
iPMI: Machine Learning-Aided Identification of Parametrial Invasion in Women with Early-Stage Cervical Cancer

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Outcome
2.3. Conventional Statistical Analysis
2.4. Predictive Models
2.4.1. Synthetic Minority Oversampling Technique
2.4.2. Development of Preoperative Computational Models
2.4.3. SHAP Analysis
2.4.4. Models’ Performance Evaluation
3. Results
3.1. Patients’ Characteristics
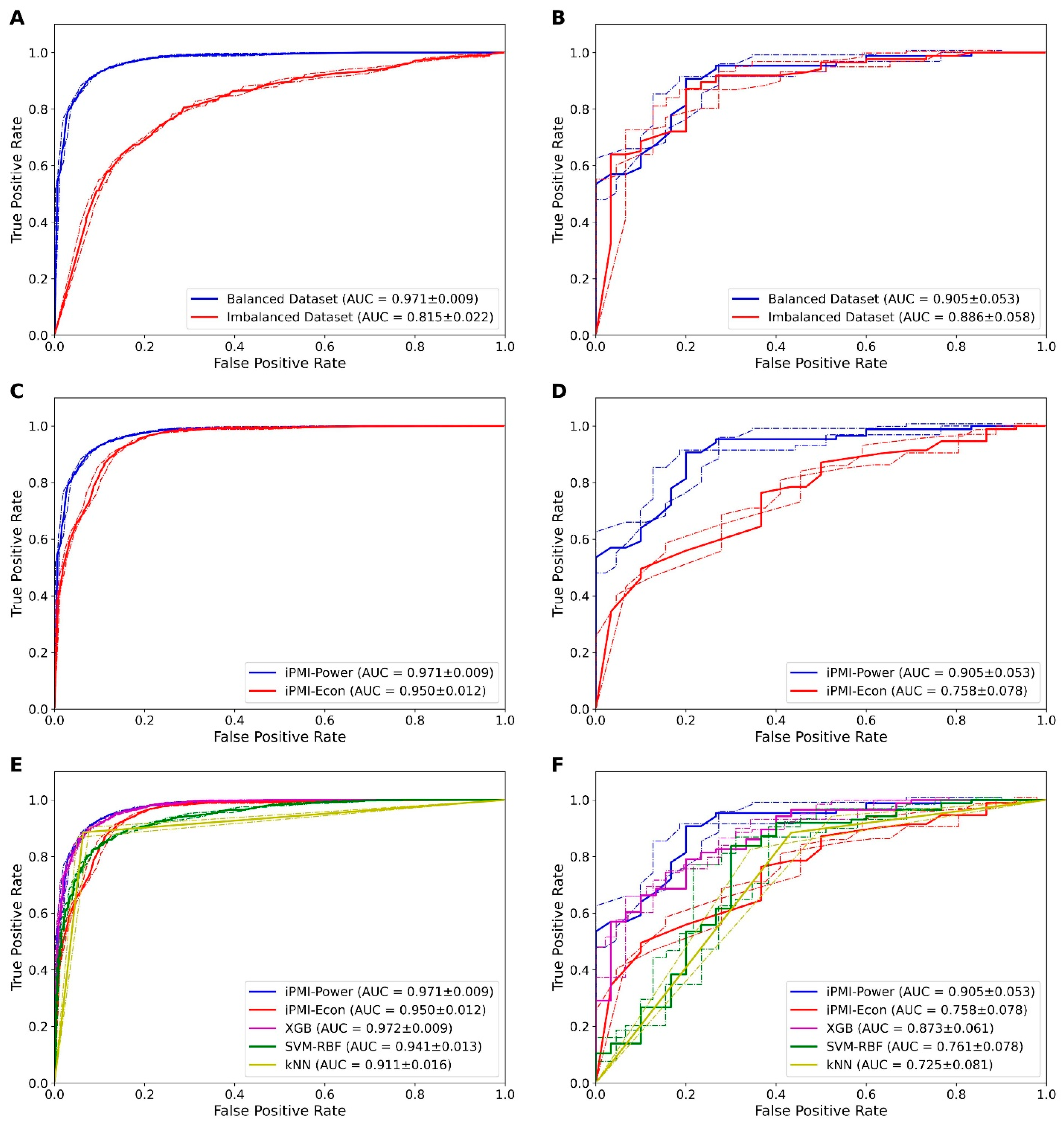
