
Comparison of HE4, CA125, ROMA and CPH-I for Preoperative Assessment of Adnexal Tumors

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
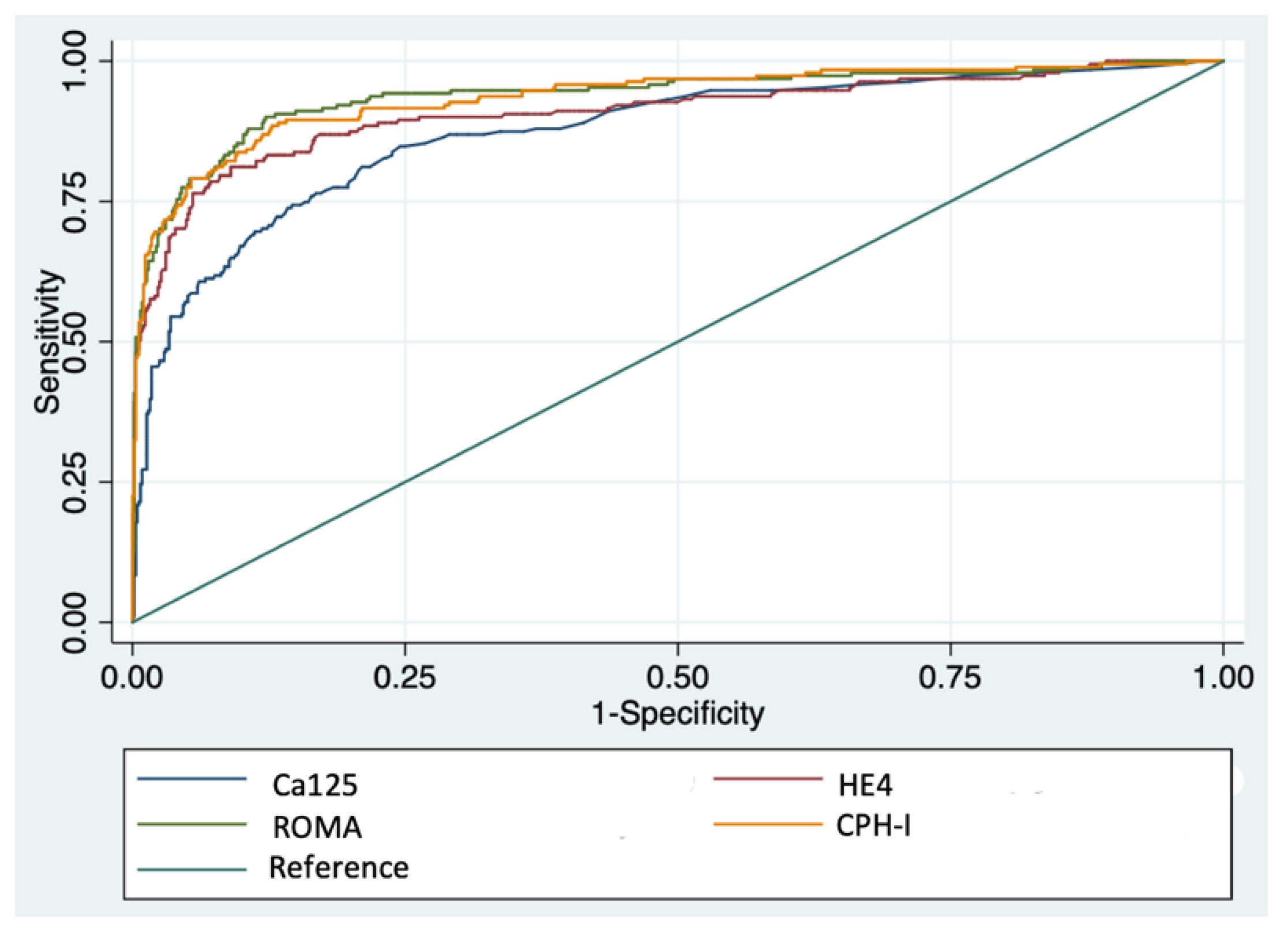
3. Results
4. Discussion
4.1. Diagnostic Performance of Tumor Markers and Probabilistic Indexes in Overall Population
4.2. Diagnostic Performance of Tumor Markers in Specific Subgroups of Patients
4.3. The Role of Isolated CA125 for Preoperative Assessment od Adnexal Tumors
4.4. Beyond CA125 and HE4: The Role of Novel Tumor Markers and Ultrasound
4.5. Strengths and Limitations of the Present Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giede, K.C.; Kieser, K.; Dodge, J.; Rosen, B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol. Oncol. 2005, 99, 447–461. [Google Scholar] [CrossRef]
- Piovano, E.; Cavallero, C.; Fuso, L.; Viora, E.; Ferrero, A.; Gregori, G.; Grillo, C.; Macchi, C.; Mengozzi, G.; Mitidieri, M.; et al. Diagnostic accuracy and cost-effectiveness of different strategies to triage women with adnexal masses: A prospective study. Ultrasound Obstet. Gynecol. 2017, 50, 395–403. [Google Scholar] [CrossRef]
- Sayasneh, A.; Kaijser, J.; Preisler, J.; Smith, A.A.; Raslan, F.; Johnson, S.; Husicka, R.; Ferrara, L.; Stalder, C.; Ghaem-Maghami, S.; et al. Accuracy of ultrasonography performed by examiners with varied training and experience in predicting specific pathology of adnexal masses. Ultrasound Obstet. Gynecol. 2015, 45, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Alcázar, J.L.; Pascual, M.A.; Graupera, B.; Aubá, M.; Errasti, T.; Olartecoechea, B.; Ruiz-Zambrana, A.; Hereter, L.; Ajossa, S.; Guerriero, S. External validation of IOTA simple descriptors and simple rules for classifying adnexal masses. Ultrasound Obstet. Gynecol. 2016, 48, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Knafel, A.; Banas, T.; Nocun, A.; Wiechec, M.; Jach, R.; Ludwin, A.; Kabzinska-Turek, M.; Pietrus, M.; Pitynski, K. The prospective external validation of International Ovarian Tumor Analysis (IOTA) simple rules in the hands of level i and II examiners. Ultraschall der Medizin 2016, 37, 516–523. [Google Scholar] [CrossRef]
- Nunes, N.; Ambler, G.; Foo, X.; Naftalin, J.; Widschwendter, M.; Jurkovic, D. Use of IOTA simple rules for diagnosis of ovarian cancer: Meta-analysis. Ultrasound Obstet. Gynecol. 2014, 44, 503–514. [Google Scholar] [CrossRef] [Green Version]
- Maggino, T.; Gadducci, A.; D’Addario, V.; Pecorelli, S.; Lissoni, A.; Stella, M.; Romagnolo, C.; Federghini, M.; Zucca, S.; Trio, D.; et al. Prospective multicenter study on CA 125 in postmenopausal pelvic masses. Gynecol. Oncol. 1994, 54, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Robert, C.B., Jr. The CA125 tumour-associate antigen: A review of the literature. Hum. Reprod. 1989, 4, 1–12. [Google Scholar] [CrossRef]
