
Traumatic Intralenticular Neovascularization in a HLA B27+ Pediatric Patient

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Case Presentation
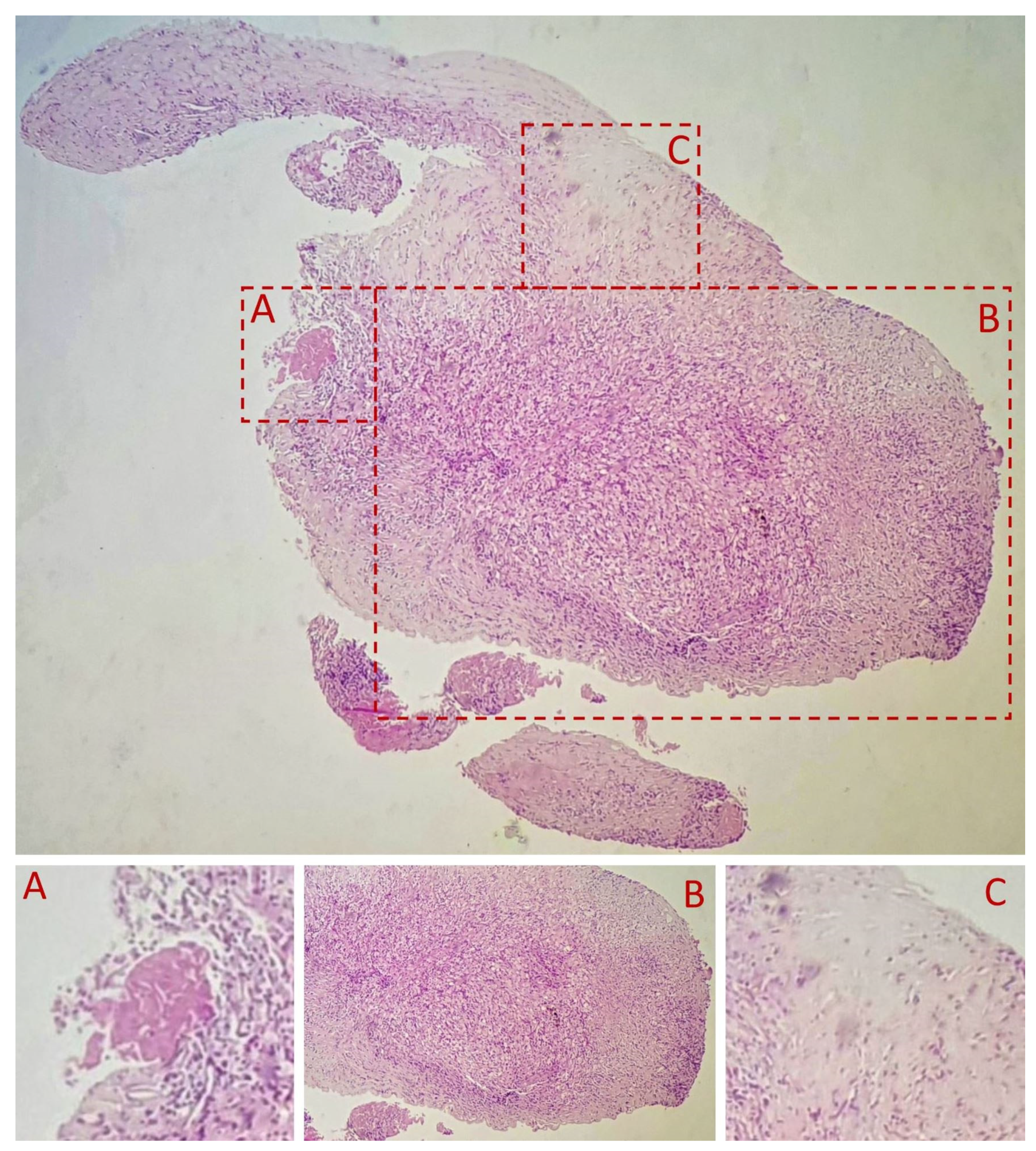
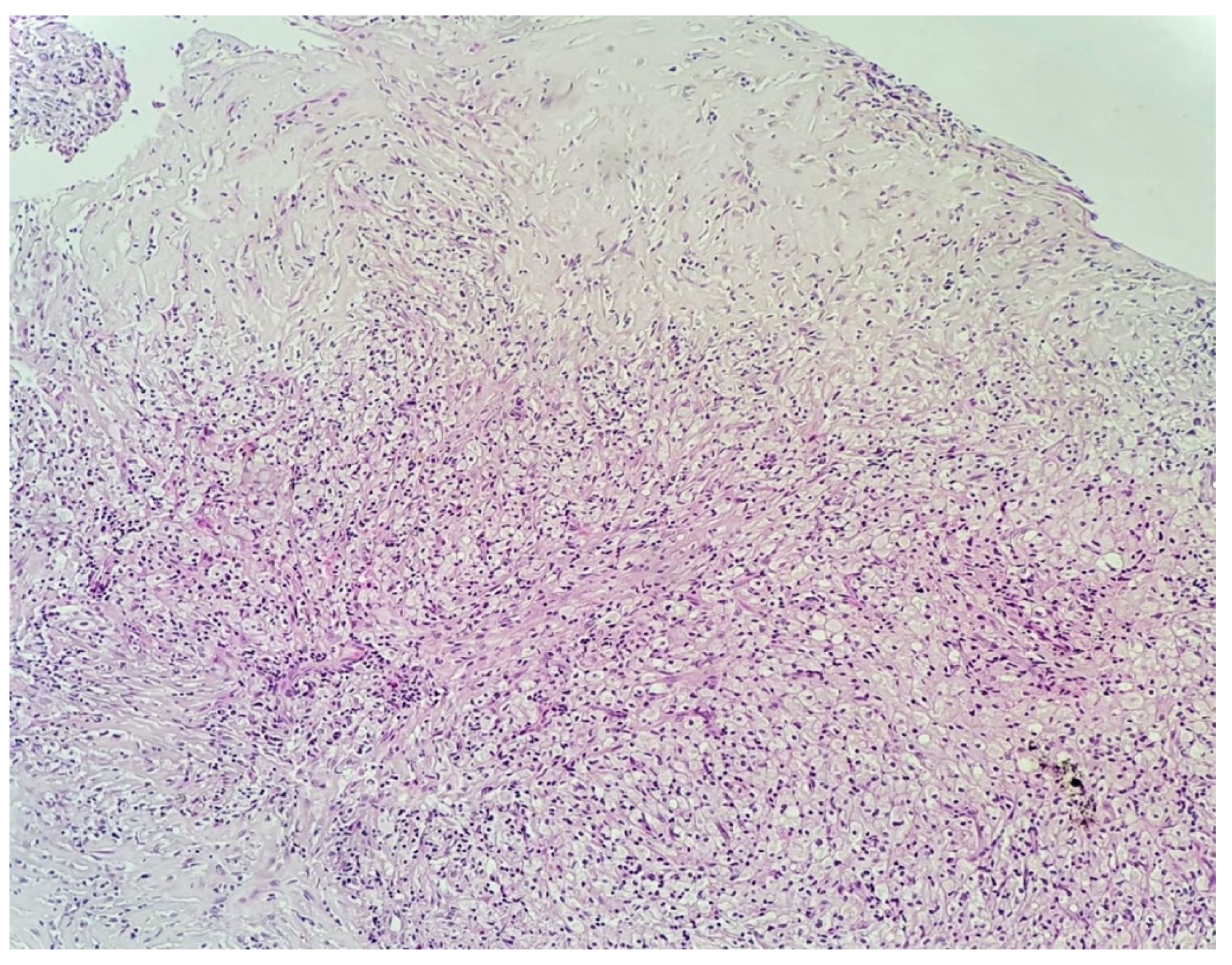
3.2. Histopathological Examination of the Specimen
4. Discussion
5. Conclusions
5.1. What Was Known
5.2. What This Paper Adds
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PFV | Persistent fetal vasculature |
| TVL | Tunica vasculosa lentis |
| IOL | Intraocular lens |
| BCVA | Best corrected visual acuity |
| HE | Hematoxylin and eosin stain |
| CD68 | Microsialine |
| HLA B27 | Human leukocyte antigen |
| ANA+ anterior uveitis | Antinuclear antibodies positive anterior uveitis |
| JIA | Juvenile idiopathic arthritis |
| TAM | Tissue activated macrophages |
| VEGF | Vascular endothelial growth factor |
| IFNγ | Interferon-gamma |
| AS | Ankylosing spondylitis |
| ICMJE | International Committee of Medical Journal Editors |
References
- Albert, D.M.; Phelps, P.O.; Surapaneni, K.R.; Thuro, B.A.; Potter, H.A.; Ikeda, A.; Teixeira, L.B.; Dubielzig, R.R. The Significance of the Discordant Occurrence of Lens Tumors in Humans versus Other Species. Ophthalmology 2015, 122, 1765–1770. [Google Scholar] [CrossRef] [Green Version]
- Zeiss, C.J.; Johnson, E.M.; Dubielzig, R.R. Feline Intraocular Tumors May Arise from Transformation of Lens Epithelium. Vet. Pathol. 2003, 40, 355–362. [Google Scholar] [CrossRef]
- Veromann, S. Eye Lens Tumors: An Experimental-Histological and Theoretical Approach–Tumor Biol; Institute of General and Molecular Pathology, Tartu University: Tartu, Estonia, 1994; Volume 15, pp. 135–140. [Google Scholar]
- David, J. Wineland. Nobel Lecture: Superposition, entanglement, and raising Schrödinger’s cat. Rev. Mod. Phys. 2013, 85, 1103–1114. [Google Scholar] [CrossRef]
- Guffey Johnson, J.; Margo, C.E. Intraocular Inflammatory Mass Associated with Lens-Induce Uveitis. Surv. Ophthalmol. 2017, 62, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.K.; Chou, L.; Shields, C.L. Cutaneous Melanoma Metastatic to Anterior Lens Capsule. JAMA Ophthalmol. March 2018, 136, e180095. [Google Scholar] [CrossRef] [PubMed]