3.2. Effect of Balanced and Imbalanced Datasets
3.3. Performance of Preoperative and Postoperative Clinicopathological Factors
3.4. Comparison of iPMI with Other ML Classifiers
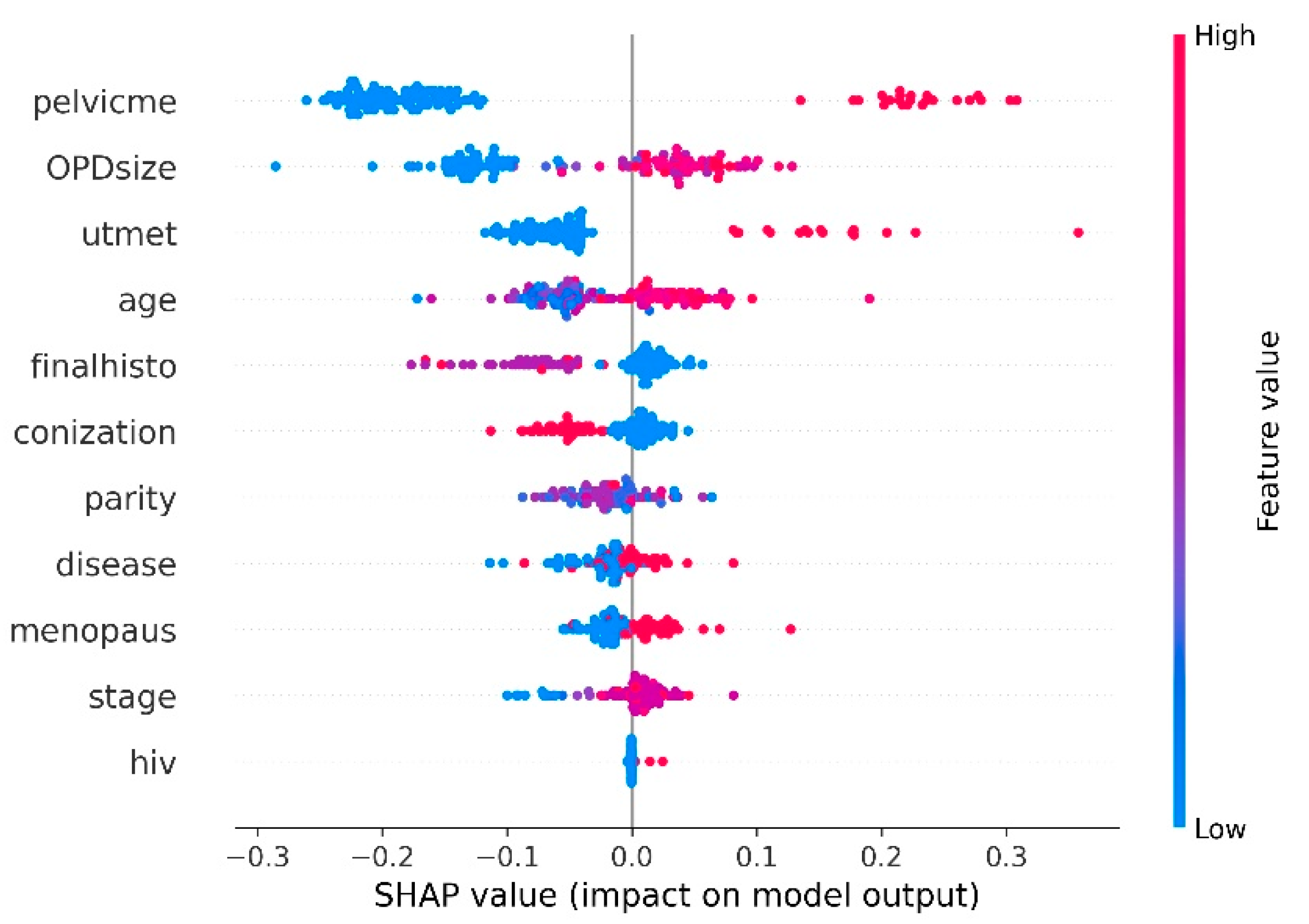
3.5. Analysis of Informative Clinicopathological Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GLOBOCAN. International Agency for Research on Cancer. 2018. Available online: http://gco.iarc.fr/ (accessed on 6 September 2020).
