | |
| Which foreign country | No | 1700 (65.2) | 478 (54.4) | 2178 (62.5) | ||
| Belgium | 16 (0.6) | 7 (0.8) | 23 (0.7) | 1.56 (0.60–3.67, p = 0.332) | ||
| Germany | 48 (1.8) | 7 (0.8) | 55 (1.6) | 0.52 (0.21–1.08, p = 0.107) | ||
| France | 55 (2.1) | 25 (2.8) | 80 (2.3) | 1.62 (0.98–2.59, p = 0.052) | ||
| Italy | 109 (4.2) | 29 (3.3) | 138 (4.0) | 0.95 (0.61–1.42, p = 0.797) | ||
| Austria | 328 (12.6) | 247 (28.1) | 575 (16.5) | 2.68 (2.21–3.25, p < 0.001) | ||
| Spain | 78 (3.0) | 19 (2.2) | 97 (2.8) | 0.87 (0.51–1.41, p = 0.582) | ||
| Other European countries | 103 (4.0) | 29 (3.3) | 132 (3.8) | 1.00 (0.64–1.51, p = 0.995) | ||
| Africa | 40 (1.5) | 12 (1.4) | 52 (1.5) | 1.07 (0.53–1.99, p = 0.846) | ||
| China | 20 (0.8) | 20 (0.6) | ||||
| Middle East | 24 (0.9) | 7 (0.8) | 31 (0.9) | 1.04 (0.41–2.30, p = 0.933) | ||
| North America | 49 (1.9) | 13 (1.5) | 62 (1.8) | 0.94 (0.49–1.70, p = 0.854) | ||
| South America | 27 (1.0) | 5 (0.6) | 32 (0.9) | 0.66 (0.22–1.58, p = 0.394) | ||
| Australia | 10 (0.4) | 1 (0.1) | 11 (0.3) | 0.36 (0.02–1.86, p = 0.325) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souverein, D.; Mank, T.G.; Euser, S.M.; Herpers, B.L. Clinical Sensitivity, Specificity and Epidemiology of SARS-CoV-2 Serological Testing Using the Biozek COVID-19 Test. Diagnostics 2022, 12, 60. https://doi.org/10.3390/diagnostics12010060
Souverein D, Mank TG, Euser SM, Herpers BL. Clinical Sensitivity, Specificity and Epidemiology of SARS-CoV-2 Serological Testing Using the Biozek COVID-19 Test. Diagnostics. 2022; 12(1):60. https://doi.org/10.3390/diagnostics12010060
Chicago/Turabian StyleSouverein, Dennis, Theo G. Mank, Sjoerd M. Euser, and Bjorn L. Herpers. 2022. "Clinical Sensitivity, Specificity and Epidemiology of SARS-CoV-2 Serological Testing Using the Biozek COVID-19 Test" Diagnostics 12, no. 1: 60. https://doi.org/10.3390/diagnostics12010060