- Moore, R.G.; Brown, A.K.; Miller, M.C.; Skates, S.; Allard, W.J.; Verch, T.; Steinhoff, M.; Messerlian, G.; DiSilvestro, P.; Granai, C.O.; et al. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol. Oncol. 2008, 108, 402–408. [Google Scholar] [CrossRef]
- Galgano, M.T.; Hampton, G.M.; Frierson, H.F. Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod. Pathol. 2006, 19, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Moore, R.G.; Miller, M.C.; Eklund, E.E.; Lu, K.H.; Bast, R.C.; Lambert-Messerlian, G. Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age. Am. J. Obstet. Gynecol. 2012, 206, 349-e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudero, J.M.; Auge, J.M.; Filella, X.; Torne, A.; Pahisa, J.; Molina, R. Comparison of serum human epididymis protein 4 with cancer antigen 125 as a tumor marker in patients with malignant and nonmalignant diseases. Clin. Chem. 2011, 57, 1534–1544. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayyani, F.; Uhlig, S.; Colson, B.; Simon, K.; Rolny, V.; Morgenstern, D.; Schlumbrecht, M. Diagnostic Performance of Risk of Ovarian Malignancy Algorithm Against CA125 and HE4 in Connection with Ovarian Cancer: A Meta-analysis. Int. J. Gynecol. Cancer 2016, 26, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, M.A.; Høgdall, E.V.S.; Christensen, I.J.; Borgfeldt, C.; Kalapotharakos, G.; Zdrazilova-Dubska, L.; Chovanec, J.; Lok, C.A.R.; Stiekema, A.; Mutz-Dehbalaie, I.; et al. A novel diagnostic index combining HE4, CA125 and age may improve triage of women with suspected ovarian cancer—An international multicenter study in women with an ovarian mass. Gynecol. Oncol. 2015, 138, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Minar, L.; Felsinger, M.; Cermakova, Z.; Zlamal, F.; Bienertova-Vasku, J. Comparison of the Copenhagen Index versus ROMA for the preoperative assessment of women with ovarian tumors. Int. J. Gynecol. Obstet. 2018, 140, 241–246. [Google Scholar] [CrossRef]
- Han, K.H.; Park, N.H.; Kim, J.J.; Kim, S.; Kim, H.S.; Lee, M.; Song, Y.S. The power of the risk of ovarian malignancy algorithm considering menopausal status: A comparison with CA 125 and HE4. J. Gynecol. Oncol. 2019, 30, e83. [Google Scholar] [CrossRef]
- Zhen, S.; Bian, L.; Chang, L.; Gao, X. Comparison of serum human epididymis protein 4 and carbohydrate antigen 125 as markers in ovarian cancer: A meta-analysis. Mol. Clin. Oncol. 2014, 2, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Van Gorp, T.; Cadron, I.; Despierre, E.; Daemen, A.; Leunen, K.; Amant, F.; Timmerman, D.; De Moor, B.; Vergote, I. HE4 and CA125 as a diagnostic test in ovarian cancer: Prospective validation of the Risk of Ovarian Malignancy Algorithm. Br. J. Cancer 2011, 104, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, A.; Derchain, S.F.; Pitta, D.R.; De Angelo Andrade, L.A.L.; Sarian, L.O. Comparing the Copenhagen Index (CPH-I) and Risk of Ovarian Malignancy Algorithm (ROMA): Two equivalent ways to differentiate malignant from benign ovarian tumors before surgery? Gynecol. Oncol. 2016, 140, 481–485. [Google Scholar] [CrossRef]