- Diepenbruck, M.; Christofori, G. Epithelial-mesenchymal transition (EMT) and metastasis: Yes, no, maybe? Curr. Opin. Cell Biol. 2016, 43, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Okumura, M. Prognostic significance of parametrial extension in patients with cervical carcinoma Stages IB, IIA, and IIB. A study of 628 cases treated by radical hysterectomy and lymphadenectomy with or without postoperative irradiation. Cancer 1984, 54, 1714–1719. [Google Scholar] [CrossRef]
- Delgado, G.; Bundy, B.; Zaino, R.; Sevin, B.U.; Creasman, W.T.; Major, F. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A gynecologic oncology group study. Gynecol. Oncol. 1990, 38, 352–357. [Google Scholar] [CrossRef]
- Wright, J.D.; Grigsby, P.W.; Brooks, R.; Powell, M.A.; Gibb, R.K.; Gao, F.; Rader, J.S.; Mutch, D.G. Utility of parametrectomy for early stage cervical cancer treated with radical hysterectomy. Cancer 2007, 110, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Querleu, D.; Cibula, D.; Abu-Rustum, N.R. 2017 Update on the querleu-morrow classification of radical hysterectomy. Ann. Surg. Oncol. 2017, 24, 3406–3412. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.A.; Benedet, J.L.; Odicino, F.; Maisonneuve, P.; Beller, U.; Creasman, W.T.; Heintz, A.P.; Ngan, H.Y.; Pecorelli, S. Carcinoma of the cervix uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2006, 95 (Suppl 1), S43–S103. [Google Scholar] [CrossRef]
- Zullo, M.A.; Manci, N.; Angioli, R.; Muzii, L.; Panici, P.B. Vesical dysfunctions after radical hysterectomy for cervical cancer: A critical review. Crit. Rev. Oncol. Hematol. 2003, 48, 287–293. [Google Scholar] [CrossRef]
- Charoenkwan, K.; Pranpanas, S. Prevalence and characteristics of late postoperative voiding dysfunction in early-stage cervical cancer patients treated with radical hysterectomy. Asian Pac. J. Cancer Prev. 2007, 8, 387–389. [Google Scholar] [PubMed]
- Barnes, W.; Waggoner, S.; Delgado, G.; Maher, K.; Potkul, R.; Barter, J.; Benjamin, S. Manometric characterization of rectal dysfunction following radical hysterectomy. Gynecol. Oncol. 1991, 42, 116–119. [Google Scholar] [CrossRef]
- Jongpipan, J.; Charoenkwan, K. Sexual function after radical hysterectomy for early-stage cervical cancer. J. Sex. Med. 2007, 4, 1659–1665. [Google Scholar] [CrossRef]
- Carter, J.; Sonoda, Y.; Baser, R.E.; Raviv, L.; Chi, D.S.; Barakat, R.R.; Iasonos, A.; Brown, C.L.; Abu-Rustum, N.R. A 2-year prospective study assessing the emotional, sexual, and quality of life concerns of women undergoing radical trachelectomy versus radical hysterectomy for treatment of early-stage cervical cancer. Gynecol. Oncol. 2010, 119, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Pieterse, Q.D.; Maas, C.P.; ter Kuile, M.M.; Lowik, M.; van Eijkeren, M.A.; Trimbos, J.B.; Kenter, G.G. An observational longitudinal study to evaluate miction, defecation, and sexual function after radical hysterectomy with pelvic lymphadenectomy for early-stage cervical cancer. Int. J. Gynecol. Cancer 2006, 16, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Takashima, A.; Kasamatsu, T.; Nakamura, K.; Mizusawa, J.; Nakanishi, T.; Takeshima, N.; Kamiura, S.; Onda, T.; Sumi, T.; et al. Clinical tumor diameter and prognosis of patients with FIGO stage IB1 cervical cancer (JCOG0806-A). Gynecol. Oncol. 2015, 137, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Velechovska, P.; Slama, J.; Fischerova, D.; Pinkavova, I.; Pavlista, D.; Dundr, P.; Hill, M.; Freitag, P.; Zikan, M. Late morbidity following nerve-sparing radical hysterectomy. Gynecol. Oncol. 2010, 116, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Peters, W.A., 3rd; Liu, P.Y.; Barrett, R.J., 2nd; Stock, R.J.; Monk, B.J.; Berek, J.S.; Souhami, L.; Grigsby, P.; Gordon, W., Jr.; Alberts, D.S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2000, 18, 1606–1613. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Cervical Cancer (Version 1.2021). Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 5 December 2020).