- Miesfeld, J.B.; Brown, N.L. Chapter Ten—Eye organogenesis: A hierarchical view of ocular development. In Current Topics in Developmental Biology; Wellik, D.M., Ed.; Academic Press: Cambridge, MA, USA, 2019; Volume 132, pp. 351–393. ISSN 0070-2153. ISBN 9780128104897. Available online: https://www.sciencedirect.com/science/article/pii/S007021531830108X (accessed on 6 May 2021). [CrossRef]
- Chen, C.; Xiao, H.; Ding, X. Persistent Fetal Vasculature. Asia Pac. J. Ophthalmol. 2018, 8, 86–95. [Google Scholar] [CrossRef]
- Cloquet, J. Mémoire sur la membrane pupillaire, et sur la formation du petit cercle artérial de l’iris. Trans. Am. Ophthalmol. Soc. 2003, 101, 59–64, discussion, 64–65. [Google Scholar]
- Hwang, Y.S.; Lai, C.C.; Lee, J.S.; Yang, K.J.; Chen, T.L. Posttraumatic neovascularization in a cataractous crystalline lens. J. Cataract. Refract. Surg. 2002, 28, 715–716. [Google Scholar] [CrossRef]
- Casey, R.; Li, W.W. Factors controlling ocular angiogenesis. Am. J. Ophthalmol. 1997, 124, 521–529. [Google Scholar] [CrossRef]
- Gupta, S.; Gogia, V.; Roshan, T.; Sen, S.; Venkatesh, P. Posterior lens capsular neovascularization of young: Management using endodiathermy assisted biopsy. Can. J. Ophthalmol. 2015, 50, e4–e7. [Google Scholar] [CrossRef] [PubMed]
- Kabat, A.G. Lenticular neovascularization subsequent to traumatic cataract formation. Optom. Vis. Sci. 2011, 88, 1127–1132. [Google Scholar] [CrossRef]
- Patyal, S.; Kakkar, S.; Gurunadh, V.S.; Pradeep, P.G. Post traumatic neovascularisation of a cataractous crystalline lens. Med. J. Armed Forces India 2015, 71, S290–S292. [Google Scholar] [CrossRef] [Green Version]
- Grange, L.K.; Kouchouk, A.; Dalal, M.D.; Vitale, S.; Nussenblatt, R.B.; Chan, C.C.; Sen, H.N. Neoplastic masquerade syndromes in patients with uveitis. Am. J. Ophthalmol. 2014, 157, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Chistiakov, D.A.; Killingsworth, M.C.; Myasoedova, V.A.; Orekhov, A.N.; Bobryshev, Y.V. CD68/macrosialin: Not just a histochemical marker. Nat. Lab. Investig. 2017, 97, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.; Guo, C.; Fisher, P.B.; Subjeck, J.R.; Wang, X.-Y. Chapter Nine—Scavenger Receptors: Emerging Roles in Cancer Biology and Immunology; Advances in Cancer Research; Wang, X.-Y., Fisher, P.B., Eds.; Academic Press: Cambridge, MA, USA, 2015; Volume 128, pp. 309–364. ISSN 0065-230X. ISBN 9780128023167. Available online: https://www.sciencedirect.com/science/article/pii/S0065230x15000329 (accessed on 6 May 2021). [CrossRef] [Green Version]
