
Complex Component of Oncocytic and Non-Oncocytic Lipoadenomas in the Parotid Gland: A Case Report

Abstract
:1. Introduction
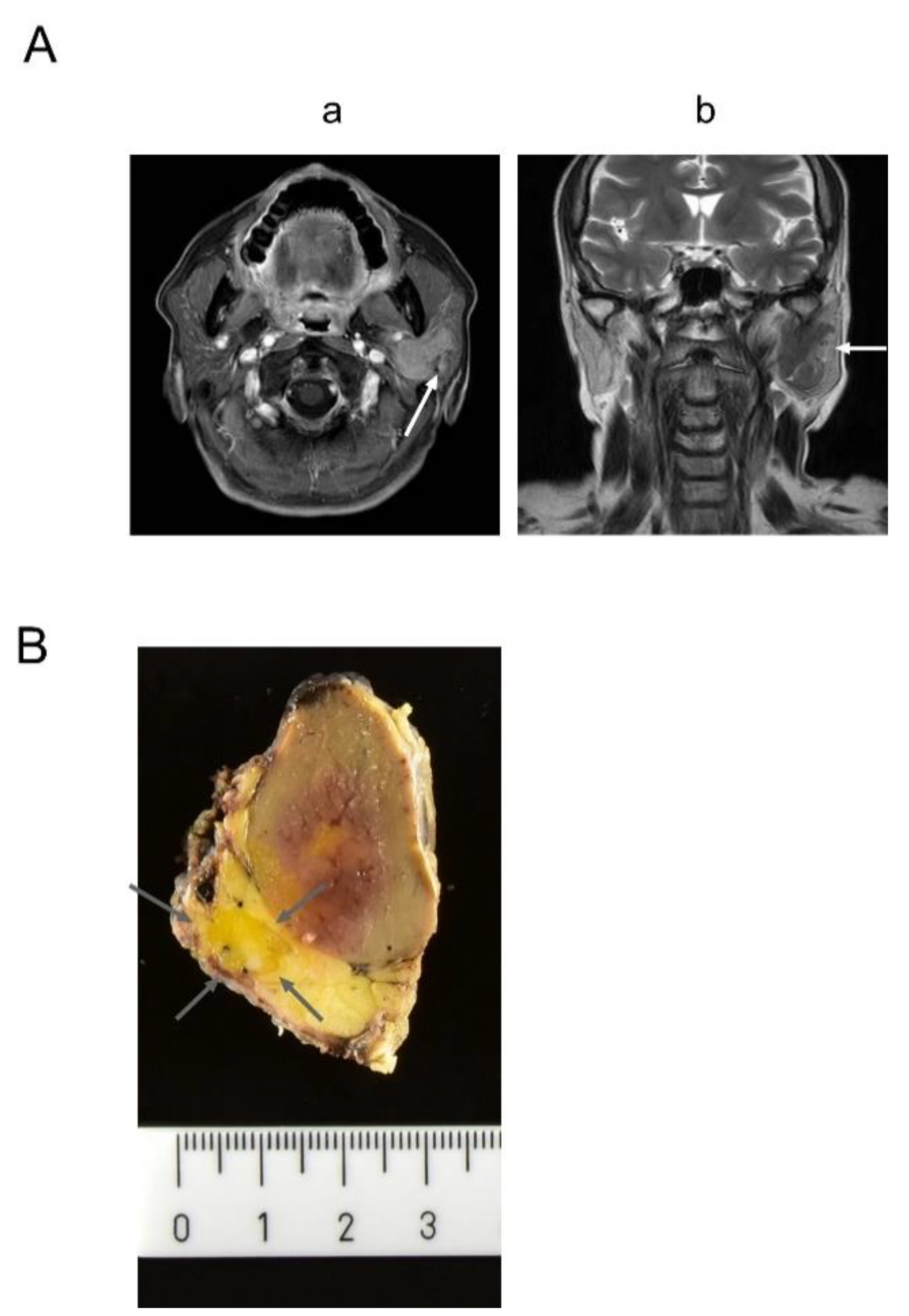
2. Clinical Summary
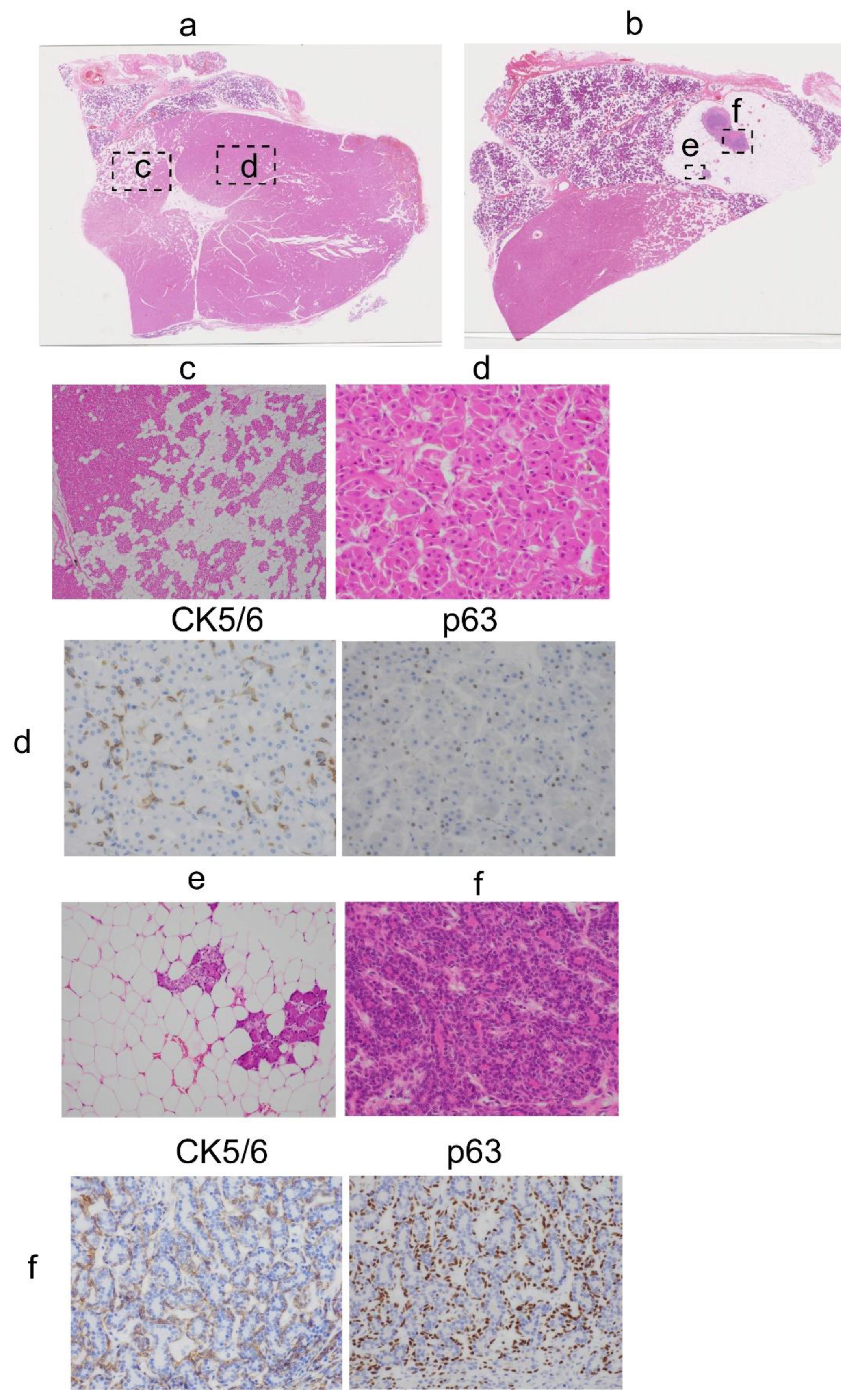
3. Pathological Findings
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Hirokawa, M.; Shimizu, M.; Manabe, T.; Ito, J.; Ogawa, S. Oncocytic lipoadenoma of the submandibular gland. Hum. Pathol. 1998, 29, 410–412. [Google Scholar] [CrossRef]
- Lau, S.K.; Thompson, L.D. Oncocytic lipoadenoma of the salivary gland: A clinicopathologic analysis of 7 cases and review of the literature. Head Neck Pathol. 2015, 9, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, M.; Hofman, V.; Pedeutour, F.; Attias, R.; Santini, J.; Hofman, P. Oncocytic lipoadenoma of the parotid gland: Immunohistochemical and cytogenetic analysis. Pathol. Res. Pr. 2010, 206, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Mitsimponas, K.T.; Agaimy, A.; Schlittenbauer, T.; Nkenke, E.; Neukam, F.W. Oncocytic lipoadenoma of the parotid gland: A report of a new case and review of the literature. Int J. Clin. Exp. Pathol. 2012, 5, 1000–1006. [Google Scholar] [PubMed]