- Kamimori, T.; Sakamoto, K.; Fujiwara, K.; Umayahara, K.; Sugiyama, Y.; Utsugi, K.; Takeshima, N.; Tanaka, H.; Gomi, N.; Takizawa, K. Parametrial involvement in FIGO stage IB1 cervical carcinoma diagnostic impact of tumor diameter in preoperative magnetic resonance imaging. Int. J. Gynecol. Cancer 2011, 21, 349–354. [Google Scholar] [CrossRef]
- Landoni, F.; Bocciolone, L.; Perego, P.; Maneo, A.; Bratina, G.; Mangioni, C. Cancer of the cervix, FIGO stages IB and IIA: Patterns of local growth and paracervical extension. Int. J. Gynecol. Cancer 1995, 5, 329–334. [Google Scholar] [CrossRef]
- Tseng, Y.J.; Huang, C.E.; Wen, C.N.; Lai, P.Y.; Wu, M.H.; Sun, Y.C.; Wang, H.Y.; Lu, J.J. Predicting breast cancer metastasis by using serum biomarkers and clinicopathological data with machine learning technologies. Int. J. Med. Inform. 2019, 128, 79–86. [Google Scholar] [CrossRef]
- Tseng, Y.J.; Wang, H.Y.; Lin, T.W.; Lu, J.J.; Hsieh, C.H.; Liao, C.T. Development of a machine learning model for survival risk stratification of patients with advanced oral cancer. JAMA Netw. Open 2020, 3, e2011768. [Google Scholar] [CrossRef]
- Yu, K.-H.; Zhang, C.; Berry, G.J.; Altman, R.B.; Ré, C.; Rubin, D.L.; Snyder, M. Predicting non-small cell lung cancer prognosis by fully automated microscopic pathology image features. Nat. Commun. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Alghamdi, M.; Al-Mallah, M.; Keteyian, S.; Brawner, C.; Ehrman, J.; Sakr, S. Predicting diabetes mellitus using SMOTE and ensemble machine learning approach: The Henry Ford ExercIse Testing (FIT) project. PLoS ONE 2017, 12, e0179805. [Google Scholar] [CrossRef] [PubMed]
- Charoenkwan, P.; Nantasenamat, C.; Hasan, M.M.; Shoombuatong, W. iTTCA-Hybrid: Improved and robust identification of tumor T cell antigens by utilizing hybrid feature representation. Anal. Biochem. 2020, 599, 113747. [Google Scholar] [CrossRef] [PubMed]
- Schaduangrat, N.; Nantasenamat, C.; Prachayasittikul, V.; Shoombuatong, W. ACPred: A computational tool for the prediction and analysis of anticancer peptides. Molecules 2019, 24, 1973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabir, M.; Arif, M.; Ahmad, S.; Ali, Z.; Swati, Z.N.K.; Yu, D.-J. Intelligent computational method for discrimination of anticancer peptides by incorporating sequential and evolutionary profiles information. Chemom. Intell. Lab. Syst. 2018, 182, 158–165. [Google Scholar] [CrossRef]
- Meng, C.; Wei, L.; Zou, Q. SecProMTB: Support vector machine-based classifier for secretory proteins using imbalanced data sets applied to Mycobacterium tuberculosis. Proteomics 2019, 19, 1900007. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Breiman, L. Random forests--Random Features; UC Berkeley Technical Report 567. 1999, pp. 1–29. Available online: https://www.stat.berkeley.edu/~breiman/random-forests.pdf (accessed on 10 August 2021).