- Ranty, M.-L.; Laurent, C.; Aziza, J.; Mahieu, L.; Olle, P.; Quintyn, J.-C.; Garnier, L.; Bienvenu, J.; Collin, L.; Delisle, M.-B.; et al. Improving the cytological diagnosis of intraocular lymphoma from vitreous fluid. Histopathology 2015, 67, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Filipe, J.C.; Palmares, J.; Delgado, L.; Lopes, J.M.; Borges, J.; Castro-Correia, J. Phacolytic glaucoma and lens-induced uveitis. Int. Ophthalmol. 1993, 17, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Ly, L.V.; Bronkhorst, I.H.; van Beelen, E.; Vrolijk, J.; Taylor, A.W.; Versluis, M.; Luyten, G.P.; Jager, M.J. Inflammatory Cytokines in Eyes with Uveal Melanoma and Relation with Macrophage Infiltration. Invest. Ophthalmol. Vis. Sci. 2010, 51, 5445–5451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalinina Ayuso, V.; van Dijk, M.R.; de Boer, J.H. Infiltration of Plasma Cells in the Iris of Children With ANA-Positive Anterior Uveitis. Invest. Ophthalmol. Vis. Sci. 2015, 56, 6770–6778. [Google Scholar] [CrossRef] [Green Version]
- Zipplies, J.K.; Kirschfink, M.; Amann, B.; Hauck, S.M.; Stangassinger, M.; Deeg, C.A. Deeg, Complement factor B expression profile in a spontaneous uveitis model. Immunobiology 2010, 215, 949–955. Available online: https://www.sciencedirect.com/science/article/pii/S0171298510000148 (accessed on 3 May 2021). [CrossRef]
- Barros, M.H.; Hauck, F.; Dreyer, J.H.; Kempkes, B.; Niedobitek, G. Macrophage polarisation: An immunohistochemical approach for identifying M1 and M2 macrophages. PLoS ONE 2013, 8, e80908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco, O.; Yanal, G.; Bala, P.A.; Klaus, L. Macrophage Polarization: Different Gene Signatures in M1(LPS+) vs. Classically and M2(LPS–) vs. Alternatively Activated Macrophages. Front. Immunol. 2019, 10, 1084. Available online: https://www.frontiersin.org/article/10.3389/fimmu.2019.01084 (accessed on 3 May 2021). [CrossRef]