- Tran, D.T.; Vo, V.K.; Le, M.T.; Chuang, L.; Nguyen, V.Q.H. Copenhagen Index versus ROMA in preoperative ovarian malignancy risk stratification: Result from the first Vietnamese prospective cohort study. Gynecol. Oncol. 2021, 162, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Fishman, D.A.; Cohen, L.; Blank, S.V.; Shulman, L.; Singh, D.; Bozorgi, K.; Tamura, R.; Timor-Tritsch, I.; Schwartz, P.E. The role of ultrasound evaluation in the detection of early-stage epithelial ovarian cancer. Am. J. Obstet. Gynecol. 2005, 192, 1214–1221. [Google Scholar] [CrossRef]
- Kurman, R.J.; Carcangiu, M.L.; Harrington, C.S.; Young, R.H. WHO Classification of Tumours of Female Reproductive Organs, 4th ed.; IARC Publications: Lyon, France, 2014; p. 307. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Van Holsbeke, C.; Paladini, D.; Van Calster, B.; Vergote, I.; Van Huffel, S.; et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef]
- Timmerman, D.; Planchamp, F.; Bourne, T.; Landolfo, C.; du Bois, A.; Chiva, L.; Cibula, D.; Concin, N.; Fischerova, D.; Froyman, W.; et al. ESGO/ISUOG/IOTA/ESGE Consensus Statement on preoperative diagnosis of ovarian tumors. Ultrasound Obstet. Gynecol. 2021, 58, 148–168. [Google Scholar] [CrossRef]
- Moore, R.G.; Jabre-Raughley, M.; Brown, A.K.; Robison, K.M.; Miller, M.C.; Allard, W.J.; Kurman, R.J.; Bast, R.C.; Skates, S.J. Comparison of a novel multiple marker assay vs the Risk of Malignancy Index for the prediction of epithelial ovarian cancer in patients with a pelvic mass. Am. J. Obstet. Gynecol. 2010, 203, 228. [Google Scholar] [CrossRef] [Green Version]
- Melo, Â.; Veríssimo, R.; Farinha, M.; Martins, N.N.; Martins, F.N. Discriminative value of CA-125, HE4, Risk of Malignancy Index II (RMI-II) and Risk of Malignancy Algorithm (ROMA) in the differential diagnosis of pelvic masses: Conclusions from a referral Centre in Portugal. J. Obstet. Gynaecol. 2018, 38, 1140–1145. [Google Scholar] [CrossRef]
- Sandri, M.T.; Bottari, F.; Franchi, D.; Boveri, S.; Candiani, M.; Ronzoni, S.; Peiretti, M.; Radice, D.; Passerini, R.; Sideri, M. Comparison of HE4, CA125 and ROMA algorithm in women with a pelvic mass: Correlation with pathological outcome. Gynecol. Oncol. 2013, 128, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Danese, E.; Ruzzenente, O.; Bresciani, V.; Nuzzo, T.; Gelati, M.; Salvagno, G.L.; Franchi, M.; Lippi, G.; Guidi, G.C. The ROMA (Risk of Ovarian Malignancy Algorithm) for estimating the risk of epithelial ovarian cancer in women presenting with pelvic mass: Is it really useful? Clin. Chem. Lab. Med. 2011, 49, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Suri, A.; Perumal, V.; Ammalli, P.; Suryan, V.; Bansal, S.K. Diagnostic measures comparison for ovarian malignancy risk in Epithelial ovarian cancer patients: A meta-analysis. Sci. Rep. 2021, 11, 17308. [Google Scholar] [CrossRef] [PubMed]