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Worachartcheewan, A.; Shoombuatong, W.; Pidetcha, P.; Nopnithipat, W.; Prachayasittikul, V.; Nantasenamat, C. Predicting metabolic syndrome using the random forest method. Sci. World J. 2015, 2015, 581501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Win, T.S.; Schaduangrat, N.; Prachayasittikul, V.; Nantasenamat, C.; Shoombuatong, W. PAAP: A web server for predicting antihypertensive activity of peptides. Future Med. Chem. 2018, 10, 1749–1767. [Google Scholar] [CrossRef]
- Shoombuatong, W.; Schaduangrat, N.; Pratiwi, R.; Nantasenamat, C. THPep: A machine learning-based approach for predicting tumor homing peptides. Comput. Biol. Chem. 2019, 80, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Pratiwi, R.; Malik, A.A.; Schaduangrat, N.; Prachayasittikul, V.; Wikberg, J.E.; Nantasenamat, C.; Shoombuatong, W. CryoProtect: A web server for classifying antifreeze proteins from nonantifreeze proteins. J. Chem. 2017, 2017, 9861752. [Google Scholar] [CrossRef]
- Laengsri, V.; Shoombuatong, W.; Adirojananon, W.; Nantasenamart, C.; Prachayasittikul, V.; Nuchnoi, P. ThalPred: A web-based prediction tool for discriminating thalassemia trait and iron deficiency anemia. BMC Med Inform. Decis. Mak. 2019, 19, 212. [Google Scholar]
- Hongjaisee, S.; Nantasenamat, C.; Carraway, T.S.; Shoombuatong, W. HIVCoR: A sequence-based tool for predicting HIV-1 CRF01_AE coreceptor usage. Comput. Biol. Chem. 2019, 80, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.M.; Schaduangrat, N.; Basith, S.; Lee, G.; Shoombuatong, W.; Manavalan, B. HLPpred-Fuse: Improved and robust prediction of hemolytic peptide and its activity by fusing multiple feature representation. Bioinformatics 2020, 36, 3350–3356. [Google Scholar] [CrossRef]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees; Routledge: Boca Raton, FL, USA, 2017. [Google Scholar]
- Lundberg, S.M.; Lee, S.-I. A unified approach to interpreting model predictions. In Proceedings of the 31st international conference on neural information processing systems 2017, Long Beach, CA, USA, 4 December 2017; pp. 4765–4774. [Google Scholar]
- Charoenkwan, P.; Hwang, E.; Cutler, R.W.; Lee, H.-C.; Ko, L.-W.; Huang, H.-L.; Ho, S.-Y. HCS-Neurons: Identifying phenotypic changes in multi-neuron images upon drug treatments of high-content screening. BMC Bioinform. 2013, 14, S12. [Google Scholar] [CrossRef] [Green Version]
- Charoenkwan, P.; Kanthawong, S.; Schaduangrat, N.; Yana, J.; Shoombuatong, W. PVPred-SCM: Improved prediction and analysis of phage virion proteins using a scoring card method. Cells 2020, 9, 353. [Google Scholar] [CrossRef] [Green Version]
- Charoenkwan, P.; Schaduangrat, N.; Nantasenamat, C.; Piacham, T.; Shoombuatong, W. iQSP: A sequence-based tool for the prediction and analysis of quorum sensing peptides via chou’s 5-steps rule and informative physicochemical properties. Int. J. Mol. Sci. 2020, 21, 75. [Google Scholar] [CrossRef] [Green Version]
