
Systemic Investigation Identifying Salivary miR-196b as a Promising Biomarker for Early Detection of Head-Neck Cancer and Oral Precancer Lesions

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and the Saliva Sample Collection
2.2. MicroRNA Extraction and Analysis
2.3. Bioinformatic Assessment of the Specific miRNAs in the Diagnostic Potential for HNSC
2.4. Statistical Analyses
3. Results
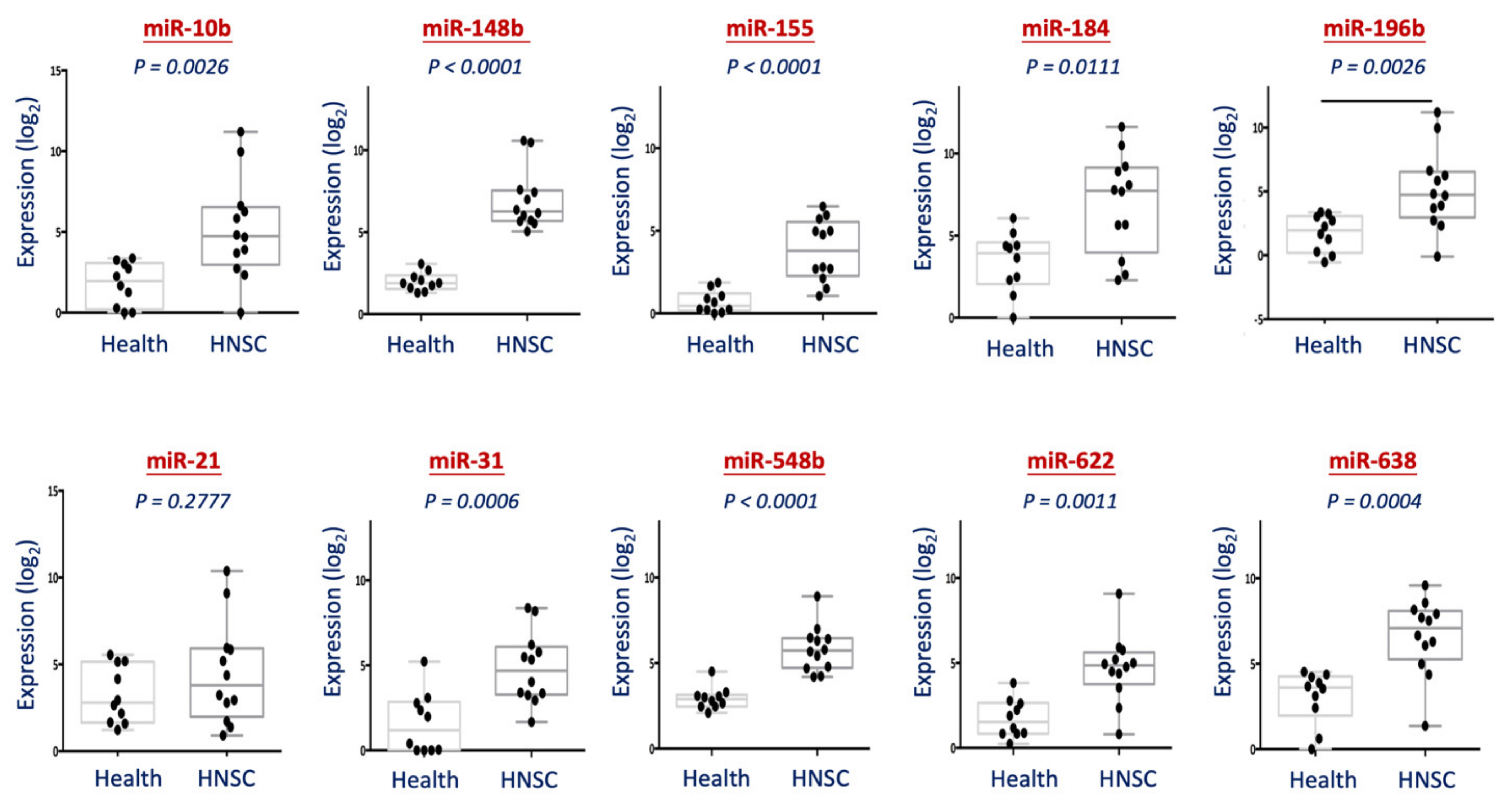
3.1. Analysis of 10 miRNAs from Saliva Specimen between Healthy Individuals and HNSC Patients
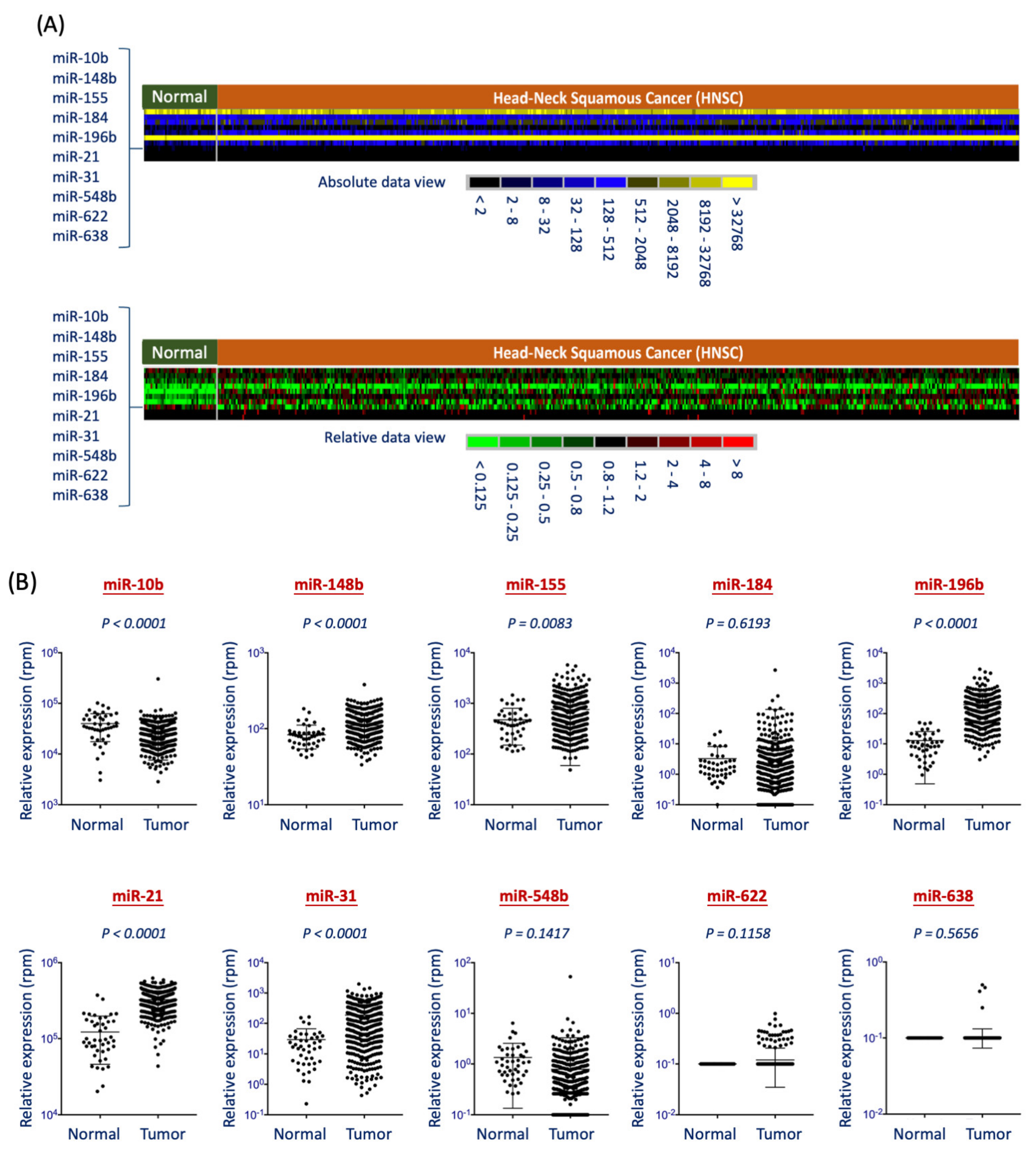
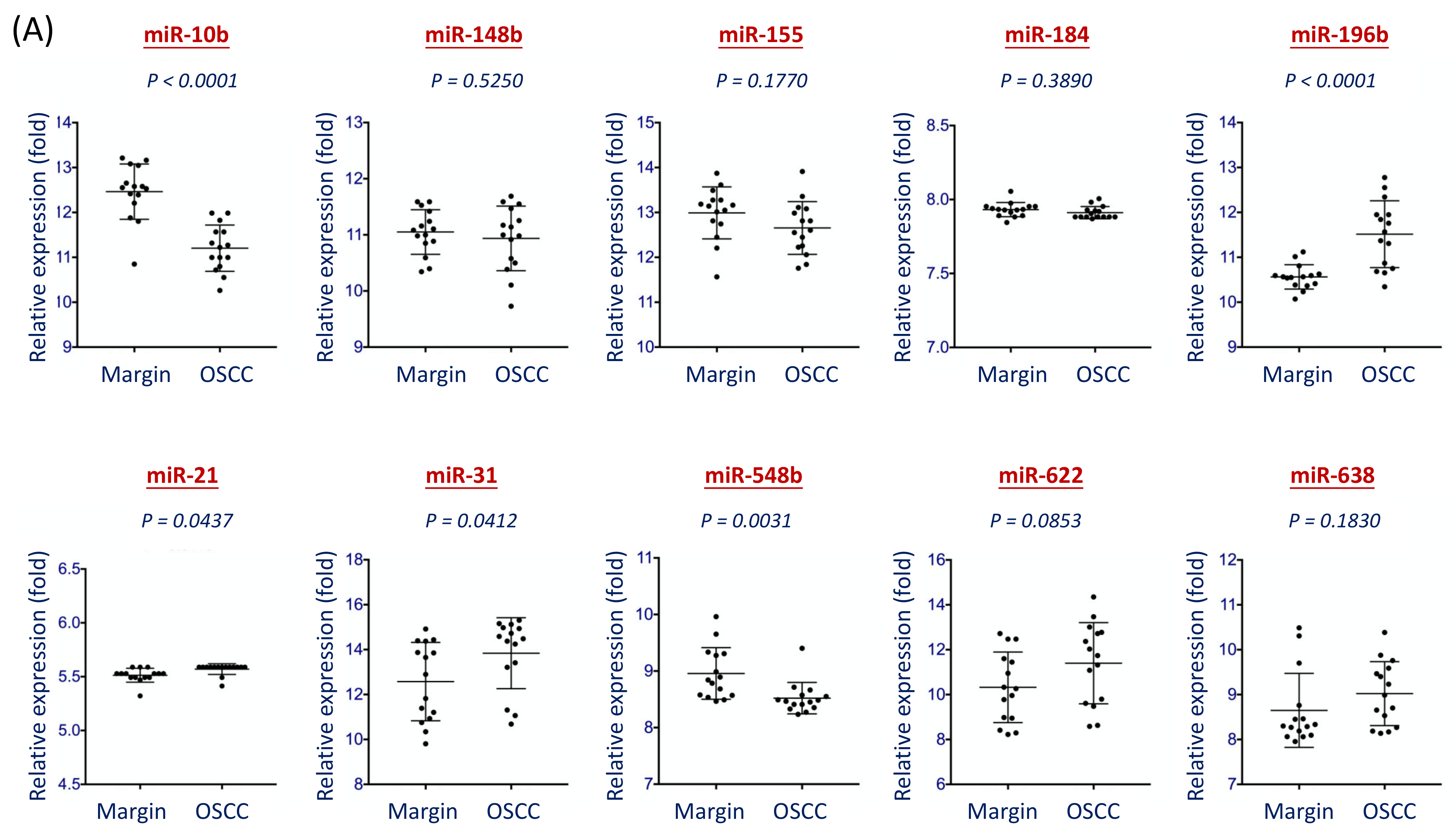
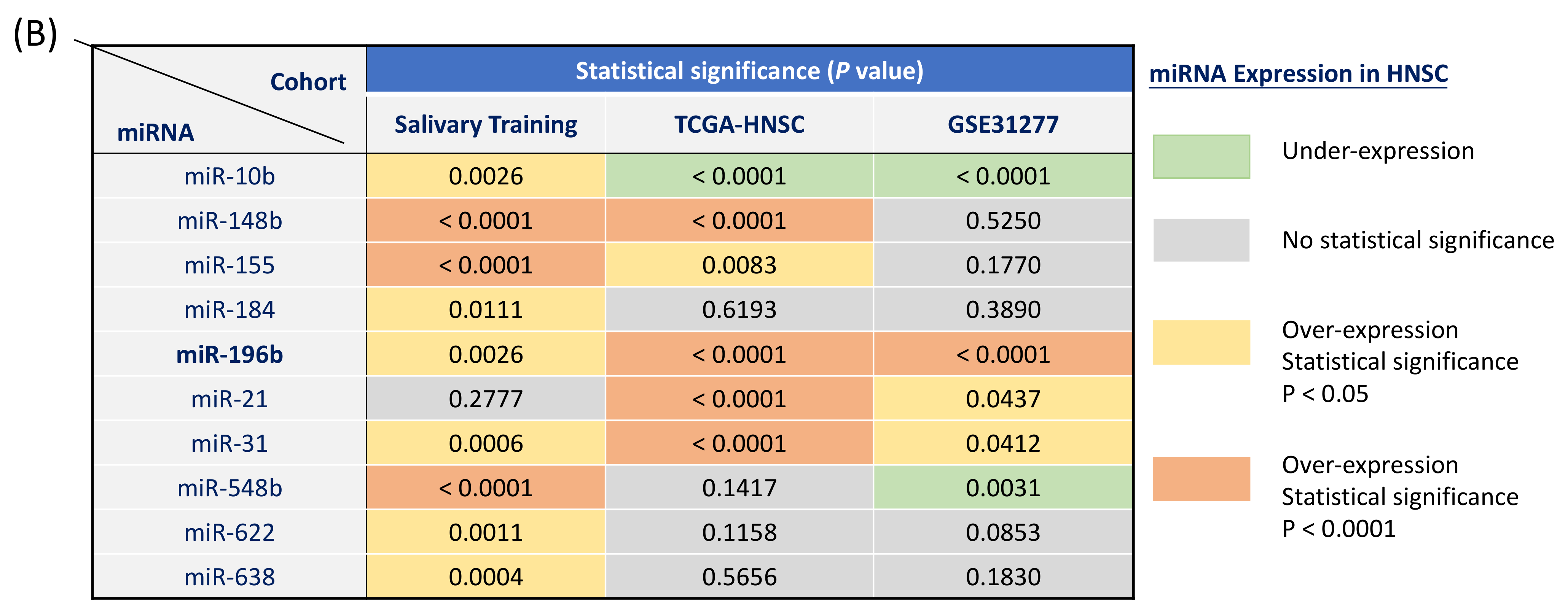
3.2. Examination of miRNA Biomarker Specific for HNSC Patients Using Two Independent Cohorts
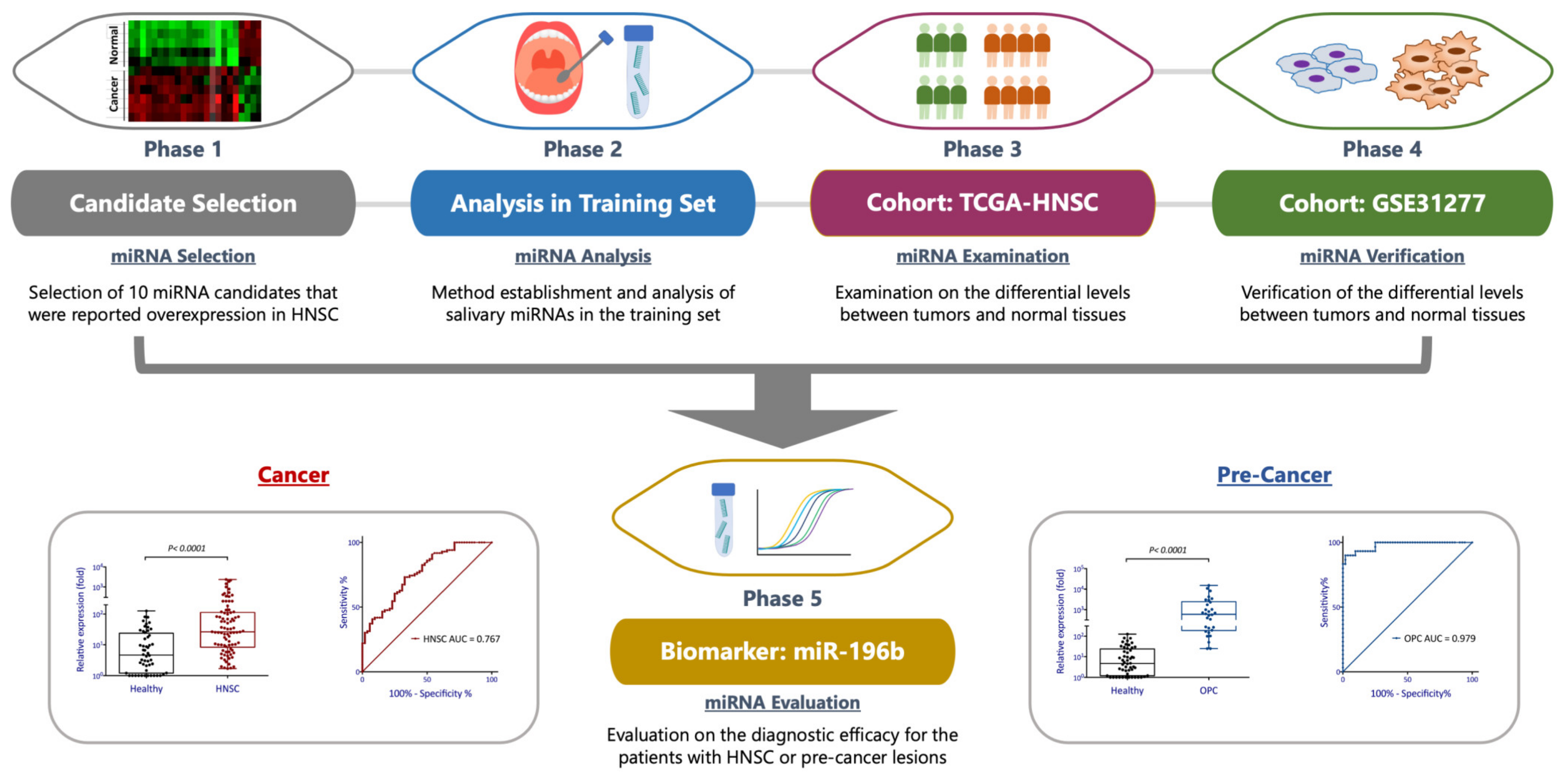
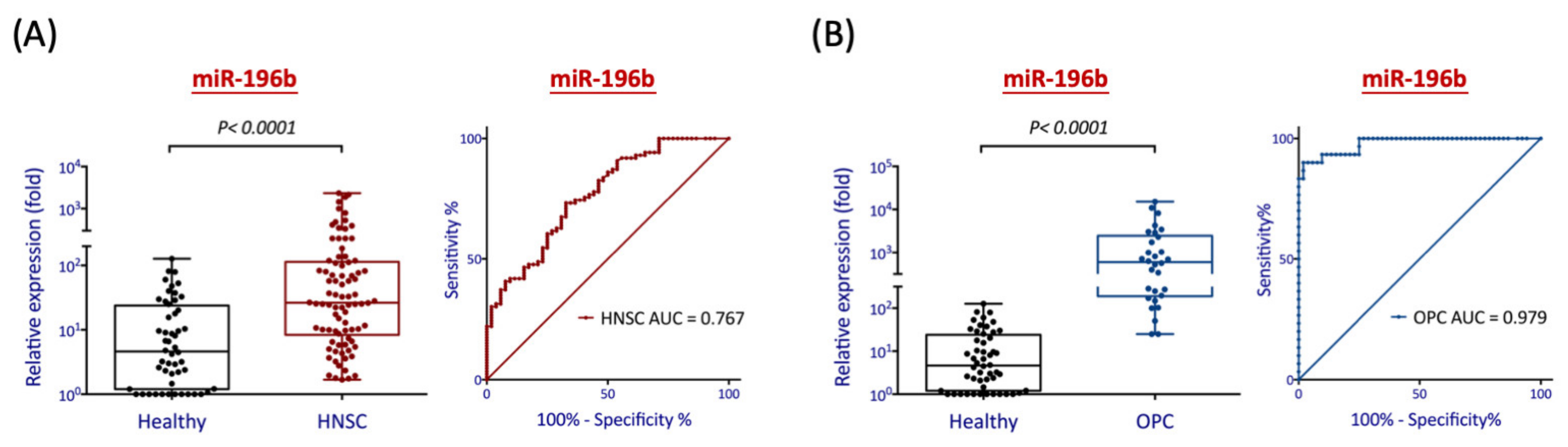
3.3. Evaluation of Salivary miR-196b as a Diagnostic Biomarker for Detection of HNSC and PreMalignancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Peitzsch, C.; Nathansen, J.; Schniewind, S.I.; Schwarz, F.; Dubrovska, A. Cancer Stem Cells in Head and Neck Squamous Cell Carcinoma: Identification, Characterization and Clinical Implications. Cancers 2019, 11, 616. [Google Scholar] [CrossRef] [Green Version]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Hisamatsu, K.; Suzui, N.; Hara, A.; Tomita, H.; Miyazaki, T.; Kobayashi, K.; Hisamatsu, K.; Suzui, N.; Hara, A.; et al. A Review of HPV-Related Head and Neck Cancer. J. Clin. Med. 2018, 7, 241. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.-C.; Cheng, A.-J.; Lee, L.-Y.; Huang, Y.-C.; Chang, J.T.