- Nikolova, T.; Zivadinovic, R.; Evtimovska, N.; Klisarovska, V.; Stanojevic, M.; Georgievska, J.; Nikolova, N. Diagnostic performance of human epididymis protein 4 compared to a combination of biophysical and biochemical markers to differentiate ovarian endometriosis from epithelial ovarian cancer in premenopausal women. J. Obstet. Gynaecol. Res. 2017, 43, 1870–1879. [Google Scholar] [CrossRef]
- Kaijser, J.; Van Gorp, T.; Smet, M.E.; Van Holsbeke, C.; Sayasneh, A.; Epstein, E.; Bourne, T.; Vergote, I.; Van Calster, B.; Timmerman, D. Are serum HE4 or ROMA scores useful to experienced examiners for improving characterization of adnexal masses after transvaginal ultrasonography? Ultrasound Obstet. Gynecol. 2014, 43, 89–97. [Google Scholar] [CrossRef]
- Jacob, F.; Meier, M.; Caduff, R.; Goldstein, D.; Pochechueva, T.; Hacker, N.; Fink, D.; Heinzelmann-Schwarz, V. No benefit from combining HE4 and CA125 as ovarian tumor markers in a clinical setting. Gynecol. Oncol. 2011, 121, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Terzic, M.; Aimagambetova, G.; Norton, M.; Della Corte, L.; Marín-Buck, A.; Lisón, J.F.; Amer-Cuenca, J.J.; Zito, G.; Garzon, S.; Caruso, S.; et al. Scoring systems for the evaluation of adnexal masses nature: Current knowledge and clinical applications. J. Obstet. Gynaecol. 2021, 41, 340–347. [Google Scholar] [CrossRef]
- Moore, R.G.; Blackman, A.; Miller, M.C.; Robison, K.; DiSilvestro, P.A.; Eklund, E.E.; Strongin, R.; Messerlian, G. Multiple biomarker algorithms to predict epithelial ovarian cancer in women with a pelvic mass: Can additional makers improve performance? Gynecol. Oncol. 2019, 154, 150–155. [Google Scholar] [CrossRef]
- Ueland, F. A Perspective on Ovarian Cancer Biomarkers: Past, Present and Yet-To-Come. Diagnostics 2017, 7, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunton, C.J.; Hutchcraft, M.L.; Bullock, R.G.; Northrop, L.E.; Ueland, F.R. Salvaging detection of early-stage ovarian malignancies when ca125 is not informative. Diagnostics 2021, 11, 1440. [Google Scholar] [CrossRef]
- Coleman, R.L.; Herzog, T.J.; Chan, D.W.; Munroe, D.G.; Pappas, T.C.; Smith, A.; Zhang, Z.; Wolf, J. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am. J. Obstet. Gynecol. 2016, 215, 82-e1. [Google Scholar] [CrossRef] [Green Version]
- Han, C.; Bellone, S.; Siegel, E.R.; Altwerger, G.; Menderes, G.; Bonazzoli, E.; Egawa-Takata, T.; Pettinella, F.; Bianchi, A.; Riccio, F.; et al. A novel multiple biomarker panel for the early detection of high-grade serous ovarian carcinoma. Gynecol. Oncol. 2018, 149, 585–591. [Google Scholar] [CrossRef]