- Charoenkwan, P.; Shoombuatong, W.; Lee, H.-C.; Chaijaruwanich, J.; Huang, H.-L.; Ho, S.-Y. SCMCRYS: Predicting protein crystallization using an ensemble scoring card method with estimating propensity scores of P-collocated amino acid pairs. PLoS ONE 2013, 8, e72368. [Google Scholar] [CrossRef]
- Charoenkwan, P.; Yana, J.; Schaduangrat, N.; Nantasenamat, C.; Hasan, M.M.; Shoombuatong, W. iBitter-SCM: Identification and characterization of bitter peptides using a scoring card method with propensity scores of dipeptides. Genomics 2020, 112, 2813–2822. [Google Scholar] [CrossRef]
- Abraham, A.; Pedregosa, F.; Eickenberg, M.; Gervais, P.; Mueller, A.; Kossaifi, J.; Gramfort, A.; Thirion, B.; Varoquaux, G. Machine learning for neuroimaging with scikit-learn. Front. Neuroinform. 2014, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Zhang, Y.; Li, R.; Mao, H.; Liu, P. Risk of parametrial invasion in women with early stage cervical cancer: A meta-analysis. Arch. Gynecol. Obstet. 2018, 297, 573–580. [Google Scholar] [CrossRef]
- Covens, A.; Rosen, B.; Murphy, J.; Laframboise, S.; DePetrillo, A.D.; Lickrish, G.; Colgan, T.; Chapman, W.; Shaw, P. How important is removal of the parametrium at surgery for carcinoma of the cervix? Gynecol. Oncol. 2002, 84, 145–149. [Google Scholar] [CrossRef]
- Frumovitz, M.; Sun, C.C.; Schmeler, K.M.; Deavers, M.T.; Dos Reis, R.; Levenback, C.F.; Ramirez, P.T. Parametrial involvement in radical hysterectomy specimens for women with early-stage cervical cancer. Obstet. Gynecol. 2009, 114, 93–99. [Google Scholar] [CrossRef]
- Kinney, W.K.; Hodge, D.O.; Egorshin, E.V.; Ballard, D.J.; Podratz, K.C. Identification of a low-risk subset of patients with stage IB invasive squamous cancer of the cervix possibly suited to less radical surgical treatment. Gynecol. Oncol. 1995, 57, 3–6. [Google Scholar] [CrossRef]
- Stegeman, M.; Louwen, M.; van der Velden, J.; ten Kate, F.J.; den Bakker, M.A.; Burger, C.W.; Ansink, A.C. The incidence of parametrial tumor involvement in select patients with early cervix cancer is too low to justify parametrectomy. Gynecol. Oncol. 2007, 105, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Vranes, B.; Milenkovic, S.; Radojevic, M.; Soldatovic, I.; Kesic, V. Risk of parametrial spread in small stage I cervical carcinoma: Pathology review of 223 cases with a tumor diameter of 20 mm or less. Int. J. Gynecol. Cancer 2016, 26, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Zapardiel, I.; Zanagnolo, V.; Mangioni, C. Class I versus class III radical hysterectomy in stage IB1-IIA cervical cancer. A prospective randomized study. Eur. J. Surg. Oncol. 2012, 38, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Sia, T.Y.; Chen, L.; Melamed, A.; Tergas, A.I.; Khoury-Collado, F.; Hou, J.Y.; St Clair, C.M.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L.; et al. Trends in use and effect on survival of simple hysterectomy for early-stage cervical cancer. Obstet. Gynecol. 2019, 134, 1132–1143. [Google Scholar] [CrossRef]