-C. Multifaceted Mechanisms of Areca Nuts in Oral Carcinogenesis: The Molecular Pathology from Precancerous Condition to Malignant Transformation. J. Cancer 2019, 10, 4054–4062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, I.-B.; Tseng, Y.-T.; Su, C.-C.; Tsai, K.-Y. Progression of precancerous lesions to oral cancer: Results based on the Taiwan National Health Insurance Database. Oral Oncol. 2013, 49, 427–430. [Google Scholar] [CrossRef]
- Melchardt, T.; Magnes, T.; Hufnagl, C.; Thorner, A.R.; Ducar, M.; Neureiter, D.; Tränkenschuh, W.; Klieser, E.; Gaggl, A.; Rösch, S.; et al. Clonal evolution and heterogeneity in metastatic head and neck cancer—An analysis of the Austrian Study Group of Medical Tumour Therapy study group. Eur. J. Cancer 2018, 93, 69–78. [Google Scholar] [CrossRef]
- Kong, L.; Birkeland, A. Liquid Biopsies in Head and Neck Cancer: Current State and Future Challenges. Cancers 2021, 13, 1874. [Google Scholar] [CrossRef]
- Lustberg, M.B.; Stover, D.; Chalmers, J.J. Implementing Liquid Biopsies in Clinical Trials: State of affairs, opportunities, and challenges. Cancer J. 2018, 24, 61–64. [Google Scholar] [CrossRef]
- Di Meo, A.; Bartlett, J.; Cheng, Y.; Pasic, M.D.; Yousef, G.M. Liquid biopsy: A step forward towards precision medicine in urologic malignancies. Mol. Cancer 2017, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, T.; Wong, D. Liquid Biopsy in Head and Neck Cancer: Promises and Challenges. J. Dent. Res. 2018, 97, 701–708. [Google Scholar] [CrossRef]
- Malapelle, U.; Buono, M.; Pisapia, P.; Russo, G.; Tufano, R.; Pepe, F.; Rolfo, C.; Troncone, G. Circulating tumor DNA in cancer: Predictive molecular pathology meets mathematics. Crit. Rev. Oncol. 2021, 163, 103394. [Google Scholar] [CrossRef] [PubMed]