- Zhu, C.; Zhang, N.; Zhong, A.; Xiao, K.; Lu, R.; Guo, L. A combined strategy of TK1, HE4 and CA125 shows better diagnostic performance than risk of ovarian malignancy algorithm (ROMA) in ovarian carcinoma. Clin. Chim. Acta 2022, 524, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Moro, F.; Esposito, R.; Landolfo, C.; Froyman, W.; Timmerman, D.; Bourne, T.; Scambia, G.; Valentin, L.; Testa, A.C. Ultrasound evaluation of ovarian masses and assessment of the extension of ovarian malignancy. Br. J. Radiol. 2021, 94, 20201375. [Google Scholar] [CrossRef] [PubMed]
- Kaijser, J.; Bourne, T.; Valentin, L.; Sayasneh, A.; Van Holsbeke, C.; Vergote, I.; Testa, A.C.; Franchi, D.; Van Calster, B.; Timmerman, D. Improving strategies for diagnosing ovarian cancer: A summary of the International Ovarian Tumor Analysis (IOTA) studies. Ultrasound Obstet. Gynecol. 2013, 41, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Sayasneh, A.; Ferrara, L.; De Cock, B.; Saso, S.; Al-Memar, M.; Johnson, S.; Kaijser, J.; Carvalho, J.; Husicka, R.; Smith, A.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model: A multicentre external validation study. Br. J. Cancer 2016, 115, 542–548. [Google Scholar] [CrossRef] [Green Version]
- Wilailak, S.; Chan, K.K.L.; Chen, C.A.; Nam, J.H.; Ochiai, K.; Aw, T.C.; Sabaratnam, S.; Hebbar, S.; Sickan, J.; Schodin, B.A.; et al. Distinguishing benign from malignant pelvic mass utilizing an algorithm with HE4, menopausal status, and ultrasound findings. J. Gynecol. Oncol. 2015, 26, 46–53. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| N = 1071 | |||
|---|---|---|---|
| Age (mean ± SD) | 47.72 ± 16.22 | ||
| Menopausal status | |||
| Premenopausal | 629 (58.73%) | ||
| Postmenopausal | 442 (41.27%) | ||
| Pathology | |||
| Benign | 778 (72.64%) | ||
| Epithelial tumor | 331 (42.5%) | ||
| Endometrioma | 210 (26.9%) | ||
| Fibroids | 56 (7.2%) | ||
| Other sex cord-stromal tumors | 4 (0.5%) | ||
| Germ cell tumors | 149 (19.2%) | ||
| Fallopian tube lesions | 24 (3.1%) | ||
| Tubo-ovaric abscesses | 4 (0.5%) | ||
| Epithelial borderline | 74 (6.91%) | ||
| Epithelial ovarian cancer (EOC) | 197 (18.39%) | FIGO stage for EOC | |
| Serous carcinoma | 124 (62.94%) | FIGO Stage I | 58 (29.44%) |
| Mucinous carcinoma | 8 (4.06%) | FIGO Stage II | 15 (7.61%) |
| Clear cell carcinoma | 17 (8.63%) | FIGO Stage III | 108 (54.82%) |
| Endometrioid Carcinoma | 33 (16.75%) | FIGO Stage IV | 16 (8.12%) |
| Undifferenciated Carcinoma | 15 (7.61%) | ||
| Metastatic cancer in the ovary | 22 (2.05%) | ||
| All Patients | Inconclusive Diagnosis * | Premenopausal | Postmenopausal | Stage I EOC | |
|---|---|---|---|---|---|
| CA125 | 0.873 (0.842–0.904) | 0.810 (0.743–0.877) | 0.759 (0.675–0.842) | 0.933 (0.907–0.959) | 0.810 (0.751–0.869) |