- Murshed, K.A.; Khalafalla, A.; Alani, B.; Farghaly, H.; Alkhalil, M. A case of oncocytic lipoadenoma of the submandibular gland and its diagnostic cytology challenges. Diagn. Cytopathol. 2020, 48, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.L.; Kuo, T.T.; Lee, L.Y. Oncocytic lipoadenoma: A rare case of parotid gland tumor and review of the literature. J. Pathol. Transl. Med. 2015, 49, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Ihrler, S.; Märkl, B.; Lell, M.; Zenk, J.; Hartmann, A.; Michal, M.; Skalova, A. Lipomatous salivary gland tumors: A series of 31 cases spanning their morphologic spectrum with emphasis on sialolipoma and oncocytic lipoadenoma. Am. J. Surg. Pathol. 2013, 37, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Nagao, T.; Sugano, I.; Ishida, Y.; Asoh, A.; Munakata, S.; Yamazaki, K.; Konno, A.; Kondo, Y.; Nagao, K. Sialolipoma: A report of seven cases of a new variant of salivary gland lipoma. Histopathology 2001, 38, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Horie, Y. Oncocytic lipoadenoma of the parotid gland. Histopathology 2000, 36, 285–286. [Google Scholar] [CrossRef] [PubMed]
- Klieb, H.B.; Perez-Ordoñez, B. Oncocytic lipoadenoma of the parotid gland with sebaceous differentiation. Study of its keratin profile. Virchows Arch. 2006, 449, 722–725. [Google Scholar] [CrossRef] [PubMed]