- Lianidou, E. Detection and relevance of epigenetic markers on ctDNA: Recent advances and future outlook. Mol. Oncol. 2021, 15, 1683–1700. [Google Scholar] [CrossRef]
- Mazumder, S.; Datta, S.; Ray, J.G.; Chaudhuri, K.; Chatterjee, R. Liquid biopsy: miRNA as a potential biomarker in oral cancer. Cancer Epidemiol. 2019, 58, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Sohel, M.H. Circulating microRNAs as biomarkers in cancer diagnosis. Life Sci. 2020, 248, 117473. [Google Scholar] [CrossRef]
- Cochetti, G.; Cari, L.; Nocentini, G.; Maulà, V.; Suvieri, C.; Cagnani, R.; De Vermandois, J.A.R.; Mearini, E. Detection of urinary miRNAs for diagnosis of clear cell renal cell carcinoma. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef]
- HasanoĞlu, S.; Göncü, B.S.; Yücesan, E.; Atasoy, S.; Kayali, Y.; Kandaş, N. Investigating differential miRNA expression profiling using serum and urine specimens for detecting potential biomarker for early prostate cancer diagnosis. Turk. J. Med Sci. 2021. [Google Scholar] [CrossRef]
- Hoshino, I. The usefulness of microRNA in urine and saliva as a biomarker of gastroenterological cancer. Int. J. Clin. Oncol. 2021, 26, 1431–1440. [Google Scholar] [CrossRef]
- Deutsch, F.T.; Khoury, S.J.; Sunwoo, J.B.; Elliott, M.S.; Tran, N.T. Application of salivary noncoding microRNAs for the diagnosis of oral cancers. Head Neck 2020, 42, 3072–3083. [Google Scholar] [CrossRef]
- Salim, U.; Kumar, A.; Kulshreshtha, R.; Vivekanandan, P. Biogenesis, characterization, and functions of mirtrons. Wiley Interdiscip. Rev. RNA 2021, e1680. [Google Scholar] [CrossRef]