- Khan, M.A. Race-related differences in HLA association with ankylosing spondylitis and Reiter’s disease in American blacks and whites. J. Natl. Med. Assoc. 1978, 70, 41–42. [Google Scholar] [PubMed]
- Tikly, M.; Njobvu, P.; McGill, P. Spondyloarthritis in Sub-Saharan Africa. Curr. Rheumatol. Rep. 2014, 16, 421. [Google Scholar] [CrossRef]
- Angeles-Han, S.T.; McCracken, C.; Yeh, S.; Jenkins, K.; Stryker, D.; Travers, C.; Rouster-Stevens, K.; Vogler, L.B.; Lambert, S.R.; Drews-Botsch, C.; et al. The Association of Race with Childhood Uveitis. Am. J. Ophthalmol. 2015, 160, 919–928.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.K.; Magrey, M.N. Racial Differences in Clinical Features and Comorbidities in Ankylosing Spondylitis in the United States. J. Rheumatol. 2020, 47, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Jamalyaria, F.; Ward, M.M.; Assassi, S.; Learch, T.J.; Lee, M.; Gensler, L.S.; Brown, M.A.; Diekman, L.; Tahanan, A.; Rahbar, M.H.; et al. Ethnicity and disease severity in ankylosing spondylitis a cross-sectional analysis of three ethnic groups. Clin. Rheumatol. 2017, 36, 2359–2364. [Google Scholar] [CrossRef]
- Shaikh, M.; Hynes, A.; Raiji, V. Patients with HLA-B27 related anterior uveitis; Racial Differences in HLA-B27 Associated Anterior Uveitis. Invest. Ophthalmol. Vis. Sci. 2014, 55, 5314. [Google Scholar]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tătaru, C.P.; Tătaru, C.I.; Dudău, M.; Moșu, A.; Luca, L.; Maria, B.; Bancu, A.; Curcă, P.F. Traumatic Intralenticular Neovascularization in a HLA B27+ Pediatric Patient. Diagnostics 2021, 11, 1493. https://doi.org/10.3390/diagnostics11081493
Tătaru CP, Tătaru CI, Dudău M, Moșu A, Luca L, Maria B, Bancu A, Curcă PF. Traumatic Intralenticular Neovascularization in a HLA B27+ Pediatric Patient. Diagnostics. 2021; 11(8):1493. https://doi.org/10.3390/diagnostics11081493
Chicago/Turabian StyleTătaru, Călin Petru, Cătălina Ioana Tătaru, Maria Dudău, Alexandra Moșu, Lăcrămioara Luca, Bosa Maria, Alice Bancu, and Paul Filip Curcă. 2021. "Traumatic Intralenticular Neovascularization in a HLA B27+ Pediatric Patient" Diagnostics 11, no. 8: 1493. https://doi.org/10.3390/diagnostics11081493