- Khurram, S.A.; Speight, P.M. Characterisation of DOG-1 Expression in Salivary Gland Tumours and Comparison with Myoepithelial Markers. Head Neck Pathol. 2019, 13, 140–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chênevert, J.; Duvvuri, U.; Chiosea, S.; Dacic, S.; Cieply, K.; Kim, J.; Shiwarski, D.; Seethala, R.R. DOG1: A novel marker of salivary acinar and intercalated duct differentiation. Mod. Pathol. 2012, 25, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Ahn, C.; DeSantis, E.; McCalmont, T. Oncocytic Metaplasia in Melanocytic Tumors. Am. J. Derm. 2018, 40, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Jo, V.Y.; Fletcher, C.D. Myoepithelial neoplasms of soft tissue: An updated review of the clinicopathologic, immunophenotypic, and genetic features. Head Neck Pathol. 2015, 9, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tasoulas, J.; Tsouroufls, G.; Klijanienko, J.; Theocharis, S. Polymorphous adenocarcinoma: An overview of immunohistochemical features and insights on molecular pathology. Histol. Histopathol. 2019, 34, 731–744. [Google Scholar] [PubMed]
- Maiorano, E.; Capodiferro, S.; Fanelli, B.; Calabrese, L.; Napoli, A.; Favia, G. Hamartomatous angiolipoma of the parotid gland (sialoangiolipoma). Head Neck Pathol. 2008, 2, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Antibody | CK5/6 | p63 | ASMA | DOG1 | S100 |
|---|---|---|---|---|---|