- Inoue, J.; Inazawa, J. Cancer-associated miRNAs and their therapeutic potential. J. Hum. Genet. 2021, 1–9. [Google Scholar] [CrossRef]
- Hui, A.B.; Lenarduzzi, M.; Krushel, T.; Waldron, L.; Pintilie, M.; Shi, W.; Perez-Ordonez, B.; Jurisica, I.; O’Sullivan, B.; Waldron, J.; et al. Comprehensive MicroRNA Profiling for Head and Neck Squamous Cell Carcinomas. Clin. Cancer Res. 2010, 16, 1129–1139. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Chen, Z.; Yu, J.; Xia, J.; Zhou, X. MicroRNA Profiling and Head and Neck Cancer. Comp. Funct. Genom. 2009, 2009, 1–11. [Google Scholar] [CrossRef]
- Lu, Y.-C.; Chen, Y.-J.; Wang, H.-M.; Tsai, C.-N.; Chen, W.-H.; Huang, Y.-C.; Fan, K.-H.; Huang, S.-F.; Kang, C.-J.; Chang, J.T.-C.; et al. Oncogenic Function and Early Detection Potential of miRNA-10b in Oral Cancer as Identified by microRNA Profiling. Cancer Prev. Res. 2012, 5, 665–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, H.-F.; Lin, S.-C.; Chang, K.-W. MicroRNA aberrances in head and neck cancer: Pathogenetic and clinical significance. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 104–111. [Google Scholar] [CrossRef]
- Chen, D.; Cabay, R.J.; Jin, Y.; Wang, A.; Lu, Y.; Shah-Khan, M.; Zhou, X. MicroRNA Deregulations in Head and Neck Squamous Cell Carcinomas. J. Oral Maxillofac. Res. 2013, 4, e2. [Google Scholar] [CrossRef]
- Zhang, H.; Linqing, Z.; Zheng, L.; Huang, X. Biomarker MicroRNAs for Diagnosis of Oral Squamous Cell Carcinoma Identified Based on Gene Expression Data and MicroRNA-mRNA Network Analysis. Comput. Math. Methods Med. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Koshizuka, K.; Hanazawa, T.; Arai, T.; Okato, A.; Kikkawa, N.; Seki, N. Involvement of aberrantly expressed microRNAs in the pathogenesis of head and neck squamous cell carcinoma. Cancer Metastasis Rev. 2017, 36, 525–545. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, W.; Kumar, A. microRNAs in oral cancer: Moving from bench to bed as next generation medicine. Oral Oncol. 2020, 111, 104916. [Google Scholar] [CrossRef] [PubMed]
- AI Rawi, N.; Elmabrouk, N.; Kou, R.A.; Mkadmi, S.; Rizvi, Z.; Hamdoon, Z. The role of differentially expressed salivary microRNA in oral squamous cell carcinoma. A systematic review. Arch. Oral Biol. 2021, 125, 105108. [Google Scholar] [CrossRef]
- Elewaily, M.I.; Elsergany, A.R. Emerging role of exosomes and exosomal microRNA in cancer: Pathophysiology and clinical potential. J. Cancer Res. Clin. Oncol. 2021, 147, 637–648. [Google Scholar] [CrossRef]
- Lu, Y.-C.; Chang, J.T.; Liao, C.-T.; Kang, C.-J.; Huang, S.-F.; Chen, I.-H.; Huang, C.-C.; Huang, Y.-C.; Chen, W.-H.; Tsai, C.-Y.; et al. OncomiR-196 promotes an invasive phenotype in oral cancer through the NME4-JNK-TIMP1-MMP signaling pathway. Mol. Cancer 2014, 13, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valastyan, S.; Weinberg, R.A. miR-31: A crucial overseer of tumor metastasis and other emerging roles. Cell Cycle 2010, 9, 2124–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurila, E.; Kallioniemi, A. The diverse role of miR-31 in regulating cancer associated phenotypes. Genes Chromosom. Cancer 2013, 52, 1103–1113. [Google Scholar] [CrossRef]