- de Boer, P.; Adam, J.A.; Buist, M.R.; van de Vijver, M.J.; Rasch, C.R.; Stoker, J.; Bipat, S.; Stalpers, L.J. Role of MRI in detecting involvement of the uterine internal os in uterine cervical cancer: Systematic review of diagnostic test accuracy. Eur. J. Radiol. 2013, 82, e422–e428. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Training Set (n = 1112) | Testing Set (n = 116) | p-Value |
|---|---|---|---|
| Age (year) | 47.33 ± 8.98 | 48.44 ± 9.85 | 0.21 |
| Parity | 2.00 (1.00–2.00) | 2.00 (1.00–2.00) | 0.12 |
| HIV positivity | 7 (0.6) | 3 (2.6) | 0.03 * |
| Menopause | 378 (34.0) | 47 (40.5) | 0.16 |
| Underlying medical disease | 379 (34.1) | 47 (40.5) | 0.17 |
| Previous abdominal surgery | 382 (34.4) | 51 (44.0) | 0.04 * |
| Prior conization | 487 (43.8) | 44 (37.9) | 0.23 |
| Tumor appearance | 0.28 | ||
| No gross lesion | 489 (46.3) | 46 (41.5) | |
| Exophytic | 224 (21.2) | 26 (23.4) | |
| Infiltrative | 298 (28.2) | 32 (28.8) | |
| Ulcerative | 13 (1.2) | 0 (0.0) | |
| Mixed | 33 (3.1) | 7 (6.3) | |
| Tumor size (cm) | 1.50 (0.00–3.00) | 2.00 (0.00–3.00) | 0.10 |
| Stage | 0.21 | ||
| IA | 204 (18.3) | 14 (12.0) | |
| IB1 | 779 (70.1) | 88 (75.9) | |
| IB2 | 27 (2.4) | 5 (4.3) | |
| IIA | 102 (9.2) | 9 (7.8) | |
| Final histology | 0.27 | ||
| Squamous | 742 (66.7) | 71 (61.2) | |
| Adenocarcinoma | 256 (23.0) | 36 (31.1) | |
| Adenosquamous | 72 (6.5) | 4 (3.4) | |
| Neuroendocrine | 30 (2.7) | 4 (3.4) | |
| Others | 12 (1.1) | 1 (0.9) | |
| Depth of invasion | 0.07 | ||
| Inner1/3 | 122 (15.5) | 14 (15.1) | |
| Middle1/3 | 180 (22.9) | 12 (12.9) | |
| Outer1/3 | 485 (61.6) | 67 (72.0) | |
| Uterine metastasis | 0.19 | ||
| No | 992 (89.2) | 100 (86.2) | |
| Yes | 95 (8.5) | 15 (12.9) | |
| HSIL | 25 (2.3) | 1 (0.9) | |
| Vaginal metastasis | 0.03 * | ||
| No | 896 (80.9) | 91 (78.5) | |
| Yes | 125 (11.3) | 21 (18.1) | |
| HSIL | 87 (7.8) | 4 (3.4) | |
| Pelvic LN metastasis | 189 (17.0) | 24 (20.7) | 0.20 |
| LVSI number in surgical specimen | 2.00 (0.00–14.00) | 3.00 (0.00–15.00) | 0.23 |
| Parametrial metastasis | 171 (15.4) | 30 (25.9) | <0.01 * |
| Factor a | Ac | Sn | Sp | MCC | AUC |
|---|---|---|---|---|---|
| baseline | 0.756 | 0.267 | 0.914 | 0.231 | 0.758 |
| (0.678–0.834) | (0.186–0.348) | (0.863–0.965) | (0.154–0.308) | (0.680–0.836) | |
| baseline+pelvicme | 0.846 | 0.567 | 0.935 | 0.553 | 0.85 |
| (0.780–0.912) | (0.477–0.657) | (0.890–0.980) | (0.463–0.643) | (0.785–0.915) | |
| baseline+utmet | 0.793 | 0.367 | 0.942 | 0.392 | 0.768 |
| (0.719–0.867) | (0.279–0.455) | (0.899–0.985) | (0.303–0.481) | (0.691–0.845) | |
| baseline+vgmet | 0.732 | 0.3 | 0.871 | 0.195 | 0.644 |