| Source | DAKO (M7237) | DAKO (M7317) | DAKO (M0851) | Nichirei (418041) | DAKO (IR504) |
| PA dilution | 1:400 | 1:300 | 1:100 | 1:2 | Ready to use |
| Autostainer | Leica (BOND-III) | Leica (BOND-III) | Leica (BOND-III) | Nichirei (Histostainer) | Leica (BOND-III) |
| Antigen retrieval | ER1 (30 min) | ER2 (20 min) | CB (10 min) | ER2 (10 min) | No antigen retrieval |
| Lesion | Oncocytic | Non-oncocytic | |
|---|---|---|---|
| Antibody | |||
| CK5/6 | Positive | Positive | |
| p63 | Positive | Positive | |
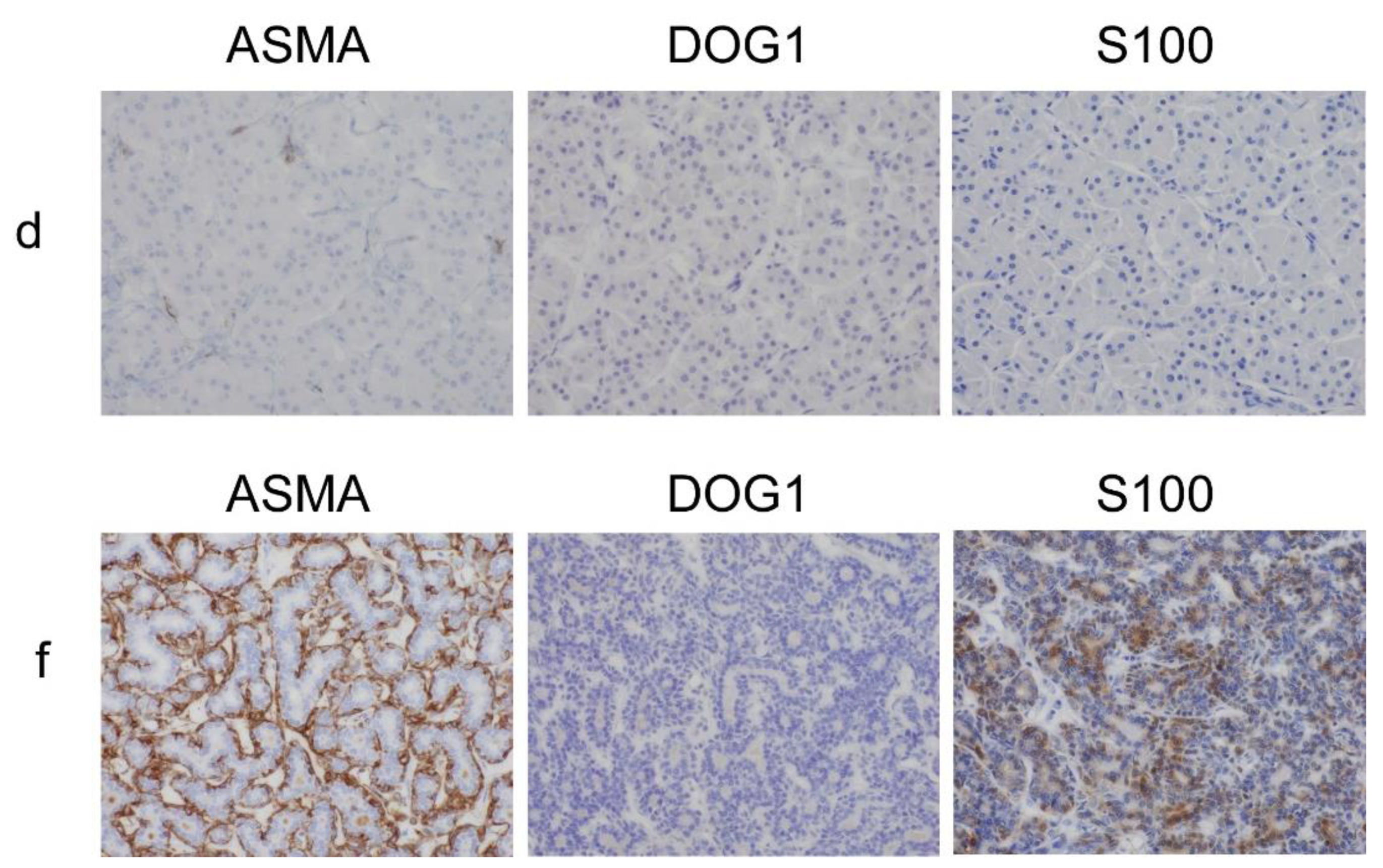
| ASMA | Negative | Positive | |
| DOG1 | Negative | Negative | |
| S100 | Negative | Positive | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, F.; Nakajima, T.; Sugino, T. Complex Component of Oncocytic and Non-Oncocytic Lipoadenomas in the Parotid Gland: A Case Report. Diagnostics 2021, 11, 1478. https://doi.org/10.3390/diagnostics11081478
Sato F, Nakajima T, Sugino T. Complex Component of Oncocytic and Non-Oncocytic Lipoadenomas in the Parotid Gland: A Case Report. Diagnostics. 2021; 11(8):1478. https://doi.org/10.3390/diagnostics11081478
Chicago/Turabian StyleSato, Fuyuki, Takashi Nakajima, and Takashi Sugino. 2021. "Complex Component of Oncocytic and Non-Oncocytic Lipoadenomas in the Parotid Gland: A Case Report" Diagnostics 11, no. 8: 1478. https://doi.org/10.3390/diagnostics11081478