- Yu, T.; Ma, P.; Wu, D.; Shu, Y.; Gao, W. Functions and mechanisms of microRNA-31 in human cancers. Biomed. Pharmacother. 2018, 108, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.-F.; Liu, C.-J.; Chiu, P.-C.; Lin, J.-S.; Chang, K.-W.; Shih, W.-Y.; Kao, S.-Y.; Tu, H.-F. MicroRNA-31 upregulation predicts increased risk of progression of oral potentially malignant disorder. Oral Oncol. 2016, 53, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-J.; Lin, S.-C.; Yang, C.-C.; Cheng, H.-W.; Chang, K.-W. Exploiting salivary miR-31 as a clinical biomarker of oral squamous cell carcinoma. Head Neck 2011, 34, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Pourdavoud, P.; Pakzad, B.; Mosallaei, M.; Saadatian, Z.; Esmaeilzadeh, E.; Alimolaie, A.; Shaygannejad, A. MiR-196: Emerging of a new potential therapeutic target and biomarker in colorectal cancer. Mol. Biol. Rep. 2020, 47, 9913–9920. [Google Scholar] [CrossRef]
- Lu, Y.-C.; Chang, J.T.; Chan, E.-C.; Chao, Y.K.; Yeh, T.-S.; Chen, J.-S.; Cheng, A.-J. miR-196, an Emerging Cancer Biomarker for Digestive Tract Cancers. J. Cancer 2016, 7, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Zhang, Y.; Zhang, L.; Weakley, S.M.; Yao, Q. MicroRNA-196: Critical roles and clinical applications in development and cancer. J. Cell. Mol. Med. 2011, 15, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.-C.; Chang, J.T.-C.; Huang, Y.-C.; Huang, C.-C.; Chen, W.-H.; Lee, L.-Y.; Huang, B.-S.; Chen, Y.-J.; Li, H.-F.; Cheng, A.-J. Combined determination of circulating miR-196a and miR-196b levels produces high sensitivity and specificity for early detection of oral cancer. Clin. Biochem. 2015, 48, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yao, C.; Li, H.; Wang, G.; He, X. Combined Elevation of microRNA-196a and microRNA-196b in Sera Predicts Unfavorable Prognosis in Patients with Osteosarcomas. Int. J. Mol. Sci. 2014, 15, 6544–6555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.