| HE4 | 0.909 (0.881–0.938) | 0.844 (0.779–0.910) | 0.863 (0.791–0.934) | 0.905 (0.870–0.940) | 0.856 (0.793–0.8869) |
| ROMA | 0.939 (0.916–0.962) | 0.893 (0.846–0.941) | 0.866 (0.796–0.937) | 0.956 (0.937–0.975) | 0.909 (0.863–0.955) |
| CPH | 0.936 (0.913–0.958) | 0.876 (0.822–0.931) | 0.860 (0.793–0.928) | 0.955 (0.935–0.975) | 0.901 (0.855–0.947) |
| Parameter | Cutoff | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|
| CA125 | 100 U/mL | 61.86 (55.21–68.09) | 92.71 (90.73–94.29) | 68.91 (62.07–75.02) | 90.30 (88.11–92.11) |
| 35/65 U/mL * | 74.42 (68.23–79.81) | 80.70 (77.81–83.24) | 50.21 (44.73–55.64) | 92.30 (90.22–94.12) | |
| 35/100 U/mL * | 66.98 (60.44–72.92) | 81.39 (78.58–83.90) | 48.48 (42.86–54.15) | 90.41 (88.07–92.32) | |
| HE4 | 70 pmol/L | 83.25 (77.31–87.88) | 86.11 (83.40–88.43) | 61.15 (55.11–66.87) | 95.14 (93.22–96.53) |
| 120 pmol/L | 69.11 (62.23–75.23) | 96.29 (94.65–97.44) | 83.02 (76.42–88.06) | 92.23 (90.10–93.93) | |
| 70/140 pmol/L * | 70.70 (63.93–76.71) | 93.5 (91.52–95.11) | 74.2 (67.40–80.01) | 92.40 (90.20–94.10) | |
| ROMA | 10% | 94.24 (89.98–96.75) | 72.71 (69.27–75.91) | 47.91 (43.84–54.01) | 97.85 (96.19–98.80) |
| 15% | 91.10 (86.21–94.37) | 84.62 (81.73–87.12) | 62.14 (56.33–67.62) | 97.17 (95.51–98.22) | |
| 12.5/14.4% * | 91.62 (86.83–94.78) | 82.58 (79.57–85.23) | 59.32 (53.63–64.77) | 97.26 (95.60–98.31) | |
| 13.1/27.7% * | 84.80 (79.00–89.20) | 89.0 (86.40–91.10) | 68.10 (61.90–73.70) | 95.50 (93.60–96.80) | |
| CPH | 1% | 96.86 (93.32–98.55) | 47.97 (44.26–51.70) | 34.01 (30.15–38.09) | 98.22 (96.17–99.18) |
| 3% | 91.10 (86.22–94.42) | 79.12 (75.91–82.01) | 54.72 (49.23–60.14) | 97.01 (95.21–98.12) | |
| 5% | 86.91 (81.39–90.97) | 87.54 (84.86–89.79) | 65.87 (59.82–71.45) | 96.03 (94.20–97.29) | |
| 7% | 82.20 (76.16–86.97) | 90.87 (88.49–92.80) | 71.36 (65.06–76.93) | 94.86 (92.90–96.309) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreras-Dieguez, N.; Glickman, A.; Munmany, M.; Casanovas, G.; Agustí, N.; Díaz-Feijoo, B.; Saco, A.; Sánchez, B.; Gaba, L.; Angeles, M.A.; et al. Comparison of HE4, CA125, ROMA and CPH-I for Preoperative Assessment of Adnexal Tumors. Diagnostics 2022, 12, 226. https://doi.org/10.3390/diagnostics12010226
Carreras-Dieguez N, Glickman A, Munmany M, Casanovas G, Agustí N, Díaz-Feijoo B, Saco A, Sánchez B, Gaba L, Angeles MA, et al. Comparison of HE4, CA125, ROMA and CPH-I for Preoperative Assessment of Adnexal Tumors. Diagnostics. 2022; 12(1):226. https://doi.org/10.3390/diagnostics12010226
Chicago/Turabian StyleCarreras-Dieguez, Núria, Ariel Glickman, Meritxell Munmany, Georgina Casanovas, Núria Agustí, Berta Díaz-Feijoo, Adela Saco, Beatriz Sánchez, Lydia Gaba, Martina Aida Angeles, and et al. 2022. "Comparison of HE4, CA125, ROMA and CPH-I for Preoperative Assessment of Adnexal Tumors" Diagnostics 12, no. 1: 226. https://doi.org/10.3390/diagnostics12010226