| (0.651–0.813) | (0.217–0.450) | (0.810–0.932) | (0.123–0.267) | (0.557–0.731) | |
| baseline+pelvicme+utmet | 0.862 | 0.6 | 0.953 | 0.618 | 0.905 |
| (0.799–0.925) | (0.511–0.689) | (0.914–0.987) | (0.530–0.706) | (0.852–0.958) | |
| baseline+pelvicme+vgmet | 0.821 | 0.433 | 0.946 | 0.461 | 0.841 |
| (0.751–0.891) | (0.343–0.523) | (0.905–0.987) | (0.370–0.552) | (0.774–0.908) | |
| baseline+utmet+vgmet | 0.793 | 0.367 | 0.942 | 0.392 | 0.768 |
| (0.719–0.867) | (0.279–0.455) | (0.899–0.985) | (0.303–0.481) | (0.691–0.845) | |
| baseline+pelvicme+utmet+vgmet | 0.836 | 0.533 | 0.942 | 0.54 | 0.879 |
| (0.769–0.903) | (0.442–0.624) | (0.899–0.985) | (0.449–0.631) | (0.820–0.938) |
| Classifier a | Ac | Sn | Sp | MCC | AUC |
|---|---|---|---|---|---|
| iPMI-Power | 0.862 | 0.6 | 0.953 | 0.618 | 0.905 |
| (0.799–0.925) | (0.511–0.689) | (0.914–0.992) | (0.530–0.706) | (0.852–0.958) | |
| SVM | 0.802 | 0.6 | 0.872 | 0.477 | 0.761 |
| (0.729–0.875) | (0.511–0.689) | (0.811–0.933) | (0.386–0.568) | (0.683–0.839) | |
| DT | 0.819 | 0.6 | 0.895 | 0.513 | 0.751 |
| (0.749–0.889) | (0.511–0.689) | (0.839–0.951) | (0.422–0.604) | (0.672–0.830) | |
| XGB | 0.862 | 0.567 | 0.965 | 0.616 | 0.873 |
| (0.799–0.925) | (0.477–0.657) | (0.932–0.998) | (0.527–0.705) | (0.812–0.934) | |
| kNN | 0.802 | 0.567 | 0.884 | 0.467 | 0.725 |
| (0.729–0.875) | (0.477–0.657) | (0.826–0.942) | (0.376–0.558) | (0.644–0.806) | |
| iPMI-Econ | 0.756 | 0.267 | 0.914 | 0.231 | 0.758 |
| (0.678–0.834) | (0.186–0.348) | (0.863–0.965) | (0.154–0.308) | (0.680–0.836) | |
| MLP | 0.836 | 0.667 | 0.895 | 0.568 | 0.843 |
| (0.769–0.903) | (0.581–0.753) | (0.839–0.951) | (0.478–0.658) | (0.777–0.909) | |
| LR | 0.784 | 0.833 | 0.767 | 0.54 | 0.869 |
| (0.729–0.859) | (0.765–0.901) | (0.690–0.844) | (0.449–0.631) | (0.808–0.930) | |
| NB | 0.664 | 0.867 | 0.593 | 0.403 | 0.844 |
| (0.578–0.750) | (0.805–0.929) | (0.504–0.682) | (0.314–0.492) | (0.778–0.910) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charoenkwan, P.; Shoombuatong, W.; Nantasupha, C.; Muangmool, T.; Suprasert, P.; Charoenkwan, K. iPMI: Machine Learning-Aided Identification of Parametrial Invasion in Women with Early-Stage Cervical Cancer. Diagnostics 2021, 11, 1454. https://doi.org/10.3390/diagnostics11081454
Charoenkwan P, Shoombuatong W, Nantasupha C, Muangmool T, Suprasert P, Charoenkwan K. iPMI: Machine Learning-Aided Identification of Parametrial Invasion in Women with Early-Stage Cervical Cancer. Diagnostics. 2021; 11(8):1454. https://doi.org/10.3390/diagnostics11081454
Chicago/Turabian StyleCharoenkwan, Phasit, Watshara Shoombuatong, Chalaithorn Nantasupha, Tanarat Muangmool, Prapaporn Suprasert, and Kittipat Charoenkwan. 2021. "iPMI: Machine Learning-Aided Identification of Parametrial Invasion in Women with Early-Stage Cervical Cancer" Diagnostics 11, no. 8: 1454. https://doi.org/10.3390/diagnostics11081454