-M.; Wang, C.-S.; Tsai, C.-Y.; Huang, C.-G.; Lee, K.-F.; Huang, H.-W.; Lin, Y.-H.; Chi, H.-C.; Kuo, L.-M.; Lu, P.-H.; et al. Circulating microRNA-196a/b are novel biomarkers associated with metastatic gastric cancer. Eur. J. Cancer 2016, 64, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Blagosklonny, M.V. Carcinogenesis, cancer therapy and chemoprevention. Cell Death Differ. 2005, 12, 592–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayáns, P.; Pérez-Sayáns, M.; Somoza-Martín, J.M.; Barros-Angueira, F.; Reboiras-López, M.D.; Rey, J.M.G.; García-García, A. Genetic and molecular alterations associated with oral squamous cell cancer. Oncol. Rep. 2009, 22, 1277–1282. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, I.A.; Sanna, V.; Ahmad, N.; Sechi, M.; Mukhtar, H. Resveratrol nanoformulation for cancer prevention and therapy. Ann. N. Y. Acad. Sci. 2015, 1348, 20–31. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Cancer | Precancer | Normal |
|---|---|---|---|
| Sex | |||
| Male | 75 (87%) | 26 (87%) | 36 (69%) |
| Female | 11 (13%) | 4 (13%) | 16 (31%) |
| Age | |||
| Range (year old) | 19–82 | 33–81 | 22–73 |
| Mean ± SD (years) | 50.8 ± 12.4 | 49.5 ± 13.4 | 45.3 ± 11.2 |
| <40 years old | 14 (16%) | 9 (30%) | 12 (23%) |
| 40–49 years old | 27 (31%) | 7 (23%) | 18 (35%) |
| 50–59 years old | 24 (28%) | 7 (23%) | 17 (33%) |
| ≥60 years old | 21 (24%) | 7 (23%) | 5 (10%) |
| Habits | |||
| Alcohol drinking | 42 (48%) | 12 (40%) | |
| Betel quid chewing | 40 (47%) | 9 (30%) | |
| Cigarette smoking | 49 (57%) | 20 (67%) | |
| Pathologic T-status | |||
| T1-T2 | 41 (48%) | ||
| T3-T4 | 45 (52%) | ||
| Pathologic N-status | |||
| pN0 | 28 (33%) | ||
| pN+ | 58 (67%) | ||
| Pathologic overall stage | |||
| I–II | 21 (24%) | ||
| III–IV | 65 (76%) | ||
| Total | 86 (100%) | 30 (100%) | 52 (100%) |
| Saliva miR-196b | |||||
|---|---|---|---|---|---|
| Disease | p-Value | AUC | Sensitivity | Specificity | Odds Ratio |
| (% Range) | (% Range) | (Range) | |||
| HNSC | <0.001 | 0.767 | 73.3% | 67.3 % | 5.64 |
| (63~83) | (53~80) | (2.7~12.0) | |||
| Oral Precancer | <0.001 | 0.979 | 90.0% | 98.1% | 459 |
| (74~98) | (90~100) | (45~4627) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, A.-J.; You, G.-R.; Lee, C.-J.; Lu, Y.-C.; Tang, S.-J.; Huang, Y.-F.; Huang, Y.-C.; Lee, L.-Y.; Fan, K.-H.; Chen, Y.-C.; et al. Systemic Investigation Identifying Salivary miR-196b as a Promising Biomarker for Early Detection of Head-Neck Cancer and Oral Precancer Lesions. Diagnostics 2021, 11, 1411. https://doi.org/10.3390/diagnostics11081411
Cheng A-J, You G-R, Lee C-J, Lu Y-C, Tang S-J, Huang Y-F, Huang Y-C, Lee L-Y, Fan K-H, Chen Y-C, et al. Systemic Investigation Identifying Salivary miR-196b as a Promising Biomarker for Early Detection of Head-Neck Cancer and Oral Precancer Lesions. Diagnostics. 2021; 11(8):1411. https://doi.org/10.3390/diagnostics11081411
Chicago/Turabian StyleCheng, Ann-Joy, Guo-Rung You, Che-Jui Lee, Ya-Ching Lu, Shang-Ju Tang, Yi-Fang Huang, Yu-Chen Huang, Li-Yu Lee, Kang-Hsing Fan, Yen-Chao Chen, and et al. 2021. "Systemic Investigation Identifying Salivary miR-196b as a Promising Biomarker for Early Detection of Head-Neck Cancer and Oral Precancer Lesions" Diagnostics 11, no. 8: 1411. https://doi.org/10.3390/diagnostics11081411